Download presentation
Presentation is loading. Please wait.

1
Infantile hemangioma Dr jayaprakash.k. p,asst prof,ICH,MCH,kottayam

2
Infantile hemangiomas (IH) are both the most common benign vascular tumors and the most common soft tissue tumors in children, 1 characterized by a unique tripartite growth cycle of proliferation, plateau, and involution
 are both the most common benign vascular tumors and the most common soft tissue tumors in children, 1 characterized by a unique tripartite growth cycle of proliferation, plateau, and involution")
3
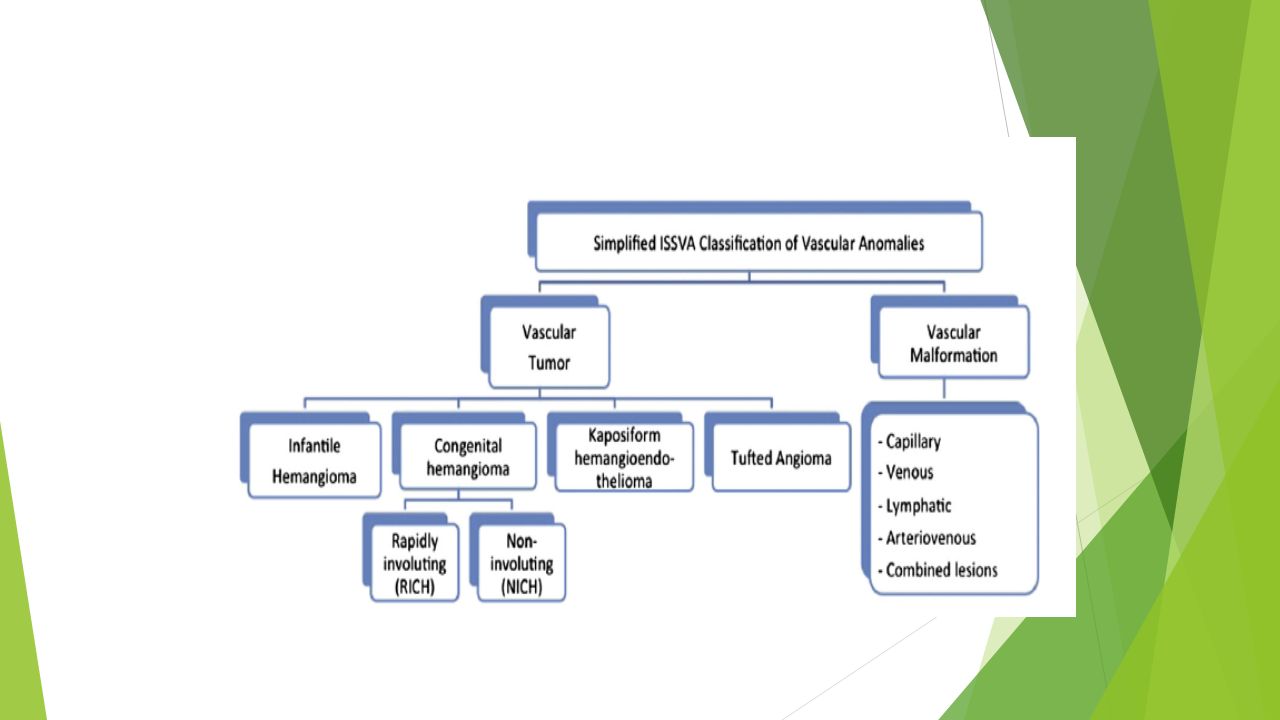
The classification rests primarily on distinguishing vascular tumors, of which IH are the most common, from vascular malformations. In all but a few cases, the diagnosis of IH can be determined by good history taking and physical examination.

4
EPIDEMIOLOGY The incidence of IH has remained unclear, because they are not often present at the time of hospital discharge after birth (when most registries for birth defects are completed.)
")
6
NATURAL HISTORY The growth cycle of IH is unique among vascular tumors and malformations, showingproliferation and preprogrammed involution. IH start with a nascent phase as either an area of pallor, a telangiectatic patch, or something mistaken for an ecchymosis or birth trauma. 16 They may present anywhere on the body surface but are present most commonly on the head and neck, a finding which is also true of vascular malformations. 17.

