Download presentation
Presentation is loading. Please wait.

1
Surgical Management of Bisphosphonate Related Osteonecrosis of the Jaw By David Telles, DDS Diplomate of the American Board of Oral and Maxillofacial Surgeons

2
Overview Background Review of AAOMS Position Paper ▫Oral vs IV Bisphosphonate Therapy ▫Recommendations ▫Staging Surgical Management Review Conclusions

3
Background The rise in bisphosphonate treatment of degenerative osseous diseases is accompanied by a proportional increase in the number of reported cases of bisphosphonate related osteonecrosis of the jaw (BRONJ precipitated by surgical procedures and may occur spontaneously (Marx et al.) presentation of this pathology varies by route of administration ▫Ruggiero 7 et al. demonstrated a more aggressive clinical course in cases of intravenous administration in contrast to administration per os (po). ▫correlated with a potential difference in the relative potency of the different drug forms, the intravenous suspension being more potent ▫intravenous form is more efficacious, the relative ease of administration in oral form translates into a greater prevalence of this drug among patients. As the use of bisphosphonates increases, dental practitioners are encountering BRONJ more often. Typical clinical ▫exposed bone or dehisced tissue with or without pain and swelling ▫untreated cases -- sites of osteonecrosis can progress into orocutaneous fistulas which may become secondarily infected.
. ▫correlated with a potential difference in the relative potency of the different drug forms, the intravenous suspension being more potent ▫intravenous form is more efficacious, the relative ease of administration in oral form translates into a greater prevalence of this drug among patients. As the use of bisphosphonates increases, dental practitioners are encountering BRONJ more often. Typical clinical ▫exposed bone or dehisced tissue with or without pain and swelling ▫untreated cases -- sites of osteonecrosis can progress into orocutaneous fistulas which may become secondarily infected..")
4
Background Dentists must determine how to treat BRONJ without further challenging the compromised bone Treatment modalities ▫conservative measures, such as antibiotics and antimicrobial rinses ▫superficial debridement ▫sequestrectomy ▫resection of the involved bone

