Download presentation
Presentation is loading. Please wait.

1
Monitoring the Safety of Influenza A (H1N1) 2009 Monovalent Vaccines Claudia Vellozzi, MD, MPH Immunization Safety Office Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Atlanta, GA November 18, 2009
 2009 Monovalent Vaccines Claudia Vellozzi, MD, MPH Immunization Safety Office Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Atlanta, GA November 18, 2009")
2
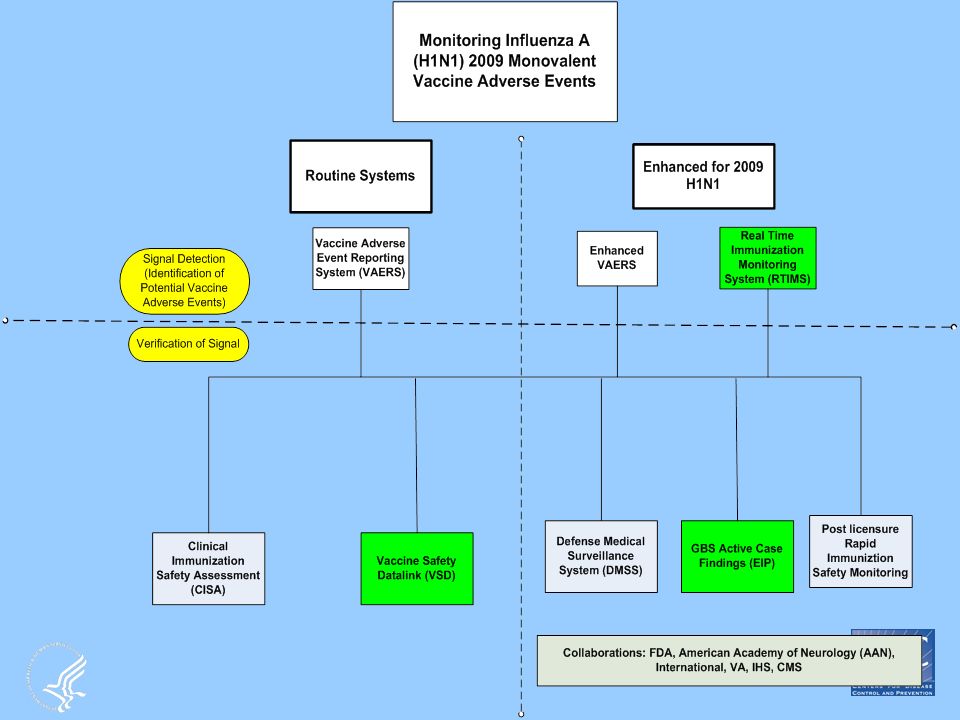
Overall Objectives for 2009 H1N1 Vaccine Safety Monitoring Identify clinically significant adverse events following receipt of 2009 HINI vaccine in a timely manner Rapidly evaluate serious adverse events following receipt of 2009 H1N1 vaccine and determine public health importance Evaluate if there is a risk of Guillain-Barré syndrome (GBS) associated with the 2009 H1N1 vaccine Communicate vaccine safety information in a clear and transparent manner to healthcare providers, public health officials, and the public
 associated with the 2009 H1N1 vaccine Communicate vaccine safety information in a clear and transparent manner to healthcare providers, public health officials, and the public")
3
Today’s Objectives Describe the CDC’s Immunization Safety Office surveillance systems for monitoring the safety of 2009 H1N1 vaccine Provide preliminary data from each of these systems

