Download presentation
Presentation is loading. Please wait.

1
Journal Club Lei Zhang PGY 3 7/16/09

2
Case 55 y.o. F, PMH HTN, DM, TIA, and diverticulosis Had multitple diverticulitis, lower GIB in the past Scheduled to have elective colon resection in 2 wks Presented to the office for pre-op clearance Denied CP, SOB, swelling

3
Case HTN well controlled with Lisinopril and HCTZ DM well controlled with Glipizide and Metformin Also taking ASA and Zocor Good functional status, able to climb 2 flight of stairs carrying grocery Recent EKG/CXR within normal limits Recent CBC, Chem 7 within normal limits

4
Anything Else Needed Pre-operatively? Add Beta-blocker?

5
Perioperative Beta Blocker use Circulation, 2006 Feringa and colleagues performed an observational cohort study of 272 vascular surgery patients Higher doses of -blockers and tight heart rate (< 70 bpm) control associated with reduced perioperative myocardial ischemia and troponin release and improved long- term outcome
 control associated with reduced perioperative myocardial ischemia and troponin release and improved long- term outcome")
6
Perioperative Beta Blocker use J AM Coll Cardio, 2006 Poldermans and colleagues randomly assigned 770 intermediate-risk patients to cardiac stress testing (n386) or no testing (n384) preoperatively Concluded that cardiac testing can safely be omitted in intermediate-risk patients if beta blockers aimed at tight heart rate control are prescribed
 or no testing (n384) preoperatively Concluded that cardiac testing can safely be omitted in intermediate-risk patients if beta blockers aimed at tight heart rate control are prescribed")
7
Perioperative Beta Blocker use BMJ, 2005 Donald Redelmeier & colleague performed retrospective cohort study in Canada in 37,151 asymptomatic patients older than 65 admitted for elective surgery (mainly abd & ortho procedure) Patients receiving long-acting beta- blockers have lower perioperative cardiac risk than short-acting agent
 Patients receiving long-acting beta- blockers have lower perioperative cardiac risk than short-acting agent")
8
ACC/AHA Guideline for Pre-op Beta-blocker Use

9
Perioperative Beta Blocker use Am Heart J. 2006 Yang & colleague performed a double-blind randomized controlled trial of perioperative metoprolol versus placebo in 496 patients undergoing vascular surgery Metoprolol was not effective in reducing the 30- day & 6-month postop cardiac event rates. Concluded that prophylactic use of perioperative beta-blockers in all vascular patients is not indicated

10
Perioperative Beta Blocker use BMJ, 2006 Anne Benedicte Juul & colleague designed a randomized, controlled and blinded multicentre trial in 921 diabetic patients, age > 39, scheduled for major non-cardiac surgery 100 mg metoprolol extended release or placebo given from the day before surgery to a max of 8 perioperative days Conclusions: Perioperative metoprolol did not significantly affect mortality and cardiac morbidity

11
Perioperative Beta Blocker use BMJ, 2006 Devereaux & colleague published a meta- analysis of randomized controlled trials in non-cardiac surgery pts β blockers might prevent major cardiovascular events but increase the risk of hypotension & bradycardia

12
Peri-operative Use of Beta-blocker Yes or NO

14
POISE TRIAL PeriOperative ISchemic Evaluation Purpose of the trial: –Comparing the effect of extended- release metoprolol with that of placebo on 30-day risk of major cardiovascular events in patients with, or at risk of, atherosclerotic disease who were undergoing non-cardiac surgery.

15
POISE TRIAL Research question – Does peri-operative β-blocker regimen benefit noncardiac surgery pts without substantial harm? Double-blinded, randomized, controlled, multi-center trial

16
POISE TRIAL Involved 8,351 pts and 190 hospitals in 23 countries Study period 10/2002 – 7/2007 Ethical approval for all participating sites obtained Written informed consent obtained from all pts

17
POISE TRIAL Inclusion criteria –undergoing non-cardiac surgery –aged 45 years or older –expected length of hospital stay > 24 h –any one of the following criteria hx of CAD hx of PVD Stroke

18
POISE TRIAL hospitalization for CHF within past 3 years undergoing major vascular surgery –Or, any three of seven risk criteria undergoing intrathoracic or intraperitoneal surgery hx of CHF hx of TIA hx of diabetes creatinine >175 μmol/L ( >2.0 mg/dL) age >70 years undergoing emergent or urgent surgery
 age >70 years undergoing emergent or urgent surgery")
19
POISE TRIAL Exclusion criteria –HR < 50 bpm –2 nd or 3 rd AVB –Asthma –Receiving β blocker or planned to start one perioperatively –Prior adverse reaction to β blocker –CABG in the preceding 5 years with no ischemia –Low-risk surgical procedure –On verapamil

