Download presentation
Presentation is loading. Please wait.

1
"Not all of us can do great things. But we can do small things with great love." — Mother TeresaMother Teresa

2
GLP-1 Receptor Agonists

3
Diabetes Prevalence: Projected Increase 2000-2030

4
Metabolic Syndrome 24% of U.S. adults Diagnosis 3 or more of the following –Hypertension > 130/85 –Waist > 40” men, >35” women –HDL < 40 for men, < 50 in women –Triglycerides > 150 –Fasting glucose > 110 JAMA May 16, 2001 JAMA Jan 16, 2002

5
Prevalence of The Met Syn : US Adults Prevalence (%) 0 5 10 15 20 25 30 35 40 45 20–2930–3940–4950–5960–69 70 Men Women Age (years) Ford ES, et al. JAMA. 2002;287:356-359.

6
Prevalence Rates (%) of Insulin Resistance in Selected Metabolic Disorders Bonora E, et al. Diabetes 1998;47:1643- 49

7
Coronary Heart Disease Mortality 0 2 4 6 81012 0 5 10 15 20 RR (95% CI), 3.77 (1.74-8.17) Follow-up, Y Cumulative Hazard (%) Yes No 866 288 852 279 834 234 292 100 Met Syn: Survival Curves No. at Risk Metabolic Syndrome Yes Metabolic Syndrome: 0 2 4 6 81012 0 5 10 15 20 RR (95% CI), 3.55 (1.96-6.43) Follow-up, Y 866 288 852 279 834 234 292 100 0 2 4 6 81012 0 5 10 15 20 RR (95% CI), 2.43 (1.64-3.61) Follow-up, Y 866 288 852 279 834 234 292 100 Cardiovascular Disease Mortality All Cause Mortality Lakka H-M, et al. JAMA. 2002;288:2709-2716. No
, 3.55 ( ) Follow-up, Y RR (95% CI), 2.43 ( ) Follow-up, Y Cardiovascular Disease Mortality All Cause Mortality Lakka H-M, et al. JAMA. 2002;288: No.")
8
-Cell Function (%) * Postprandial Hyperglycemia IGT † Type 2 Diabetes Phase I Type 2 Diabetes Phase II Type 2 Diabetes Phase III 25 100 75 0 50 -12-10-6-20261014 Years From Diagnosis Patients treated with insulin, metformin, sulfonylureas ‡ * Dashed line shows extrapolation forward and backward from years 0 to 6 from diagnosis based on Homeostasis Model Assessment (HOMA) data from UKPDS. † IGT=impaired glucose tolerance ‡ The data points for the time of diagnosis (0) and the subsequent 6 years are taken from a subset of the UPKDS population and were determined by the HOMA model. Lebovitz HE. Diabetes Rev. 1999;7:139-153. UKPDS: -Cell Loss Over Time
 and the subsequent 6 years are taken from a subset of the UPKDS population and were determined by the HOMA model. Lebovitz HE. Diabetes Rev. 1999;7: UKPDS: -Cell Loss Over Time.")
10
History: GLP1-RAs 1902 Bayliss & Starling: role of a gut-derived hormone (“secretin”) stimulated pancreatic juices. Introduced the word “hormone” (Gr: impetus). 1932 LaBarre term “incretin” to refer to a substance derived from the gut that caused hypoglycemia but did not cause exocrine secretion after eating. 1964–1967 Clinical proof that a gut-derived factor positively modulated insulin secretion; that more insulin was secreted from oral glucose than IV glucose. 1971 John Brown: Isolated, sequenced gastric inhibitory peptide (GIP), and renamed it glucose dependent insulinotropic peptide after finding that plasma glucose has to be elevated in order for GIP to induce insulin secretion. 1985 The second incretin, GLP-1, described. 2002 Exendin-4, a GLP-1 receptor agonist extracted from Gila monster lizard saliva, shown to stimulate insulin secretion in a glucose-dependent manner in subjects with and without T2DM.
