Download presentation
Presentation is loading. Please wait.

1
PAIN MECHANISMS

2
PAIN Unpleasant sensory and emotional experience associated with actual or potential tissue damage Functions: Stop Signal Warning of a threat Basis of learning Forces a person to rest

3
Chances are, you know someone in pain
50 million Americans are partially or totally disabled by chronic pain Nine out of ten Americans (aged 18 and older) suffer from pain at least once a month 26 million Americans (15%) have severe pain 50% of Americans (aged 65 and older) suffer from pain on a daily basis Sources: The Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) Gallup Survey June 1999 Untying the Knot
 suffer from pain at least once a month. 26 million Americans (15%) have severe pain. 50% of Americans (aged 65 and older) suffer from pain on a daily basis. Sources: The Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) Gallup Survey June Untying the Knot.")
4
Chronic pain has many faces
Other than cancer pain, doctors report treating patients for chronic pain associated with the following conditions - Lower back pain (75%) - Osteoarthritis (40%) - Headaches (26%) - Migraines (26%) - Fibromyalgia (12%) Sources: 1999 National Pain Survey © Ortho-McNeil Pharmaceutical 2002 Untying the Knot
 - Osteoarthritis (40%) - Headaches (26%) - Migraines (26%) - Fibromyalgia (12%) Sources: 1999 National Pain Survey. © Ortho-McNeil Pharmaceutical Untying the Knot.")
5
Components of chronic pain
Many people who suffer from chronic pain experience two aspects of pain: Persistent pain – pain that lasts 12 or more hours each day 1 Breakthrough pain – flare of pain that “breaks through” the medicine taken around-the-clock, which typically peaks in as little as 3 minutes and may last up to 30 minutes 2,3 1. Labcevic JS. Pain management: medical and legal issues of undertreatment. In Weiner RS (Ed.), Pain Management: a practical guide for clinicians. Sixth edition. CRC Press LLC : Lobb J. Understanding Breakthrough Pain. National Pain Foundation Website Available at: Portenoy, RK, Hagen NA. Breakthrough pain: definition, prevalence and characteristics. Pain ; 41: Untying the Knot
, Pain Management: a practical guide for clinicians. Sixth edition. CRC Press LLC. 2002: Lobb J. Understanding Breakthrough Pain. National Pain Foundation Website Available at: Portenoy, RK, Hagen NA. Breakthrough pain: definition, prevalence and characteristics. Pain. 1990; 41: Untying the Knot.")
6
Pain impacts quality of life
43% of adults (83 million) report pain frequently affects their participation in life’s activities 55% of senior citizens report suffering from pain on a daily basis Senior citizens report that severe or moderate pain often lasts over two years Sources: Gallup Survey June NPF Telephone Survey Untying the Knot
 report pain frequently affects their participation in life’s activities. 55% of senior citizens report suffering from pain on a daily basis. Senior citizens report that severe or moderate pain often lasts over two years. Sources: Gallup Survey June NPF Telephone Survey. Untying the Knot.")
7
Pain has economic implications
In 1995 pain caused 50 million lost work days at a cost of more than $3 billion in lost wages 8% of the workforce claimed short term disability due to pain (average of 17 days) Note: Short term disability starts after sick days are depleted, indicating significant lost work time. Sources: Survey by Louis Harris & Associates © Ortho-McNeil Pharmaceutical 2002 Untying the Knot
 Note: Short term disability starts after sick days are depleted, indicating significant lost work time. Sources: 1996 Survey by Louis Harris & Associates. © Ortho-McNeil Pharmaceutical Untying the Knot.")
8
Strengthening the doctor-patient relationship
Pain accounts for 80% of all physician visits 64% of pain sufferers will see a doctor only when they cannot stand the pain any longer 42% of people who visit their doctor for pain feel misunderstood by their physician Sources: Gallup Survey June Survey by Gatchel & Turk, Psychological Approaches to Pain Management Untying the Knot

9
Strengthening the doctor-patient relationship
22% of chronic pain patients have changed doctors (at least 3 times) in their search for pain relief The primary reasons why chronic pain patients change physicians are: the doctor’s - attitude toward their pain - knowledge about pain - ability to treat pain Source: Chronic Pain in America: Roadblocks to Relief Conducted by: Roper Starch Worldwide Inc. January 1999 Untying the Knot
 in their search for pain relief. The primary reasons why chronic pain patients change physicians are: the doctor’s. - attitude toward their pain. - knowledge about pain. - ability to treat pain. Source: Chronic Pain in America: Roadblocks to Relief Conducted by: Roper Starch Worldwide Inc. January Untying the Knot.")
10
Case Study #2 A 42 year-old female injured her neck in an automobile accident 2 months prior to seeking help. She noted a dull pain in her jaw during this period. Three weeks prior to admission a sharp, shooting pain (like an “electric shock”) was noted beginning in her neck and shooting to her jaw and face. The pain could be triggered by coughing, sneezing and straining to pick up heavy objects.
 was noted beginning in her neck and shooting to her jaw and face. The pain could be triggered by coughing, sneezing and straining to pick up heavy objects.")
11
Case Study #2 (cont’d) The patient also reported parasthesia as a “tingling numbness” of the left cheek. Neurological examination revealed absent jaw jerk (masseter deep tendon reflex) on the left. Motor strength of the upper and lower limbs was normal and there were no Babinski signs.
 on the left. Motor strength of the upper and lower limbs was normal and there were no Babinski signs.")
12
Case Study #2 (Question)
The pain this patient experienced is due to Excitation of nociceptors Excitation of medium- and large-diameter sensory nerve fibers Excitation of small-diameter myelinated and unmyelinated sensory nerve fibers Pressure on a dorsal root More than one but not all of the above

16
INFLAMMATION

17
Tissue Injury & Inflammation
“Inflame” – to set fire. Inflammation is “dynamic response of vascularized tissue to injury.” Is a protective response. Serves to bring defense & healing mechanisms to the site of injury.