7
Typically, most begin to proliferate to a noticeable degree at between 2 and 4 weeks of life, although IH that are located primarily in the subcutis, known as deep IH, presenting as bluish or skin-colored nodules may not be noted until even a few months of age

8
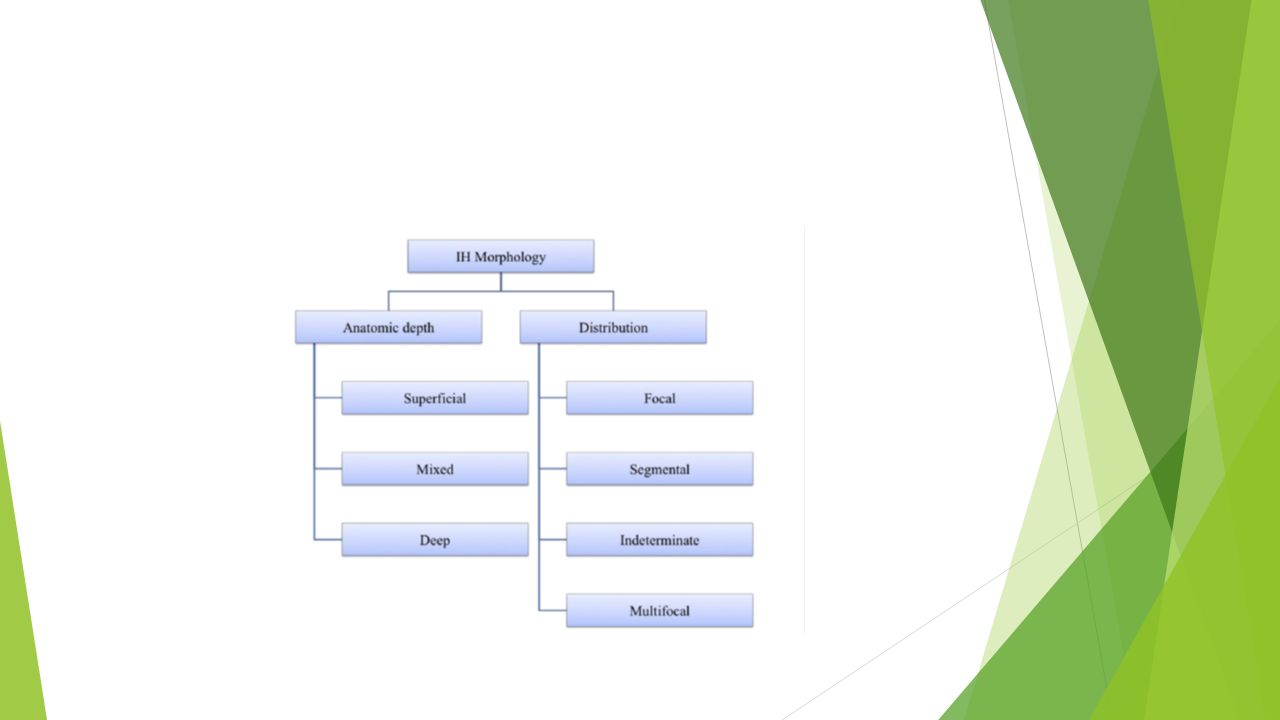
IH morphology can be described by the following 2 complementary concepts First, the concept of depth of involvement in the dermis, fat, and soft tissue is informative not only in establishing the diagnosis but can help to predict concern for future deformity and residua. In addition to deep lesions, IH can present as superficial, with bright pink, fuchsia, or red on the surface of a papule, plaque, or nodule Most IH present as mixed morphology, with both superficial and deep components,with a pink surface overlying a soft tissue swelling with a pink to bluish hue (

9
Second, the outline and distribution of IH on the body surface, in additionto the anatomic depth, provide valuable prognostic information about the possible need for treatment and potential associated complications. In this schema, IH are regarded as localized when they seem to arise from an isolated focal point as with a solitary nodule; these are the most common presentation. IH are deemed segmental when they occupy a subunit of a body part such as the forearm or a broad region on the face. Segmental IH are more often, but not always, plaques as opposed to nodules

