Download presentation
Presentation is loading. Please wait.

1
Mr James Campbell FRCOG

2
Background - Menstrual disorders
1 in 20 women aged present to their GP per year £ 7 million (!) is spent per year on primary care prescriptions One of the most common reasons for specialist referral Accounting for a third of gynaecological outpatient workload
 is spent per year on primary care prescriptions. One of the most common reasons for specialist referral. Accounting for a third of gynaecological outpatient workload.")
3
Heavy menstrual bleeding (HMB)
Major impact on health-related quality of life 22% of otherwise healthy women Major problem in public health significant cost invasive treatments 12% of all specialist referrals Main presenting symptom for half of the hysterectomies performed in the UK Vessey M et al. The epidemiology of hysterectomy: findings of a large cohort study. Br J Obstet Gynaecol 1992; 99;

4
Increasing prevalence
More periods per lifetime Earlier menarche Increased life expectancy Ability to regulate fertility Less time spent breastfeeding More demanding lifestyles and reduced tolerance of troublesome periods

5
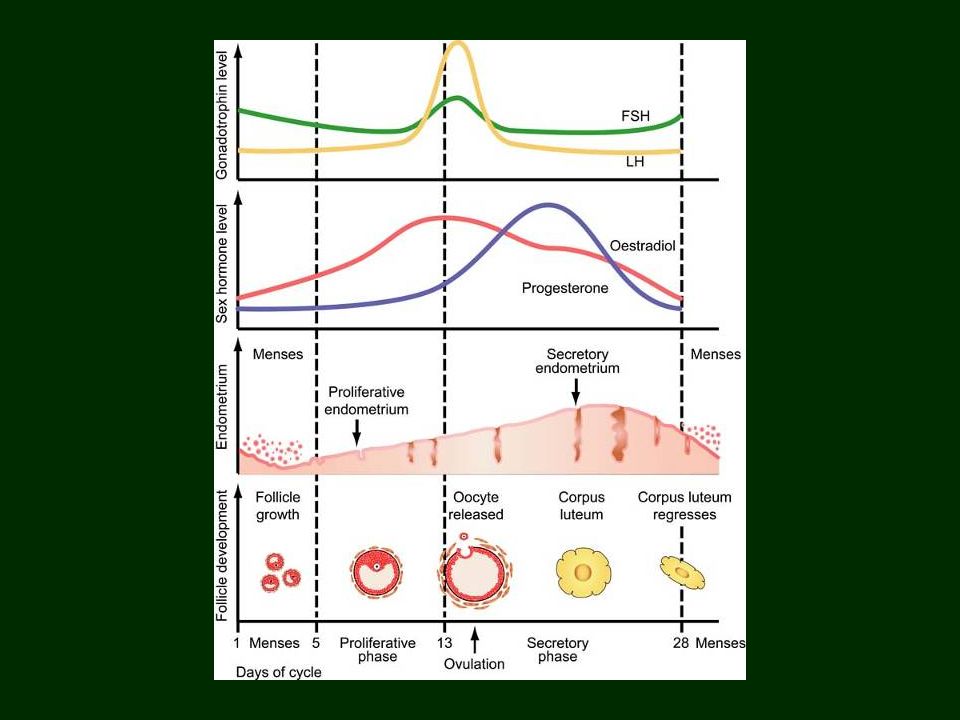
Menstruation Shedding of the superficial layers of the endometrium
following the withdrawal of ovarian steroids

14
Normal menstruation Menarche - 13 years Menopause - 51 years
Regular cycles – 5 / 28 Menstrual loss – 40ml (<80ml) Pelvic discomfort
 Pelvic discomfort.")
15
Menstrual disorders Heavy menstrual bleeding (HMB)
Intermenstrual / Postcoital bleeding Dysmenorrhoea = ‘painful periods’ Premenstrual tension (PMT) Post-menopausal bleeding Oligo- or Amenorrhoea
 Post-menopausal bleeding. Oligo- or Amenorrhoea.")
16
HMB - Etiology Endometrial origin Uterine / pelvic pathology
Increased fibrinolysis and prostaglandins Uterine / pelvic pathology Fibroids / Polyps Pelvic infection (Chlamydia) Endometrial or cervical malignancy Medical disorders Coagulopathy / Thyroid disease / Endocrine disorders Iatrogenic (anti-coagulation / copper IUCDs)
 Endometrial or cervical malignancy. Medical disorders. Coagulopathy / Thyroid disease / Endocrine disorders. Iatrogenic (anti-coagulation / copper IUCDs)")
17
Clinical evaluation & management
Patient presenting with heavy menstrual bleeding