18
Triple Response of Lewis
Flush: capillary dilatation. Flare: arteriolar dilatation. Weal: exudation, edema.

19
(Flare, Flush & Weal – Lewis)
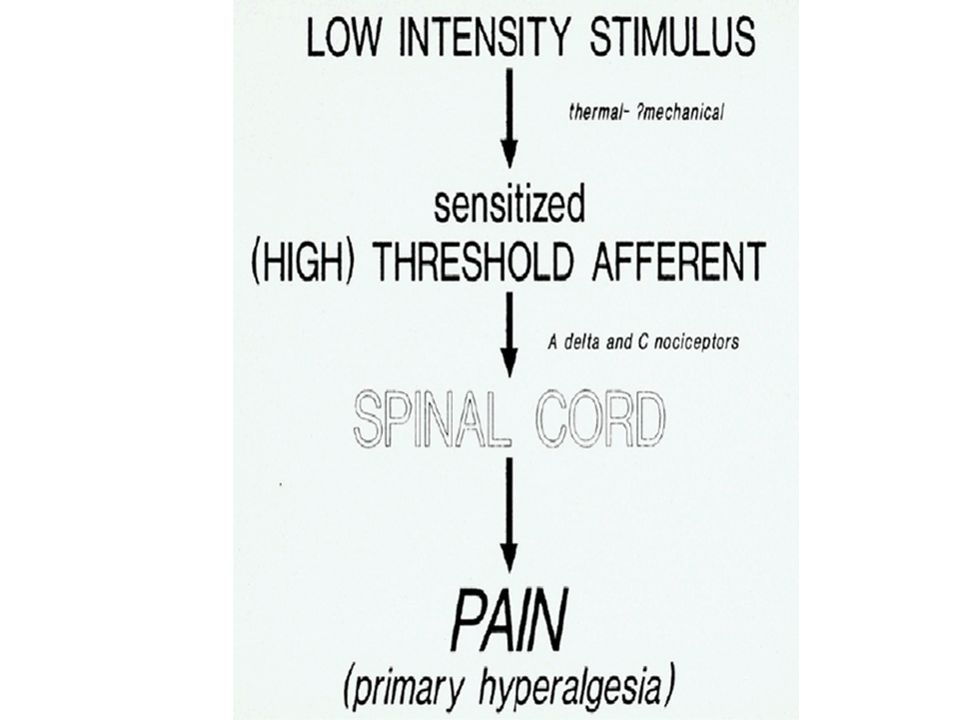
Red, Warm & Swollen (Flare, Flush & Weal – Lewis) Triple response HYPERALGESIA IN AREAS SURROUNDING INJURY
 Triple response. HYPERALGESIA IN AREAS SURROUNDING INJURY.")
20
“The Angry” Axon Reflex antidromic stimulation

23
Spinothalamic (Anterolateral) System
 System")
24
The Spinothalamic System
The spinothalamic system provides for temperature and pain sensibility. This small fiber, evolutionarily old system provides for perceptual capabilities that have a larger component of emotional tone, the affective component, than do perceptions provided for by the DCML system. Because its fibers ascend in the anterolateral portion of the spinal cord, the spinothalamic system is also called the anterolateral system.

25
Spinothalamic System Receptor = Nociceptor (responds to noxious stimuli such as pain and temperature) Nociceptors are naked nerve endings of primary (first order) afferent neurons Nociceptor signaling regulated by ion channels and membrane receptor proteins Pain and temperature signals transmitted from nociceptors to first order primary afferents without synapse First order neurons release SP and glutamate primarily and synapse in the Substantia Gelatinosa (SG) of spinal cord.
 afferent neurons. Nociceptor signaling regulated by ion channels and membrane receptor proteins. Pain and temperature signals transmitted from nociceptors to first order primary afferents without synapse. First order neurons release SP and glutamate primarily and synapse in the Substantia Gelatinosa (SG) of spinal cord.")
26
Decussation of Second Order Spinothalamic Neurons
Pain signals transmitted to second order neurons contralaterally at spinal level of stimulated receptor or at a spinal segment above or below the stimulated receptor (tract of Lissauer) making pain and temperature difficult to localize to a single dermatome precisely. Brown-Sequard syndrome (spinal cord hemisection) lesions produce ipsilateral and contralateral loss of pain and temperature sensation in the dermatomes at the spinal level of the lesion but only contralateral loss in the dermatomes below the spinal level of the lesion
 making pain and temperature difficult to localize to a single dermatome precisely. Brown-Sequard syndrome (spinal cord hemisection) lesions produce ipsilateral and contralateral loss of pain and temperature sensation in the dermatomes at the spinal level of the lesion but only contralateral loss in the dermatomes below the spinal level of the lesion.")
27
Hemisection of Spinal Cord Brown-Sequard Syndrome