5
Vaccine Safety Datalink (VSD): Background Established in 1990 A collaborative project among CDC and 8 managed care organizations (MCOs) Allows for planned immunization safety studies as well as timely investigations arising from –hypotheses from medical literature and pre-licensure –reports to the Vaccine Adverse Event Reporting System (VAERS) –changes in immunization schedules, or the introduction of new vaccines Since 2005, conducts routine Rapid Cycle Analysis (RCA) of newly licensed and approved vaccines or modifications to existing vaccine recommendations
: Background Established in 1990 A collaborative project among CDC and 8 managed care organizations (MCOs) Allows for planned immunization safety studies as well as timely investigations arising from –hypotheses from medical literature and pre-licensure –reports to the Vaccine Adverse Event Reporting System (VAERS) –changes in immunization schedules, or the introduction of new vaccines Since 2005, conducts routine Rapid Cycle Analysis (RCA) of newly licensed and approved vaccines or modifications to existing vaccine recommendations")
6
VSD Population Collects medical care and vaccination data on more than 9.5 million members annually (3.1% of the US population) As of 12/31/2008 : 2,252,024 children (<18) enrolled –3.0% of US population 7,245,835 adults (≥18) enrolled –3.1% of US population Average yearly birth cohort ~ 95,000
 As of 12/31/2008 : 2,252,024 children (<18) enrolled –3.0% of US population 7,245,835 adults (≥18) enrolled –3.1% of US population Average yearly birth cohort ~ 95,000")
7
VSD Sites: 2009 Northwest Kaiser Permanente No. CA Kaiser Permanente Harvard Pilgrim Group Health Cooperative So. CA Kaiser Permanente Kaiser Permanente Colorado Health Partners Marshfield Clinic CDC AHIP

8
VSD Data Files + Chart Review Immunizations Records Hospital discharge diagnosis codes Enrollment and demographics Birth and death certificate information Linked by Study IDs Outpatient and Clinic visits +