18
TAKE A HISTORY

19
Relevant history Frequency and intensity of bleeding – Menstrual diary
Pelvic pain / Pressure symptoms Abnormal vaginal discharge Sexual and contraceptive history Obstetric history Smear history History of coagulation disorder

20
Examination Clinical examination General appearance (? Pallor)
Abdominal examination (?Pelvic mass) Speculum examination Assess vulva, vagina and cervix Bimanual examination Elicit tenderness Elicit uterine / adnexal enlargement
 Speculum examination. Assess vulva, vagina and cervix. Bimanual examination. Elicit tenderness. Elicit uterine / adnexal enlargement.")
21
Investigations Indicated if age > 40 years
or failed medical treatment FBC / Coagulation screen Thyroid function (only if clinically indicated) Smear / Endocervical swabs / High vaginal swabs Pelvic ultrasound (USS) Saline hysterosonography (?Polyps) Hysteroscopy Endometrial biopsy (Pipelle / D&C)
 Smear / Endocervical swabs / High vaginal swabs. Pelvic ultrasound (USS) Saline hysterosonography ( Polyps) Hysteroscopy. Endometrial biopsy (Pipelle / D&C)")
22
Hysteroscopy

23
Endometrial biopsy

24
Endometrial Hyperplasia WHO Classification
Simple hyperplasia No risk of malignant transformation Complex hyperplasia Low risk (~5%) Simple atypical hyperplasia Unknown risk Complex atypical hyperplasia Significant risk (at least 30%)
 Simple atypical hyperplasia. Unknown risk. Complex atypical hyperplasia. Significant risk (at least 30%)")
25
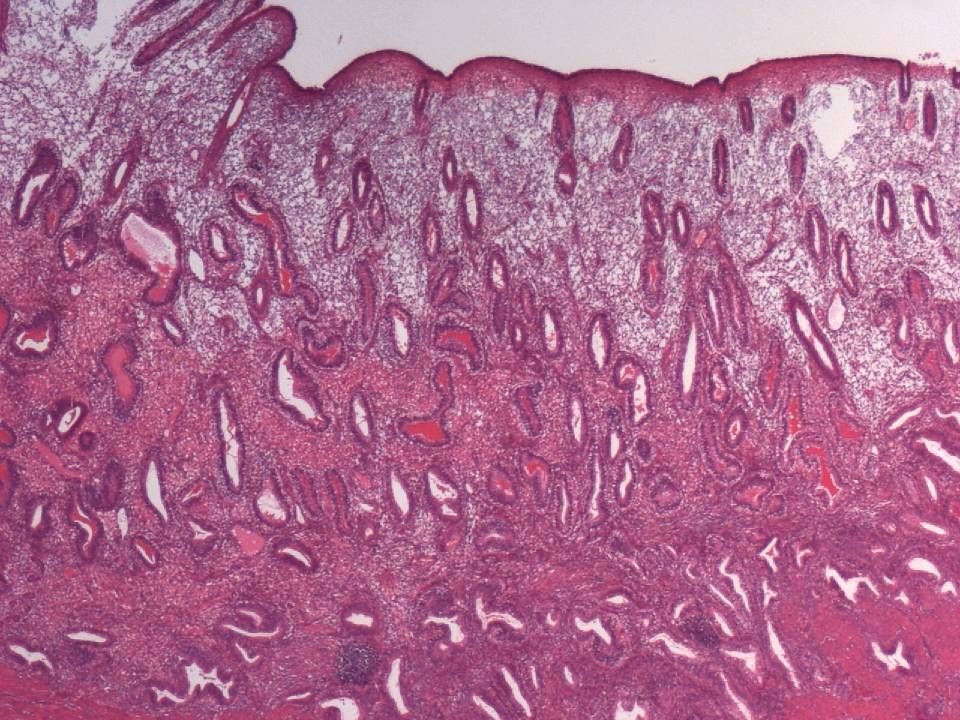
Endometrium: simple hyperplasia