14
This infant with multifocal IH had similar multifocal IH throughout the liver parenchyma; both the cutaneous and visceral IH responded well to propranolol

15
(A) This infant presented with an unusually severe ulceration down to muscle. (B) This infant presented with painful ulceration in the left axilla, which required addition of propranolol after failure of wound care alone. (C) A deep ulcer on the left cheek of an infant girl.
 This infant presented with painful ulceration in the left axilla, which required addition of propranolol after failure of wound care alone. (C) A deep ulcer on the left cheek of an infant girl..")
16
Excellent outcome after a course of propranolol for the patient in Fig. 10C shows a smooth white scar

17
This infant had both cerebrovascular anomalies and gastrointestinal bleeding as manifestations of her PHACE syndrome

18
During the first 2 months of life, nearly all hemangiomas double in size, and newer evidence suggests that the most rapid period of growth occurs between 5.5 and 7.5 weeks of age, with most rapid proliferation complete in the first 8 weeks of life. 16 Most reach 80% of maximum size at between 3 and 5 months of age, although segmental and deep IH have a more prolonged growth phase. 2

19
Maximum size isgenerally fulfilled at 9 months and almost always by 12 months of age, although rare reports exist of growth extending beyond age 2 years. 21 Plateau in growth then occurs and is followed by involution, which occurs over several years, withthe most rapid phase of involution occurring between ages 1 and 4 years. The growth cycle is dynamic, and within the same lesion, central graying and regression may begin to occur as the periphery is still proliferating.

20
COMPLICATIONS Most IH follow a benign course without the need for intervention aside from anticipatory guidance, but evidence shows that approximately 12% are complex and warrant referral for specialist evaluation

21
Size and location on the face are the other most important predictors of complications and need for treatment. The risk of permanent disfigurement is the most common reason that therapy is initiated, for the purpose of preventing the development of further distortion or destruction of anatomy

22
Ulceration is the most frequently occurring complication, occurring in up to 25% ofpatients at referral centers. 9 The first 4 months of life are the period of highest risk for the development of ulceration, and the occurrence of a gray-white discoloration akin to that typically seen and described as graying in the involuting IH can herald impending ulceration and should be a cause for worry, because it seems to represent necrosis of the overlying epidermis

23
d/d

24
MULTIFOCAL IH Infants can present with multiple, often small, focal IH; clinically, some infants presentwith monomorphic small superficial His, sometimes numbering in the hundreds,whereas others present with multiple focal IH of various sizes and appearance. This phenomenon has been referred to as benign neonatal hemangiomatosis when itoccurs without visceral involvement and as diffuse or disseminated neonatal hemangiomatosis (DNH) when it is accompanied by symptomatic IH internally, in the liver,gastrointestinal tract, lung, or central nervous system
 when it is accompanied by symptomatic IH internally, in the liver,gastrointestinal tract, lung, or central nervous system.")
25
Just as morphologic categorization is informative in IH, infantile hepatic hemangiomas (IHH) are characterized by Christison-Lagay and colleagues 33 as focal, multifocal,or diffuse. Focal hepatic hemangiomas occur most often without cutaneous involvement and may be diagnosed on prenatal ultrasonography; their clinical coursesuggests that they are the hepatic counterparts of rapidly involuting congenital hemangiomas(RICH), because they resolve spontaneously within several months of lifeand are generally asymptomatic; like congenital hemangiomas, they are glucosetransporter 1 negative, differentiating them from IH.
, because they resolve spontaneously within several months of lifeand are generally asymptomatic; like congenital hemangiomas, they are glucosetransporter 1 negative, differentiating them from IH..")
26
Multifocal and diffuse IHH areIH and follow an identical growth cycle of nascency, growth, and involution. Multifocalhepatic hemangiomas can be complicated y high-output heart failure from associatedportovenous or arteriovenous shunts, but multifocal lesions are often asymptomatic.There are several reports detailing positive response to therapy With propranolol and corticosteroids, separately or in combination

27
Diffuse IHH is the more ominous presentation, characterized by subtotal replacement of the liver parenchyma by vascular tumor. Abdominal compartment syndrome,respiratory and cardiac compromise, and multiorgan dysfunction are possible. Diffuse IHH can be associated with profound hypothyroidism from production of type III iodothyroninedeiodinase, placing infants at risk for mental retardation and cardiaccompromise. 37. Kulungowski and colleagues 38 found hypothyroidism in all patients with diffuse lesions, in 21% with multifocalIHH, and in no patients with focal disease.

