Download presentation
Presentation is loading. Please wait.

1
SPHSC 543 MARCH 5 & 12, 2010 Questions?

3
TREATMENT Assessment will have identified if there is a problem and what the problem is. Any treatment plan must meet three criteria: should be safe should strive to maintain optimal nutrition should be farsighted

4
TREATMENT What the child needs to bring to the treatment process: …Functioning GI system …Stable pulmonary system …Developmentally appropriate oral sensorimotor and feeding skills Look at relationships between oral and respiratory systems, and child’s learning and communication strategies.

5
TREATMENT What influences tone/movement patterns? Look at limiting movement patterns and look for automatic reflexes that can be elicited to promote normal patterns of movement. Family dynamics …Important in evaluation and treatment planning

6
BASIC PRINCIPLES Facilitate normal patterns of movement and normalize ability to accept/integrate input – visual, auditory, vestibular, taste and temperature Include treatment into typical ADLs of childhood …Mealtime …Toothbrushing …Bathing …Dressing …Play Remember: The ultimate goal may not be achieving full oral feeding …Success may include whole or part nutrition by non-oral means

7
TREATMENT Can be direct …Oral “exercises” …Non-nutritive oral stimulation (NNOS) …Therapeutic tastes Can be indirect …Alterations in Environment Positioning Seating Communication signals Food consistency
 …Therapeutic tastes Can be indirect …Alterations in Environment Positioning Seating Communication signals Food consistency")
8
TERMINIOLOGY Feeding Therapy Implies primary goal is oral feeding Oral Sensorimotor Treatment …Primary goal is coordinated movements of the mouth, respiratory and phonatory systems for communication and oral feeding …Focus is on the ‘total’ child

9
TREATMENT VS MANAGEMENT Treatment …Goal is to improve a problem or condition underlying feeding dysfunction Management …Underlying cause of problem cannot be modified by treatment techniques at this time …Address symptomatology to maintain health and nutrition …“Buy time” until the underlying problem changes through maturation or medical improvement

10
OPTIONS FOR TREATMENT/MANAGEMENT Medical techniques …Medications, O2, NGT Surgical techniques …Repair of anatomical anomalies …G Tube placement Modification of feeding situation …State …Posture and position …Swallowing …Oral-motor control …Coordination of SSB …Tactile responses

11
GETTING READY Prepare the infant …State, tone and movement, tactile responses Prepare the environment …Visual stimuli …Noise …Temperature Prepare the feeder

12
STATE Feeding possible in drowsy/semi-dozing, quiet alert and active alert states Hypersensitive, easily disorganized –drowsy versus active/alert state Sleepy –very alert Look at patterns of states, transitions between states, and stability of state May need to modify environment during feeding

13
STATE Tactile …Alerting effect …Often combined with movement Temperatures …Cooler …Change clothes/diaper …Unbundle …Cool washcloth

14
AROUSAL From sleepy/semi-drowsy to calm, alert …Variable, not predictable, not rhythmic Movement …Can have a strong alerting effect …Picking up baby, being in an upright position …Rocking from side-to-side Auditory …pitch, tone, rhythm, quiet to louder, lively music

15
CALMING Irritable, crying, hyperstimulated, disorganized, easily startled Containment and rhythmicity are key Tactile …Firm, deep pressure and containment Swaddling …Physical containment …Tonic, disorganized …Frequent, firm proprioceptive and deep pressure contact

16
CALMING Swaddling continued …Arms together in midline, hips flexed, head covered …Use well-flexed, vertical position …Use body – posture and firmness of holding …Infant massage Movement …Rhythmic, constant, predictable …Try different rhythms …Bouncing, rocking when swaddled

17
CALMING Auditory …Decreasing auditory input …White noise, rhythmic, repetitive music …Minimal speech Tone, posture, position …Balance between flexor and extensor …Movements should be smooth and well modulated …Alignment of head, neck and trunk are crucial

18
OPTIMAL FEEDING POSITION Overall flexion Orientation of head and extremities about the midline Shoulders symmetric and forward Arms flexed and toward body midline Hips flexed from 45-90 degrees

19
SEATING/POSITIONING Look at shoulder girdle, trunk, hips/pelvis, sitting base, stability of feet, eye contact/control, head control and spinal mobility …Soft chair (bean bag) or foam/towel between shoulders – retraction …Vest attached to chair, foam/towels on table – protraction …Hold shoulders down …May need trunk supports/pads …Rolled towels under knees – posterior pelvic tilt …Lumbar spine – anterior pelvic tilt …Seat depth, width, angle
 or foam/towel between shoulders – retraction …Vest attached to chair, foam/towels on table – protraction …Hold shoulders down …May need trunk supports/pads …Rolled towels under knees – posterior pelvic tilt …Lumbar spine – anterior pelvic tilt …Seat depth, width, angle")
20
SEATING/POSITIONING …Sitting base – wider (pommel) more stable; hip adductor to bring knees together …Foot rest, towels, blankets, books …Eye control/contact – supine – no demands for head control. …Feeder should be at eye level …Head/spine – must look at hips, pelvis, trunks and shoulder girdle first. Slight recline, head rest, chin tuck …Abdomen – build muscle tone and control. Improve breathing and postural adjustments during mealtimes

21
SEATING/POSITIONING Freedom of movement – spinal movement and changes movement around body axis

22
FEEDING POSITIONS En face …Maximal head control is possible, harder to provide trunk support Supine in lap …Hard to control side-to-side head movement …Hands free tube feeders, pacifier for NNS …Can be inclined Sidelying on lap …Trunk straight and well supported …Helps retracted tongue come forward

25
FEEDING POSITIONS Head in greater flexion …Facilitate sucking and lip seal …Compensate for poor laryngeal elevation Head in slight extension …Assists breathing

