Download presentation
Presentation is loading. Please wait.

1
DURANOGLU Yasar; MD Akdeniz University Medical School Department of Ophthalmology Antalya/TURKEY 2012

2
The inferior oblique muscle is the shortest of all the eye muscles, being only 37 mm long. It arises in the anteroinferior angle of the bony orbit in a shallow depression in the orbital plate of the maxilla near the lateral edge of the entrance into the nasolacrimal canal.

3
The muscle continues from its origin backward, upward and laterally, passing between the floor of the orbit and the inferior rectus muscle. It inserts by a short tendon (1 to 2 mm) in the posterior and external aspect of the sclera.
 in the posterior and external aspect of the sclera..")
4
The width of the insertion varies widely (5 to 14 mm) and may be around 9mm on average.
 and may be around 9mm on average.")
5
Its anterior margin is about 10 mm behind the lower edge of the insertion of the lateral rectus muscle; its posterior end is 1 mm below and 1 to 2 mm in front of the macula. Near its insertion the posterior border of the muscle is related to the inferior vortex vein.

6
Unlike the other extraocular muscles the inferior oblique is almost wholly muscular.

7
Overaction of the inferior oblique muscle is manifested by overelevation of the adducted eye.

8
The term “primary overaction of the inferior oblique muscle” is used if it is not associated with the palsy of the contralateral superior rectus muscle or the palsy of the ipsilateral superior oblique muscle.

9
When upshoot in adduction is caused by an overaction of inferior oblique muscle and other possible causes have been ruled out, the treatment, when indicated, is surgical and consists of a weakening procedure of the overacting muscle.

10
Among the various weakening procedures of the inferior oblique muscle overaction, the most commonly performed techniques include myectomy, recession, denervation– extirpation, anterior transposition and disinsertion.

11
The most effective procedure remains controversial. A review of published reports revealed that each technique appeared the intended result but these investigators differed in their choices for reasons of simplicity, quickness and complications.

12
The criteria of a successful result were; 1-Correction of versions in adduction 2- Correction of hyperdeviation in the field of action of the inferior oblique 3- Correction of diplopia.

13
Clinical failure was defined as persistence of overaction of the inferior oblique muscle in adduction and persistence of hyperdeviation in primary gaze.

14
SURGICAL TECHNIQUE

16
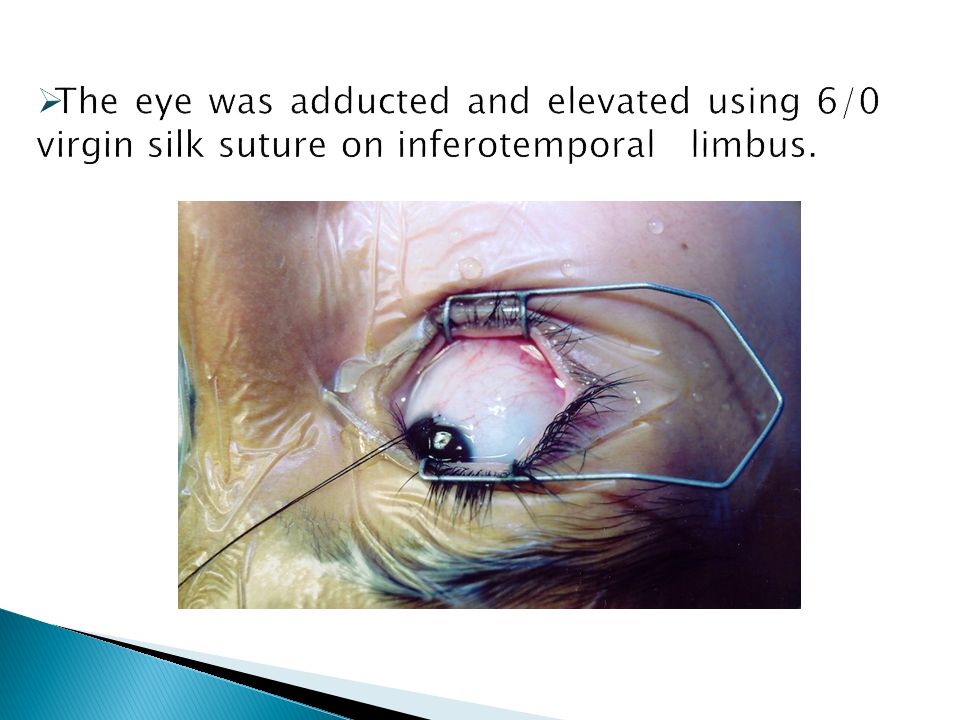
A fornix incision was performed in the same quadrant and eight millimetres away from the limbus. After passed to the subtenon space and visualized directly of the muscle fold, the tissue overlying of the inferior oblique muscle was pulled inferiorly using a Graefe hook.