9
VSD 2009 H1N1 Vaccine Safety Monitoring Specific Aims Conduct rapid surveillance of 2009 H1N1 vaccine safety using – self controlled case series (SCCS) using binomial maximized sequential probability ratio tests (maxSPRT) –comparisons with historical seasonal influenza vaccines using Poisson maxSPRT Conduct comprehensive analyses after immunization program is completed of associations between H1N1 vaccine and adverse events using a variety of statistical methods –Confirmatory Logistic Regression, SCCS, others (as needed)
 using binomial maximized sequential probability ratio tests (maxSPRT) –comparisons with historical seasonal influenza vaccines using Poisson maxSPRT Conduct comprehensive analyses after immunization program is completed of associations between H1N1 vaccine and adverse events using a variety of statistical methods –Confirmatory Logistic Regression, SCCS, others (as needed)")
10
SCCS Example Vaccination ------------------------------------------------------------------------------------------- Days -56 -15 0 42 84 Unexposed (pre) Exposed Unexposed (post)
 Exposed Unexposed (post)")
11
VSD 2009 H1N1 Vaccine Adverse Events under surveillance GBS – first ever and first in a year diagnosis, complemented by chart review Demyelinating disease Disorders of the peripheral nervous system and neuropathies Seizures (epilepsy, convulsions) Encephalitis, myelitis, encephalomyelitis Bell’s Palsy Other cranial nerve disorders (Facial nerve disorders, Trigeminal nerve disorders) Ataxia (other cerebellar ataxia, ataxia) Anaphylaxis Angioneurotic edema, Allergic Reaction, Urticaria Myocarditis and pericarditis (LAIV only) Hemorrhagic stroke (subarachnoid hemorrhage, intracerebral hemorrhage, other and unspecified intracranial hemorrhage) Ischemic stroke (excludes transient ischemic attack) Wheezing (LAIV only) Asthma, wheezing, respiratory distress/insufficiency, other diseases of trachea/bronchi Multiple definitions with and without bronchiolitis Pregnancy Outcomes – Spontaneous Abortions, Stillborn & Pre-eclampsia, eclampsia Adjuvanted Outcomes – Autoimmune hepatitis and Thrombocytopenia
 Encephalitis, myelitis, encephalomyelitis Bell’s Palsy Other cranial nerve disorders (Facial nerve disorders, Trigeminal nerve disorders) Ataxia (other cerebellar ataxia, ataxia) Anaphylaxis Angioneurotic edema, Allergic Reaction, Urticaria Myocarditis and pericarditis (LAIV only) Hemorrhagic stroke (subarachnoid hemorrhage, intracerebral hemorrhage, other and unspecified intracranial hemorrhage) Ischemic stroke (excludes transient ischemic attack) Wheezing (LAIV only) Asthma, wheezing, respiratory distress/insufficiency, other diseases of trachea/bronchi Multiple definitions with and without bronchiolitis Pregnancy Outcomes – Spontaneous Abortions, Stillborn & Pre-eclampsia, eclampsia Adjuvanted Outcomes – Autoimmune hepatitis and Thrombocytopenia")
12
VSD 2009 H1N1 Vaccine Pregnancy Studies Active surveillance in pregnant women –Outcomes: Fever (>100° F),allergic reactions, miscarriage, stillbirth, premature labor and preeclampsia (includes 2 VSD sites) Retrospective analysis evaluating the safety of 2009 H1N1 vaccines in pregnant women and their offspring (includes all VSD sites)
,allergic reactions, miscarriage, stillbirth, premature labor and preeclampsia (includes 2 VSD sites) Retrospective analysis evaluating the safety of 2009 H1N1 vaccines in pregnant women and their offspring (includes all VSD sites)")
13
VSD 2009 H1N1 Vaccine Pregnancy Studies Conduct a survey of pregnant women who receive any combination of seasonal or H1N1 vaccines or refuse vaccination (includes one VSD site) Specific Aims Assess where and when pregnant women are vaccinated and if not vaccinated—why not Accurately capture pregnancy related start dates for future linkage with the electronic medical record Assess non-medically attended AEs –Systemic and local reactions (Fever, chills, headache, swelling, etc.) –ILI and URI symptoms, GI symtoms, sleep disturbances, other
 Specific Aims Assess where and when pregnant women are vaccinated and if not vaccinated—why not Accurately capture pregnancy related start dates for future linkage with the electronic medical record Assess non-medically attended AEs –Systemic and local reactions (Fever, chills, headache, swelling, etc.) –ILI and URI symptoms, GI symtoms, sleep disturbances, other")
14
VSD 2009 H1N1 Vaccine Doses Administered as of Nov 13, 2009 Age Group Novel H1N1-09, nasal (LAMV) Novel H1N1-09, preservati ve-free Novel H1N1-09, unknown formulatio ns Novel H1N1-09, inactivated, no adjuvantTotal < 25104,7412,2754,94892,019203,983 25-4915,6191,4295,89854,31577,261 50-644467404,84034,91540,941 65+137674914,2134,908 Total120,9434,51116,177185,462327,093 206,150 Inactivated Doses
 Novel H1N1-09, preservati ve-free Novel H1N1-09, unknown formulatio ns Novel H1N1-09, inactivated, no adjuvantTotal < 25104,7412,2754,94892,019203, ,6191,4295,89854,31577, ,84034,91540, ,2134,908 Total120,9434,51116,177185,462327, ,150 Inactivated Doses")
15
VSD 2009-10 Seasonal Vaccine Doses Administered as of Nov 13, 2009 Age GroupLAIVTIVTotal <2581,838524,549606,387 25-4917,749455,141472,890 50-64498507,813508,311 65+281557,624557,905 Total100,3662,045,1272,145,493

16
VSD 2009-10 Seasonal Influenza Vaccine Safety Preliminary Findings

17
2009-10 Seasonal Trivalent Inactivated Influenza Vaccine (TIV): SCCS – preliminary results Total Doses Administered– 2,045,127
: SCCS – preliminary results Total Doses Administered– 2,045,127")
18
2009-10 Seasonal TIV Historical Comparison- preliminary results Total Doses Administered: 2,045,127

19
VSD 2009 H1N1 Safety Preliminary Findings

20
2009 H1N1 MIV: Historical Comparison- Preliminary Results Total Doses Administered – 206,150

