Download presentation
Presentation is loading. Please wait.

1
A Safer Approach to Chronic Pain Management Tom Wroth MD, MPH Jerry McKee Pharm.D., M.S., BCPP NCCHCA Annual Conference Asheville, NC June 23, 2012

2
Objectives At the completion of this discussion, attendees will be able to Understand the need for practices to approach chronic pain management in a systematic way Understand the scope and clinical significance of chronic pain management issues nationally and in North Carolina Describe the CCNC chronic pain initiative and its goals Relate how specific practice level interventions can successfully and appropriately address the needs of chronic pain patients

3
Chronic Pain Chronic pain is defined as persistent pain, which can be either continuous or recurrent and of sufficient duration and intensity to adversely affect a patient's well-being, level of function, and quality of life. (Wisconsin Medical Society Task Force on Pain Mgt, 2004)
.")
4
Why Should Health Centers Focus on Chronic Pain? Common medical problem in the community –~10% of adults –Leads to significant disability Increased prevalence in health center populations (Medicaid, Medicare, Uninsured) Co-morbid chronic conditions: DM, CAD, HTN, Depression Changing epidemiology of accidental overdose
 Co-morbid chronic conditions: DM, CAD, HTN, Depression Changing epidemiology of accidental overdose.")
5
Why Should Health Centers Focus on Chronic Pain? Source of burnout and frustration for providers and staff Source or RISK for practices –Medical licensure and privileging –Medico-legal risk: accidental overdose We are a Patient Centered Medical Home –Team based care –Collaborative care model

6
The Challenge: There is not enough time… With a typical panel of primary care patients- 10.6 hours per day for chronic disease care 7.4 hours per day for preventive care 4.6 hours per day for acute care Chronic pain management requires time and teamwork

7
Challenges: Clinicians can Foster Misuse Confrontation phobia –Fear of damaging physician-patient relationship –Trouble saying “No” –Not skilled in discussing addiction Enabling behaviors –Physicians desire to relieve distress/pain

8
Chronic Pain and Co- Morbidities Depression – Prevalence of 35-50% Anxiety – increased prevalence –Associated with avoidant coping pattern Substance abuse – increased prevalence Sleep Disorders –Lack of restorative sleep perpetuates chronic pain and reduces function Personality disorders Hx of childhood abuse

9
Definitions Misuse-use for purpose other than intended (get high) Abuse- harmful use of a drug (drinking and driving) Tolerance-body adapts to a certain dose such that more is needed to achieve the same effect Physical Dependance- withdrawal occurs when substance is stopped Addiction-behavioral term- denotes psychological dependence, compulsive use, for reasons other than therapeutic use
 Abuse- harmful use of a drug (drinking and driving) Tolerance-body adapts to a certain dose such that more is needed to achieve the same effect Physical Dependance- withdrawal occurs when substance is stopped Addiction-behavioral term- denotes psychological dependence, compulsive use, for reasons other than therapeutic use")
10
How Prevalent is Misuse? Total Pain Population Aberrant behavior 40% Abuse 20% Addiction 2-5%

11
US Prescription Overdoses

12
CDC Vital Statistics, Nov 2011 15,000 deaths annually In 2010, 1 in 20 used pain killers for nonmedical purposes Enough prescription painkillers were prescribed in 2010 to medicate every American adult around-the-clock for a month.