28
Brown-Sequard Syndrome

30
Role of Thalamus Second order neurons transmit pain and temperature signals to thalamus contralateral to stimulated receptor VPM processes pain and temperature signals from trigeminal (CNV) analog of spinothalamic system for head and neck VPL processes pain and temperature signals from peripheral regions of the body such as viscera, trunk and limbs Medial (intralaminar) thalamic nuclei process pain and temperature signals from reticular formation (spinoreticular fibers) such as raphe nuclei and locus coruleus Central (thalamic) pain signals cannot be localized (e.g., metastatic cancer) and central (thalamic) pain syndrome is relieved by producing electrical lesions in a thalamotomy procedure
 analog of spinothalamic system for head and neck. VPL processes pain and temperature signals from peripheral regions of the body such as viscera, trunk and limbs. Medial (intralaminar) thalamic nuclei process pain and temperature signals from reticular formation (spinoreticular fibers) such as raphe nuclei and locus coruleus. Central (thalamic) pain signals cannot be localized (e.g., metastatic cancer) and central (thalamic) pain syndrome is relieved by producing electrical lesions in a thalamotomy procedure.")
31
Role of Cerebral Cortex
Pain and temperature signals transmitted from VPL and VPM (specific thalamic nuclei) to somatosensory cortices SI and SII for localization Pain and temperature signals transmitted from medial intralaminar (nonspecific) nuclei to all regions of cerebral cortex for “alerting” response, which induce wakefulness and inhibit sleep Pain and temperature signals also transmitted from intralaminar nonspecific nuclei to limbic system, hypothalamus and associated structures for emotional, endocrine, stress and autonomic responses which produce fear, suffering, cardiovascular, respiratory, gastrointestinal, urogenital and stress-related hormonal responses
 to somatosensory cortices SI and SII for localization. Pain and temperature signals transmitted from medial intralaminar (nonspecific) nuclei to all regions of cerebral cortex for alerting response, which induce wakefulness and inhibit sleep. Pain and temperature signals also transmitted from intralaminar nonspecific nuclei to limbic system, hypothalamus and associated structures for emotional, endocrine, stress and autonomic responses which produce fear, suffering, cardiovascular, respiratory, gastrointestinal, urogenital and stress-related hormonal responses.")
32
Functional Properties of the Spinothalamic System
The spinothalamic system subserves pain and temperature sensibility and provides for a less precise, less well-localized, more emotion laden type of somatic sensibility than the DCML system. The affective component of the pain experience is due to the divergent projections of the spinothalamic system, especially those into the reticular formation, intralaminar thalamic nuclei, and limbic system.

33
Learning Objectives: Differentiate between the mechanisms of somatic pain, visceral pain, referred pain and phantom limb pain.

34
GIII (A-delta) and GIV (C-fibers) Afferents for Pain
 and GIV (C-fibers) Afferents for Pain")
35
Transient Receptor Potential Vanilloid-1 (TRPV1) Channels
All animals need to sense temperature to avoid hostile environments and to regulate their internal homeostasis. A particularly obvious example is that animals need to avoid damagingly hot stimuli. The mechanisms by which temperature is sensed have until recently been mysterious, but in the last couple of years, we have begun to understand how noxious thermal stimuli are detected by sensory neurons. Heat has been found to open a nonselective cation channel in primary sensory neurons, probably by a direct action. In a separate study, an ion channel gated by capsaicin, the active ingredient of chili peppers, was cloned from sensory neurons. This channel (vanilloid receptor subtype 1, VR1) is gated by heat in a manner similar to the native heat-activated channel, and our current best guess is that this channel is the molecular substrate for the detection of painful heat. Both the heat channel and VR1 are modulated in interesting ways. The response of the heat channel is potentiated by phosphorylation by protein kinase C, whereas VR1 is potentiated by externally applied protons. Protein kinase C is known to be activated by a variety of inflammatory mediators, including bradykinin, whereas extracellular acidification is characteristically produced by anoxia and inflammation. Both modulatory pathways are likely, therefore, to have important physiological correlates in terms of the enhanced pain (hyperalgesia) produced by tissue damage and inflammation.
 is gated by heat in a manner similar to the native heat-activated channel, and our current best guess is that this channel is the molecular substrate for the detection of painful heat. Both the heat channel and VR1 are modulated in interesting ways. The response of the heat channel is potentiated by phosphorylation by protein kinase C, whereas VR1 is potentiated by externally applied protons. Protein kinase C is known to be activated by a variety of inflammatory mediators, including bradykinin, whereas extracellular acidification is characteristically produced by anoxia and inflammation. Both modulatory pathways are likely, therefore, to have important physiological correlates in terms of the enhanced pain (hyperalgesia) produced by tissue damage and inflammation.")
36
Vanilloid Receptor

37
Purinergic (ATP) Receptors
It has been well known that pain is caused by nociceptive stimulation such as protons (i.e. acidic solutions), heat and capsaicin, a pungent ingredient of chili peppers. For a long period, the signal transduction mechanism of pain activated by these nociceptive stimuli has not been clarified. Recent advance, especially the identification of TRPV1 receptor (for which capsaicin, protons and heat are ligands), P2X and P2Y receptor (for which ATP is a ligand) and acid sensing ion channel made a remarkable progress in understanding the mechanism of nociceptive neurons.
, heat and capsaicin, a pungent ingredient of chili peppers. For a long period, the signal transduction mechanism of pain activated by these nociceptive stimuli has not been clarified. Recent advance, especially the identification of TRPV1 receptor (for which capsaicin, protons and heat are ligands), P2X and P2Y receptor (for which ATP is a ligand) and acid sensing ion channel made a remarkable progress in understanding the mechanism of nociceptive neurons.")
38
Learning Objectives: Explain the roles of the axon reflex and hyperalgesia in the Triple Response of Lewis.