20
POISE TRIAL Patients were randomly assigned to two groups via a 24-h computerized randomization phone service Participants, health-care providers, data collectors, and outcome adjudicators were masked to treatment allocation

21
Trial Profile… Figure 1

22
Table 2

23
Method 1 st dose of the study drug (ie, oral extended-release metoprolol 100 mg or matching placebo) given 2–4 h before surgery VS checked each time before medication to ensure HR > 50 bpm & SBP > 100 mm Hg
 given 2–4 h before surgery VS checked each time before medication to ensure HR > 50 bpm & SBP > 100 mm Hg")
24
Method Within 6 h postop, pt received 1 st post-op dose 12 h after 1 st post-op dose, start Metoprolol extended-release 200mg or placebo p.o. daily for 30 days If HR <45bpm or SBP < 100, study drug withheld until recovered Study drug was then restarted at 100mg daily

25
Method If HR consistently 45–49 bpm, SBP >100 mm Hg, delayed taking the study drug for 12 h If unable to take p.o., study drug given by slow or rapid IV infusion q6h Investigators were allowed to select either the slow or rapid IV infusion

26
Method Slow infusion – 15 mg of study drug in 25 mL NS over 60 min –HR & BP checked at 10, 30, and 60 min into the infusion If HR/BP drop, study drug reduce to 10mg

27
Method Rapid infusion – 5 mg of the study drug IV over 2 min and repeated every 5 min for a total of 15 mg ECG recorded 6–12 h postoperatively and on the 1 st, 2 nd, and 30 th days Troponin or CK-MB at 6–12 h postoperatively & on the 1 st, 2 nd, and 3 rd days

28
POISE TRIAL Primary outcome –cardiovascular death –non-fatal MI –non-fatal cardiac arrest at 30 days

29
Statistical Analysis Study has 85% power to detect a relative risk reduction of 25% All analyses used Cox proportional hazards models

30
Table 3

31
Results Fewer in the metoprolol group reached the primary endpoint (hazard ratio 0·84, 95% CI 0·70–0·99, p=0·039) Fewer patients in the metoprolol group had a non-fatal MI (hazard ratio 0·70, 95% CI 0·57–0·86; p=0·0008) Fewer in the metoprolol group had cardiac revascularisation or developed new A fib
 Fewer patients in the metoprolol group had a non-fatal MI (hazard ratio 0·70, 95% CI 0·57–0·86; p=0·0008) Fewer in the metoprolol group had cardiac revascularisation or developed new A fib")
32
Result More in the Metoprolol group had a stroke (hazard ratio 2·17, 95% CI 1·26–3·74, p=0·0053) More people receiving metoprolol died (1·33, 1·03–1·74, p=0·0317) More pts receiving Metoprolol had significant hypotension and bradycardia
 More people receiving metoprolol died (1·33, 1·03–1·74, p=0·0317) More pts receiving Metoprolol had significant hypotension and bradycardia")
33
Primary MIs Strokes Death Figure 2

34
Results Median length of hospital stay was 8 (IQR 4–14) days in the Metoprolol group and 8 (4–15) days in the placebo group (p=0·4046) The number of nights spent in ICU/CCU was much the same in the two groups
 days in the Metoprolol group and 8 (4–15) days in the placebo group (p=0·4046) The number of nights spent in ICU/CCU was much the same in the two groups")
35
Results At discharge, Metoprolol group had –a lower mean HR(71·6 [SD 12·0]vs 78·6 [11·8]; p<0·0001) – lower mean SBP & DBP (129 [18·9]/72 [11·1] vs 131 [18·2]/74 [11·1]mm Hg; p<0·0001)
![Results At discharge, Metoprolol group had –a lower mean HR(71·6 [SD 12·0]vs 78·6 [11·8]; p<0·0001) – lower mean SBP & DBP (129 [18·9]/72 [11·1] vs 131 [18·2]/74 [11·1]mm Hg; p<0·0001)](http://images.slideplayer.com/22/6366350/slides/slide_35.jpg "Results At discharge, Metoprolol group had –a lower mean HR(71·6 [SD 12·0]vs 78·6 [11·8]; p<0·0001) – lower mean SBP & DBP (129 [18·9]/72 [11·1] vs 131 [18·2]/74 [11·1]mm Hg; p<0·0001)")
36
Discussion Why extended-release Metoprolol have increased risk of death and stroke? Clinically significant hypotension, bradycardia and stroke contribute to the increasing risk of death