5
Background Uses of bisphosphonates ▫ Inhibition of bone resorption ▫ Osteolytic disease (Paget’s, Multiple Myeloma) ▫ Metastatic bone disease ▫ Hypercalcemia associated with malignancy ▫ Osteoporosis ▫ Anti-tumor activity (Rosen, Theriault et.al. 2001) Mechanism of Action ▫ Effects on osteoclasts- Precursor cells, cytoskeleton, apoptosis 4 (Hughes et.al. 1995) ▫ Anti-angiogenesis - Zometa study 8 ▫known that they inhibit osteoclastic function, increase osteoclast apoptosis, inhibit osteoclast differentiation, and stimulate osteoclast inhibitory factor, all of which may lead to inhibition of bone resorption and increase in bone mass (Curi M et. al.)
 Mechanism of Action ▫ Effects on osteoclasts- Precursor cells, cytoskeleton, apoptosis 4 (Hughes et.al. 1995) ▫ Anti-angiogenesis - Zometa study 8 ▫known that they inhibit osteoclastic function, increase osteoclast apoptosis, inhibit osteoclast differentiation, and stimulate osteoclast inhibitory factor, all of which may lead to inhibition of bone resorption and increase in bone mass (Curi M et. al.).")
6
IV vs Oral Ruggiero et. al. (2004) study - 63 cases oral osteonecrosis (56 on IV treatment, 7 on oral treatment) Association between IV bisphosphonate exposure and BRONJ may be hypothesized based on the following observations ▫1) a positive correlation between bisphosphonate potency and risk for developing BRONJ ▫2) a negative correlation between bisphosphonate potency and duration of bisphosphonate exposure prior to developing BRONJ ▫3) a positive correlation between duration of bisphosphonate exposure and developing BRONJ.
 study - 63 cases oral osteonecrosis (56 on IV treatment, 7 on oral treatment) Association between IV bisphosphonate exposure and BRONJ may be hypothesized based on the following observations ▫1) a positive correlation between bisphosphonate potency and risk for developing BRONJ ▫2) a negative correlation between bisphosphonate potency and duration of bisphosphonate exposure prior to developing BRONJ ▫3) a positive correlation between duration of bisphosphonate exposure and developing BRONJ..")
7
IV vs Oral Incidence ▫IV bisphosphonates and incidence of BRONJ clinical efficacy of IV bisphosphonates for the treatment of hypercalcemia and bone metastases is well established exposure in the setting of managing malignancy remains the major risk factor for BRONJ Based on case series, case-controlled and cohort studies, estimates of the cumulative incidence of BRONJ range from 0.8%-12% (AAOMS Position paper)
")
8
IV vs Oral Incidence: Oral ▫over 190 million oral bisphosphonate prescriptions have been dispensed worldwide. ▫several BRONJ cases related to oral bisphosphonates ▫Patients under treatment with oral bisphosphonate therapy are at a considerably lower risk for BRONJ than cancer patients treated with monthly IV bisphosphonates ▫Data from the manufacturer of alendronate (Merck), the incidence of BRONJ was calculated to be 0.7/100,000 person/years of exposure
, the incidence of BRONJ was calculated to be 0.7/100,000 person/years of exposure.")
9
IV vs Oral Incidence: Oral ▫Surveillance data from Australia estimated the incidence of BRONJ for patients treated weekly with alendronate as 0.01-0.04%. ▫In a survey study of over 13, 000 Kaiser- Permanente members, the prevalence of BRONJ in patients receiving long-term oral bisphosphonate therapy was reported at 0.06% (1:1,700). ▫When PO given > 3 yrs – correlation to increased risk for developing BRONJ
. ▫When PO given > 3 yrs – correlation to increased risk for developing BRONJ.")
10
Risk Factors Systemic FactorsLocal Factors -Potency of bisphosphonate -Length of bisphosphonate treatment -Race (usually Caucasians) -Age (usually >60) -Primary disease multiple myeloma >breast CA>other CA -Misc-steroid treatment, diabetes, smoking, alcohol, poor oral hygiene, concurrent chemo therapy -Recent history of invasive dental surgery (dentoalveolar surgery i.e. exodontias, implants, periodontal surgery is 7x more likely to develop BRONJ) -Anatomy – tori, mylohyoid ridge, palatal tori -Concomitant oral disease – periodontal and dental abscesses are at a 7x increase for BRONJ
 -Anatomy – tori, mylohyoid ridge, palatal tori -Concomitant oral disease – periodontal and dental abscesses are at a 7x increase for BRONJ.")
11
BRONJ Case Definition ▫Current or previous treatment with a bisphosphonate ▫Exposed bone in the maxillofacial region that has persisted for more than eight weeks ▫No history of radiation therapy to the jaws