13
Drug overdose death rate --- United States, 2008 Source: Len Paulozzi, CDC Nov. 2011

14
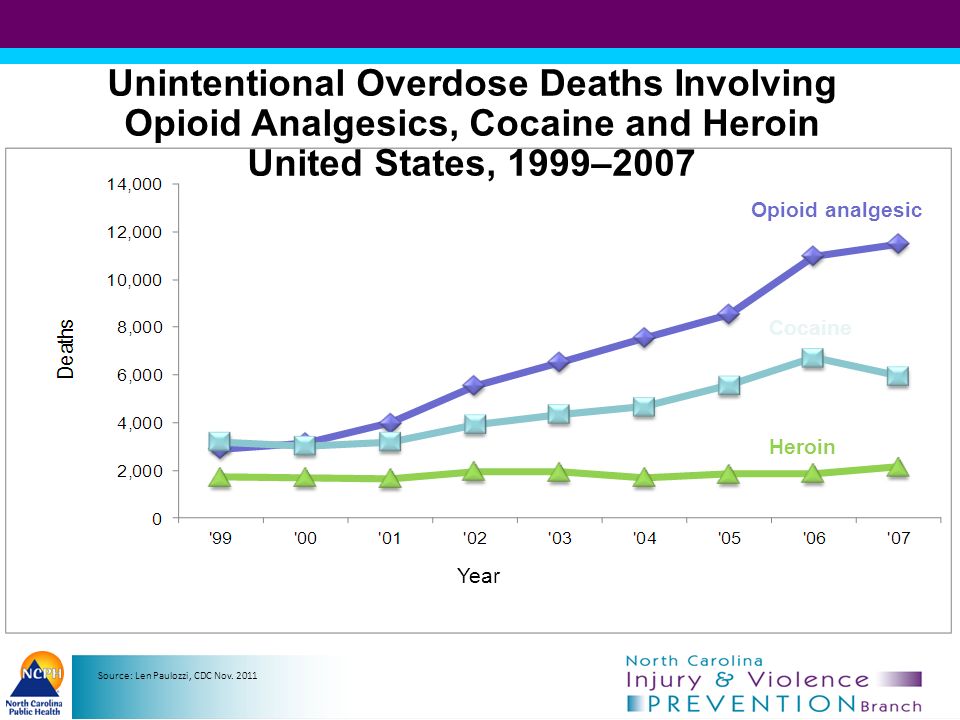
14 Unintentional Overdose Deaths Involving Opioid Analgesics, Cocaine and Heroin United States, 1999–2007 Opioid analgesic Cocaine Heroin National Vital Statistics System, http://wonder.cdc.gov, multiple cause dataset Year Source: Len Paulozzi, CDC Nov. 2011
15
Unintentional drug overdose death rates and total sales of opioid analgesics in morphine equivalents by year in the U.S. Source: Len Paulozzi, CDC Nov. 2011

16
North Carolina Poisonings

17
Source: NC State Center for Health Statistics, Death file 2010; Analysis by Injury Epidemiology and Surveillance Unit Leading Causes of Injury Deaths (by Number of Deaths, All Ages, North Carolina Residents: 2010) Unintentional Motor Vehicle Crashes Suicides Unintentional Poisoning Unintentional Falls Homicides Unintentional Suffocation Unintentional Drowning Total Deaths = 5,983 * Unintentional Other and Unintentional Unspecified are two separate categories. Other comprises several smaller defined causes of death, while Unspecified refers to unintentional deaths that were not categorized due to coding challenges. Unintentional, Other & Unspecified*

18
Unintentional Poisoning Deaths by County: N.C., 1999-2009 Source: N.C. State Center for Health Statistics, Vital Statistics-Deaths, 1999-2009 Analysis by Injury Epidemiology and Surveillance Unit

19
Source: Farhad Modarai¹, Karin Mack¹, Leonard Paulozzi¹, Scott K. Proescholdbell² Data Source: ARCOS Data

20
Mortality Rates of Unintentional and Undetermined Opioid Overdoses and Dispensation Rates of Opioid Analgesics*: North Carolina Residents, 2009 *Source: Mortality data: State Center for Health Statistics, NC Division of Public Health, 2009 Population data: National Center for Health Statistics, 2009 Prescription dispensation data: Controlled Substances Reporting System, 2009 Analysis: KJ Harmon, Injury Epidemiology and Surveillance Unit, Injury and Violence Prevention Branch,, NC Division of Public Health

21
Number of Times in which a Drug was Mentioned as a Cause of Death: N.C., 2010* Source: N.C. State Center for Health Statistics, Vital Statistics-Deaths, 2010 Analysis by Injury Epidemiology and Surveillance Unit *Categories are not mutually exclusive †Includes licit drugs that are misused/abused

22
By combining prescription records with toxicology data, we were able to get an idea of how many cases had a prescription for the drug(s) that contributed to their death. Combining CSRS and OCME data Number of cases Deaths per drug