26
SWALLOWING Depends on where the problem is: …Poor organization of bolus in oral phase …Delayed swallow reflex initiation …Abnormal pharyngeal phase …Incoordination of pharyngeal/esophageal peristalsis

27
IMPROVE BOLUS FORMATION Problem with tongue control …Provide single bolus then pause to allow organization …Small boluses (0.1-0.5 cc, 1 Tbsp to 2 oz) …Allows establishment of suck …Thicken liquid Moves slower, easier for tongue to maintain bolus
 …Allows establishment of suck …Thicken liquid Moves slower, easier for tongue to maintain bolus")
28
DELAYED SWALLOW REFLEX INITIATION Thermal stimulation …Triggers faster swallow reflex in adults …Refrigerator-chilled liquids or semisolids …May diminish over subsequent swallows If non-orally fed – may suck on frozen pacifier Thicken liquid/pureed foods Improving laryngeal closure …Forward head flexion/chin tuck …Angled bottle, cut out cup, straw

29
ASPIRATION DURING SWALLOW Usually caused by reduced or insufficient laryngeal elevation/closure and part of the bolus seeps under epiglottis into airway Treatment techniques aimed at improving laryngeal elevation and changing viscosity of bolus to minimize seep Strong forward head flexion or chin tuck – changes relative position of larynx so needs less elevation Use cut out cup or straw to assist in maintaining neck flexion; use angled bottle Thickening feedings – moves slower so more time to elevate

30
ASPIRATION AFTER THE SWALLOW Usually secondary to residue …Decreased pharyngeal peristalsis …Dysfunction of the CP muscle …Inadequate pressure gradients Noisy, wet-sounding breathing that is worse following feeding Modify food texture Encourage “dry” swallows Palatal trainer

31
DECISION-MAKING AND ASPIRATION Degree of swallowing dysfunction Amount of aspiration Response to treatment Underlying pulmonary status Tracheostomy Therapeutic feeds Full PO with modifications

32
GER Non-oral restriction decreases GER but may still have…. …Ascending aspiration …Need to increase/maintain oral skills …Provide therapeutic feeds

33
ORAL-MOTOR CONTROL Hypotonia – poor stability and abnormal control Need to ‘wake up’ or ‘alert’ CNS …Tapping …Vibration …Quick stretch Masseter and buccinator muscles Lips/tongue

34
ORAL-MOTOR CONTROL Hypertonia – abnormal movement and may lead to abnormal alignment Neurological insult or abnormality, stress …Preparatory movements Handling Body alignment …Firm pressure …Shaking/vibrating …Tongue retraction …Environmental management

35
TONGUE Neck extension – functionally pulls tongue into retracted position May be hypertonic or passively retracted May be actively seeking point of stability (micrognathia) Postural support – improve head/neck alignment Handling – normalize tone, neck/shoulders Modify tone in tongue …Finger in midline …Shaking, jiggling, tapping, stroking, vibrating Longer nipple
 Postural support – improve head/neck alignment Handling – normalize tone, neck/shoulders Modify tone in tongue …Finger in midline …Shaking, jiggling, tapping, stroking, vibrating Longer nipple")
36
TONGUE Bunched, humped, retracted, hypotonic Lacks central groove Get tongue forward Downward pressure to midline Stroking forward with downward pressure Firm straight nipple with cross-cut

37
TONGUE Tongue-tip elevation – pressed against hard palate, distal to alveolar ridge Common in preemies – may be a means of stabilization Postural support Preparatory handling Quick swiping or vibration Downward pressure Assist with mouth opening …Stimulation to lips …Downward pressure on jaw

38
TONGUE Protrusion – sits on lower lip below nipple and interferes with lip seal Hypotonia/weakness/increased tone Neck extension Postural support – neutral or slightly flexed Preparatory handling to reduce tone Sensory input – firm tapping Firm, downward pressure to midline Firm straight nipple Facilitate lip activity

39
POOR MOUTH OPENING Poor arousal Neurologic insult Prepare state Elicit rooting reflex Assist mouth opening – gentle downward pressure Inhibit jaw clenching – vibration, very small- range, low amplitude side-to-side movement Touch/pressure to gums

40
WEAK SUCK Ineffective feeding Overall weakness, medical/nutritional compromise, immaturity, myopathies, respiratory/endurance Provide oral stability – optimal positioning, firm cheek/jaw support, traction on nipple Increasing flow rate (with caution)
")
41
JAW MOVEMENT Excessive – no stable base for tongue, lip seal may be compromised Develop stable base for jaw, slightly tucked chin position, develop neck flexor musculature Preemies – often have jaw instability. Poor developed tone/bulk in oral-facial mm, minimal active neck flexion, neck hyperextension common Neurologically-based hypertonicity – poorly balanced control between opening and closing mm. May lead to strong downward thrust of jaw Neck hyperextension – could be immature development of neck flexion, abmormal mm tone or stress

42
ABNORMAL TONGUE MOVEMENT Attempts to use marked jaw depression to create negative pressure suction Postural support – neck/head alignment key. Don’t allow neck hyperextension. Head in neutral or slight flexion will provide additional positional stability to jaw. External support – firm pressure under jaw. Keep pressure distal and under mandible, proximally will be under base of tongue could interfere with sucking.

43
ABNORMAL TONGUE Increased neck flexion – if doesn’t respond well to external support, bring head into strong neck flexion. Help grade jaw movement. Continually monitor respiratory status. Handling techniques to reduce overall mm tone May need to target tongue

44
LIP SEAL Negative pressure reduced or broken intermittently Smacking/kissing, excessive fluid loss Low tone, weakness – preemies or conditions Excessive jaw movements

45
ABNORMAL TONGUE MOVEMENTS Strong protrusion – treat tongue Treat underlying problems first– facial weakness/hypotonia, excessive jaw movement External support – cheeks/lips and jaw support, too.