12
Staging Stage 0 ▫Symptoms odontalgia not explained by an odontogenic cause dull, aching bone pain in the body of the mandible, which may radiate to the temporomandibular joint region sinus pain, which may be associated with inflammation and thickening of the maxillary sinus wall altered neurosensory function ▫Clinical Findings loosening of teeth not explained by chronic periodontal disease periapical/periodontal fistula that is not associated with pulpal necrosis due to caries ▫Radiographic Findings alveolar bone loss or resorption not attributable to chronic periodontal disease changes to trabecular pattern—dense woven bone and persistence of unremodeled bone in extraction sockets thickening/obscuring of periodontal ligament (thickening of the lamina dura and decreased size of the periodontal ligament space) inferior alveolar canal narrowing
 inferior alveolar canal narrowing")
13
Staging and Treatment strategies Clinical Staging of BRONJTreatment Stage 0: No exposed bone but history of oral/IV bisphosphonate treatment Perceived risk, but no treatment necessary Encourage oral hygiene, preventive strategies Stage 1: exposed/necrotic bone in patients who have no infection/ no pain Chlorhexidine gluconate, encourage oral hygiene, no surgery Stage 2: exposed bone in patients with pain and evidence of infection Chlorhexidine gluconate, antimicrobial therapy with cultures taken to determine if actinomyces species present Stage 3:exposed bone in patients with pain and infection, and one or more of the following: pathologic fracture, extraoral fistula or osteolysis extending to the inferior border, exposed necrotic bone extending beyond the region of alveolar bone, i.e., inferior border and ramus in the mandible, maxillary sinus and zygoma in the maxilla, oral antral/oral nasal communication Surgical debridement/resection in combination with antibiotics, removal of mobile segments of sequestrum -If pathologic fracture present, pt may require removal of compromised bone and reconstruction (vascularized fibular flap, Engroff et al)
")
14
Treatment cond.. Regardless of the disease stage, mobile segments of bony sequestrum should be removed without exposing uninvolved bone ▫extraction of symptomatic teeth within exposed, necrotic bone should be considered since it is unlikely that the extraction will exacerbate the established necrotic process. Discontinuation of bisphosphonate therapy ▫IV bisphosphonates Discontinuation of IV bisphosphonates offers no short-term benefit if systemic conditions permit, long-term discontinuation may be beneficial stabilizing established sites of BRONJ reducing the risk of new site development and reducing clinical symptoms risks and benefits of continuing bisphosphonate therapy should be made only by the treating oncologist in consultation with the OMS and the patient. ▫Oral bisphosphonates Discontinuation of oral bisphosphonate therapy in patients with BRONJ has been associated with gradual improvement in clinical disease. Discontinuation for 6-12 months may result in either spontaneous sequestration or resolution following debridement surgery

15
Literature review Treatment options ▫Conservative treatment Long term Abx Chlorhexidine gluconate 0.12% rinse bid ▫Sequestrectomy/Surgical Debridement ▫Resection ▫Drug holidays ▫HBO therapy ▫PRP Supplementation

16
Literature review - Curri M et al Treatment of Avascular Osteonecrosis of the Mandible in Cancer Patients With a History of Bisphosphonate Therapy by Combining Bone Resection and Autologous Platelet-Rich Plasma: Report of 3 Cases ▫Case series of 3 cases and lit review ▫Outline refractory cases of BROJN requiring resection ▫Tx comprised of surigcal debridement/sequestrectomy supplemented with PRP ▫3 cases resolved without further bony exposures ▫PRP – factors Plateletderived growth factor (PDGF) Transforming growth factor- (TGF-) vascular endothelial growth factor epidermal growth factor …..can induce paracrine effects on stimulated cells Several studies reported a positive effect in bone regeneration and soft tissue healing when PRP was applied in oral and maxillofacial reconstructive surgeries, cosmetic surgeries, periodontal and peri-implant defects
 Transforming growth factor- (TGF-) vascular endothelial growth factor epidermal growth factor …..can induce paracrine effects on stimulated cells Several studies reported a positive effect in bone regeneration and soft tissue healing when PRP was applied in oral and maxillofacial reconstructive surgeries, cosmetic surgeries, periodontal and peri-implant defects")
17
Literature review – Carlson E et. al. Role of Surgical Resection in the Management of Bisphosphonate-Related Osteonecrosis of the Jaws 103 sites of BRONJ in 82 patients ▫32 maxilla and 71 mandible ▫30 were taking an oral bisphosphonate and 52 taking parenteral bisphosphonate Resection performed in 95 sites in 74 patients, whereas 8 sites diagnosed in 8 patients were not resected 27 sites resected in patients treated with oral bisphosphonates 68 sites resected in patients treated with parenteral bisphosphonates