23
Chronic Pain Initiative CCNC and Project Lazarus: Chronic Pain and Community Initiative

24
A set of inter-related programs designed to improve the medical care received by chronic pain patients, and in the process, to reduce the misuse, abuse, potential for diversion and overdose from opioid medication. Key program components: ClinicalCommunity Focus Primary Care Physician ToolkitTake only your own medications Emergency Department ToolkitKeep medications in a safe place Care Management ToolkitEducation on dangers of opioids Network CPI Champion What is the Chronic Pain Initiative? Model is based on proper assessment, diagnosis, and treatment plan with Pain agreement as necessary

25
Community Care of North Carolina (CCNC), in conjunction with non-profit organization Project Lazarus, is responding to some of the highest drug overdose death rates in the country through its Chronic Pain Initiative (CPI). Goals Reduce opioid-related overdoses Optimize treatment of chronic pain Manage substance abuse issues (opioids)
.")
26
Project Lazarus/Chronic Pain Initiative Model Community Awareness Epidemiologic Surveillance Overdose Prevention and Diversion Control Program Evaluation Overdose Rescue

27
Source: Wilkes Co. Health Department; NC SCHS; CDC Wonder Project Lazarus. First Site – Wilkes County. Accidental poisoning deaths decrease by more than 65% after start-up

28
Wilkes Recipients of Opioids*: As deaths go down, patients continue to get their pain medication Source: NC CSRS and Project Lazarus

29
Project Lazarus Expands: in 2012 joins North Carolina’s Medicaid Authority (CCNC) for statewide implementation Project Lazarus – Strategies to community coalitions Chronic Pain Initiative – Strategies to health care providers Community awarenessProvider education Coalition formation and developmentED policy change Diversion controlExpanded access to drug treatment Pain patient supportPatient risk reduction
 for statewide implementation Project Lazarus – Strategies to community coalitions Chronic Pain Initiative – Strategies to health care providers Community awarenessProvider education Coalition formation and developmentED policy change Diversion controlExpanded access to drug treatment Pain patient supportPatient risk reduction")
30
Why are we looking at replication? Evidence exists that the Wilkes County approach is changing conditions in ways that will reduce misuse, abuse, diversion and overdose from prescription opioids. Changes in how medical professionals manage chronic pain patients and monitor their prescription use. Change in policy and practice within ED of Wilkes Regional Medical Center Increased access to Naloxone and understanding of when and how to use Pill take-back days Community awareness, coalition building for community education Reduction in unintentional poisoning deaths, especially those stemming from narcotics prescribed by providers based in Wilkes County

31
Cost of Hospitalizations for Unintentional Poisonings: NC, 2008 Average cost of inpatient hospitalizations for an opioid poisoning*: $16,970. Number of hospitalizations for unintentional and undetermined intent poisonings**: 5,833 Estimated costs in 2008: $98,986,010 Does not include costs for hospitalized substance abuse *Agency for Healthcare Research and Quality ** NC State Center for Health Statistics, data analyzed and prepared by K. Harmon, Injury and Violence Prevention Branch, DPH, 01_19_2011 Prepared by Project Lazarus through an unrestricted educational grant from Purdue Pharma LP: NED101356

32
Key Ingredients in Chronic Pain Initiative Establishment (or prior existence) of a community coalition that is able to develop and implement effective strategies to reduce substance use A sense of urgency among local actors who have influence Dedicated manager of the coalition with skills in process and content Appropriate strategy for achieving a change in prevailing medical practice re: treatment of chronic pain patients (PCP and ED locations) Tailored to local conditions Includes education on the extent of the problem in the community and the role of providers in limiting supply and opportunities for diversion Includes useful tools that providers can adopt (e.g., Medication Agreements, guidelines for proper script writing) Explicit recommendations for hospital policies that limit dispensing of narcotics (especially to ED patients) Take advantage of leverage points in larger environment (e.g., CSRS, Medicaid lock-in policy)
 of a community coalition that is able to develop and implement effective strategies to reduce substance use A sense of urgency among local actors who have influence Dedicated manager of the coalition with skills in process and content Appropriate strategy for achieving a change in prevailing medical practice re: treatment of chronic pain patients (PCP and ED locations) Tailored to local conditions Includes education on the extent of the problem in the community and the role of providers in limiting supply and opportunities for diversion Includes useful tools that providers can adopt (e.g., Medication Agreements, guidelines for proper script writing) Explicit recommendations for hospital policies that limit dispensing of narcotics (especially to ED patients) Take advantage of leverage points in larger environment (e.g., CSRS, Medicaid lock-in policy) ")
33
Key Ingredients in Chronic Pain Initiative Makes effective use of various partners in carrying out strategies including but not limited to: Public health department – multiple strategies County Medical Director – to reach physicians and ED Medical providers – to change their own practice and educate other providers Pharmacist – to other pharmacies in community Law enforcement Schools Behavioral Health, Prevention and Treatment Programs and Organizations