28
Recent evidence also supports thelong-held dogma that infants with 5 or more cutaneous IH deserve screening abdominal ultrasonography to look for hepatic involvement. 39 Although there are reports ofgastrointestinal tract involvement complicating multifocal IH, it has been suggestedthat involvement here is associated with segmental IH instead of multifocal

29
COMPLICATIONS ASSOCIATED WITH SEGMENTAL IH PHACE (OMIM 606519), a neurocutaneous syndrome of skin, brain, eye, and ventral body anomalies, is the most well-ocumented segmental IH syndrome occurring in the setting of segmental facial IH, although a few cases have been reported with nonfacial IH and systemic complications relevant to PHACE
, a neurocutaneous syndrome of skin, brain, eye, and ventral body anomalies, is the most well-ocumented segmental IH syndrome occurring in the setting of segmental facial IH, although a few cases have been reported with nonfacial IH and systemic complications relevant to PHACE")
30
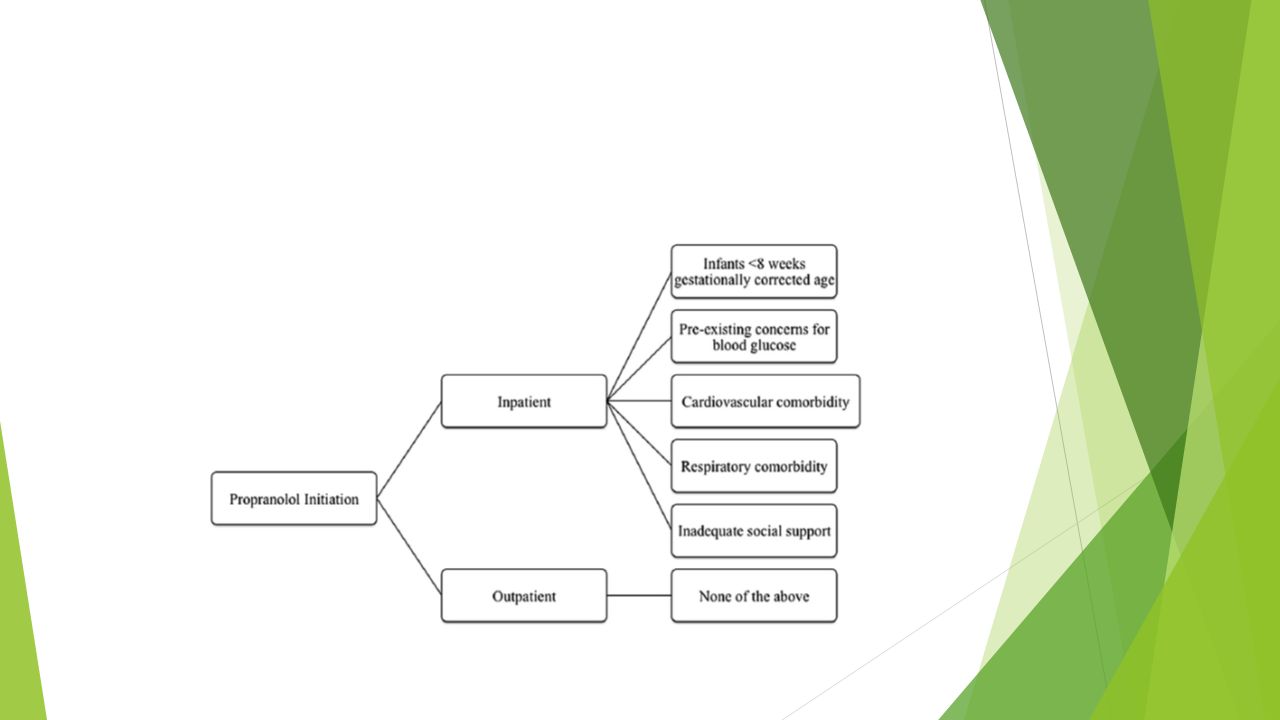
The most dramatic changes have occurred in the realm of therapy, with the complete shift toward b-blockers as the standard of care. The proposed mechanism of action of propranolol includes rapid vasoconstriction, which corresponds to the color change from pink to violaceous typically seen in the first 1 to 2 days of therapy. Inhibition of angiogenesis by downregulation of proangiogenic growth factors vascular endothelial growth factor, basic fibroblast growth factor, and matrix metalloproteinases 2 and 9 seems to correspond togrowth arrest.