46
CHEEKS Hypotonia/weakness, diminished fat pads Poor stability leads to poor lip seal. Excessive jaw excursion may result Increase facial tone Cheek/jaw support

47
POOR INITIATION OF SUCKING Crying, fussing, ‘tuning out’ – baby hungry and will become increasingly frustrated May root excessively and unable to inhibit – turns head wildly from side-to-side Extreme mouth opening and unable to close Tongue protrusion/lapping pattern may be attempt as sucking Hypersensitive response or poorly developed sucking patttern Poor state/organizational abilities – overly hungry

48
POOR INITIATION Treat underlying problems – if poor state/organization treat those underlying conditions Preparatory handling Stabilize front of head with jaw control as needed Place nipple firmly at midline, cheek support as needed –for central reference point Assist with mouth closure – firm jaw control to assist with closure, grading of mouth open, vibration to relax tension and assist with closure Facilitate appropriate tongue movement

49
COORDINATION OF SSB Prolonged sucking – feeding induced apnea Having difficulty ‘pacing’ SS and B Strong, rapid sucking with difficulty initiating breathing even when nipple removed More common in preemies External pacing Be sure baby can initiate breathing May have better regulation later in feeding Decrease rate of flow – thicker liquid, slower flow – to allow time to organize

50
COORDINATION OF SSB Short sucking bursts 1-3 sucks in a burst before pausing for multiple breaths Pauses too frequent/long compared to sucking bursts May be adaptive response VFSS Look at respiratory status Endurance

51
COORDINATION OF SSB Uneven pattern with duration of bursts/pauses varying considerably May be uneven pattern of breathing and swallowing within the sucking burst. Frequent choking/coughing noted General neurological disorganization, respiratory problem, nipple flow problem Assist with external organization Understand respiratory status Pace, reduce flow rate, bolus size

52
ORAL-TACTILE HYPERSENSITIVITY Responses are exaggerated out of proportion to stimulus (e.g., placing bottle or toy in mouth) At the extreme end of hypersensitive responses Easily elicited, stronger, more negative and often include a behavioral response May cry, grimace, wiggle, arch away, keep mouth closed. If feeder persists may begin to gag and may vomit.

53
MULTIFACTORIAL CAUSE Immaturity and illness – immature CNS, at the mercy of physiologic status, poor regulatory filtering mechanisms, becomes a pattern Delayed introduction of oral feeding – critical period for acquisition of oral feeding skills may be missed (Illingworth & Lister) Unpleasant oral-tactile experiences – negative or traumatic oral-facial experiences during the course of medical treatment
 Unpleasant oral-tactile experiences – negative or traumatic oral-facial experiences during the course of medical treatment")
54
TREATMENT Adaptive, well-modulated responses is the goal. Reduce aversive stimuli – look at care routines Grade oral/tactile stimuli – start in a range where the child is comfortable and slowly build up to a point where it is not tolerated and then step back slightly. “Dance” on the edge of the infant’s tolerance. …May need to start distal and move proximal …May need to move from smooth to soft to unusual to prickly, firm to light pressure, etc.

55
VIBRATION Vibratory afferents are carried along different neural pathways than light touch and touch/pressure. More integrating and less likely to stimulate an aversive response. Can be effective even with preemies Hold vibrator against finger, nipple, pacifier. Use an electric toothbrush.

56
ORAL EXPLORATION Mouthing toys and hands is a crucial component in helping them tolerate increasing complexity and variety of oral sensations. Variety – don’t let child get ‘stuck’ on only one thing. Feeding specialist needs to reintroduce this stage of normal development in a way the baby can tolerate.

57
ENDURANCE AND RESPIRATORY COMPROMISE Need to increase ventilation and cardiac output to match ‘work’ of feeding Reduced intake, poor weight gain Generally has normal OM control and SSB Initially feeds well but stops early in feeding Regulate liquid flow – faster at beginning to get more in, softer nipple, slightly larger hole. Monitor carefully!! Manipulate feeding schedule – limit feeding time, time between feedings, demand schedule Nutritional supplements, caloric density

58
ENDURANCE AND RESPIRATORY COMPROMISE Structural abnormalities or respiratory disease = increase WOB Much of available energy is used in cardiorespiratory system with little reserve for additional activity (i.e., feeding) Increase WOB may lead to GER Treatment for endurance should be considered Reduce expectations for feeding Small volume feedings; pacing Stopping or postponing oral feeding Supplemental O2, nebulizers
 Increase WOB may lead to GER Treatment for endurance should be considered Reduce expectations for feeding Small volume feedings; pacing Stopping or postponing oral feeding Supplemental O2, nebulizers")
59
VENTILATION VERSUS PERFUSION Ventilation – amount of air in and out of lungs and alveoli Perfusion – ability of alveoli to exchange gas Supplemental O2 is not helpful in all respiratory problems – if perfusion is poor, increasing O2 amount will not improve saturation in blood May still be helpful with feeding since ventilation- perfusion ratio may change with increased work Need oximetry

60
INCREASED NUTRITIONAL REQUIREMENTS: ADDITIONAL CALORIES Skill in balancing medical and nutritional needs with parents’ skills and expectations Frequently an issue with respiratory/endurance problems OM skills generally intact so leads to optimism and enthusiastic pursuit of oral feeding Perception of failure on the part of the infant or parent if goals not readily achieved

61
INCREASED NUTRITIONAL REQUIREMENTS: ADDITIONAL CALORIES May need to change the way in which progress is measured …Primary goal should be infant’s overall growth …Oral feeding often comes at a high price …Supplemental nutrition should be viewed as support rather than last resort or failure …Provides a built-in nutritional system during setbacks …Focus on quality of oral control and parent-child interaction rather than calories …Small volume/partial oral to build motoric and sensory foundations, hunger/satiation

