Download presentation
Presentation is loading. Please wait.

1
The Biomechanics of the Human Upper Extremity
Dr Ayesha Basharat

3
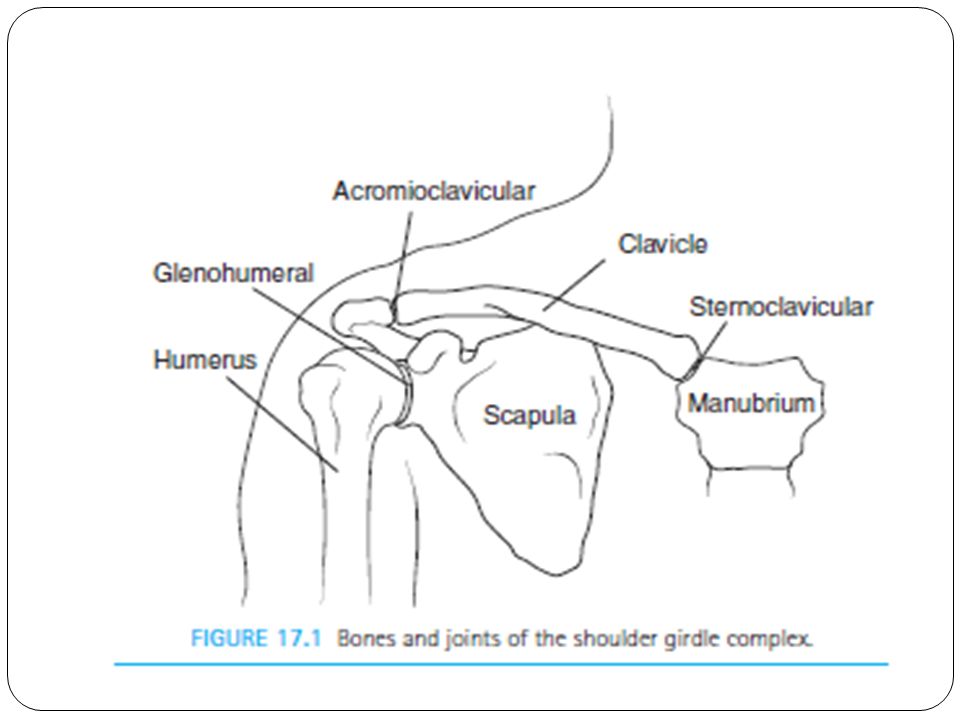
Shoulder Girdle Includes: G-H joint Subacromial space S-T joint
A-C joint S-C joint

5
Sternoclavicular Joint
Provides major axis of rotation for movement of clavicle and scapula Freely permitted frontal and transverse plane motion. Close pack position is with maximum shoulder elevation

6
Sternoclavicular Joint
Joint capsule Anterior & posterior S-C ligaments Intra-articular disc Interclavicular ligament Costoclavicular ligament

8
Sternoclavicular Joint
Motions: Protraction/retraction Elevation/depression Axial rotation (spin)
")
9
Acromioclavicular Joint
Irregular Diarthrodial joint between the acromion process of the scapula and the distal clavicle. allows limited motions in all three planes. Rotation occurs during arm elevation Close-packed position with humerus abducted to 90 degrees In close- Packed position there is maximum contact between the articulating surfaces and stability is also maximum.

10
Acromioclavicular Joint
Joint capsule A-C ligaments Intra-articular disc Coracoclavicular ligaments

12
Coracoclavicular Joint
A syndesmosis with coracoid process of scapula bound to the inferior clavicle by the Coracoclavicular ligament. Permits little movement