26
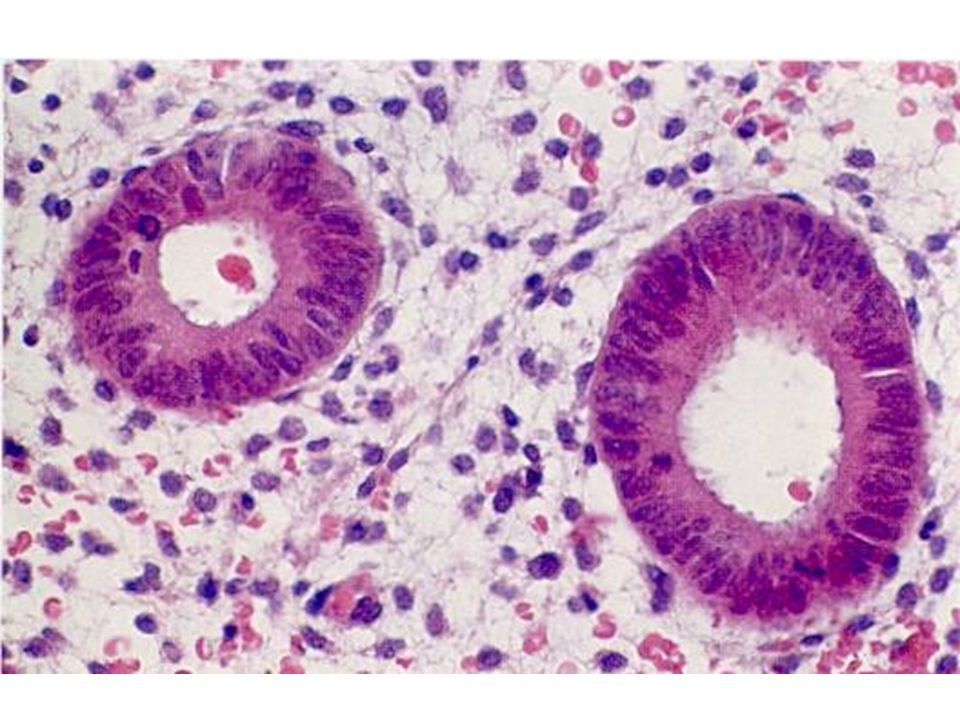
Complex non-atypical hyperplasia

27
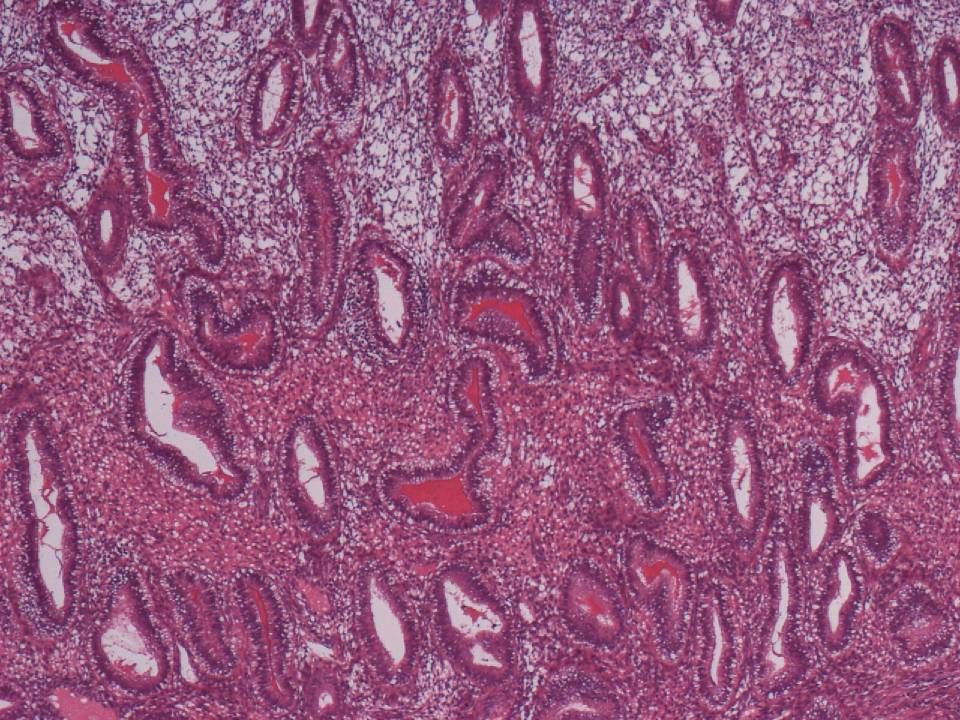
Complex atypical hyperplasia

28
Causes of HMB

29
Endometrial origin “Dysfunctional uterine bleeding”

30
Anovulatory Cycles Reasons for heavy menstrual bleeding
Endometrium develops under the influence of oestrogen Corpus luteum fails to develop absence of progesterone Spiral arteries do not develop properly and are unable to undergo vasoconstriction at the time of shedding Endometrium supplied by thin-walled vessels Result – prolonged heavy bleeding