62
NON-ORAL FEEDING Full non-oral feeding – …Motor deficit …Extreme tactile hypersensitivity/aversion …State or arousal problems …Medical conditions that preclude oral feeding …Any combination of these Existing OM skills should be maintained for future oral feeding and speech Prevent oral aversion and hypersensitivity due to lack of oral input Facilitate oral hygiene

63
NON-ORAL WITH TX ORAL FEEDS Primarily non-oral Feeding-related functions show adequate competence to allow small amount of safe oral feeding To improve OM skills and move toward larger volumes as able. Safe for oral but cannot take full oral Allowed to feed as much as possible within certain parameters (length, frequency) with balance non- oral
 with balance non- oral.")
64
NON-ORAL PLUS ORAL Limited nippling at each feeding using good techniques and within physiologic parameters. Amount not finished is given though tube Use only with indwelling NGT or GT Often used with preemies Alternate nipple and tube feedings Should be close to taking full volume Good for those with limited endurance

65
NON-ORAL PLUS ORAL Daytime oral and nighttime tube

66
TRANSITION FROM TUBE TO ORAL Begin the process of transitioning to oral feeding at the point when non-oral feeding begins Comprehensive and aggressive oral therapy program …Normal OM skills …Expected short-term use (6-12 months) Primary objectives …Minimize negative or aversive oral stimulation …Promote pleasurable experiences and oral exploration …Maintain/build OM skills and interest …Associate oral activity with satisfaction of hunger …Maintain whatever degree of oral intake that is safe …When possible, expand rather than introduce
 Primary objectives …Minimize negative or aversive oral stimulation …Promote pleasurable experiences and oral exploration …Maintain/build OM skills and interest …Associate oral activity with satisfaction of hunger …Maintain whatever degree of oral intake that is safe …When possible, expand rather than introduce")
67
TRANSITION Consistency, whatever program is established, is essential Assess child and parents’ readiness Often lengthy and difficult; it’s a process …“He will eat when he’s hungry” does not apply …Set goals that reflect steps rather than final outcome Establishing level and quality of OM skills Determine swallowing ability What’s the original medical condition? What’s the current status?

68
LETTING GO Degree of OM impairment Lack of change/improvement in medical status Move away from oral goal in a way that supports the child and family Quality of life …‘Recreational’ oral feeding …Tolerates oral stimulation for ongoing hygiene to face, mouth, teeth, gums

69
DESENSITIZATION HIERARCHY From 18 months and older No obvious OM deficits May have oral sensory problems due to sensory deprivation Tolerating – …Be in same room …Looking at food Interacting – …Uses utensils in play, preparation

70
DESENSITIZATION HIERARCHY Smelling …Tolerates odor of food Touching …Tolerates on fingers, hand, upper body, chin/cheek, nose, lips, teeth and tongue Tasting …Licks lips or tongue …Bites and spits out …Bites and holds in mouth before spitting out …Chews and partially swallows …Chews/swallows with drink …Chews/swallows independently

71
DESENSITIZATION HIERARCHY Eating Gradual changes that lead the child to functional eating without any specific intervention by others except expected monitoring for age Individual variation as needed …Collaboration with MD, RD, daycare, school or other therapists, with caregivers and child as primary team members! …Consistent approach and encouragement/feedback

72
MEALTIME ENVIRONMENTS Home, daycare, school, restaurant …Modify environment as best you can …Placemats, utensils, cups, bowls …Proud plates, brag books Adaptive seating …Lightweight, washable, easy to use …Fits under table to allow child to be included in mealtime

73
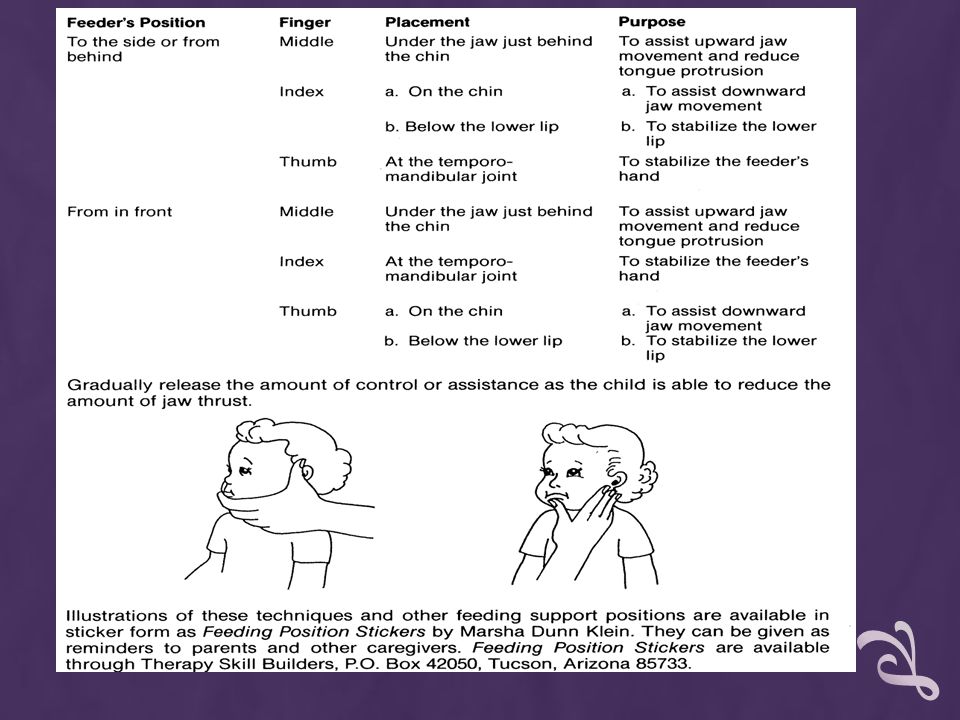
ORAL CONTROL – FROM SIDE OR BEHIND First do positioning for best posture Middle finger …Behind chin on belly of tongue …Inhibits jaw opening, helps closing, indirectly inhibits tongue protrusion Index finger …Between lower lip and chin …Facilitates graded jaw opening, helps control head Thumb …Under chin, provides jaw stability only