23
Yaşar DURANOĞLU MD *, İclal YÜCEL MD*, Selda KIVRAKDAL, MD* *Akdeniz University School of Medicine Department of Ophthalmology Antalya – Turkey * Ann Ophthalmol (Skokie). 2006 Spring;38(1):29-33.
:")
24
In this paper, we compared of two different techniques for high score of the inferior oblique muscle overaction in the patients with infantile esotropia. Both techniques reduced the score of the overactive inferior oblique muscle, but eyes with disinsertion, distal muscle resection and tucking tended to be more effective.

25
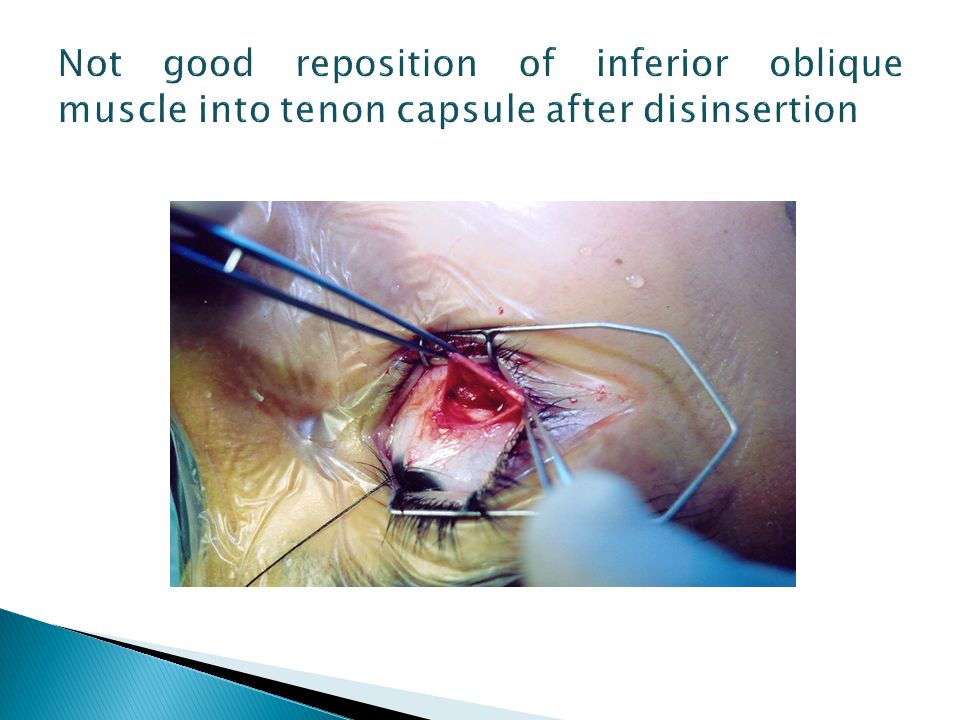
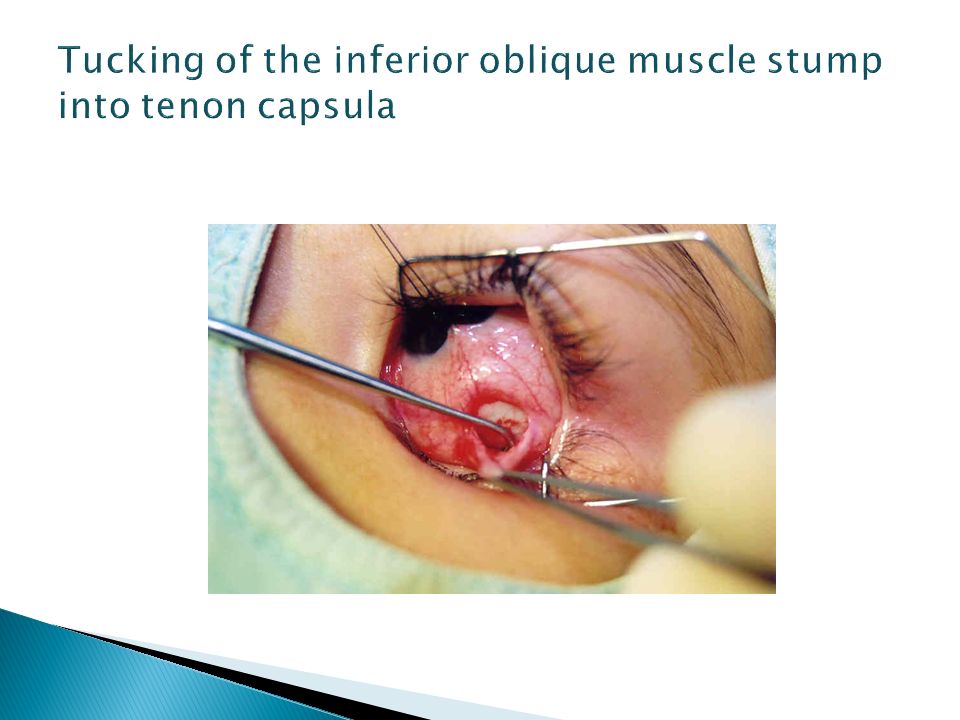
Tucking the muscle stump into tenon capsule was claimed to leave the muscles in a uniform position from the original insertion.