18
Literature review – Carlson E et. al. Role of Surgical Resection in the Management of Bisphosphonate-Related Osteonecrosis of the Jaws ▫95 resected sites, 87 (91.6%) healed in an acceptable fashion with resolution of disease. ▫27 resected sites in patients taking an oral bisphosphonate medication, 26 (96.3%) healed satisfactorily refractory disease developing in 1 site ▫Of 68 resected sites in patients taking a parenteral bisphosphonate medication, 61 (89.7%) healed satisfactorily refractory disease developing in 7 sites ▫All 29 patients(100%) undergoing resection of the maxilla related to either an oral or parenteral bisphosphonate healed acceptably ▫Refractory cases: 8 patients -- did so with a range of 7 to 250 days postoperatively (mean, 73 days). 6 developed after a marginal resection of the mandible for BRONJ Three sites = new primary disease developed in 2 patients postoperatively -- Both were taking parenteral BP ▫Histologic examination of the resected specimens identified malignant disease in 4 specimens in 3 patients
 healed in an acceptable fashion with resolution of disease. ▫27 resected sites in patients taking an oral bisphosphonate medication, 26 (96.3%) healed satisfactorily refractory disease developing in 1 site ▫Of 68 resected sites in patients taking a parenteral bisphosphonate medication, 61 (89.7%) healed satisfactorily refractory disease developing in 7 sites ▫All 29 patients(100%) undergoing resection of the maxilla related to either an oral or parenteral bisphosphonate healed acceptably ▫Refractory cases: 8 patients -- did so with a range of 7 to 250 days postoperatively (mean, 73 days). 6 developed after a marginal resection of the mandible for BRONJ Three sites = new primary disease developed in 2 patients postoperatively -- Both were taking parenteral BP ▫Histologic examination of the resected specimens identified malignant disease in 4 specimens in 3 patients.")
19
Literature review – Carlson E et. al. Role of Surgical Resection in the Management of Bisphosphonate-Related Osteonecrosis of the Jaws Resection of BRONJ permits acceptable healing in patients taking an oral bisphosphonate medication Resection of maxilla in patients taking an oral or parenteral bisphosphonate medication follows a predictable course with regard to healing Resection of mandible in patients taking a parenteral bisphosphonate medication follows a variable postoperative course ▫Although a high degree of success is realized Consider resection of necrotic bone of the maxilla and mandible that develops in patients taking bisphosphonate medications. Refractory disease ▫successfully managed with a more aggressive resection, specifically, a segmental resection of the mandible after a marginal resection of the mandible where refractory disease developed

20
Literature Review – Marx et al Oral Bisphosphonate-Induced Osteonecrosis: Risk Factors, Prediction of Risk Using Serum CTX Testing, Prevention and Treatment ▫CTX (C-terminal telopeptide) - a breakdown product of bone resorption - used pre-operatively as a determinant for BRONJ - inverse relationship between the risk for BRONJ and the level of CTX - less than 100pg/mL pose a high risk - between 100 and 150 are at moderate risk - over 150 are minimal risk. ▫With cessation of the drug, values increased an average of 25.9 pg/mL per month, therefore justifying the implementation of a drug holiday.