74
ORAL CONTROL – FROM FRONT Helps maintain eye contact Requires more control from the child Index or middle finger …Under chin …Provides jaw stabilization Thumb …On chin …Facilitates graded jaw opening

75
TOLERATING FACE WASHING Preparation for mealtime/snack activity and at end of meal/snack Provide postural support and stability Provide oral control as needed Use firm, deep pats moving distal to proximal …Cheek bones to lips, one side then the other, upper lip stretching downward, chin moving upward Use different textured cloths Use rhythm/singsong

76
SPOON FEEDING Wash your hands and help child wash theirs Provide postural support and stability Begin with jaw closed Spoon approaches from low to midline Graded jaw opening – support as needed Put spoon straight in – about half way Press down and flat on tongue, hold to allow tongue to quiet and lips to close. Take spoon straight out Let upper lip learn to be active so don’t scrape against the lip

77
SPOON FEEDING Clamping – provide extra flexion and wait for child to relax Sensitivity – face washing and tooth brushing Lip retraction – positioning toward midline Tongue thrust before swallow – better head/neck control and oral control No swallow – chin tuck/neck elongation, reload spoon and come towards them

78
CHEWING Wash your hands and help child wash theirs Provide postural support and stability Provide oral control Begin with jaw closed Food approaches from midline and low or level with mouth. Use food that is easy to handle Graded jaw opening while maintaining flexion Place food on chewing surface of teeth at side Facilitate graded jaw closure Maintain oral control; watch head and trunk Don’t facilitate chewing motion – wait with continuous oral control

79
CHEWING Tone in cheeks – use finger to stretch and release cheeks before starting Poor lip closure – face wipe to stretch upper lip down, lower lip up. Push jaw up. Exaggerated jaw movement – use oral control to grade jaw

80
CUP DRINKING In typically developing children, spoon feeding builds to cup drinking Wash your hands and help child wash theirs Provide postural support and stability Provide oral control Thicker liquids are easier to control in the beginning Begin with jaw/lip closure Approach at midline or slightly below level of the mouth Place cup between lips – not between teeth

81
CUP DRINKING Rest rim on but do not push down on lower lip Tilt cup until it touches upper lip and wait Goal is active downward motion of upper lip to draw in liquid Don’t remove cup unless child pulls away – watch child’s signals Maintain oral control

82
CUP DRINKING Bite reflex – move out so it doesn’t happen Gulping – prevent with slight chin tuck/neck elongation so the kid is looking down in the cup Use thicker liquids, cut out cup, clear cup, let child help “hold” the cup

83
STRAW Prerequisites: nasal breathing, lip seal with active lip function, light jaw closure, cheek and tongue movement to build up negative pressure Wash, provide posture support and stability, provide oral control Dip straw into liquid and place finger over hole on top Place straw between lips, let a drop of liquid out and wait for active suck Gradually require more suction by keeping finger over hole Short, wide and small diameter straws Use juice box

84
BOTTLE FEEDING Need NNS to serve as a link that will facilitate transition to NS Wash hands, provide posture support and stability Provide oral control from the front – tongue control with middle finger, thumb and index finger on cheek to provide movement forward to facilitate sucking Bottle approach from midline or below Facilitate graded jaw opening Pressure on tongue with nipple to stimulate suck Rock or shake nipple may help if has intermittent suck

85
SELF-FEEDING Wash, provide posture support and stability Provide oral control if it has not been discontinued prior to this stage Begin with finger foods to eliminate use of utensils Hand-over-hand or child holding on to your fingers as you hold the food or spoon Food or spoon at midline on table. Gather food on spoon. Jaw is closed. Food or spoon at midline.

86
SELF FEEDING Spoon straight in, maybe pressing down on tongue for stability/organization Spoon straight out, maybe pausing to let lips and jaw close May need slight chin tuck/neck elongation to prevent biting on spoon Spoon back to plate/bowl Finger foods follow the same pattern but are presented laterally to facilitate chewing

87
QUALITIES OF UTENSILS Spoons – …size of bowl …depth of bowl …Size and weight of handle Cups – …size …height/width …cut out cup – see liquid, to prevent hyperextension …Cup lip …Flexibility …Handles or no handles

88
QUALITIES OF UTENSILS Finger foods …Shape …Texture …Way to make it graspable

89
TREATMENT IDEAS You set the stage – playful, fun, positive and calm Activities with no food …Touch/pressure to hands/feet (weight bearing, holding, deep pressure) …Massage and vibration – Begin distal and move proximal …Play with cups, utensils, dolls, tooth brushes, etc. …Rhythm, bouncing, patting, stroking …Sensory – lentils, corn meal, rice, play doh, damp sand, damp sponge, finger paints

90
TREATMENT IDEAS Food activities – play – explore, measure, pour, art, put food on toy, put toy in mouth, drive food in cars, peanut butter play doh, etc. Help prepare food – buy it, stir, grind, pass it, feed you, join the family at meal times, wash dishes Many short work periods better than one long one Once a week with family follow through Carryover to home