32
Persistent Anovulation
Infertility Endometrial hyperplasia Increased risk of endometrial carcinoma

33
Management of HMB Anti-fibrinolytics
Tranexamic acid (Cyclokapron®) Prostaglandin synthetase inhibitor Mefenamic acid (Ponstan®) Combined oral contraceptive pill (COC) Progestogens GnRH analogues Endometrial ablation Hysterectomy
 Prostaglandin synthetase inhibitor. Mefenamic acid (Ponstan®) Combined oral contraceptive pill (COC) Progestogens. GnRH analogues. Endometrial ablation. Hysterectomy.")
34
Management - Progestogens
Luteal phase progestogens (only useful if anovulatory) Long-acting progestogens (Depoprovera / Implanon) Mirena IUS
 Long-acting progestogens. (Depoprovera / Implanon) Mirena IUS.")
35
Mirena IUS

36
Endometrial ablation Day-case procedure or out-patient setting
1st generation Trans-cervical resection 2nd generation Thermal balloon Microwave Impedance controlled Similar outcome to Mirena IUS

37
Hysterectomy “Treatment of choice for cancer,
but a choice of treatment for menorrhagia” Lilford RJ (1997) BMJ 314; Surgical access Total versus subtotal hysterectomy Removal versus conservation of ovaries and use of HRT
 BMJ 314; Surgical access. Total versus subtotal hysterectomy. Removal versus conservation of ovaries and use of HRT.")
38
Abdominal hysterectomy
Vaginal hysterectomy

39
Evaluation & Management Polyps and Fibroids
Uterine pathology Evaluation & Management Polyps and Fibroids

40
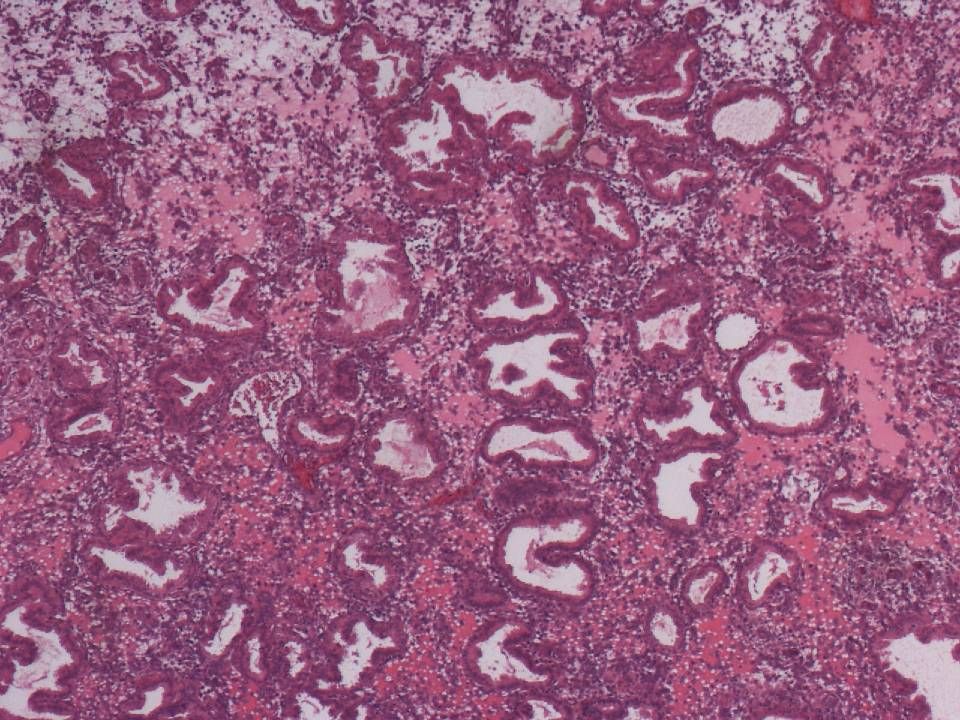
Endometrial polyps Localised overgrowths of endometrium projecting into uterine cavity Common in peri- and postmenopausal women (10 – 24% of women undergoing hysterectomy) Account for 25% of abnormal bleeding in both pre- and postmenopausal women Typically benign, but malignant change can rarely occur Non-neoplastic lesions of endometrium containing glands, stroma and thick-walled vessels Glands may be inactive, functional or hyperplastic Association with tamoxifen use
 Account for 25% of abnormal bleeding in both pre- and postmenopausal women. Typically benign, but malignant change can rarely occur. Non-neoplastic lesions of endometrium containing glands, stroma and thick-walled vessels. Glands may be inactive, functional or hyperplastic. Association with tamoxifen use.")
41
Endometrial Polyp