26
Leuder et al postulated that there was no correlation between outcome and the intraoperative behaviour of the inferior oblique muscle. They also suggested tucking of the inferior oblique muscle stump into Tenon's capsule. *Lueder GT; Tucking the inferior oblique muscle into tenon capsule following myectomy. J Pediatr Ophthalmol Strabismus 1988, 35:277-80.

27
Reattachment site of the inferior oblique muscle following disinsertion shows wide variations ranging from the original insertion site to other areas adjacent to lateral rectus or inferior rectus insertion. This wide variation of the reattachment site may be the cause of different surgical results with the same weakening procedures. * Wertz RD, Romano PE, Wright P; İnferior oblique myectomy, disinsertion and recession in rhesus monkeys. Arc Ophthalmol 1977; 95:857-60.

28
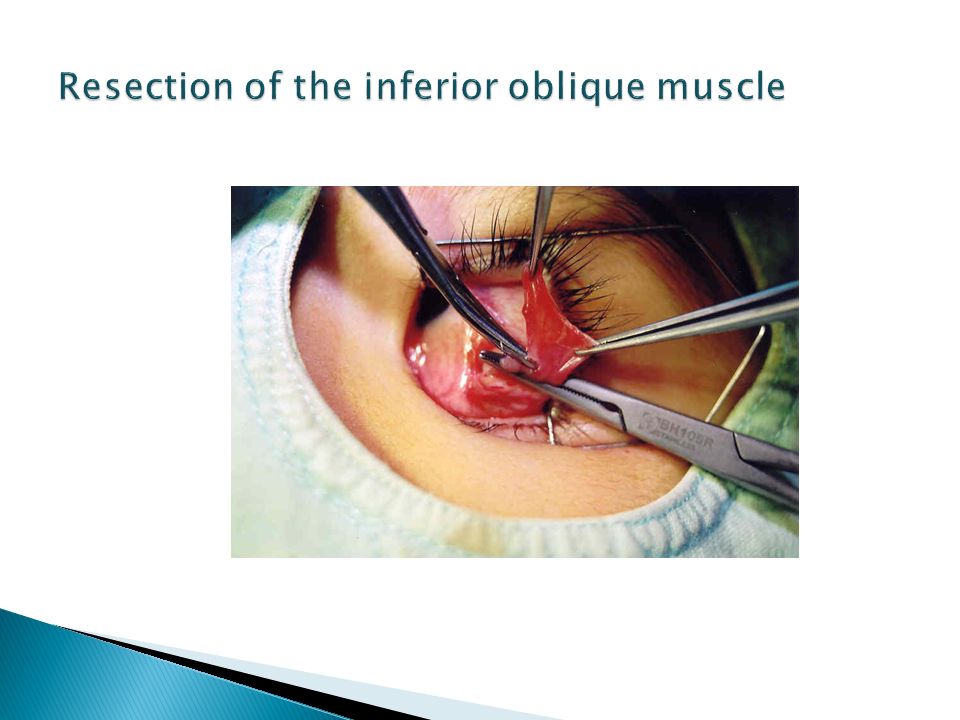
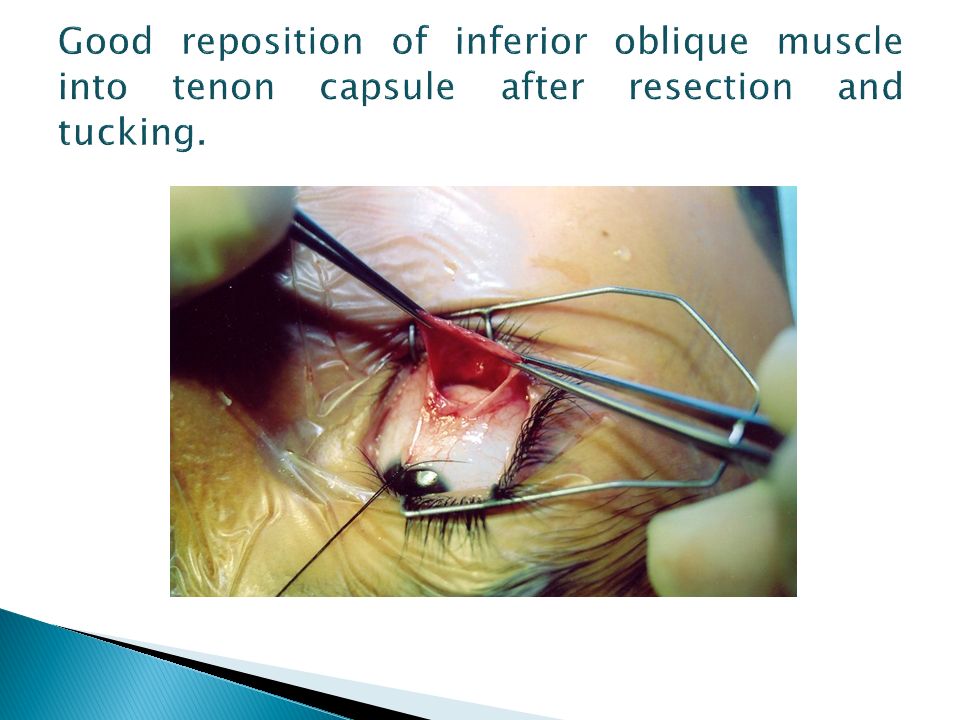
In our study, the stump of the inferior oblique muscle were resected and tucked into tenon capsule. For this reason, stable and complete reattachment to the right site can be occurred.

29
We have also found that inferior oblique muscle disinsertion-resection and tucking procedure is simple, safe, fast and effective weakening procedure with good results and may be preferred for cases with high degree of inferior oblique muscle action.

30
This procedure does not require the scleral sutures and being faster and simplier than the other weakening procedures. None of these patients have recurrent overaction of this muscle.