91
TOOTHBRUSHING Goals: …To improve oral hygiene …Reduce limiting movement patterns …Normalize response to sensory stimulation Procedure (may vary per child) …Introduce activities with fingers or toys – touch, taste, movement in mouth that is enjoyable …Explore and play with toothbrush, NUK …Provide sensory input with fingers – proceed slowly and systematically within child’s tolerance level
 …Introduce activities with fingers or toys – touch, taste, movement in mouth that is enjoyable …Explore and play with toothbrush, NUK …Provide sensory input with fingers – proceed slowly and systematically within child’s tolerance level")
92
TOOTHBRUSHING Procedure …Use small sponge, washcloth, NUK …Brush all parts of the mouth – tongue, lips, cheeks, gums. Brush sides of tongue to encourage lateralization …Introduce taste on finger, cloths, toothbrushes …When able to tolerate oral stimulation, brushing movements and taste in mouth, introduce small amounts of toothpaste …Use a basting syringe to squirt water in mouth and have child lean forward to let water fall from mouth

93
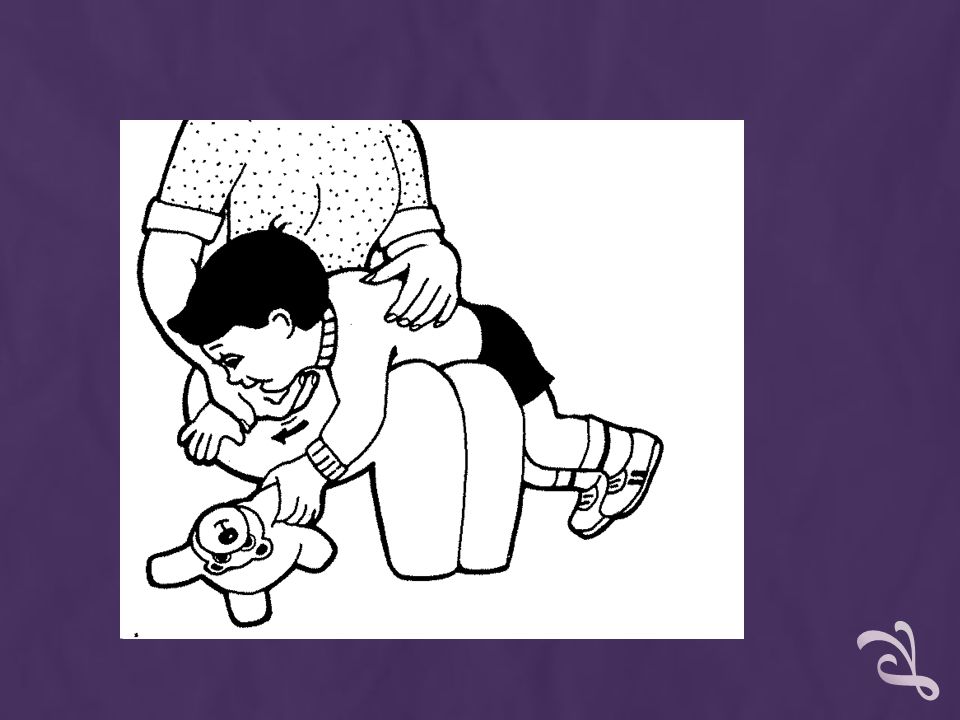
JAW THRUST Sitting posture Reduce sensory input that might overload the child Position prone on your lap or over a bolster with arms forward. Shoulders should be higher than hips. Let gravity help the tongue and jaw to drop into a more forward position. Reduce hypersensitivity caused by teeth contacting spoon, toy, finger. Carefully graded pressure to face, gums and teeth Jaw control and closure Toothbrushing to normalize sensory stimulation

94
JAW CLENCHING/TOOTH GRINDING Postural control to eliminate instability Position prone on lap/bolster with shoulders higher than hips. Gravity will pull jaw into more open position Build postural control to develop proximal stability. Reduce hypersensitivity – pressure to face, gums, teeth Toothbrushing Help child explore mouth movements and sensations so they don’t get ‘stuck’ with clenching What is child communicating by clenching/grinding?

95
JAW RETRACTION Better sitting posture Reduce sensory input that might overload child Position prone on lap/bolster and use gravity

96
JAW INSTABILITY Build postural tone in trunk to build proximal stability Play games that allow tapping, stroking and other tactile input to TMJ Support jaw with hands Have child hold on to the edge of a cup with the teeth while drinking. Utilizes normal developmental strategy

97
TONIC BITE REFLEX Posture Sensory overload Graded pressure to face, gums, teeth Toothbrushing Reduce frequency of elicitation – use a clear rhythm when feeding so mouth is more open, place cup on lower lip so cannot bite to stabilize, use a coated spoon

98
TONGUE RETRACTION Use physical handling to build tone in trunk, shoulders and neck to provide proximal stability Prone on lap/bolster With child prone, stimulate lips, move into mouth, stroke tongue Keep head in chin-tucked position with neck elongated. Tap upward on chin at base of tongue

99
EXAGGERATED TONGUE PROTRUSION AND TONGUE THRUST Exaggerated tongue protrusion – maintains easy flow of movement seen in normal suckle pattern but protrusive movement is exaggerated and moves beyond the border of the gums/lips Tongue thrust – forceful protrusion of the tongue from the mouth. Stronger than tongue protrusion and can break a previously sustained rhythm Physical handling to build tone in trunk and proximal stability Sitting posture Change food consistency so tongue protrusion is not needed to move it backward (e.g., no up-down movement for sucking or chewing, no lateralization)
.")
100
EXAGGERATED TONGUE PROTRUSION AND TONGUE THRUST Place hand on jaw to keep tongue in mouth Initiation of suckling or suck pattern from the lips rather than the tongue – use thickened liquids, pureed foods, cup with wide mouth, jaw support Place spoon in child’s mouth and press down on the middle of the tongue. Remove the spoon and encourage lip closure

101
LIP RETRACTION AND PURSING Better sitting posture Reduce sensory input Look at sensory properties of food Create a relaxed environment so child can use more mature feeding patterns without effort Reduce hypertonicity in neck and shoulder girdle – scissor-fashion on cheek Place fingers on side of child’s nose and vibrate downward to bottom of upper lip Face wiping

