Download presentation
Presentation is loading. Please wait.

1
MedsCheck and Hospital Medication Reconciliation Improving Patient Safety Building the Community Pharmacy and Hospital Partnership Ottawa Ontario Oct. 14, Margaret Colquhoun Project Leader ISMP Canada

2
ISMP Canada www.ismp-canada.org
To identify risks in medication use systems, recommend optimal system safeguards and advance safe medication practices. Work to advance safe medication use.

3
Agenda Welcome and Introductions Medication reconciliation
Overview and progress of work in institutions including discharge medication reconciliation 3. MedsCheck and Medication Reconciliation Pre-surgical MedsCheck for elective surgical patients – who, what, how? 4. Planning Together Summary and next steps Staying in touch

4
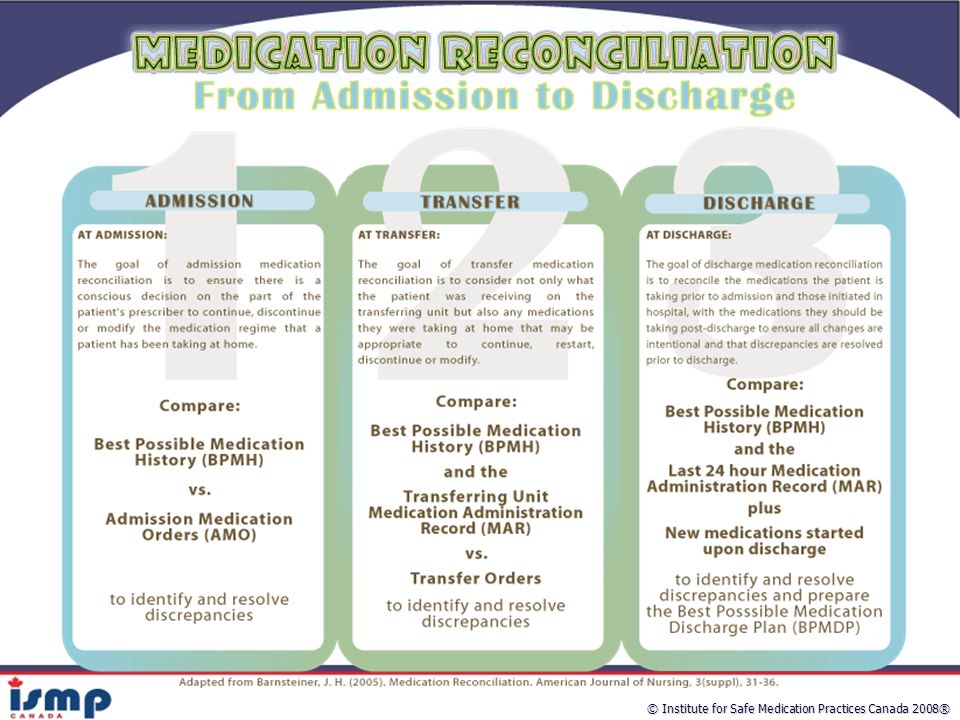
Medication Reconciliation
Formal and consistent process in which most accurate list of patient’s home medications are compared at transitions of care: admission, transfer, discharge, LTC, homecare Discrepancies are identified, brought to attention of physician, required changes are made and communicated Intended to minimize potential patient harm from unintended discrepancies

5
Medication Reconciliation
Is also… A high priority objective for all hospitals in Ontario A Required Organizational Practice for Accreditation Canada One of the Safer Healthcare Now! Initiatives A process that will become the new way…not a project