21
Summary No potential associations or signals have been identified following the monitoring of 2009-10 Seasonal TIV (2,045,127) and LAIV (100,366) doses 2009 H1N1 influenza vaccines have only recently begun to be administered in the VSD MCOs and data are insufficient to assess the safety of the vaccines The VSD will continue to monitor both seasonal and H1N1 influenza vaccines on a weekly basis
 and LAIV (100,366) doses 2009 H1N1 influenza vaccines have only recently begun to be administered in the VSD MCOs and data are insufficient to assess the safety of the vaccines The VSD will continue to monitor both seasonal and H1N1 influenza vaccines on a weekly basis")
22
EIP Guillain-Barré Syndrome (GBS) Surveillance Project: Association of Influenza A (H1N1) 2009 Vaccine and GBS
 Surveillance Project: Association of Influenza A (H1N1) 2009 Vaccine and GBS")
23
EIP GBS Surveillance Sites, 2009- 2010 Connecticut Colorado Oregon California Tennessee Georgia Maryland New York Minnesota Population: ~ 44.9 million New Mexico

24
EIP Guillain-Barré Surveillance (GBS) Surveillance Project CDC's Emerging Infections Program (EIP) –partnership of state and local health departments, academic centers, and CDC –performs surveillance and public health research on emerging infections October 1, 2009 time limited surveillance for GBS Objectives: –Rapidly detect cases of GBS and report (with vaccination status) –Assess and measure if there is an association between 2009 (H1N1) vaccine and GBS Methods: –Population ~45 million persons (statewide in CT, MD, MN, NM, TN and selected regions of CA, CO, GA, NY, and OR) –Active network of neurologists and acute care facilities contacted weekly –Report all GBS cases, standardized case finding, medical record abstraction, patient interviews –Calculation of measures of association
 Surveillance Project CDC s Emerging Infections Program (EIP) –partnership of state and local health departments, academic centers, and CDC –performs surveillance and public health research on emerging infections October 1, 2009 time limited surveillance for GBS Objectives: –Rapidly detect cases of GBS and report (with vaccination status) –Assess and measure if there is an association between 2009 (H1N1) vaccine and GBS Methods: –Population ~45 million persons (statewide in CT, MD, MN, NM, TN and selected regions of CA, CO, GA, NY, and OR) –Active network of neurologists and acute care facilities contacted weekly –Report all GBS cases, standardized case finding, medical record abstraction, patient interviews –Calculation of measures of association")
25
EIP Guillain-Barre Surveillance Case Finding * Weekly query with established network of neurology providers, sentinel pharmacies Additional: Hospital discharges Passive provider reporting (reportable condition) AAN educational initiative; VAERS 10 EIP (40 million) Exclusion (non-cases) [Brighton not met or other neurologic diagnosis] reported weekly to CDC Clinical Network * Active Case-Finding Possible Cases Confirmed Probable Indeterminate Record review; contact provider; antecedent & vaccine history Brighton 1, 2 Brighton 3 Info pending Re-assess at 14 days Patient Interviews
![EIP Guillain-Barre Surveillance Case Finding * Weekly query with established network of neurology providers, sentinel pharmacies Additional: Hospital discharges Passive provider reporting (reportable condition) AAN educational initiative; VAERS 10 EIP (40 million) Exclusion (non-cases) [Brighton not met or other neurologic diagnosis] reported weekly to CDC Clinical Network * Active Case-Finding Possible Cases Confirmed Probable Indeterminate Record review; contact provider; antecedent & vaccine history Brighton 1, 2 Brighton 3 Info pending Re-assess at 14 days Patient Interviews](http://images.slideplayer.com/22/6381008/slides/slide_25.jpg "EIP Guillain-Barre Surveillance Case Finding * Weekly query with established network of neurology providers, sentinel pharmacies Additional: Hospital discharges Passive provider reporting (reportable condition) AAN educational initiative; VAERS 10 EIP (40 million) Exclusion (non-cases) [Brighton not met or other neurologic diagnosis] reported weekly to CDC Clinical Network * Active Case-Finding Possible Cases Confirmed Probable Indeterminate Record review; contact provider; antecedent & vaccine history Brighton 1, 2 Brighton 3 Info pending Re-assess at 14 days Patient Interviews")