. 1932 LaBarre term incretin to refer to a substance derived from the gut that caused hypoglycemia but did not cause exocrine secretion after eating. 1964–1967 Clinical proof that a gut-derived factor positively modulated insulin secretion; that more insulin was secreted from oral glucose than IV glucose. 1971 John Brown: Isolated, sequenced gastric inhibitory peptide (GIP), and renamed it glucose dependent insulinotropic peptide after finding that plasma glucose has to be elevated in order for GIP to induce insulin secretion. 1985 The second incretin, GLP-1, described. 2002 Exendin-4, a GLP-1 receptor agonist extracted from Gila monster lizard saliva, shown to stimulate insulin secretion in a glucose-dependent manner in subjects with and without T2DM..")
16
Mean ± SE; N=6; *P 0.05; 0 1 -0 2 =glucose infusion time Nauck. J Clin Endocrinol Metab. 1986;63:492. Copyright 1986, The Endocrine Society. Venous Plasma Glucose (mmol/L) Time (min) C-Peptide (nmol/L) 11 5.5 0 0101 60120180 0101 60120180 0.0 0.5 1.0 1.5 2.0 Time (min) 0202 0202 Incretin Effect Oral Glucose IV Glucose * * * * * * * Incretin Effect: Amplification of the Beta-cell Response to Oral vs IV Glucose Challenge
 Time (min) C-Peptide (nmol/L) Time (min) Incretin Effect Oral Glucose IV Glucose * * * * * * * Incretin Effect: Amplification of the Beta-cell Response to Oral vs IV Glucose Challenge.")
17
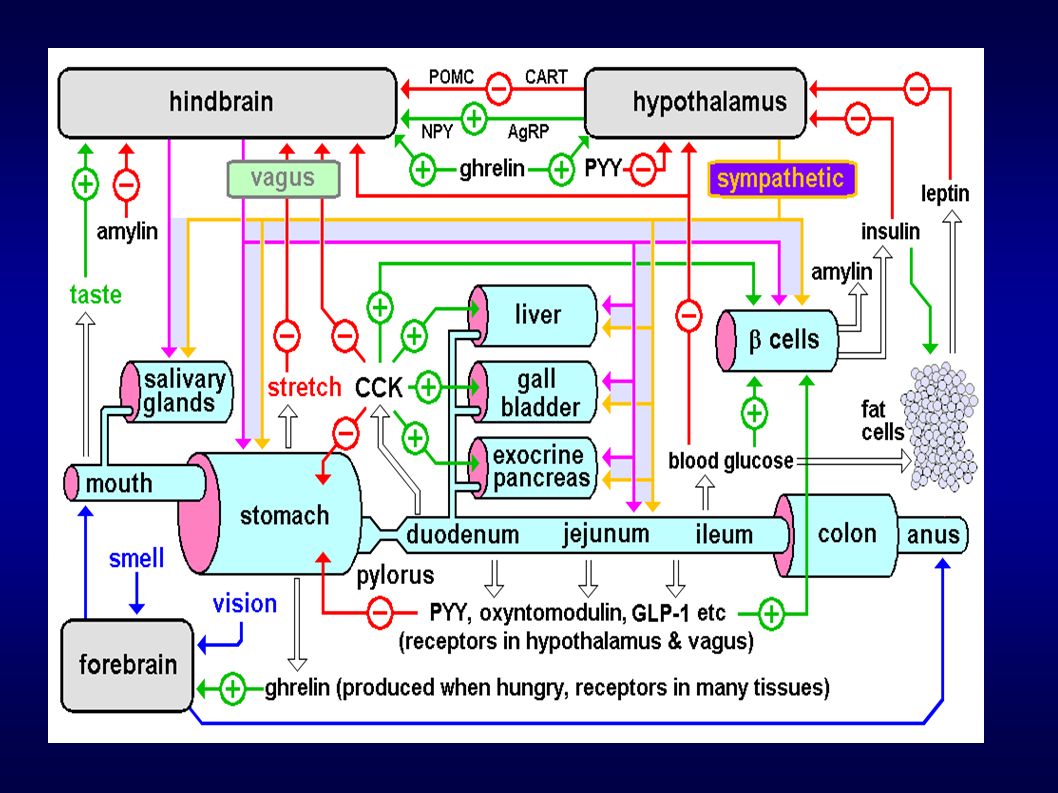
Two Incretins: GIP and GLP-1 Both secreted by enteroendocrine cells by sensing an increase in the concentration of carbs/fats in the lumen of the GI tract. Both degraded by DPP-4 (dipeptidyl peptidase-4). T/2 < 2min. Both stimulate beta cells to secrete ~80% more insulin in response to the same amount of blood glucose. GIP GIP produced by K cells in the proximal small intestine. GIP enhances insulin induced lipoprotein lipase activity, triglyceridegenesis, beta cell proliferation and survival. GLP-1 L-cells in the small bowel and ascending colon synthesize GLP-1 and GLP-2 Posttranslational product of the proglucagon gene encode glucagon, GLP-1 and GLP-2 Tissue-specific post-translational processing of proglucagon, product secretion and degradation. In T2DM: hyperglycemia down-regulates GIPR expression/activity but not GLP-1 receptor expression/activity. Defective GLP-1 secretion in pts with impaired glucose tolerance, resulting in reduced concentrations of post-prandial GLP-1, contributing to a blunted insulin secretory response to meals.
. T/2 < 2min. Both stimulate beta cells to secrete ~80% more insulin in response to the same amount of blood glucose. GIP GIP produced by K cells in the proximal small intestine. GIP enhances insulin induced lipoprotein lipase activity, triglyceridegenesis, beta cell proliferation and survival. GLP-1 L-cells in the small bowel and ascending colon synthesize GLP-1 and GLP-2 Posttranslational product of the proglucagon gene encode glucagon, GLP-1 and GLP-2 Tissue-specific post-translational processing of proglucagon, product secretion and degradation. In T2DM: hyperglycemia down-regulates GIPR expression/activity but not GLP-1 receptor expression/activity. Defective GLP-1 secretion in pts with impaired glucose tolerance, resulting in reduced concentrations of post-prandial GLP-1, contributing to a blunted insulin secretory response to meals..")
18
Incretin effect in T2DM Nauck. Diabetologia. 1986;29:46. ©2006, ICHE Infuse glucose to maintain glycemia at same levels as following a 50-g oral challenge Record -cell secretory responses to oral and IV administration of glucose Compare healthy with T2DM