34
Can coalitions help reduce Rx drug abuse? Counties with coalitions had 6.2% lower rate of ED visits for substance abuse than counties with no coalitions (but this could be due to random chance) However, counties with a coalition where the health department was the lead agency had a statistically significant 23% lower rate of ED visits (X 2 =2.15, p=0.03) than other counties In counties with coalitions 1.7% more residents received opioids than in counties without a coalition. Coalitions may be useful in reducing the harms of Rx drug abuse while improving access to pain medications at the same time. More professional coalitions may have a greater impact on reducing Rx drug harms. Data Sources: NC Health Directors Survey, NC DETECT (2010), CSRS (2008-2010)
 However, counties with a coalition where the health department was the lead agency had a statistically significant 23% lower rate of ED visits (X 2 =2.15, p=0.03) than other counties In counties with coalitions 1.7% more residents received opioids than in counties without a coalition. Coalitions may be useful in reducing the harms of Rx drug abuse while improving access to pain medications at the same time. More professional coalitions may have a greater impact on reducing Rx drug harms. Data Sources: NC Health Directors Survey, NC DETECT (2010), CSRS ( ).")
35
Contents of the Toolkit General information Managing chronic pain Proper prescription writing Precautions Tools for managing chronic pain patients Universal Precaution for Prescribing and Algorithm for assessing and managing pain Pain Treatment Agreement Format for progress notes Medication flowsheet Personal care plan Prescriber and Patient education materials Screening Forms and Brief Intervention Naloxone Prescribing Controlled Substance Reporting System (CSRS)
")
36
Primary Care Tool Kit Physician toolkit for treating chronic pain patients Encourage the use of Pain Treatment Agreements with chronic pain patients Encourage use of Provider Portal Encourage use of Controlled Substance Reporting System (CSRS) Encourage the assignment of pharmacy home for chronic pain patients- lock-in program
 Encourage the assignment of pharmacy home for chronic pain patients- lock-in program")
37
Emergency Department Tool Kit Care management for pain patients visiting ED ED policy that restricts the dispensing of narcotics Encourage the Use of the CSRS by ED physicians Encourage the Use of Provider Portal in the ED Identify Chronic Pain Patients and Refer for Care Coordination based on ED assessment

38
Care Management Tool Kit Provide support to ED identification of chronic pain patients- referrals to PCP or specialty services Provide care management for patients identified by PCP practice as CPI patient; consider pharmacy lock-in program Ongoing care management for Medicaid patients with narcotic prescriptions above threshold pain patients via TREO data Educate PCPs and providers in utilization of Chronic Pain Tool Kit

39
Emergency Department Policy Non-narcotic pain medication for “frequent fliers.” Prescriptions for narcotic or sedating medications that have been lost, stolen or expired will not be refilled in the Emergency Department Referrals to Primary Care Providers Accepting New Patients. Prescriptions necessary only in limited quantities North Carolina Controlled Substances Reporting System, checked for any prescription for a controlled substance

40
Contact Dr. Mike Lancaster mlancaster@n3cn.org mlancaster@n3cn.org Fred Wells Brason II fbrason@projectlazarus.org fbrason@projectlazarus.org www.communitycarenc.org www.communitycarenc.org www.projectlazarus.org www.projectlazarus.org