26
Descriptive Epidemiology of GBS Active Case Finding, Oct 1-Nov 9, 2009 Confirmed (Brighton Case Definition* Level 1 /2)9 Probable (Brighton Case Definition Level 3)1 Indeterminate (Brighton Criteria Not Available)6 Non-Case (Brighton Clinical Criteria Not Met)8 Case under investigation17 TOTAL41 *www.Brightoncollaboration.org
9 Probable (Brighton Case Definition Level 3)1 Indeterminate (Brighton Criteria Not Available)6 Non-Case (Brighton Clinical Criteria Not Met)8 Case under investigation17 TOTAL41 *")
27
Descriptive Epidemiology of GBS Active Case Finding, Nov 9, 2009 Characteristic + H1N1 vaccine - H1N1 vaccine Vaccine unknown/ missing/ Total n (%) Case Status Confirmed (Brighton Level 1 and 2) 0 (0.0)5 (83.3)4(100.0)9 (90.0) Probable (Brighton Level 3) 0 (0.0)1 (16.7)0 (0.0)1 (10.0) TOTAL0 (0.0)6(100.0)4(100.0)10(100.0) Age (years) 0-240 (0.0)2 (33.3)1 (25.0)3 (30.0) 25-490 (0.0)2 (33.3)1 (25.0)3 (30.0) 50-640 (0.0)2 (33.3)2 (50.0)4 (40.0) 65+0 (0.0)
 Case Status Confirmed (Brighton Level 1 and 2) 0 (0.0)5 (83.3)4(100.0)9 (90.0) Probable (Brighton Level 3) 0 (0.0)1 (16.7)0 (0.0)1 (10.0) TOTAL0 (0.0)6(100.0)4(100.0)10(100.0) Age (years) (0.0)2 (33.3)1 (25.0)3 (30.0) (0.0)2 (33.3)1 (25.0)3 (30.0) (0.0)2 (33.3)2 (50.0)4 (40.0) 65+0 (0.0)")
28
Select Methods Using Vaccine Coverage Data Observed vs. historical GBS rates –Compares observed no. GBS cases occurring within 42 days of H1N1 vaccination to expected no. among vaccinees –Earliest incidence metric –Limitations: historical rate comparison (may not be valid comparison, different case finding) Initially only crude, or age-specific with assumptions on vaccine administration With BFRSS data, fewer assumptions needed for age-specific comparisons GBS rates in vaccinated vs. unvaccinated persons –Use BFRSS vaccine coverage data, calculate person-time exposed and unexposed to vaccine, calculate rates –Strength: rates in vaccinated and unvaccinated persons will both be calculated from active surveillance data –Limitations BRFSS data not available until mid-November and may only be available at the state level (not EIP catchment area specific) GBS rates in H1N1 vaccinated vs. seasonal vaccine recipients –Use BFRSS vaccine coverage data –Age-adjust
 Initially only crude, or age-specific with assumptions on vaccine administration With BFRSS data, fewer assumptions needed for age-specific comparisons GBS rates in vaccinated vs. unvaccinated persons –Use BFRSS vaccine coverage data, calculate person-time exposed and unexposed to vaccine, calculate rates –Strength: rates in vaccinated and unvaccinated persons will both be calculated from active surveillance data –Limitations BRFSS data not available until mid-November and may only be available at the state level (not EIP catchment area specific) GBS rates in H1N1 vaccinated vs. seasonal vaccine recipients –Use BFRSS vaccine coverage data –Age-adjust.")
29
Real Time Immunization Monitoring System (RTIMS) Contributors: Johns Hopkins Bloomberg School of Public Health (JHU) CDC ISO (AHIP) WorldAPP (WA) State and local health departments (HD) Hospitals, schools, clinics, pharmacies
 Contributors: Johns Hopkins Bloomberg School of Public Health (JHU) CDC ISO (AHIP) WorldAPP (WA) State and local health departments (HD) Hospitals, schools, clinics, pharmacies")
30
RTIMS Automated web-based surveillance system Captures self reported data from vaccine recipients Predecessor: Telewatch –Used for monitoring patients with chronic diseases –Modified for monitoring yellow fever vaccine 1 –Piloted for influenza vaccine November 2008 Capacity: –On line and database: 1-10 million vaccine recipients –Follow-up personnel: expandable