102
LOW TONE IN CHEEKS/LIMITED UPPER LIP MOVEMENT Physical handling to build tone in trunk and proximal stability Patting, tapping, stroking, etc. on cheeks and lips Increase sensory input to lips/cheeks through play, food selection (spicy, tart, sour, ice) Teach straw drinking while helping child to close lips
 Teach straw drinking while helping child to close lips.")
103
HYPERREACTION Consult medical personnel to rule out/discus neurological dysfunction Better posture Reduce sensory information overload Use firm pressure with finger, toy, spoon while slowly moving back in mouth to the point of gag Jaw control techniques to limit exaggerated movement

104
HYPOREACTION Consult medical personnel to rule out/discus neurological dysfunction Build posture tone in trunk and proximal stability Select type, intensity and frequency of sensory stimulation

105
SENSORY DEFENSIVENESS Child has stronger reactions to a specific sensation than would be expected Introduce slow vestibular stimulation to help child integrate multiple sensory information Use music to organize and integrate sensory reactions Use appropriate touch especially to mouth Verbally prepare child (“Here it comes!”) toothbrushin
 toothbrushin")
106
SENSORY OVERLOAD Modify space – reduce clutter, dim lights, quiet, soft music Explore graded touch Use music to help organize and integrate sensory reactions

107
SUCKING/SUCKLING Better feeding position Reduce sensory input that overloads child Prone on lap or bolster using angled bottle Help with jaw support Music with regular rhythm and 60 bpm Use binky trainer to control liquid flow

108
TRANSITION FROM SUCKLE TO SUCK Develop activity in cheeks and upper lip – easier to teach using a spoon blenderized foods Use a cup with thick liquid. Provide jaw/cheek support resting cup on lower lip. When given jaw/cheek support, a more mature up-down suck pattern often will emerge. Sucking pattern should be initiated from the lips rather than from the tongue.

109
DROOLING Inadequate head/trunk control to support efficient swallow Decreased saliva control with motor demands Teething Poor jaw stability Nasal congestion Reduced sensory cues to face Attention or power Cranial nerve dysfunction Side-effect of medication or allergic reaction Sweet foods

110
DROOLING Improve head and neck control Improve sensory awareness in face and within mouth. Increase awareness of wetness and dryness Improve jaw, lip and cheek control Emphasize and value dryness Teach straw drinking to improve cheek/lip control

111
TANTRUMS Serve foods that are appropriate to sensory characteristics and motor requirements of the child Explore child’s communication patterns Explore your reactions to child’s tantrum and eliminate power contest Remain neutral and limit feeding time, depending on abilities Serve appropriate portion sizes Say nothing and walk out of the room, or remove child from room Offer food only at regularly scheduled meals/snacks

112
DIAGNOSTIC TESTS/PROCEDURES Basic understanding of common tests regardless of professional practice setting. Strengths/limitations Implications of results Integrate data into clinical feeding observation Is additional information needed? Most developed for adults; lack of normative data with children (manometry, FEES, scintigraphy)
.")
113
PHYSIOLOGICAL MONITORING Heart rate, respiratory rate, oxygen saturation Cardiorespiratory monitor …Numerical and visual display of heartbeat and respiration …Averaged over a given period of time (e.g., 10 secs …Strengths – quick approximation of infant’s status. …Movement artifact /not always accurate

114
PHYSIOLOGICAL MONITORING Oximetry – …Oxygen saturation of capillary blood flow through an external sensor. …Expressed as a percentage of 100. Normal infant -- sats above 95% Below 90% generally indicate some degree of hypoxia. …Baseline, changes in response to work/handling, effectiveness of O2 treatment

115
PHYSIOLOGICAL MONITORING Strengths – …Easy to transport, non-invasive …Ongoing, instantaneous info …More reliable index than observation Limitations – …Very sensitive to movement …Natural pigment of baby …Ambient light/infrared heating sources

116
PHYSIOLOGICAL MONITORING Pneumogram – …Two-channel study based on chest wall excursion and heart rate …Computerized –multichannel recording of parameters such as heart rate, RR, O2 sats, nasal airflow, esophageal pressures …Gives exact values rather than averaged values so subtle changes in parameters are identified.

117
PHYSIOLOGICAL MONITORS Polysomnogram – “Sleep study” …Multichannel recording of respiration, airflow, chest and diaphragm movement, oxygen and carbon dioxide levels, heart rate and esophageal pressures …EEG recordings for length of two complete sleep cycles …Measures the greatest number of variables …Differentiates between central and obstructive apnea, apnea secondary to seizures, obstructive apnea due to GER or airway collapse …Limitations – specialized sleep lab, expertise

118
GASTROINTESTINAL Technetium scan (AKA GE scintigraphy or a milk scan) …Small amount of radionuclide isotope is added to the feeding …Images are made every 30 seconds over a one hour period after the feeding looking for material in the esophagus. …Number/height of reflux episodes calculated and compared with standards …Gastric emptying computed by measuring the percentage of food remaining within the stomach after on hour.