41
Controlled Substance Reporting System (CSRS)
")
42
Controlled Substances Reporting System NCGS 90-113.70-76 Passed in August 2005 Reporting began July 2007 Required all dispensers to report to a centralized data base Weekly reporting began 01/02/10

43
CSRS Data Overview Over 84,000,000 prescriptions in the database (started July 1, 2007) Approx. 17.5 million per year Over 2,750,000 queries have been made of the system Over 11,300 dispensers and practitioners currently registered to use the system Averaging 2,300 queries per day

44
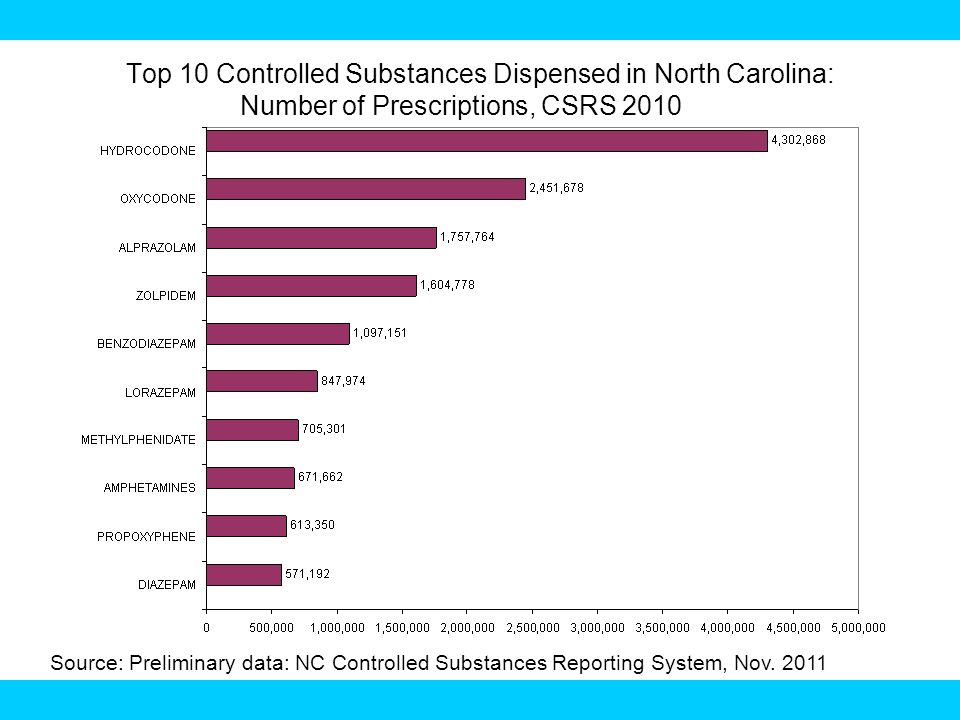
Top 10 Controlled Substances Dispensed in North Carolina: Number of Prescriptions, CSRS 2010 Source: Preliminary data: NC Controlled Substances Reporting System, Nov. 2011
45
Doctor Shopping*: Trends for Schedule II Patients with Multiple Prescribers and DispensersSource: NC CSRS *Based on number of prescribers AND number of pharmacies within each 6 month period for schedule II.

46
How to contact the CSRS www.nccsrs.org Call Bill Bronson, John Womble, or Devon Scott 919.733.1765 E-mail William.Bronson@William.Bronson@dhhs.nc.gov Johnny.Womble@Johnny.Womble@dhhs.nc.gov Devon.Scott@dhhs.nc.gov