21
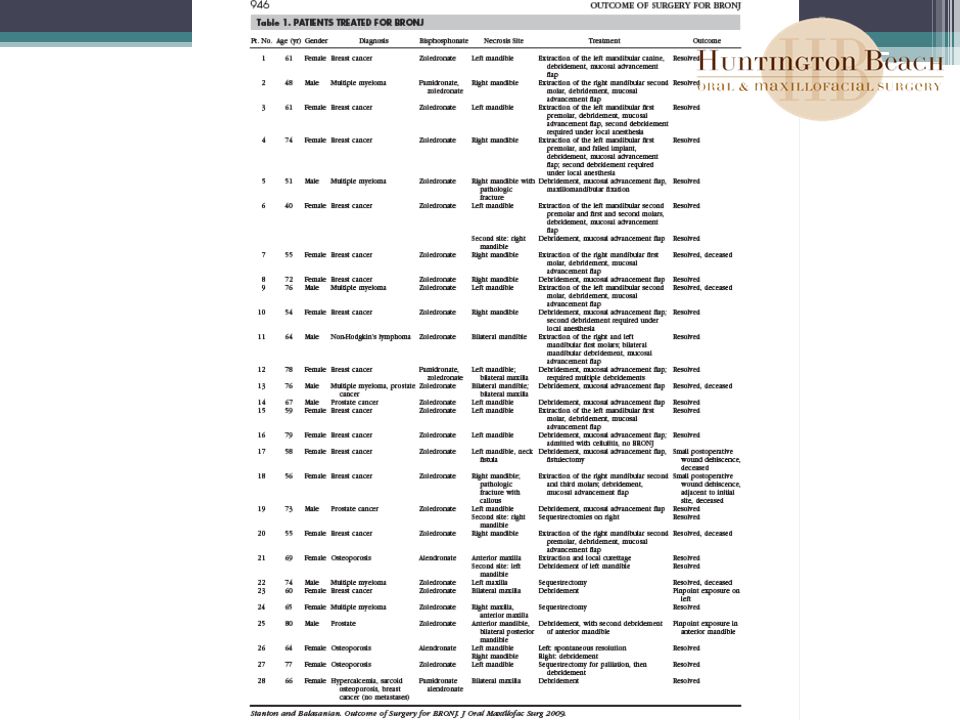
Literature review – Stanton, D. et. al. Outcome of Surgical Management of Bisphosphonate- Related Osteonecrosis of the Jaws: Review of 33 Surgical Cases 33 BRONJ cases treated surgically by a single surgeon at the Hospital of the University of Pennsylvania 30 debridement patients, 25 (including 1 sequestrectomy patient who required formal debridement) healed completely ▫Of 30 pts who underwent surgical debridement ▫18 healed following this initial treatment and remained healed ▫4 patients requiring sequestrectomy, 3 healed after the initial treatment ▫28 of 33 patients healed completely with complete mucosal coverage and elimination of pain ▫Four patients developed occurrence of BRONJ at a separate site 32 of 37 BRONJ occurrences healed with surgical debridement protocol or sequestrectomy. Follow-up range was 1 to 40 months (average 10.7).
 healed completely ▫Of 30 pts who underwent surgical debridement ▫18 healed following this initial treatment and remained healed ▫4 patients requiring sequestrectomy, 3 healed after the initial treatment ▫28 of 33 patients healed completely with complete mucosal coverage and elimination of pain ▫Four patients developed occurrence of BRONJ at a separate site 32 of 37 BRONJ occurrences healed with surgical debridement protocol or sequestrectomy. Follow-up range was 1 to 40 months (average 10.7)..")
23
Literature Review Abu-Id et al recommended ▫radical surgical resection up to the vital bone, because their study found conservative treatment to be unsuccessful in 61.5% of cases