6
Primary Medication History: MD or RN Admission Reconciliation
Schematic of Structured, Multidisciplinary Integrated Medication Reconciliation Strategy Primary Medication History: MD or RN ER Ward BPMH: Taken by pharmacist Admission Reconciliation BPMH medical chart One history only 1 Wong J. Annals of Pharmacotherapy 2008 (in press)
")
8
Published Studies: “Unintended Medication Discrepancies at the time of Hospital Admission”
151 patients At least 4 regular prescriptions, admitted to GIM teaching hospital 53.6% of patients at least 1 unintended discrepancy [95% CI 45.7%-61.6%] 46.4% of errors – omitted medication Patient Impact : 38.6% had the potential to cause moderate to severe discomfort or clinical deterioration Cornish P et al. Arch Intern Med 2005:165;

9
Published Studies: “Patient Medication Adverse Events Post Discharge”
23% of Discharged Patients from a Canadian Hospital experienced an adverse event – of those 72% were drug related 328 patients who were discharged from a Canadian teaching hospital were studied prospectively in 2002 for 14 weeks. (AJ Forster,et al., CMAJ 2004:170(3) ) Developed by Courtyard-Group for E-Health Conference 2004
 ) Developed by Courtyard-Group for E-Health Conference")
10
Published Studies: The Case for Medication Reconciliation
Many patients (70%) not receiving medication instructions at discharge (Alibhai SMH, Han RK, Naglie G. Medication Education of Acutely Hospitalized Older Patients. J Gen Intern Med 1999 Oct;14: )
 not receiving medication instructions at discharge. (Alibhai SMH, Han RK, Naglie G. Medication Education of Acutely Hospitalized Older Patients. J Gen Intern Med 1999 Oct;14: )")
11
Glaucoma meds missed for 14 days
Stories from Medication Reconciliation Teams: Medication reconciliation Failures Transplant rejection drugs not ordered on admission (>48hr delay in restarting) Glaucoma meds missed for 14 days #1 Kidney transplant patient admitted and rejection drugs not continued for >48hrs. Med rec in 24hrs would have solved this quicker. Potential for harm very real and very great. #2 Patient transferred from RGH to PH under care of family physician. Med rec process identified pts glaucoma eye drops not ordered or given for 2 weeks. Potential for harm – real. #3 Hydromorphone 3mg q12h at home transcribed as 30mg q12h on admission. Pharmacy processed orders. Patient was admitted on a Friday afternoon and was given one dose Friday night and another Saturday am. Family arrived Saturday and took patient out on pass and called in a few hours later stating the patient had become lethargic with decreased responsiveness. Family was directed to take patient to ER for assessment – observed for several hours and back to normal. Patient taken back to LTC facility and received Saturday pm dose and Sunday am dose – once again unresponsive and then the problem was found. #4 Elderly patient was admitted with newly diagnosed afib and had simple hospital course saw rate control calcium channel blocker therapy changed from amlodipine to diltiazem. Patient not informed of change and went home and took both. Readmitted 3 days later due to severe bradycardia and nearly required pacemaker.
 Glaucoma meds missed for 14 days. #1 Kidney transplant patient admitted and rejection drugs not continued for >48hrs. Med rec in 24hrs would have solved this quicker. Potential for harm very real and very great. #2 Patient transferred from RGH to PH under care of family physician. Med rec process identified pts glaucoma eye drops not ordered or given for 2 weeks. Potential for harm – real. #3 Hydromorphone 3mg q12h at home transcribed as 30mg q12h on admission. Pharmacy processed orders. Patient was admitted on a Friday afternoon and was given one dose Friday night and another Saturday am. Family arrived Saturday and took patient out on pass and called in a few hours later stating the patient had become lethargic with decreased responsiveness. Family was directed to take patient to ER for assessment – observed for several hours and back to normal. Patient taken back to LTC facility and received Saturday pm dose and Sunday am dose – once again unresponsive and then the problem was found. #4 Elderly patient was admitted with newly diagnosed afib and had simple hospital course saw rate control calcium channel blocker therapy changed from amlodipine to diltiazem. Patient not informed of change and went home and took both. Readmitted 3 days later due to severe bradycardia and nearly required pacemaker.")
12
Med Rec Admission Failure
LB was admitted to a medical ward with a working diagnosis of community acquired pneumonia Appropriate antibiotics & symptom management ordered & commenced 2 days later LB suffered a myocardial infarction (HR 168) Beta-blocker was not continued on admission
 Beta-blocker was not continued on admission.")
13
Current Picture We do not have seamless communication systems…………and patients know it There is duplication of effort in community and hospital There is potential for unintended adverse drug events