47
Step-by-Step Approach to Improving Chronic Pain Management

49
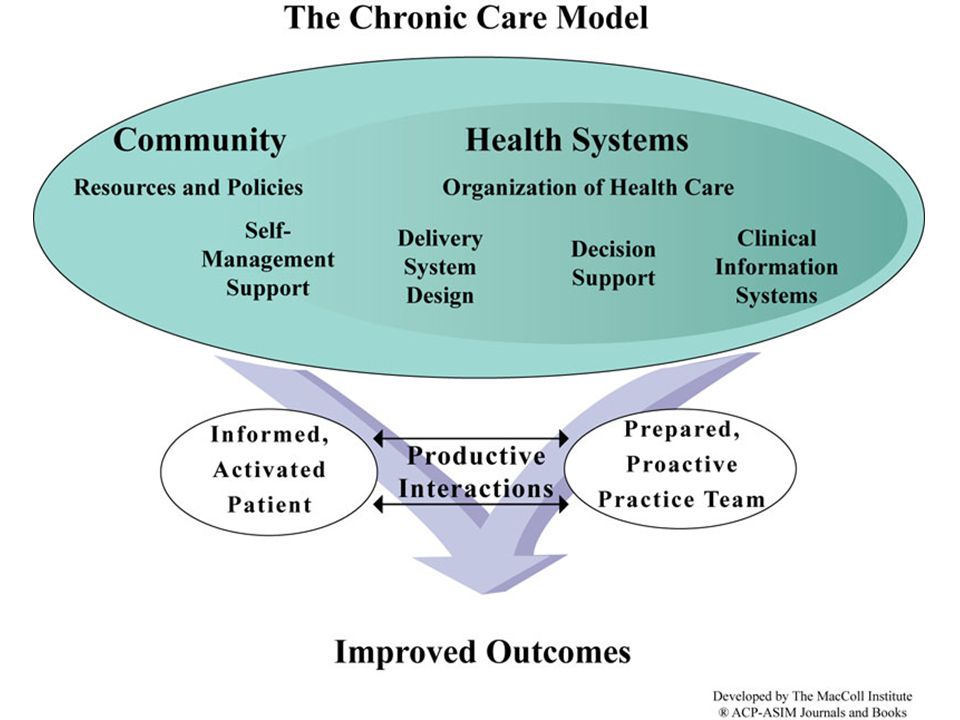
Principles of Chronic Disease Management Use clinical information systems to Identify the population Identify best practices and develop practice guidelines Create team based approach with defined roles Define measures that will reflect performance improvement and report back to team Develop tools to support self management

50
Step 1: Use Information Systems to Identify the Population Use EMR or practice management software query to identify the number of patients with chronic pain –Chronic Pain Syndrome – 338.4, back pain, headache, neck pain, fibromyalgia *ICSI Guideline –Encourage providers to code 338.4 in addition to specific diagnosis –Look at # patients per provider or practice to identify your hot spots

51
Identify the Population: Chronic Pain on Problem List

52
One Center has a high prevalence of opioid prescribing

53
Step 2: Identify Best Practices Start a workgroup with a clinical champion Identify practice guidelines –North Carolina Medical Board –Institute for Clinical Systems Improvement –Specialty societies: AAFP –Washington Medical Directors Group