31
Objectives 1.To monitor influenza vaccine recipients for adverse events (early signal detection) 2.To identify host factors associated with adverse events 3.To compare rates of adverse events associated with different influenza vaccine products 4.To expedite reporting of AEs to VAERS
 2.To identify host factors associated with adverse events 3.To compare rates of adverse events associated with different influenza vaccine products 4.To expedite reporting of AEs to VAERS")
32
Study Population Seasonal & 2009 H1N1 Influenza vaccine recipients Target population – Pregnant women, health care workers, school aged children State & local health departments, hospitals, schools and OB clinics

33
Timeline for Surveys 2 nd Follow-up 1 st Follow up Day 2 Day 7 Day 42 Baseline survey Pregnancy Follow-up?

34
Study Information Card Provided at Time of Vaccination FrontBack

35
RTIMS Information Flow Electronic (Registrie s) RTIMS Survey Permission to Contact at Time of Vaccination JHU Data entry Formatting Vaccine Recipient WorldAPP Weblinks CDC, JHU, HDs Paper or link www.myflushot.org or www.myflushot.o rg website sign-up 3-4 min initial <1 min follow-up
 RTIMS Survey Permission to Contact at Time of Vaccination JHU Data entry Formatting Vaccine Recipient WorldAPP Weblinks CDC, JHU, HDs Paper or link or rg website sign-up 3-4 min initial <1 min follow-up")
36
State Participation - Active Capture (31 Contacted) On BoardConsideringDeclinedPRISM CO, IN, MD, RI, UT, WV, NC, NJ, KS IL, WAAK, AR, CT, DC, IA, MA, ME, MT, MS, ND,NY, OK, SC, TN, VA, VT AZ, FL, GA, MI, MN, PA, WI
 On BoardConsideringDeclinedPRISM CO, IN, MD, RI, UT, WV, NC, NJ, KS IL, WAAK, AR, CT, DC, IA, MA, ME, MT, MS, ND,NY, OK, SC, TN, VA, VT AZ, FL, GA, MI, MN, PA, WI")
37
4,730 Baseline Surveys by Risk Group and Gender as of Nov 9, 2009

38
Type of Vaccine Received by Risk Group as of Nov 9, 2009

39
Diagnoses after Flu Vaccine by Vaccine as of Nov 9, 2009

40
Limitations Surveys after vaccination Possible selection bias: –Females more likely to participate –Persons with reactions more likely to complete? –Drop outs? Some reluctance to have VAERS form filed –name and contact information Active solicitation of symptoms –Some multiple symptoms

41
Acknowledgements VSD –Eric Weintraub –James Baggs –Frank DeStefano CDC/EIP –Melissa Viray –Paige Lewis –Oliver Morgan –Scott Fridkin RTIMS –Neal Halsey –Rosanna Setse