14
What is the patient supposed to be on?
Hospital Perspective What is the patient supposed to be on? Patient Interview Labels on Rx Vials Medication Lists Family MD list Patient’s own list Patient’s Actual Medication Use Medical chart Medication wallet cards Community pharmacist Patient’s Prescribed Medication Regimen What is the “truth”?

15
Community Perspective
What is the patient supposed to be on? Other sources of information: Patient profile on the computer (not reflective of recent changes) Patient or agent (usually know little) Hospital Physician /Nursing station (impossible to acquire info) RX’s from the hospital Missing information (medication name, dose, frequency, quantities LTD codes) Illegible Automatic substitutions while in hospital Drugs not covered by ODB or drug plan Section 8’s not applied for Knowing which meds were intentionally discontinued or were they unintentionally missed
 Patient or agent (usually know little) Hospital Physician /Nursing station (impossible to acquire info) RX’s from the hospital. Missing information (medication name, dose, frequency, quantities LTD codes) Illegible. Automatic substitutions while in hospital. Drugs not covered by ODB or drug plan. Section 8’s not applied for. Knowing which meds were intentionally discontinued or were they unintentionally missed.")
16
MedsCheck Ontario Ministry of Health and Long-Term Care
Funded by MOHLTC One-on-one 30 minute appointment with the community pharmacist Reviews all the patient’s medications (prescribed and OTC) Helps patients better understand their medication therapy and ensure that medications are taken as prescribed.
 Helps patients better understand their medication therapy and ensure that medications are taken as prescribed.")
17
Who is eligible for a MedsCheck?
All Ontarians are eligible Once per year No additional cost to client Provided they are taking 3 or more medications for a chronic condition. Community Pharmacist is reimbursed for their professional services.

18
MedsCheck Personal Medication Record

19
What’s a MedsCheck Follow-up?
MedsCheck Follow-up is a program for patients who may benefit from additional MedsChecks during the annual timeframe. There is no limit to the number of Medscheck Follow-ups provided they meet the following criteria: A planned hospital admission (e.g. elective surgery) A physician or registered nurse in the extended class (RN[EC]) request A recent discharge from hospital (within 2 weeks)
 A physician or registered nurse in the extended class (RN[EC]) request. A recent discharge from hospital (within 2 weeks)")
20
Overview of MedsCheck/Medication Reconciliation Pilot
To facilitate the linkage of the MedsCheck program in community pharmacies with the medication reconciliation process in hospitals in communities across Ontario.

21
Pilot Objectives To Improve : Communication of medication information
Continuity of care for the patient/client at transitions of care. Accuracy of medication ordering Efficiency by reducing re-work

22
Linking MedsCheck to MedRec Pilot ISMP Canada 2008
14 hospitals Pre-admission surgical clinic - elective patients Requesting patients to arrange a MedsCheck 1-2 weeks prior to their pre-admission clinic appointment Create the Best Possible Medication History (BPMH) in hospital using MedsCheck as the primary source of information Collect data - time to complete BPMH and quality of MedsCheck
 in hospital using MedsCheck as the primary source of information. Collect data - time to complete BPMH and quality of MedsCheck.")
23
Our Initial Focus: Pre Surgical Admission Reconciliation
1 Pre-op Appointment 1 Prevent inadvertent omission of needed home meds Prevent errors associated with orders having incorrect doses or dosage forms Day of Surgery OR 2 1 Prevent failure to restart home meds following discharge and transfer Prevent duplicative therapy at discharge (i.e. brand/generic, formulary substitutions) 2 Surgical Unit Transfer Units (Rehab) 2 Home
 2. Surgical Unit. Transfer Units (Rehab) 2. Home.")
24
Co-ordination Process Flow
Patient gets a MedsCheck 2 weeks before pre-op clinic date Pt brings MedsCheck and vials to pre-op clinic date Surgeon asks Pt to get a MedsCheck BPMH created using MedsCheck plus 1 other source UPDATE: Booklets Pamphlets Hip/Knee binders Verbal reminders Hospitals: Phone reminders Calling/Faxing their pharmacies Day Surgery nurse reviews medication list with patient on day of surgery POST-OP Surgeon reviews and orders meds using BPMH BPMH is updated Discharge MedRec Patients sees community pharmacist for MedsCheck Follow-up