39
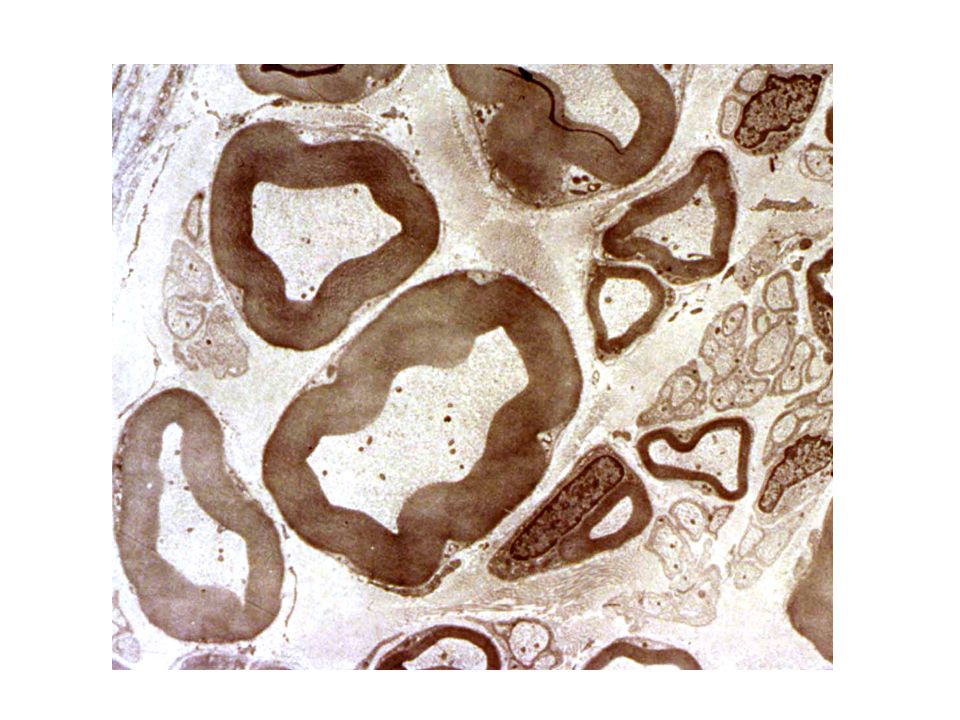
Thermal and Pain Receptors
The spinothalamic system receives its input from free (naked, bare) nerve endings that are the peripheral terminals of small- diameter myelinated (A) and unmyelinated (C) primary afferent fibers.
 nerve endings that are the peripheral terminals of small- diameter myelinated (A) and unmyelinated (C) primary afferent fibers.")
41
Capsaicin Menthol

42
Thermoreceptor: frequency proportional to delta-T
Set point Learning Objectives: Explain the responses of a thermal receptor to changes in temperature.

43
Learning Objectives: Explain the mechanisms of paradoxical cold and pain associated with stimulating thermal receptors.

44
Pin-prick test

45
Sources of chemical stimuli: neurons, blood, damaged
Hmine, BK, PG, 5-HT, H+, K+ Ach, SP Sources of chemical stimuli: neurons, blood, damaged tissues, mast cells, platelets Learning Objectives: Explain the adequate stimulus for nociceptors and compare the mechanisms of slow and fast pain.

48
Small Diameter Afferent Fibers
Cutaneous mechanoreceptors Respond to nondiscriminative tactile stimuli Pinch, rub, stretch, squeeze A-delta and C fiber, high-threshold Cutaneous thermoreceptors Respond to transient change in temperature Innocuous ward and cool stimuli

49
Small Diameter Afferent Fibers
Cutaneous nociceptors – cutaneous pain A-delta mechanoreceptors Mechanical tissue damage C-polymodal nociceptors Mechanical tissue damage, noxious thermal stimuli, endogenous algesic chemicals C-fiber mechanonociceptors A-delta heat thermonociceptors A-delta, C-fiber cold thermonociceptors C-fiber chemonociceptors – algesic chemicals

50
Deep Nociceptors Muscle nociceptors – GIII, GIV afferents
Bradykinin 5-HT (Inflammation releases 5-HT in TMJD) K+ GLUT Joint nociceptors – GIII, GIV afferents Inflammation (K+, Bradykinin, 5-HT, GLUT) Kaolin (experimental models) Carregeenan (experimental models)
 K+ GLUT. Joint nociceptors – GIII, GIV afferents. Inflammation (K+, Bradykinin, 5-HT, GLUT) Kaolin (experimental models) Carregeenan (experimental models)")
51
Visceral Nociceptors Heart – A-delta and C afferents H+ K+ Ischemia
Bradykinin PGE-2

52
Lung Nociceptors Lung Irritant Receptors – A-delta afferents
Irritant aerosols and gases Mechanical stimuli Lung “J” Receptors – C-fibers Capsaicin Pulmonary congestion, edema Inhaled irritants

53
G.I. Tract Nociceptors Rapidly-adapting mechanoreceptors, slowly adapting mechanoreceptors, chemoreceptors (A-delta and C-fibers) Irritation of the mucosa Distension Powerful contraction Torsion Traction Bloating Cramping Appendicitis Impaction