42
Extra slides

43
The VSD Distributed Data Model CDC Hub “Direct” “Indirect” SAS Programs, Logs, Output, & Analytical Datasets

44
VSD 2009 H1N1 Vaccine Study Design and Analytic Plan Challenges for studying the safety of influenza vaccines –Confounding by indication –Vaccine recommendations have expanded and changed –Influenza vaccines are often given over a very short period of time. –Individuals may have received vaccine outside their MCO (count as unvaccinated) –Seasonality of adverse events may confound interpretation To address the challenges to monitor 2009 H1N1 safety more than one approach will be included in both: – Rapid Cycle Analyses (RCA) weekly surveillance (near real time and critical to rapid safety assessment) –End of season analysis
 –Seasonality of adverse events may confound interpretation To address the challenges to monitor 2009 H1N1 safety more than one approach will be included in both: – Rapid Cycle Analyses (RCA) weekly surveillance (near real time and critical to rapid safety assessment) –End of season analysis.")
45
VSD Methodological approaches in evaluating H1N1 vaccine safety

46
VSD 2009 H1N1 Vaccine Adverse Event Definitions Risk periods (windows) –AE-specific as described in published studies or biologic plausibility –Length of windows – vary from 2 to 60 days –Day of vaccination included in the risk period if it is biologically plausible for AE to occur same day of vaccination (e.g., anaphylaxis). To improve the specificity –Limit to AEs occuring in inpatient or ED settings –First event to occur in a year For AEs that may have more than one “new” onset in a year a shorter period of time will be included in analysis (ex;wheezing, seizures)
.")
47
How the VSD Evaluates Signals 1.Check data quality 2.Check inputs, background incidences, i.e. temporal trends 3.Check whether comparison groups are defined appropriately 4.Conduct the analysis using a different control group (e.g., concurrent vs. historical) or different vaccine 4.Conduct a temporal scan to see if outcomes cluster during a post-vaccination time window 5.Conduct a definitive study using logistic regression analysis 6.Review charts to confirm or exclude cases as true cases
 or different vaccine 4.Conduct a temporal scan to see if outcomes cluster during a post-vaccination time window 5.Conduct a definitive study using logistic regression analysis 6.Review charts to confirm or exclude cases as true cases.")
48
Weekly maxSPRT Results for GBS, Age ≥6 Months, 2007/08 Season

49
VSD Investigators and Collaborators - Partial List Centers For Disease Control, VSD team James Baggs, PhD Julianne Gee, MPH Natalie McCarthy, MPH Eric Weintraub, MPH Kaiser Permanente of No. California (NCK), Oakland CA Roger Baxter, MD Nicky Klein, MD, PhD Ned Lewis Northwest Kaiser Permanente (NWK), Portland OR Allison Naleway, PhD John Mullooly, PhD Karen Riedlinger Lois Drew Harvard Pilgrim /Harv. Vanguard (HAR) Boston, MA Tracy Lieu, MD, MPH Richard Platt, MD, MSc Katherine Yih, PhD, MPH Richard Fox Grace Lee, MD, MPH Sharon Greene, MD, MPH Group Health Cooperative (GHC), Seattle WA Lisa Jackson, MD, MPH Jennifer Nelson, PhD Lora Bounds Marshfield Clinic Rsch. Foundation (MFC) Marshfield WI Edward Belongia, MD James Donahue, MD Nick Berger Health Partners Rsch Foundation (HPM) Minneapolis MN Jim Nordin, MD Amy Butani Kaiser Permanente of Colorado (KPC) Denver, CO Simon Hambidge, MD, PhD Jason Glanz, MS, PhD David McClure, PhD Matt Daley, MD David Ryerson So. California Kaiser Permanente (SCK), CA Los Angeles, CA Steven Jacobson, MD, PhD Wansu Chen, MS Sungching Glenn, MS Sites include > 125 staff working on VSD
, Oakland CA Roger Baxter, MD Nicky Klein, MD, PhD Ned Lewis Northwest Kaiser Permanente (NWK), Portland OR Allison Naleway, PhD John Mullooly, PhD Karen Riedlinger Lois Drew Harvard Pilgrim /Harv. Vanguard (HAR) Boston, MA Tracy Lieu, MD, MPH Richard Platt, MD, MSc Katherine Yih, PhD, MPH Richard Fox Grace Lee, MD, MPH Sharon Greene, MD, MPH Group Health Cooperative (GHC), Seattle WA Lisa Jackson, MD, MPH Jennifer Nelson, PhD Lora Bounds Marshfield Clinic Rsch. Foundation (MFC) Marshfield WI Edward Belongia, MD James Donahue, MD Nick Berger Health Partners Rsch Foundation (HPM) Minneapolis MN Jim Nordin, MD Amy Butani Kaiser Permanente of Colorado (KPC) Denver, CO Simon Hambidge, MD, PhD Jason Glanz, MS, PhD David McClure, PhD Matt Daley, MD David Ryerson So. California Kaiser Permanente (SCK), CA Los Angeles, CA Steven Jacobson, MD, PhD Wansu Chen, MS Sungching Glenn, MS Sites include > 125 staff working on VSD.")
50
EIP Guillain-Barre Surveillance Timeline Vaccine Delivered OCT NOVDECJANMARFEBMAYAPR Case Only Methods: Descriptive Epidemiology Observed vs. Background Rates of GBS: Crude and Age-Specific Comparisons Estimated GBS Rates in Vaccinated vs. Unvaccinated Persons: Crude and Age-Specific Comparisons Case-Cohort analysis BRFSS Vaccine Coverage Data Available Potential Analytic Studies: Self Control Case Series (SCCS)
.")
51
4,790 Completed Baseline Surveys by Risk Group and Age Group as of Nov 9, 2009