119
GASTROINTESTINAL Strength …Info on several important parameters of GER: Acidity/alkaline reflux …Unlikely to miss reflux events …Height of reflux in esophagus …Contribution of delayed gastric emptying …Radioactive tracer not absorbed and total radiation exposure is low Criticized …Overly sensitive to reflux …High false positive rate

120
GASTROESOPHAGEAL Barium swallow (AKA esophogram or upper GI) …Evaluates structure and function of esophagus and stomach …Ba delivered either orally or NG tube …Fluoroscopy – real-time events observed …Still photos taken for later review …Esophageal motility can be evaluated …Presence of spontaneous reflux or attempt to elicit by giving pressure to abdomen …Rad exposure is proportional to time of exposure, but generally brief …Not sensitive enough to GER, may detect aspiration
 …Evaluates structure and function of esophagus and stomach …Ba delivered either orally or NG tube …Fluoroscopy – real-time events observed …Still photos taken for later review …Esophageal motility can be evaluated …Presence of spontaneous reflux or attempt to elicit by giving pressure to abdomen …Rad exposure is proportional to time of exposure, but generally brief …Not sensitive enough to GER, may detect aspiration")
121
UGI From Wolf & Glass, 1992

122
GASTROINTESTINAL pH probe –GER …Sensor inserted through nose to an area just above LES to continuously measure acidity of esophagus …At least a 24 hour hospital stay …Record kept at beside of baby’s activities for later correlation with changes in pH. Data is recorded on the total number of episodes of pH <4.0, total time with pH<4.0, number of episodes greater than 5 mins, and longest episode of pH<4.0. Typically, episodes of pH<4.0 must last longer than 10 secs to be recorded.

123
GASTROINTESTINAL pH probe –GER …Sensor inserted through nose to an area just above LES to continuously measure acidity of esophagus …At least a 24 hour hospital stay …Record kept at beside of baby’s activities for later correlation with changes in pH. Data is recorded on the total number of episodes of pH <4.0, total time with pH<4.0, number of episodes greater than 5 mins, and longest episode of pH<4.0. Typically, episodes of pH<4.0 must last longer than 10 secs to be recorded

124
GASTROESOPHAGEAL Data generates a reflux score ‘Gold standard’ for evaluation of GER

125
AIRWAY/GASTROINTESTINAL Pediatric Endoscopy …Esophagoscopy/esophageal manometry, laryngoscopy, bronchoscopy Rigid or flexible tube Directly observes structures within the body Obtain tissue via biosy or aspiration Treatment Advances in fiberoptics permitted flexible endoscopes that can be used with even extremely small infants

126
VIDEOFLUOROSCOPIC SWALLOWING STUDY (VFSS) VFSS aka MBS …Specifically designed to assess the pharyngeal swallow …Normal feeding situation is simulated but may need to use ‘tricks’ …Purpose –document aspiration, reason for aspiration and the point at which it occurs …Assess possible therapeutic interventions …Positioning can be customized
 VFSS aka MBS …Specifically designed to assess the pharyngeal swallow …Normal feeding situation is simulated but may need to use ‘tricks’ …Purpose –document aspiration, reason for aspiration and the point at which it occurs …Assess possible therapeutic interventions …Positioning can be customized")
127
VFSS From Wolf & Glass, 1992

128
CFE LIMITATIONS Info not readily obtained at bedside: …VP function …Laryngeal elevation and closure …Pharyngeal motility, transit time …Pooling of secretions and contrast in valleculae and pyriform …Number of swallows to clear material …Presence and timing of aspiration in relation to the swallow. …Bolus movement through UES and esophagus

129
VFSS SLP/MD …Observations relating to timing of swallow …Coordination in oral/pharyngeal phase …Phary peristalsis …Pooled material prior to swallow or residue after …Esophageal transit time …Aspiration before, during, after swallow

130
VFSS Seating/postioning – …Support of trunk, neck and head …Semireclining angle of approx 45 degrees. …Tumbleform chair …Child’s own seating system …Most wheelchairs don’t fit; some have removable parts …Height of seat in relation to floor

131
VFSS Need careful guidelines for appropriate …Radiologic risks to infant versus the yield of info from the test …How will information be used? Personnel involved varies – …OT, SLP, MD, tech …Regardless, should have expertise in infant and skill in interpreting images Parent participation

132
VFSS Emergency back up equip and personnel as needed Flexible enough protocol to address each baby’s needs Endurance

133
VFSS -- FEEDING TECHNIQUE Multiple variables …Nipple, syringe, nipple alternating with pacifier to look at NNS and NS, spoon, cup, straw, liquid thickness, solids Bolus type, amount, texture, temperature, timing can be varied Risk of aspiration kept at minimum Caregivers provide samples of food …Regularly given …Causing trouble …Introduction Lateral view -- most important and most information

134
VFSS AP view— …Documenting asymmetry/pooling …Head positions Therapeutic changes Flexed, extended, turned, etc. Neurologically impaired …Better at handling homogeneous consistency

135
VFSS Alternate feeding methods with plans for oral-motor stimulation Repeat studies: …Significant change in medical or neurological status …Recurrence of previous symptoms …Previous documentation of silent aspiration …Tx program changes are indicated for diet textures or compensation techniques Improved oral-motor function in profoundly neurologically impaired children have not shown to be directly correlated with improved pharyngeal transit time.

136
VFSS -- LIMITATIONS Lack of standardization – …Positioning …Amount and order of presentation …Therapeutic modifications …Overly sensitive

137
VFSS VS CLINICAL FEEDING EVALUATION (CFE) Benefits of CFE first – …Establish baseline behaviors to compare with feeding during VFSS. …Feeding during VFSS is often not representative Paradoxical performance Has significant feeding d/o but swallows Ba without difficulty Pre-determine types/textures of foods, order of presentation, optimal positioning, equipment needed Able to formulate and test treatment strategies

138
VFSS Confirms need for VFSS …Radiation exposure Signs during CFE …Coughing/choking …Noisy, wet respirations …Subtle signs –unexplained respiratory infection or illness, difficulty managing oral secretions. Aspiration can be silent …Logemann reports 40% of adult patients who asp during VFSS not identified during bedside

139
VFSS Pay particular attention to medical history, parent descript of feeding, subtle indicators of potential swallow dysfunction Generalizability of feeding sample has been questioned …Relatively brief sampling …Ba may alter baby’s swallowing response Not intended to identify GER as objective, but can be seen

Similar presentations





 …Poor weight gain/growth failure …Below 3 rd – 5 th percentile …No gain for three consecutive months.>")