25
Supports for Hospitals
Checklists Revised sample forms Data collection tools pre and post MedsCheck Community pharmacists BPMH presentations and meetings such as this one Sharing teleconferences

26
Sample: My Total Joint Replacement Passport
Transportation Appointment with your surgeon for postoperative follow-up visit Anticoagulation therapy stop date Staples/clip removal date Discharge date from hospital Community Care Access Centre (CCAC) visit or Outpatient Physiotherapy postoperative appointment MedsCheck appointment with your community pharmacist (if you are on 3 or more prescribed meds) Appointments with specialists Appointment with your family doctor Preoperative assessment Date of surgery Date Appointment/Activity My Total Joint Replacement Passport Please use this passport to record the dates for all of your appointments and other activities. The next page explains each appointment / activity in more detail. My surgeon is Dr. _________________________. His/her office will contact me with my surgery date. My family member/friend who will assist me throughout my joint replacement is: _______________________. He/she can be reached at: _________________. Bring this passport with you to all appointments. Used with permission from Markham Stouffville hospital
 visit or Outpatient Physiotherapy postoperative appointment. MedsCheck appointment with your community pharmacist (if you are on 3 or more prescribed meds) Appointments with specialists. Appointment with your family doctor. Preoperative assessment. Date of surgery. Date. Appointment/Activity. My Total Joint Replacement Passport. Please use this passport to record the dates for all of your appointments and other activities. The next page explains each appointment / activity in more detail. My surgeon is Dr. _________________________. His/her office will contact me with my surgery date. My family member/friend who will assist me throughout my joint replacement is: _______________________. He/she can be reached at: _________________. Bring this passport with you to all appointments. Used with permission from Markham Stouffville hospital.")
28
Sample: Forms and Applications
The forms and applications must be completed before your preoperative visit to the hospital. If you have any questions, it is fine to contact your surgeon’s office for assistance. These forms must be brought with you to your preoperative assessment visit at the hospital: History and Physical Form Anesthesia Patient Questionnaire Inpatient Rehabilitation Application MedsCheck from your community pharmacist if you are on 3 or more prescribed medications