19
Nauck. Diabetologia. 1986;29:46. Incretin Effect Reduced in T2DM Compared With NGT Incretin Effect Insulin (mmol/L/min) Glucose: IV (isoglycemic infusion) Oral (50 g) 30.0 72.8 23.5 34.7 11.3 38.9 -Cell Secretory Response NGT=normal glucose tolerance Contributions of Incretin Factors (%) ©2006, ICHE
 Glucose: IV (isoglycemic infusion) Oral (50 g) -Cell Secretory Response NGT=normal glucose tolerance Contributions of Incretin Factors (%) ©2006, ICHE.")
20
0 5 10 15 20 060120180240 NGT IGT T2DM Breakfast * * * * * ** * Time (min) Toft-Nielsen. J Clin Endocrinol Metab. 2001;86:3717; with permission. GLP-1 Secretion Impaired in T2DM GLP-1 (pmol/L) *P<0.05 vs T2DM NGT=normal glucose tolerance IGT=impaired glucose tolerance ©2006, ICHE
 *P<0.05 vs T2DM NGT=normal glucose tolerance IGT=impaired glucose tolerance ©2006, ICHE.")
21
GLP Degraded by DPP-4

22
DPP-4 requires an Ala, Pro or HOPro at the penultimate N-terminal position.

23
82-Week Extension Study Exenatide (10 mcg BID) Added to Metformin Change in A1C Change in Weight Change From Baseline (%) Change From Baseline (kg) Ratner. Diabetes Obes Metab. 2006;8:419.