24
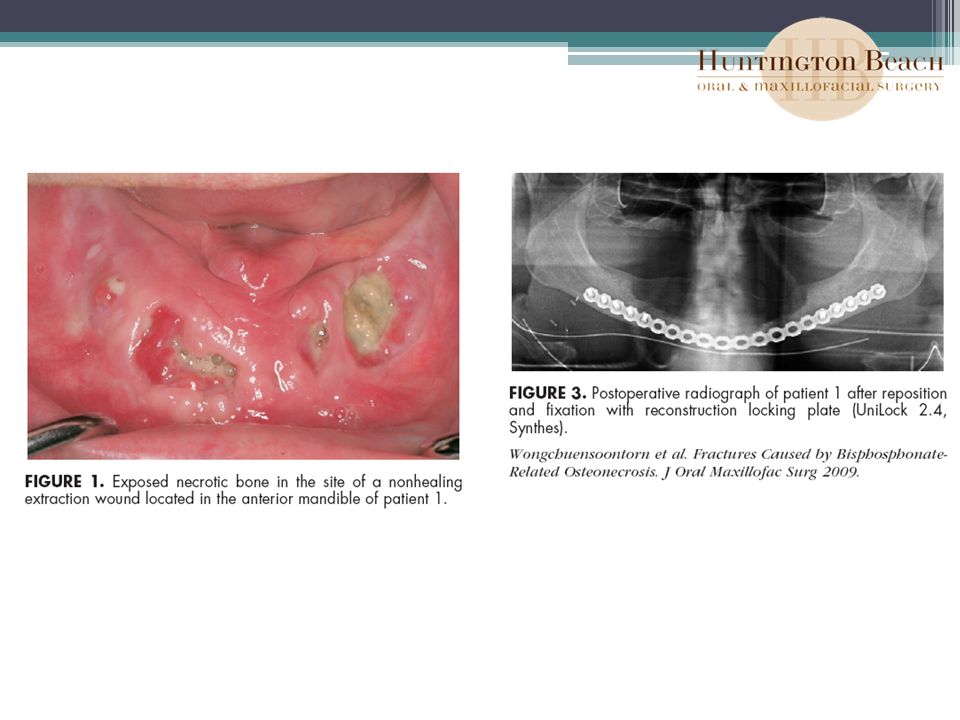
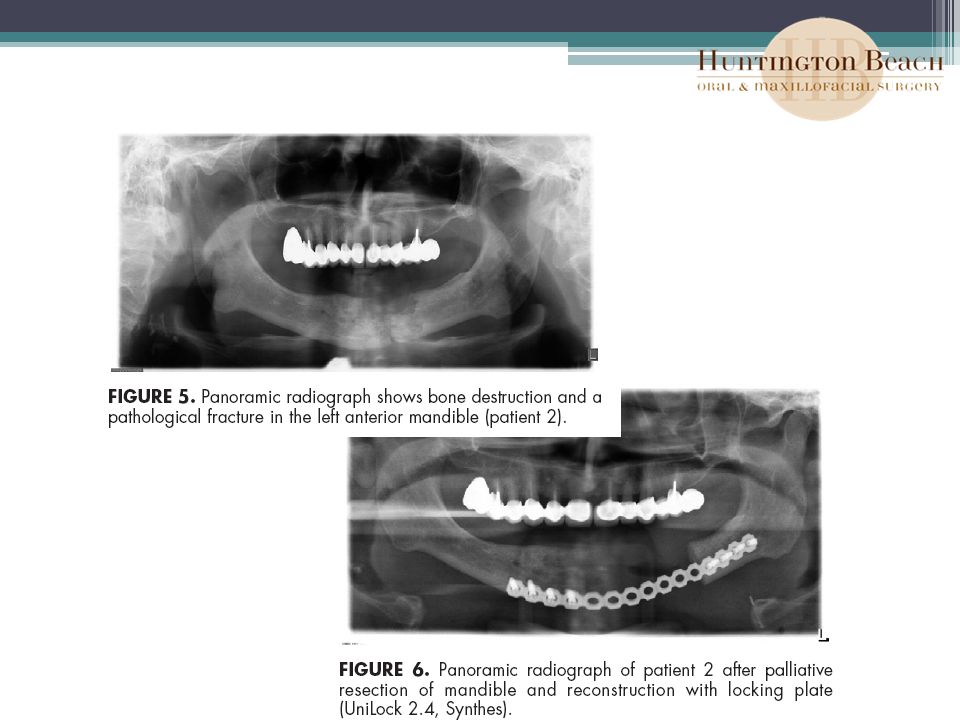
Literature Review: Wongchuensoontorn, C. et al Pathological Fractures in Patients Caused by Bisphosphonate-Related Osteonecrosis of the Jaws: Report of 3 Cases ▫Case series of 3 pts with pathologic fracture – whom were taking bisphosphonate therapy ▫2 of the cases undergone previous treatment with marginal resection of the mandible 3 rd case patient suffered from a pathological fracture after teeth extractions and debridement ▫ORIF with osteosynthesis the management of pathological fractures resulting from BRONJ may require segmental resection and immediate reconstruction with a reconstruction plate, as seen in our second case ▫Applied 2.4-mm reconstruction plate is the standard implant for fractures of an atrophic mandible