54
The NC Medical Board Position statement 2008 2010: 30% of NCMB infractions were due to improper prescribing Medical board advises: –Clear documentation of history and physical, review of records, documentation of prescriptions, response to treatment, clear indication for treatment –Use of practice safeguards (contracts, UDS, CSRS) –Identifying high risk patients and referring as necessary (pain management or substance abuse) –Identifying “red flags”
 –Identifying high risk patients and referring as necessary (pain management or substance abuse) –Identifying red flags")
55
Guidelines Institute for Clinical Systems Improvement (ICSI) –Healthcare Guideline: Assessment and Management of Chronic Pain, 2011 Washington State Medical Directors: –Interagency Guidelines on Opioid Dosing for Chronic Pain, 2010 American Pain Society –Guidelines for the Use of Opioid Therapy in Patients with Chronic Pain, 2009
 –Healthcare Guideline: Assessment and Management of Chronic Pain, 2011 Washington State Medical Directors: –Interagency Guidelines on Opioid Dosing for Chronic Pain, 2010 American Pain Society –Guidelines for the Use of Opioid Therapy in Patients with Chronic Pain, 2009")
56
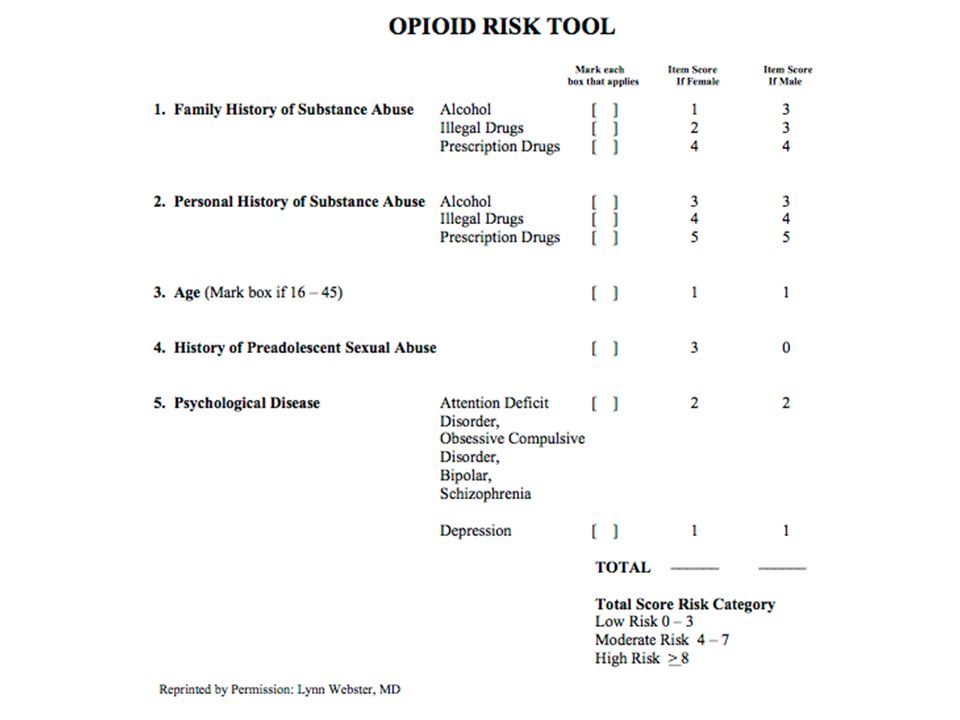
Step 2: Identify Best Practices Assessment: –Functional assessment- SF-36 –Risk for Misuse Opioid Risk Tool DIRE, COMM, SOAP Baseline Urine Drug Screen NC Controlled Substance Reporting System Department of Corrections Website –Depression and Substance Abuse Screen PHQ9, CAGE

58
Decision Support Risk Assessment, Depression Screen, NC CSRS, UDS, Pain Contract

60
Step 2: Identify Best Practices Management –Treatment agreement –Safe opioid prescribing < 100 mg MED, Drug combinations –Monitoring High Risk Patients Urine Drug Screen NC CSRS –Guidelines for referral to Pain management Substance Abuse Mental Health

62
“Rational Prescribing Practices” Framework for prescribing medications with abuse potential Have a clear clinical indication Assess risk using validated tools Establish therapeutic agreement Monitor and assess regularly Document appropriately Be willing to intervene Flinch JW, Prmary Care Clinics of N America, 1993

63
Step 3: Create a “Care Pathway” that Uses a Team Based Care Approach Provider –Code Chronic Pain 338.4 –Excellent documentation of assessment and management –Management decisions Start, Continue, or Stop opioids Referral Safe opioid prescribing –Identify high risk patients for monitoring

64
Step 3: Care Pathway Nursing: –Obtain Urine Drug Screen at defined intervals –PHQ9, Functional Assessment Tool Nursing/Care Management/Pharmacy –Opioid Risk Tool –NC CSRS report to provider (must be done by pharmacist or provider) –Department of Corrections report to provider Quality/Administration: Quality data reporting and feedback
 –Department of Corrections report to provider Quality/Administration: Quality data reporting and feedback")
65
Use Tools to Identify Gaps in Care Decision Support: ‘What needs to be done’

66
Step 3: Define measures that will reflect performance improvement and report back to team How do you know if you are improving care? –% patients on opioids with risk assesment (ORT or PHQ9) –% patients on opioids with pain management agreement –% patients on opioids with Urine Drug Screen in 12 months
 –% patients on opioids with pain management agreement –% patients on opioids with Urine Drug Screen in 12 months.")
67
Incorporate Pain Measures into Quality Plan % Patients with Contract