31
Third, hastening of the induction of apoptosis of endothelial cells,known to occur in natural involution, has been proposed to result in the Stimulationof IH regression

32
In addition to propranolol, nadolol and atenolol have beensuggested as alternative systemic b-blockers for IH. 57–59 T Topical timolol 4–6 (generally preferred in the 0.5% gel forming solution formulation) is an alternative forsmaller, cosmetically sensitive lesions and can be used as an adjunct to systemictherapy in some cases, either to ostpone initiation of systemic therapy or to speedtapering of propranolol with subsequent transition to timolol to prevent posttreatmentrebound growth. The most commonly used dosage of propranolol is 2 mg/kg/d, although some evidencesuggests that infants may respond well at 1 to 1.5 mg/kg/d or require asmuch as 3 mg/kg/d.
 is an alternative forsmaller, cosmetically sensitive lesions and can be used as an adjunct to systemictherapy in some cases, either to ostpone initiation of systemic therapy or to speedtapering of propranolol with subsequent transition to timolol to prevent posttreatmentrebound growth. The most commonly used dosage of propranolol is 2 mg/kg/d, although some evidencesuggests that infants may respond well at 1 to 1.5 mg/kg/d or require asmuch as 3 mg/kg/d..")
34
The most frequent nonb-blocker therapeutic intervention is wound care for ulceration. 24,64 Barrier creams with petrolatum or zinc oxide can ease pain and help to prevent contamination, especially in the diaper area, which can cause irritation andimpede healing. Hydrocolloid dressings (eg, Duoderm), silver impregnated dressings (eg, AquacelAg), and petrolatum gauze can be helpful to protect and gently debridethe ulcer. In the appropriate setting of odor or purulent discharge, topical or oralantibiotics may be necessary. U
, silver impregnated dressings (eg, AquacelAg), and petrolatum gauze can be helpful to protect and gently debridethe ulcer. In the appropriate setting of odor or purulent discharge, topical or oralantibiotics may be necessary. U.")
35
Pulsed dye laser has also been used to treat ulcerated IH, although the mechanism of action is poorly understood. 65 The ability of propranolol to speed ulcer healing has been widely reported

36
KEY POINTS Infantile hemangiomas (IH) show great heterogeneity in size, morphology, growth, residuaremaining after involution, and in degree of response to therapy. Propranolol is now preferred first-line therapy, given that its efficacy, tolerability, andsafety are superior to that of oral corticosteroids. The period of most rapid proliferation is complete by 8 weeks after birth, suggesting that referral to pecialists should occur early, within the first month of life for concerning IH. More infants are now treated with propranolol than were previously treated with Oral corticosteroids,and the full implications of this shift in practice are not yet clear

Similar presentations



: Three cases Deba P Sarma, MD Omaha.>")

 Closed wound: Skin is intact (not opened) include crushing injury and contusions. Wounds A) Skin involvement: 1) Open wound: when the whole thickness.>")




 For Treating Cutaneous Leishmaniasis Dr. Eshtyag Abdeen Ali Dermatologist.>")




 Disease (strep throat, necrotizing fasciitis, impetigo) By: Dr. Awatif Alam.>")