42
Endometrial polyps Diagnosis Management
Pelvic USS / Saline hysterosonography Hysteroscopy Management Operative removal with polyp forceps / curette or hysteroscopic resection

43
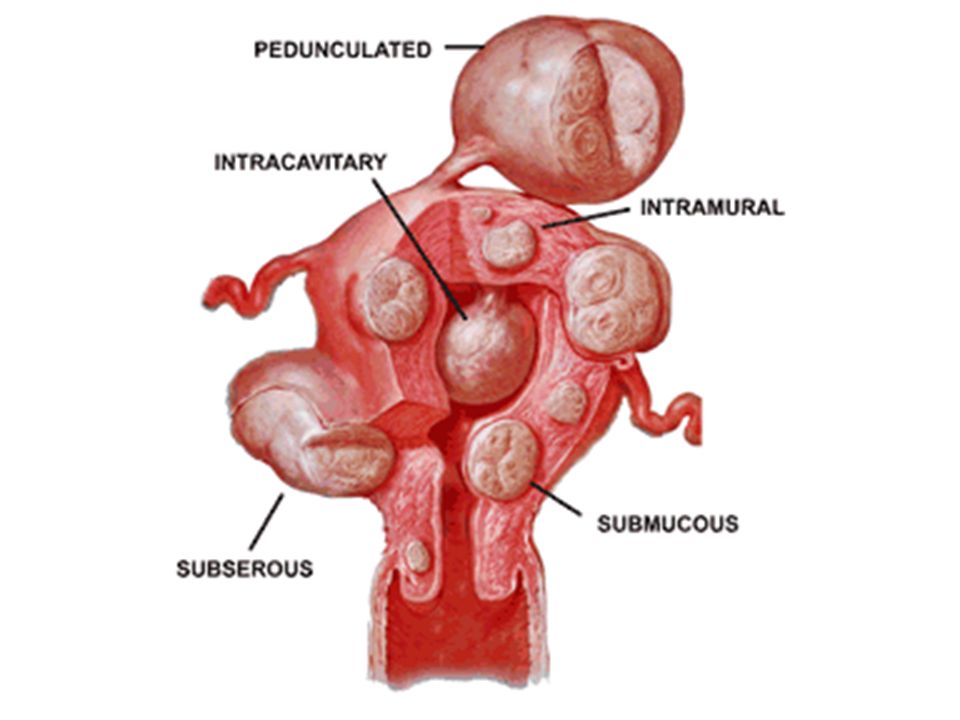
Uterine Fibroids (Leiomyomata)
Occur in 20 – 30% of women over 30 years Usually multiple Almost invariably benign Variable sizes, up to 20 cm or more Sex steroid-dependent – regress after the menopause