54
Distribution of Nociceptors
UG Tract - C-polymodal (e.g., testis) Intense mechanical stimuli Noxious heat Algesic chemicals Bone - periosteum Blood Vessels - walls Brain – none C-fibers in dura mater
 Intense mechanical stimuli. Noxious heat. Algesic chemicals. Bone - periosteum. Blood Vessels - walls. Brain – none. C-fibers in dura mater.")
55
CNS Neurotransmitters of A-delta and C-fibers
Substance P (Neuropeptide) Calcitonin Gene Realted Peptide (CGRP) Excitatory amino acids – e.g., glutamate Release in ischemia/hypoxia - neurotoxicity
 Calcitonin Gene Realted Peptide (CGRP) Excitatory amino acids – e.g., glutamate. Release in ischemia/hypoxia - neurotoxicity.")
56
Membrane Receptors of A-delta and C-fibers in CNS
Purinergic (ATP) GABA-ergic Mu opioid receptor (MOR)
 GABA-ergic. Mu opioid receptor (MOR)")
57
Large Multimodal RFs Receptive fields of central neurons within the spinothalamic system are often large. Individual neurons may respond to several different stimuli (multimodal responses). RFs may be bilateral. Some neurons are specifically sensitive to noxious stimulation; others are sensitive to temperature changes.
. RFs may be bilateral. Some neurons are specifically sensitive to noxious stimulation; others are sensitive to temperature changes.")
58
Spinal tract of CNV (Trigeminal Analog of STT)
Spinal tract of CNV descends and crosses in medulla and cervical spinal cord Learning Objectives: Memorize the structures and functions of the spinothalamic somatosensory systems.

59
Spinal Tract of CNV Trigeminal analog of spinothalamic system transmits pain and temperature signals from head and neck to VPM of thalamus Second order neurons in in spinal tract of CNV transmits pain and temperature contralaterally via decussations in pons, medulla or cervical spinal cord Cervical spinal lesions can produce abnormal pain and temperature sensations in head and neck (e.g., cervical arthritis, whiplash injury producing temporomandibular disease)
")
60
Coarse Somatotopic Organization
Somatotopic organization in the spinothalamic system is not as distinct as in the DCML system, except in the spinal cord.

61
STT fibers distribute widely to specific and nonspecific nuclei
Learning Objectives: Explain how knowledge of the Brown-Sequard syndrome can be used to localize neural lesions.

62
Spinal cord distribution of STT fibers
Pain and temperature deficits referred to receptor dermatome: Law of projection Hand/arm medial, foot/leg lateral distribution Inverse to DCML Learning Objectives: Memorize the spinal organization of spinothalamic somatosensory system fibers.

63
Features of the Pain Experience

64
Features of the Pain Experience
Pain is a complex perceptual experience. It is difficult, except at the conceptual level, to separate the objective sensory aspects from the cognitive and emotional reactions to the presence of pain. The complexity of the pain experience is matched by the complexity of the central pathways for nociceptive inputs. For pain from superficial tissues, it is customary to distinguish fast (pricking) pain, due to activation of A (GIII) fibers, from slow (burning) pain which is due to activation of C (GIV) fibers. Fast pain does not last much longer than the stimulus, is easy to endure, and is not accompanied by much of an affective, or emotional, component. It is like the pain from a hypodermic needle during an injection. Slow pain persists, is hard to endure, and has a large affective component; autonomic responses may occur. Slow pain is associated with suffering and is most often the kind of pain that brings the patient to the doctor's office.
 pain, due to activation of A (GIII) fibers, from slow (burning) pain which is due to activation of C (GIV) fibers. Fast pain does not last much longer than the stimulus, is easy to endure, and is not accompanied by much of an affective, or emotional, component. It is like the pain from a hypodermic needle during an injection. Slow pain persists, is hard to endure, and has a large affective component; autonomic responses may occur. Slow pain is associated with suffering and is most often the kind of pain that brings the patient to the doctor s office.")
65
Control of Nociceptive Inputs and Modulation of Pain
The brain is able to modulate all the varieties of sensation via efferent connections to receptors or neurons in sensory pathways. This is also true for nociception and there are three (non-mutually exclusive) mechanisms by which nociceptive inputs are modulated.
 mechanisms by which nociceptive inputs are modulated.")
66
Gate Control Theory of Pain
Large-diameter primary afferent fibers (Aα and Aβ fibers) can inhibit, via inhibitory interneurons, dorsal horn neurons (projection neurons) that give rise to spinothalamic tract fibers. This form of control of nociceptive input is known as the gate control theory of Melzack and Wall, after the scientists who proposed it. Electrical stimulation of the dorsal columns or of large, myelinated peripheral nerve fibers by transcutaneous electrical nerve stimulation (TENS) may relieve pain by this mechanism. Acupuncture anesthesia may also be an example of dorsal column-anterolateral system interaction since it is reported to be effective only when needles are inserted near bundles of Group II fibers. Dorsal column-anterolateral system interactions may occur at several levels, including spinal cord dorsal horn, spinal V nucleus, and thalamus.
 can inhibit, via inhibitory interneurons, dorsal horn neurons (projection neurons) that give rise to spinothalamic tract fibers. This form of control of nociceptive input is known as the gate control theory of Melzack and Wall, after the scientists who proposed it. Electrical stimulation of the dorsal columns or of large, myelinated peripheral nerve fibers by transcutaneous electrical nerve stimulation (TENS) may relieve pain by this mechanism. Acupuncture anesthesia may also be an example of dorsal column-anterolateral system interaction since it is reported to be effective only when needles are inserted near bundles of Group II fibers. Dorsal column-anterolateral system interactions may occur at several levels, including spinal cord dorsal horn, spinal V nucleus, and thalamus.")
67
Gate Control Theory of Pain
Learning Objectives: Explain the gate control theory of pain.