24
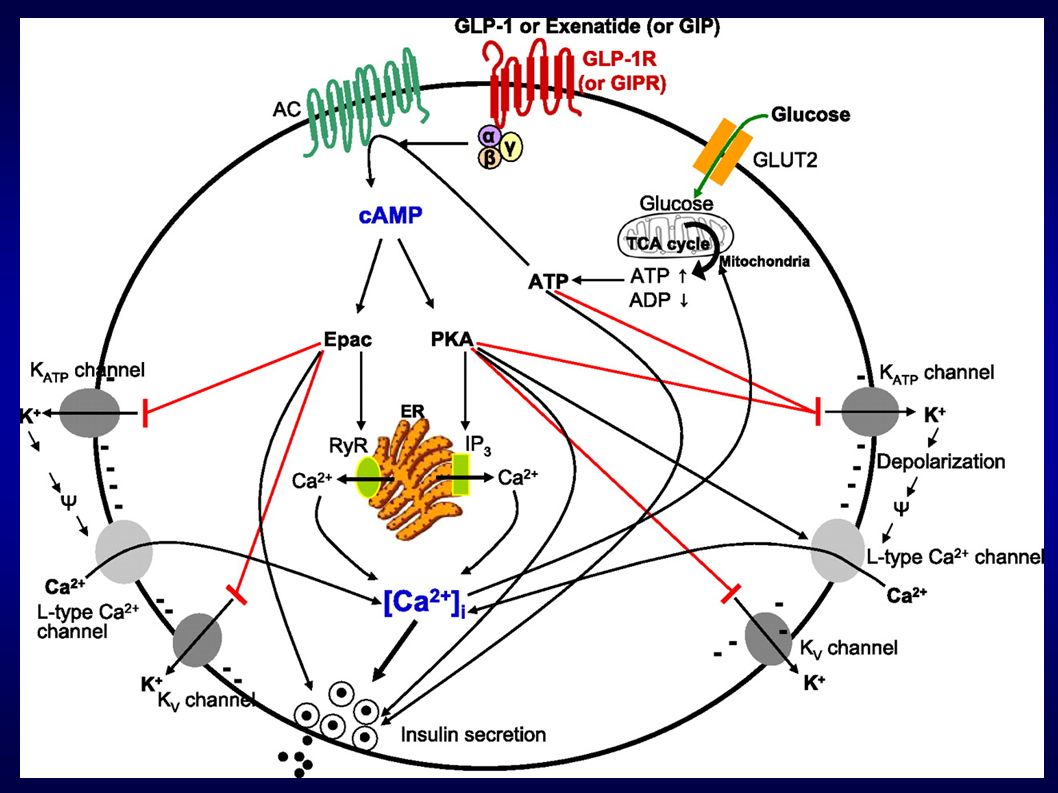
GLP-1 in the Pancreas Beta Cell Stimulates insulin synthesis, secretion, and glucokinase expression. Stimulates expression of GLUT-2 transporter, thereby increasing efficacy and potency of glucose as a stimulus for insulin secretion Restores first phase insulin response Increases proinsulin mRNA stability & gene transcription GLP-1 increases number of beta cells by: Up-regulates beta-cell transcription factor pancreatic duodenal homeobox-1 protein Transactivates the epidermal growth factor receptor Up regulates glucokinase and glucose transporter-2 Inhibiting beta cell apoptosis Delta Cell: Stimulates somatostatin secretion. Alpha Cell: Inhibits glucagon secretion in T1 and T2 DM depending on glucose levels. Probably mediated by paracrine effects via insulin or beta cell product, since no GLP-1 receptors on the alpha cell.

27
Extrapancreatic Effects of GLP-1 Stomach: Decreases gastric acid secretion, delays gastric emptying and motility, which helps to spread glucose absorption out over time, and thus limit hyperglycemia. Neurally mediated central vagal stimulation. CNS: GLP-1 from L-cells and CNS increases satiety. GLP-1 crosses BBB Muscle: Increases glucose uptake, glycogen synthase a activity. Liver: Decreases glucose production Stimulates glycogen synthase a activity Adipocyte Stimulates glucose uptake, lipogenesis Cardiovascular Improves LVEF post MI (Nickolaides et al, 2004) Improves endothelial dysfunction in pts with T2DM with CAD (Nystrom 2004) Cardioprotective effects against ischemia
 Improves endothelial dysfunction in pts with T2DM with CAD (Nystrom 2004) Cardioprotective effects against ischemia.")
28
Metformin: decreases hepatic glucose production, decreases GI glucose absorption and increases glucose uptake by fat and muscle.