45
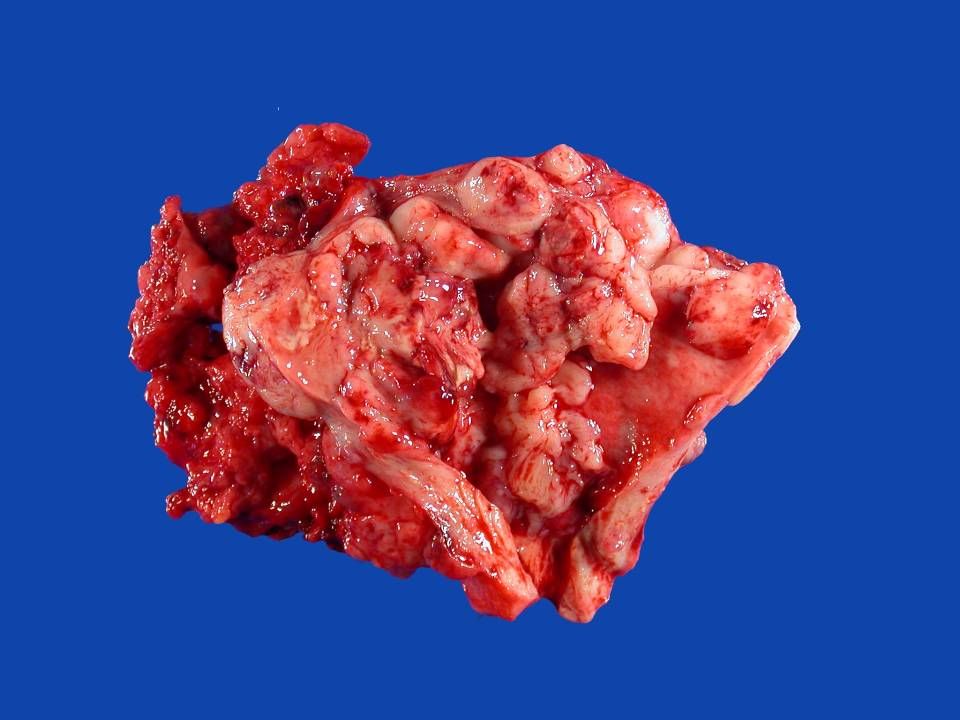
Submucosal uterine fibroid

47
Leiomyoma with central degeneration

48
Leiomyoma

49
Uterine fibroids Symptoms Diagnosis 50% asymptomatic
HMB / Dysmenorrhoea Pressure effects Infertility Pregnancy complications Diagnosis Clinically enlarged uterus Pelvic USS Hysteroscopy / Laparoscopy

50
Uterine fibroids - Management
Conservative Ensure Dx of fibroids and R/O adnexal mass Medical Tranexamic acid / NSAIDs Mirena IUS GnRH agonists Surgical Myomectomy (hysteroscopic / laparascopic / by laparotomy) Hysterectomy Uterine artery embolization
 Hysterectomy. Uterine artery embolization.")
51
Postmenopausal bleeding
Evaluation

52
Postmenopausal bleeding (PMB)
ALL WOMEN WITH PMB MUST BE INVESTIGATED Purpose of investigation: Exclude malignancy of endometrium and cervix Endometrial Ca in up to 4% of women with PMB Precursors of endometrial Ca (complex hyperplasia +/- atypia)
")
53
PMB – Exclude malignancy
History and assessment of risk factors Use of HRT / Tamoxifen / BMI / Family Hx Clinical Examination (!) R/O cervical carcinoma Trans-vaginal USS Assessment of endometrial thickness (<3mm) Endometrial sampling (+/- uterine evaluation) Treatment for endometrial Ca Hysterectomy +/- radiotherapy
 R/O cervical carcinoma. Trans-vaginal USS. Assessment of endometrial thickness (<3mm) Endometrial sampling (+/- uterine evaluation) Treatment for endometrial Ca. Hysterectomy +/- radiotherapy.")
54
Endometrial Carcinoma
Type I Oestrogen dependent 80% Low grade Endometrioid histology Assoc with obesity (40%), nulliparity, late menopause, tamoxifen Type II Non-oestrogen dependent Older postmenopausal women High grade Serous, clear cell and mixed histology Tamoxifen; no association with hyperoestrogenism or hyperplasia Aggressive behaviour
, nulliparity, late menopause, tamoxifen. Type II. Non-oestrogen dependent. Older postmenopausal women. High grade. Serous, clear cell and mixed histology. Tamoxifen; no association with hyperoestrogenism or hyperplasia. Aggressive behaviour.")
57
Endometrioid carcinoma

58
Endometrioid Carcinoma

62
Endometrial Carcinoma Prognostic Factors
Histological type Histological grade Depth of myometrial invasion Lymphovascular space invasion FIGO stage

63
Case 1 43 year old, para 2 + 0, company executive Presenting complaint
excessive menstrual blood loss requirement for contraception History Menarche aged 13 years Used OC pill until 35 years Smokes 15 / day Examination Normal sized uterus and normal adnexae

64
Case 2 38 year old, para 0 + 0, primary school teacher
Presenting complaint excessive menstrual blood loss and dysmenorrhoea History Menarche aged 12 years Used OC pill until 25 years Currently using tranexamic acid with unsatisfactory effect Examination Uterus appears enlarged to 18/40 size

65
Case 3 59 year old, para 0 + 0, retired Presenting complaint History
vaginal bleeding on two occasions over last 3 months History Menopause aged 49 years Polycystic ovarian syndrome Infertility BMI = 38 / Overweight for many years

66
How would you evaluate this case?
Would you carry out any investigations? What management options would you discuss and recommend?

Similar presentations