68
Gate Control Theory of Pain
Pain and temperature signals cause C and A-delta fibers to release an excitatory neurotransmitter (e.g., glutamate, SP) and stimulate second order neurons directly Pain and temperature signals also cause C and A-delta fibers to release an inhibitory neurotransmitter (e.g., GABA, enkephalin) and inhibit an inhibitory interneuron, thereby, opening the gate for transmitting pain and temperature signals to second order neurons Tactile signals cause A-fibers to release an excitatory neurotransmitter and stimulate the inhibitory interneuron which closes the gate for transmitting pain and temperature signals to second order neurons Tactile stimulation such as stroking, massaging or kissing an affected area closes the gate and raises the pain threshold
 and stimulate second order neurons directly. Pain and temperature signals also cause C and A-delta fibers to release an inhibitory neurotransmitter (e.g., GABA, enkephalin) and inhibit an inhibitory interneuron, thereby, opening the gate for transmitting pain and temperature signals to second order neurons. Tactile signals cause A-fibers to release an excitatory neurotransmitter and stimulate the inhibitory interneuron which closes the gate for transmitting pain and temperature signals to second order neurons. Tactile stimulation such as stroking, massaging or kissing an affected area closes the gate and raises the pain threshold.")
69
Role of Enkephalins and Endorphins in Modulating Pain
Enkephalins and endorphins are naturally occurring brain peptides with an opiate-like effect on pain transmission. Certain inhibitory interneurons in the dorsal horn use enkephalin as a neurotransmitter. The interneurons are activated by serotonergic fibers that descend from the reticular formation. Enkephalin causes a decrease in the EPSP produced by the 1o nociceptor via a presynaptic inhibitory action. In part, the effect is due to a decrease in the duration of the action potential in the C fiber terminal. When that occurs, less glutamate (GLU) and substance P are released from the terminal. Enkephalin also may cause a postsynaptic hyperpolarization due to a conductance-increase IPSP.
 and substance P are released from the terminal. Enkephalin also may cause a postsynaptic hyperpolarization due to a conductance-increase IPSP.")
70
Learning Objectives: Explain the relationship between serotonin and enkephalin in the perception of pain.

72
Role of Serotonin and Norepinephrine
Reticulospinal fibers from raphe nuclei project to dorsal horn of spinal cord and release serotonin which stimulates interneurons to release enkephalin Enkephalin inhibits transmission of pain and temperature signals in second order neurons Reticulospinal fibers from locus coruleus also project to dorsal horn of spinal cord and release norepinephrine which inhbits pain and temperature signals by an unknown mechanism Mental illnesses such as depression decrease serotonin and norepinephrine and lower pain thresholds while antidepressant drugs and therapies (e.g., exercise) which increase serotonin and norepinephrine levels raise pain thresholds
 which increase serotonin and norepinephrine levels raise pain thresholds.")
73
Role of Efferent Pathways in Modulating Pain
Some individuals may, in the midst of great exertion or focused activity, fail to notice a major injury. One factor that may account for this type of modulation of nociceptive inputs is that nerve fibers arising from cortex, reticular formation, etc., can inhibit spinothalamic system neurons. For instance, corticospinal tract fibers that originate in SI cortex and which are active during voluntary movements terminate in the dorsal horn of the spinal cord. Activity in these fibers could cause inhibition of second order neurons in the spinothalamic system.

74
Cortex and Pain The cortical contribution to pain perception is not well understood. Surgical excision of SI cortex is not an effective therapy for chronic pain. However, electrolytic lesions of the thalamus can produce analgesia or hypalgesia (lost or decreased pain perception). Lesions of the ventrobasal complex may cause loss of touch and cutaneous pain; lesions of the intralaminar nuclei may cause loss of deep pain. Vascular lesions along the somatosensory pathway may cause a late-developing "central pain" that appears in the anesthetic limb. This type of pain is called thalamic pain. It is similar to phantom limb pain and may arise due to the loss of inhibitory control by large-diameter fibers over nociceptive neurons representing the affected limb. These data have led to the notion that pain is appreciated at a subcortical, probably thalamic, level.
. Lesions of the ventrobasal complex may cause loss of touch and cutaneous pain; lesions of the intralaminar nuclei may cause loss of deep pain. Vascular lesions along the somatosensory pathway may cause a late-developing central pain that appears in the anesthetic limb. This type of pain is called thalamic pain. It is similar to phantom limb pain and may arise due to the loss of inhibitory control by large-diameter fibers over nociceptive neurons representing the affected limb. These data have led to the notion that pain is appreciated at a subcortical, probably thalamic, level.")
75
Learning Objectives: Compare and contrast the roles of the hypothalamus, the nonspecific thalamic nuclei and the ventrobasal thalamic nuclei on autonomic, emotional, motivational, discrimninatory and cognitive perceptual factors in somatosensory functions.

76
Plasticity of Pain Perception
The pain experience is complex and remarkably plastic. Drugs, fear, stress, joy, hypnosis, ritualistic participation, psychosurgery, etc., may profoundly influence it. Both the perception of pain (knowledge that tissue has been damaged) and the emotional reaction to it (the degree of suffering) can be altered. Pain is not necessarily commensurate with the extent of tissue damage.
 and the emotional reaction to it (the degree of suffering) can be altered. Pain is not necessarily commensurate with the extent of tissue damage.")
77
Clinical Features of Spinothalamic Lesions
Decrease in pain sensibility (hypalgesia or analgesia). Decrease in temperature sensibility. Increase in pain sensibility (hyperpathia or hyperalgesia).
. Decrease in temperature sensibility. Increase in pain sensibility (hyperpathia or hyperalgesia).")
78
Stress Analgesia Release of NE by sympathetic neurons
Stimulates release of Enk in spinal cord