53
Diagnoses after Flu Vaccine by Gender as of Nov 9, 2009

54
Daily Visits to http://www.myflushot.org http://www.myflushot.org

55
Links clicked on to arrive at http://www.myflushot.org http://www.myflushot.org HITSEntry Link________________________________________________________ 3615http://www.cdc.gov/h1n1flu/vaccination/public/vaccination_qa_pub.htmhttp://www.cdc.gov/h1n1flu/vaccination/public/vaccination_qa_pub.htm 3486Unknown 1240http:// www.cdc.gov/h1n1flu/vaccination/vaccine_safety_qa.htm 1123Entered URL directly 917http:// www.cdc.gov/h1n1flu/vaccination/ 589http:// www.cdc.gov/h1n1flu/vaccination/vaccine_keyfacts.htm 564http:// www.cdc.gov/H1N1flu/vaccination/pregnant_qa.htm 358http:// www.cdc.gov/h1n1flu/vaccination/gbs_qa.htm 327http:// www.cdc.gov/h1n1flu/vaccination/vaccine_safety.htm 303http:// www.in.gov/flu/ 178http:// www.cdc.gov/h1n1flu/vaccination/general.htm 105http:// cdc.gov/h1n1flu/vaccination/public/vaccination_qa_pub.htm 103http:// www.in.gov/flu/2443.htm 94 http:// www.vaccinesafety.edu/ >60% of traffic comes from the CDC

56
2009-10 Seasonal TIV Historical Comparison- preliminary results Window (days) AgeObservedExpectedRRsignal GBS1-42>6 mos77.50.9NO Encephalitis1-21>6 mos13.60.3NO Ataxia1-42>6 mos913.80.7NO Anaphylaxis0-2>6 mos12.10.5NO Total Doses Administered: 2,045,127
 AgeObservedExpectedRRsignal GBS1-42>6 mos NO Encephalitis1-21>6 mos NO Ataxia1-42>6 mos NO Anaphylaxis0-2>6 mos NO Total Doses Administered: 2,045,127")
Similar presentations


 Project and Monitoring of Pandemic Influenza Vaccines Aug. 21, 2008 Pandemic Influenza Vaccine: Doses Administered and Safety.>")










: Proposed Revision of ICD-9 Codes Rachel Gorwitz, MD, MPH Division of Healthcare Quality Promotion Centers.>")
 of 30 or higher. Body Mass.>")