28
Future research The National Institutes of Health have provided funding opportunities for research on the pathophysiology of bisphosphonate-associated osteonecrosis of the jaw. ▫resulted in multiple research efforts focusing on several facets of this disease entity. ▫1) the effect of bisphosphonates on intra-oral soft tissue wound healing ▫2) analysis of alveolar bone hemostasis and the response to bisphosphonate therapy ▫3) antiangiogenic properties of bisphosphonates and their effects on jaw bone healing ▫4) pharmacogenetic research; 5) development of valid BRONJ risk assessment tools. Continued governmental and institutional support is required in order to elucidate the underlying pathophysiological mechanisms of BRONJ at the cellular and molecular level. Novel strategies for: the prevention ▫risk reduction ▫treatment of BRONJ need to be developed
 the effect of bisphosphonates on intra-oral soft tissue wound healing ▫2) analysis of alveolar bone hemostasis and the response to bisphosphonate therapy ▫3) antiangiogenic properties of bisphosphonates and their effects on jaw bone healing ▫4) pharmacogenetic research; 5) development of valid BRONJ risk assessment tools. Continued governmental and institutional support is required in order to elucidate the underlying pathophysiological mechanisms of BRONJ at the cellular and molecular level. Novel strategies for: the prevention ▫risk reduction ▫treatment of BRONJ need to be developed.")
29
References American Association of Oral and Maxillofacial Surgeons Position Paper on Bisphosphonate-Related Osteonecrosis of the Jaws. JOMS, 65: 369-376, 2007. Engroff SL. Et al Treating Bisphosphonate Osteonecrosis of the Jaws: Is there a Role for Resection and Vascularized Reconstruction? JOMS, 65:2374-2385, 2007. Grant, BT, et al Outcomes of Placing Dental Implants in Patients Taking Oral Bisphosphonates: A Review of 115 Cases. JOMS. 66:223-230, 2008 Ito M, Chokki M,, Ogino Y, Satomi Y, Azuma Y, Ohta T, Kiyoki M. Comparison of cytotoxic effects of bisphosphonates in vitro and in vivo. Calcif Tissue Int 1998:63:143-147 Marx, RE. Oral Bisphosphonate-Induced Osteonecrosis: Risk Factors, Prediction of Risk Using Serum CTX Testing, Prevention and Treatment. JOMS, 65: 2397-2410, 2007. Rogers MJ, Watts DJ, Russell RG. Overview of Bisphosphonates. CANCER supplement 1997;80:1652- 1660 Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. Journal of Oram and Maxillofacial Surg 2004;62:527-534 Wood J, Bonjean K, Ruetz S. Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid. J Pharmacol Exp Ther 2002: 302: 1055-1061.

30
References Curi, M et al.. Treatment of Avascular Osteonecrosis of the Mandible in Cancer Patients With a History of Bisphosphonate Therapy by Combining Bone Resection and Autologous Platelet-Rich Plasma: Report of 3 Cases. J Oral Maxillofac Surg 65:349-355, 2007 Carlson, E et al. The Role of Surgical Resection in the Management of Bisphosphonate-Related Osteonecrosis of the Jaws. J Oral Maxillofac Surg 67:85-95, 2009 Stanton, D. et al. Outcome of Surgical Management of Bisphosphonate-Related Osteonecrosis of the Jaws: Review of 33 Surgical Cases. J Oral Maxillofac Surg 67:943-950, 2009 Wongchuensoontorn, C. et al. Pathological Fractures in Patients Caused by Bisphosphonate- Related Osteonecrosis of the Jaws: Report of 3 Cases. J Oral Maxillofac Surg 67:1311-1316, 2009

Similar presentations

>")

















>")