79
Movement Analgesia Rhythmic movement releases 5-HT Gum chewing
Locomotion

80
Projected Pain Activation of nociceptive fibers anywhere along their course is felt (projected) as a pain in the peripheral distribution of the fibers. Examples: "to hit one's funny bone" or pain in the leg due to pressure on a spinal nerve at its entrance to the spinal cord.
 as a pain in the peripheral distribution of the fibers. Examples: to hit one s funny bone or pain in the leg due to pressure on a spinal nerve at its entrance to the spinal cord.")
81
Referred Pain Pain arising from disease of the viscera, but felt at a relatively distant superficial site. Referred pain appears in parts of the periphery supplied by the same segment of the spinal cord as the affected organ; referred pain occurs in the associated dermatome. It probably arises due to convergence of visceral nociceptive afferents (sympathetic afferents) and skin afferents onto the same dorsal horn neurons. Hyperpathia and reflex muscle spasms may also be present.
 and skin afferents onto the same dorsal horn neurons. Hyperpathia and reflex muscle spasms may also be present.")
82
Neuralgia "Spontaneous" pains arising in a root or nerve distribution due to relatively long-term damage (tension, pressure, crushing). An innocuous stimulus in the nerve distribution can elicit the pain, which is often severe. Examples: herpes zoster (shingles) infection, trigeminal neuralgia.
. An innocuous stimulus in the nerve distribution can elicit the pain, which is often severe. Examples: herpes zoster (shingles) infection, trigeminal neuralgia.")
83
Causalgia "Spontaneous" pains arising in a nerve or root distribution following rapid, violent injury to a nerve, such as due to a bullet wound. Probably due to a disorder of sensory processing. Example: anesthesia dolorosa (tactile anesthesia with intense pain in the affected area).
.")
84
Phantom Limb Pain Burning, shooting, or crushing pains may be experienced in the missing part following amputation. When triggered from the stump, they may be a type of neuroma pain. In other cases, a disorder of central processing is implicated.

85
Stress-Related “Tight” Muscle Pain
Sympathetic neurons release NE Skeletal muscle spindles stimulated Increased neuronal activity in m. spindles Increased tension (tone) of muscles Decreased blood flow to skeletal muscles Ischemia-induced pain (release of LA, BK, K+, H+, etc. in skeletal muscle)
 of muscles. Decreased blood flow to skeletal muscles. Ischemia-induced pain (release of LA, BK, K+, H+, etc. in skeletal muscle)")
86
Modulation of Pain by Mesolimbic Pathways
Substantia nigra (SN) releases dopamine (DA) DA is reward (pleasure) molecule in nucleus accumbens and elevates mood DA stimulates release of serotonin which in turn stimulates release of enkephalins and endorphins in hypothalamus and raises pain threshold Enkephalin and endorphins share Glu-Gly-Gly-Phe-Met or –Leu pentapeptide sequence. Enkephalin response is lcoal and over in seconds but endorphins circulate in blood for hours Raphe nuclei release serotonin (5-HT) and release enkephalin in spinal cord, raises pain threshold LC releases norepinephrine (NE) and also raises pain threshold
 releases dopamine (DA) DA is reward (pleasure) molecule in nucleus accumbens and elevates mood. DA stimulates release of serotonin which in turn stimulates release of enkephalins and endorphins in hypothalamus and raises pain threshold. Enkephalin and endorphins share Glu-Gly-Gly-Phe-Met or –Leu pentapeptide sequence. Enkephalin response is lcoal and over in seconds but endorphins circulate in blood for hours. Raphe nuclei release serotonin (5-HT) and release enkephalin in spinal cord, raises pain threshold. LC releases norepinephrine (NE) and also raises pain threshold.")
87
Role of LC and Norepinephrine
LC release of NE in spinal cord raises pain threshold by unknown mechanism Local release of NE by sympathetic nerves at muscle spindles and damaged spinal neurons lowers pain threshold by an unknown mechanism Pain increases skeletal muscle tone and rigidity “Guarding” response to visceral pain Sympathetic innervation of muscle spindles may tighten skeletal muscles and constrict blood vessels, decreasing blood flow to muscles, producing ischemia/hypoxia and release of lactic acid (anaerobic metabolism). Lactic acid stimulates nociceptors. Release of NE by LC neurons projecting to cortex stimulates wakefulness and inhibits sleep (alerting response)
. Lactic acid stimulates nociceptors. Release of NE by LC neurons projecting to cortex stimulates wakefulness and inhibits sleep (alerting response)")
88
Role of Raphe and 5-HT 5-HT release by raphe in dorsal horn raises pain threshold by releasing enkephalin 5-HT release by DA from NA releases enk in hypothalamus 5-HT release stimulates limbic system (Hallucinogen LSD is a 5-HT receptor agonist/antagonist) 5-HT release in cortex stimulates wakefulness and inhibits sleep (alerting response)
 5-HT release in cortex stimulates wakefulness and inhibits sleep (alerting response)")
89
Stress and Nociception Anti-stress and Anti-nociception
LC stimulates release of DA in NA LC stimulates hypothalamus to release CRH, ACTH from pituitary and cortisol from adrenal cortex DA in PFC stimulates executive decisions (start vs. stop, right vs. wrong) DA from NA stimulates 5-HT which releases enk in hypothalamus and raises pain threshold DA is anti-stress molecule; DA decreases release of CRH, ACTH and cortisol Cortisol level is a physiological index of stress Popularized by anti-cortisol dietary supplements to reduce belly fat Relacor
 DA from NA stimulates 5-HT which releases enk in hypothalamus and raises pain threshold. DA is anti-stress molecule; DA decreases release of CRH, ACTH and cortisol. Cortisol level is a physiological index of stress. Popularized by anti-cortisol dietary supplements to reduce belly fat. Relacor.")
90
Stress and Pain Stress response releases DA, 5-HT, NE and enkephalin, raises pain threshold (anti-nociception) Stress response also increases CRH, ACTH and cortisol Depression is a stress that decreases release of DA, 5-HT and enkephalin, lowers pain threshold (nociception) and increases CRH, ACTH and cortisol (stress hormones) Opiates and other addictive drugs inhibit stress response and raise pain threshold (anti-nociception), decreasing stress responsiveness
 and increases CRH, ACTH and cortisol (stress hormones) Opiates and other addictive drugs inhibit stress response and raise pain threshold (anti-nociception), decreasing stress responsiveness.")
91
Clinical Problem Ian is a 17 year-old male who was brought to the ER by ambulance after smoking marijuana in the basement of his friend’s house. Ian ran up the stairs to get away when he heard his friend’s parents return home and hit his head on a low overhanging wooden supporting beam. Ian fell down one flight of stairs and believes that he lost consciousness for a few seconds. This was followed by numbness in his right arm and fingers. He regained sensation in the ambulance and experienced intense pain in his right limb and shoulder during movement. Removal of his shirt for examination was intensely painful and accompanied by shouting and cursing. Because of this, his shirt remains off and he screams in pain every time someone enters his room.