68
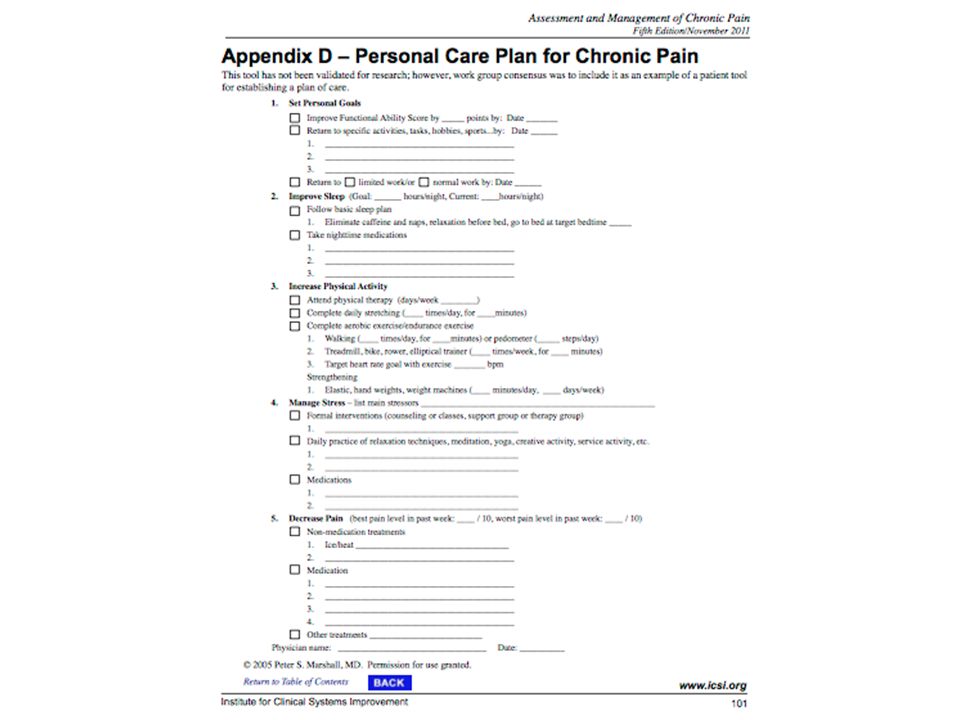
Step 4: Self Management Support Use “Collaborative Care Model” to develop written plan of care for patient –Set personal goals related to function –Improve sleep –Increase physical activity –Manage stress –Decrease pain »ICSI, Healthcare Guideline: Assessment and Management of Chronic Pain, 2011 Referral to community resources, cognitive behavior therapy, physical therapy, support groups

70
Step 5: Collaborate with Community Partners “It takes a village to take care of a chronic pain population’’ –CCNC Chronic Pain Initiative Use medical management committee to develop common guidelines Use CCNC care managers as referral source Meet with ER Physicians Identify suboxone providers Project Lazarus: Naloxone rescue initiative

71
Step 6: Collaborate with Pain Management Specialists Identify specialists in your area Share your guidelines for assessment, management, and referral Develop consultation relationships where information can be shared on high risk patients

72
PHS Pain Management Specialty Clinic 7 month experience with integrated pain management specialist –½ day every 2 weeks –Internal referrals of high risk patients with specific management questions –Goal of consultation Increase capacity of primary care provider to care for chronic pain patients Develop management plan Identify patients that would benefit from procedures or other referrals

73
PHS Pain Management Specialty Clinic Preliminary Results: –46 patients with average of 2.9 visits –Structured assessment and management protocols with care management support –Improved confidence and capacity in practice –Improved utilization of pain contracts, assessment tools –Decreased risk associated with aberrant patient behaviors

74
PHS Pain Management Specialty Clinic Functional assessment –Baseline SF-36 = 28.9 –Mean increase = 3.7 Depression –Mean PHQ9 = 12 –Mean change in PHQ 9 score = -5 Risk assessment –% with CSRS issue = 4.3% –% with unexpected findings on UDS = 32.6%

75
Conclusions There is a public health need for practices to improve management of chronic pain Team based care and care pathways can help providers improve care Practices should collaborate with community partners and specialists to help manage the population

76
76 Questions ?

Similar presentations







>")