31
Effectiveness of Disinsertion–Resection and Tucking of the Inferior Oblique Muscle in Patients With Unilateral Long-Standing Superior Oblique Muscle Palsy Yasar Duranoglu, MD September/October 2007 Volume 44 · Issue 5

32
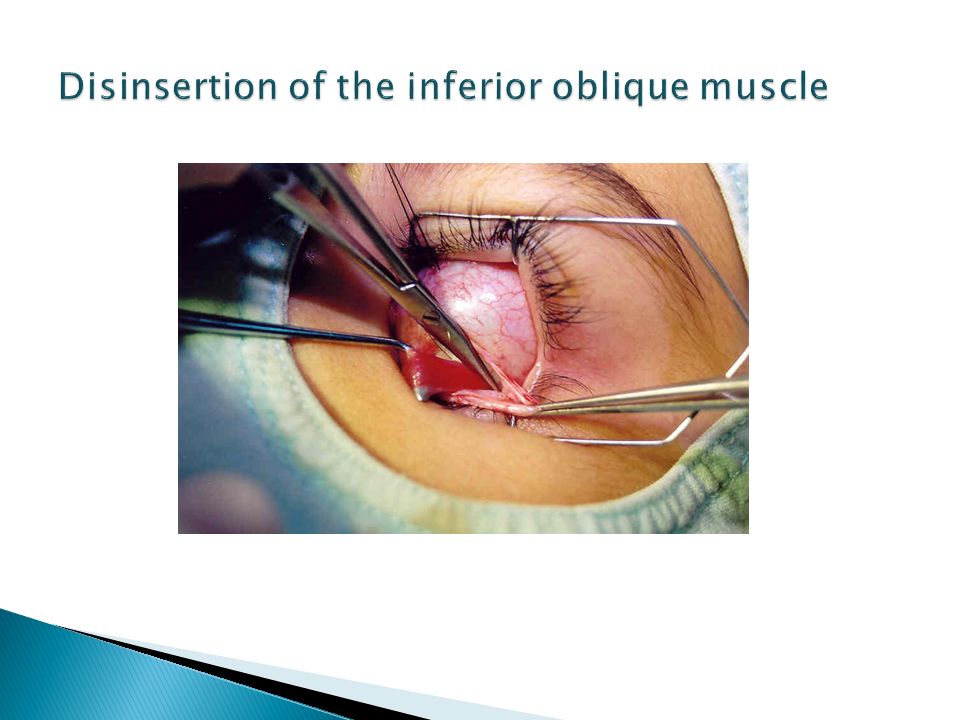
In this study the muscle was disinserted by Westcott Scissors. Four millimetres resection at the distal part of the muscle and tucking the muscle stump into tenon capsule were performed as the standard surgical procedure.

33
Mean vertical deviation was 15,9 (ranging from 12 to 17) prism dioptres (PD) preoperatively and 25 patient had no vertical deviation ( 80,6 %), 6 patient had average 3 PD residual but smaller hypertropia in primary position at last assessment.
 prism dioptres (PD) preoperatively and 25 patient had no vertical deviation ( 80,6 %), 6 patient had average 3 PD residual but smaller hypertropia in primary position at last assessment.")
34
The most common features were diplopia in 25 patient (80,6 %) and Abnormal Head Position in 28 patient (90,3 %) tilting toward the unaffected site.
 and Abnormal Head Position in 28 patient (90,3 %) tilting toward the unaffected site.")
35
Satisfactory outcome was defined as resolution of diplopia/visual symptoms or acceptable reduction/elimination of Abnormal Head Position. Satisfactory outcome was achieved following surgery in 26 (83,8 %) patient.
 patient..")
36
No patient had hypotropia in primary position. In addition no patient had elevation deficiency or lower lid elevation. Unilateral inferior oblique muscle weakening surgical procedures often lead to the appearance of inferior oblique muscle overaction the contralateral eye. In this study no patients had clinical evidence of contralateral inferior oblique muscle overaction pre- and postoperatively.

37
Although more experience would be needed to evaluate long term results, we concluded that the disinsertion-resection and tucking procedure of the inferior oblique muscle was safe, simple and effective in eliminating IOMO and AHP, as well as reducing the hyperdeviation in the patients with ULSSOMP.

Similar presentations

, Mc Nab A (2), Ben Simon G (2), Kowal L (2). 1-Hadassah.>")
 Sutures>")
To improve function and apperance 2)To (may) relieve asthenopia and double vision 4)To restore.>")





 Journal of American Association for Peadiatric Ophthalmology and strabismus 2008.>")