92
Complex Regional Pain Syndrome: The Angry Axon Reflex

95
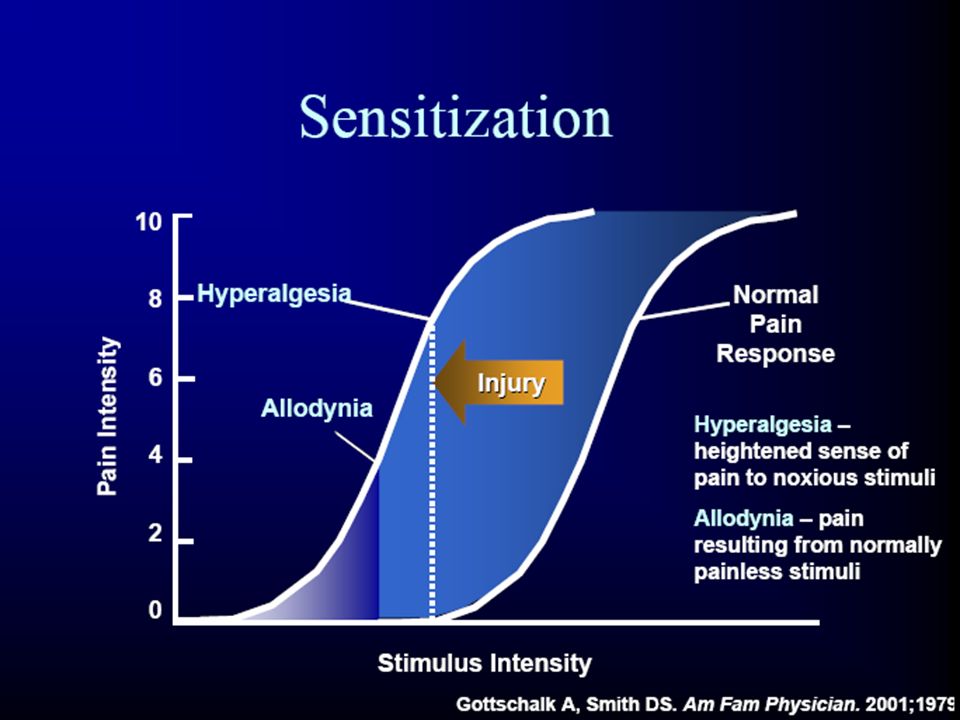
Hyperalgesia vs Allodynia
Pain to stroking stimuli A-beta fiber mediated Decreases with ischemic block Hyperalgesia Pain to punctate stimuli (von Frey) A-delta and C-fiber mediated Persists with ischemic block
 A-delta and C-fiber mediated. Persists with ischemic block.")
99
Case Study #2 (Question)
The pain this patient experienced is due to Excitation of nociceptors Excitation of medium- and large-diameter sensory nerve fibers Excitation of small-diameter myelinated and unmyelinated sensory nerve fibers Pressure on a dorsal root More than one but not all of the above

100
Case Study #2 (Answer) Two of the statements are true. The pain is caused by pressure on a dorsal root. The pressure causes excitation of small-diameter GIII and GIV primary afferent fibers within the dorsal root. Their activity leads to the perception of pain and their peripheral terminals, the nociceptors themselves, are not being excited by a noxious stimulus. (Law of Projection).
.")
101
Case Study #2 (Question)
Does the patient’s localization of pain indicate the site of the injury? A. No, the injury was distant from the pain B. No, the injury was on the opposite side B. Yes, the injury was in the vicinity C. Yes, the injury was to the jaw muscle

102
Spinal tract of CNV (Trigeminal Analog of STT)
Spinal tract of CNV descends and crosses in medulla and cervical spinal cord Learning Objectives: Memorize the structures and functions of the spinothalamic somatosensory systems. Shortcut to ovation

103
–Lewis Carroll, Alice’s Adventures in Wonderland
Alice, speaking to the Cheshire Cat: “Would you tell me, please, which way I ought to go from here?” “That depends a good deal on where you want to get to,” said the Cat. “I don’t much care where,” said Alice. “Then it doesn’t matter which way you go,” said the Cat. “–so long as I get somewhere,” Alice added as an explanation. “Oh, you’re sure to do that,” said the Cat, “if you only walk long enough.”

Similar presentations












 is a potential receptive.>")




 respond differently to pain than.>")



 Proprioception (joint position and movement senses) Pain.>")

 Introduction –Adrian’s work on sensory coding –Spinal cord and dorsal root ganglia.>")

>")