29
W.B.: 54 yo sero (-) T2DM 12/08/09 12/08/09: 295 # Met 500 mg bid Lantus 90 U/d Glu 177, A1C 10.2 C-pep 3 ng/ml, 24 h UFC (-), IgF1 (-) GAD, IAA (-) Microalbuminuria 12/22/09: Met 1000 bid Lantus 85 U/d Novolog 1/10 g CCF, 1/25 mg/dl >100 Byetta 5 mcg sq bid
 T2DM 12/08/09 12/08/09: 295 # Met 500 mg bid Lantus 90 U/d Glu 177, A1C 10.2 C-pep 3 ng/ml, 24 h UFC (-), IgF1 (-) GAD, IAA (-) Microalbuminuria 12/22/09: Met 1000 bid Lantus 85 U/d Novolog 1/10 g CCF, 1/25 mg/dl >100 Byetta 5 mcg sq bid")
30
Labs

31
Stopping Lantus

32
Stopping Novolog

33
Investigational Agonists Subcutaneous injection AdministrationAgent Base Peptide/Protract. Mechanism Half-Life/Dosing Frequency a Development Status Exenatide QW Exendin-4 Microsphere with biodegrad. polymer > 1 week 1X weekly FDA review Albiglutide GLP-1 Dimer Bound to albumin DPP-4 site AA subst. 6-8 days ≤ 1X weekly Phase 3 trials Taspoglutide GLP-1 Sustained-release DPP-4 site AA subst. NEP site AA subst. ≈ 6-7 days ≤ 1X weekly Phase 3 trials LY2189265 GLP-1 DPP-4-protected IgG4-Fc-linked ≈ 4 days 1X weekly Phase 3 trials Lixisenatide Exendin-4 6 C-terminal lysines 2.7 - 4.3 hours 1X daily Phase 3 trials

34
GLP-1 RAs AEs (% of Pts) Nausea – LEAD-6 Study: Lira vs Exn bid: 25.5 vs 28% – DURATION-5: Exn bid vs Exn qW: 14 vs 35% – T-EMERGE-2: Taspo 20 vs Exn bid: 47 vs 30% Vomiting – LEAD-6 Study: Lira vs Exn bid: 6 vs 9.9% – T-EMERGE: Taspo 20 vs Exn bid: 23 vs 11% Antibody Formation – LEAD-6 Study: Lira vs Exn bid: 2.6 vs 61.1%
 Nausea – LEAD-6 Study: Lira vs Exn bid: 25.5 vs 28% – DURATION-5: Exn bid vs Exn qW: 14 vs 35% – T-EMERGE-2: Taspo 20 vs Exn bid: 47 vs 30% Vomiting – LEAD-6 Study: Lira vs Exn bid: 6 vs 9.9% – T-EMERGE: Taspo 20 vs Exn bid: 23 vs 11% Antibody Formation – LEAD-6 Study: Lira vs Exn bid: 2.6 vs 61.1%")
35
GLP-1 AEs cont. Pancreatitis – Wide baseline incidence: 4.21-45.33/100,000 annual incidence rates for first attack – Diabetics have a 3 fold increased incidence – Post marketing incidence in 2007 with Exenatide 27/100,000 pt-yrs – Liraglutide 7 cases pancreatitis/4257 pts a.c.t. 1/2381 in comparator group Elevation in Calcitonin – Thyroid C-cell responsiveness to GLP-1 RAs are species specific and appear to activate rodent but not human C-cells – 2 yrs of liraglutide exposure no change in CT levels vs comparator Hypoglycemia – Does not inhibit counter-regulatory response of glucagon

36
T1DM and T2DM

Similar presentations






 ELISA ‘Total Amide’ ‘Active’.>")





![Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]](/15/4663650/big_thumb.jpg "Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]>")



 muscle proteins liver glycogen fat lipids glucose.>")
 muscle proteins liver glycogen fat lipids glucose.>")