37
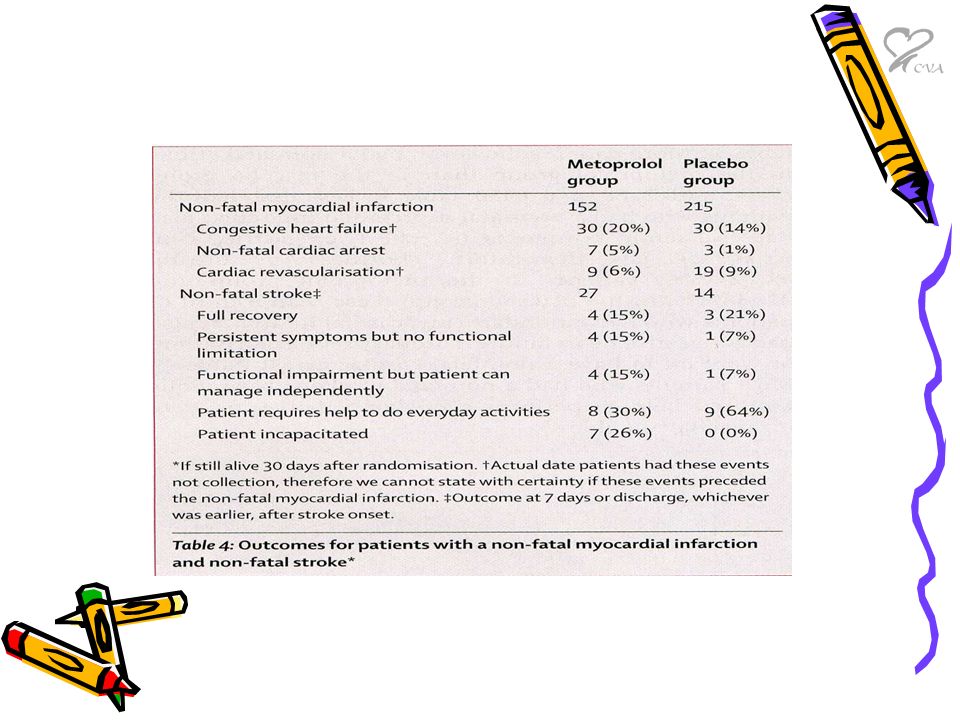
Table 5

38
Discussion Sepsis or infection was the only cause of death that was significantly more common in Metoprolol group Hypotension caused by β blockers could have predisposed pts to developing nosocomial infection

39
Discussion β blockers suppress tachycardia could delay the recognition of sepsis and infection, therefore delaying treatment, which might increase the risk of death

40
Discussion Pts receiving β-blocker who develop sepsis or infection might not have the capacity to mount enough response to sustain life or allow adequate delivery of antibiotics to tissue

41
Discussion POISE researchers also performed several meta-analysis of trials of periop Beta-blocker use –Decrease risk of non-fatal MI –Increase risk of death –Increase risk of non-fatal stroke

42
Figure 4

43
Conclusion

44
Summary Are the results valid? –Yes Are the results important? –Yes Can you apply the results to your patient? –Yes

45
Validity This is a large, multi-center, randomized, double-blind, controlled clinical trial Both groups were comparable in terms of back ground information, type of surgery, anesthesia, and medications Both groups were treated equally

46
Validity Confounding criteria were well-accounted between the two groups Clear inclusion and exclusion criteria Study has detailed medication administration and side-effect monitoring protocol Follow-up was complete for majority of pts

47
Validity Although involving large of amount of pts and study personnel from 190 hospitals in 23 countries, the study was well regulated by central and on-site monitoring system Problems found in Iran and Colombia were caught immediately and data excluded from the study

48
Applicability This is a large multi-country study, involving different racial, ethnic & economic population; it is safe to generalized the study results to our practice patients

49
Significance The study have enormous influence on current medicine practice It challenged the currently popular concept of perioperative Beta- blocker use

50
Significance For every 15 patients in POISE trial, one had a cardiovascular death, non- fatal myocardial infarction, non-fatal cardiac arrest, or non-fatal stroke at 30-day follow-up

51
Significance Suggest that the addition of perioperative Beta-blocker potentially has serious risks Lead to the further question of who will benefit from Beta-blocker and who will not?

52
Thank You

53
ACC/AHA Guideline for Preop Eval for Noncardiac Surgery Pts with active cardiac conditions, indicate major clinical risk –unstable coronary syndromes, acute MI < 7 days recent MI > 7 days but </= 1 month with evidence of ischemia unstable or severe angina –decompensated heart failure, –significant arrhythmias –severe valvular disease

54
ACC/AHA Guideline for Preop Eval for Noncardiac Surgery Pts with clinical risk factors –history of heart disease, hx MI or Q waves by ECG –history of compensated or prior CHF –history of cerebrovascular disease, TIA, stroke –diabetes mellitus, preop use of insulin –renal insufficiency, preop Cr >2.0

Similar presentations

 Clinical events (morbidity.>")


>")











>")