29
Sample: Surgical Assessment Clinic (SAC) Checklist
Translator - If your primary language is not English, please arrange to have a translator with you for all your appointments including on the day of your surgery. A family member, friend, or caregiver who will be helping you after surgery. A snack and drink as you will be at the hospital for 4-5 hours; this is particularly important if you have diabetes. MedsCheck from your community pharmacist if you are on 3 or more prescription medications. All medications you are taking at home in their original containers with the labels (include prescription eye drops and creams, herbal and over-the-counter medications). Copies of any recent blood work or diagnostic tests that you have had done outside of Markham Stouffville Hospital. History and Physical form – completed by your family physician. The Anesthesia Patient Questionnaire – completed by you. Rehabilitation Application – completed by you. The forms given to you with this guide are to be brought in with you to the SAC appointment or returned prior to the appointment. If you have mailed or faxed these forms, you must ensure they reach the hospital before this appointment. Surgical Assessment Clinic (SAC) Appointment Checklist What to Bring with You Bring this patient guide with you. Your orthopedic team will review your passport with you to ensure you are completing all of your presurgical preparations correctly. Used with permission from Markham Stouffville hospital
. Copies of any recent blood work or diagnostic tests that you have had done outside of Markham Stouffville Hospital. History and Physical form – completed by your family physician. The Anesthesia Patient Questionnaire – completed by you. Rehabilitation Application – completed by you. The forms given to you with this guide are to be brought in with you to the SAC appointment or returned prior to the appointment. If you have mailed or faxed these forms, you must ensure they reach the hospital before this appointment. Surgical Assessment Clinic (SAC) Appointment Checklist. What to Bring with You. Bring this patient guide with you. Your orthopedic team will review your passport with you to ensure you are completing all of your presurgical preparations correctly. Used with permission from Markham Stouffville hospital.")
30
Coordinating MedsCheck and Medication Reconciliation in Ontario will:
Positively impact the entire continuum of patient care: Seamless transfer of information Support patients to take/receive medications correctly and appropriately during transitions in care. Reduce the potential for medication errors/adverse drug events Improves efficiency and accuracy

31
Coordinating MedsCheck and Medication Reconciliation in Ontario will:
Develop and strengthen the relationship between patients and their community pharmacist. Improve patients understanding of their medications by reviewing them in the community and again in hospital at discharge. Encourage hospital and community pharmacies to work more closely together to improve communication and patient care.

32
Hospital Roles Change processes to direct patients to book a MedsCheck prior to pre-admission clinic date. Surgeons, pre-admit nurses, forms and tools Pilot hospitals have resources to share E.g Checklist Train preadmission staff to ask for a MedsCheck by name when doing BPMH and use it. Further implement discharge medication reconciliation

33
Community Pharmacists Role
Book MedsCheck for pre-admission clinic patients when they ask or if contacted by the hospital Perform MedsCheck Record all the medications the patient is actually taking. If it differs from the prescribed instructions then document the discrepancy in comments section. Include all current prescription and over-the-counter medications. (aspirin, iron, potassium) Ask about medications dispensed from other pharmacies. Perform Follow-up MedsCheck at Discharge within 2 weeks
 Ask about medications dispensed from other pharmacies. Perform Follow-up MedsCheck at Discharge within 2 weeks.")
34
Innovations we’ve heard about - hospitals
Using SPEP students to follow patient from SAC visit to admission Using volunteers to phone patients to remind them to get a MedsCheck Phoning/faxing pharmacies (with the patient’s permission) to inform them of the patients who are having a surgery and their pre-admission clinic date Writing articles in local paper about this new initiative to inform patients Faxing community pharmacies a form to fax back so that it is completed in the hospital format as that you would use in hospital. (Note: some community pharmacies are using electronic version) Working with community pharmacists on discharge med rec form.
 to inform them of the patients who are having a surgery and their pre-admission clinic date. Writing articles in local paper about this new initiative to inform patients. Faxing community pharmacies a form to fax back so that it is completed in the hospital format as that you would use in hospital. (Note: some community pharmacies are using electronic version) Working with community pharmacists on discharge med rec form.")
35
Innovations we’ve heard about……community
Designated MedsCheck day - considered a viable business plan that pays for itself SPEP Students - good educational experience Scheduling daily time for MedsCheck BPMH training (Enhancing MedsChecks) Accommodating patients who cannot get a MedsCheck from their own pharmacy
 Accommodating patients who cannot get a MedsCheck from their own pharmacy.")
36
Making it Happen What are the barriers in hospitals?
What are the barriers in community to accommodating more patients for a MedsCheck or complying with patient/hospital request to book a MedsCheck? How can we work together?

37
Conclusion We have opportunities in Ontario to help us overcome the
challenges of medication information transfer

38
Questions mcolquhoun or

Similar presentations


















 introduced.>")
 VIHA Pharmacy Resident 2009-10.>")