13
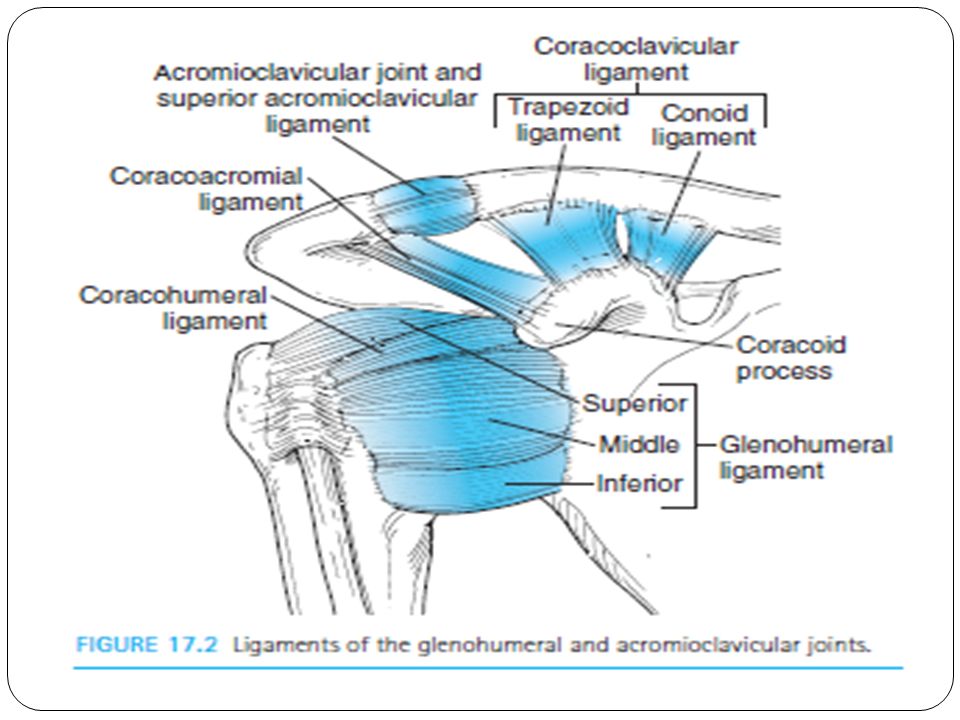
Glenohumeral Joint Most freely moving joint in human body
Glenoid Labrum composed of: fibrocartilage rim & Joint capsule Tendon of long head of biceps brachii Glenohumeral ligaments Rotator Cuff Muscles Most stable in close-packed position, when the humerus is abducted and laterally rotated.

14
Glenohumeral Motion Passive restraints Active restraints
Controlled by: Passive restraints Active restraints

15
Glenohumeral Motion Passive Restraints: Bony geometry Labrum
Capsuloligamentous structures Negative intra-articular pressure

16
Capsuloligamentous Structures
SGHL MGHL IGHL complex anterior band posterior band axillary pouch

17
Restraints to External Rotation
Dependent on arm position: 00 - SGHL, C-H & subscapularis 450 - SGHL & MGHL 900 - anterior band IGHLC

18
Restraints to Internal Rotation
Dependent on arm position: 00 - posterior band IGHLC 450 - anterior & posterior band IGHLC 900 - anterior & posterior band IGHLC

19
Restraints to Inferior Translation
Dependent on arm position: 00 - SGHL & C-H 900 - IGHLC

20
Scapulothoracic Joint
Region between the anterior scapula and thoracic wall. Functions of muscles attaching to scapula: Contract to stabilize shoulder region Facilitate movements of the upper extremity through appropriate positioning of the Glenohumeral joint.

21
Movements of the Shoulder Complex
Humerus movement usually involves some movement at all three shoulder joints Positioning further facilitated by motions of spine Scapulohumeral Rhythm

22
Scapulohumeral Rhythm
The ratio has considerable variation among individuals but is commonly accepted to be 2:1 (2 of glenohumeral motion to 1 of scapular rotation) overall motion. During the setting phase (0 to 30 abduction, 0 to 60 flexion), motion is primarily at the glenohumeral joint, whereas the scapula seeks a stable position. During the mid-range of humeral motion, the scapula has greater motion, approaching a 1:1 ratio with the humerus later in the range, the glenohumeral joint again dominates the motion
 overall motion. During the setting phase (0 to 30 abduction, 0 to 60 flexion), motion is primarily at the glenohumeral joint, whereas the scapula seeks a stable position. During the mid-range of humeral motion, the scapula has greater motion, approaching a 1:1 ratio with the humerus. later in the range, the glenohumeral joint again dominates the motion.")
24
Movements of the Shoulder Complex
Muscles of the Scapula Muscles of the Glenohumeral Joint Flexion Extension Abduction Adduction Medial and Lateral Rotation of the Humerus Horizontal Adduction and Abduction at the Glenohumeral Joint

25
Horizontal Adduction and Abduction at the Glenohumeral Joint
HORIZONTAL ADDUCTION: Anterior to joint: Pectoralis major (both heads), anterior deltoid, Coracobrachialis Assisted by short head of biceps brachii HORIZONTAL ABDUCTION: Posterior to joint: Middle and posterior deltoid, infraspinatus, teres minor Assisted by teres major, Latissimus dorsi
, anterior deltoid, Coracobrachialis. Assisted by short head of biceps brachii. HORIZONTAL ABDUCTION: Posterior to joint: Middle and posterior deltoid, infraspinatus, teres minor. Assisted by teres major, Latissimus dorsi.")
26
Loads on the Shoulder Shoulder joint has to bear most of the weight amongst all other articulations of the shoulder girdle Shoulder has to provide direct mechanical support Large leverage More compressive forces on the shoulder joint Deltoid produces upward shear forces as compared to rotator cuff which produces downward shear forces.

27
Arm Abduction and Flexion
27

28
Muscle Action on the Shoulder Girdle
28

29
Loads on the Shoulder Arm segment moment arm:
Perpendicular distance between weight vector and shoulder Large torques from extended moment arms countered by shoulder muscles Load reduced by half with maximal elbow flexion

30
Common Shoulder Injuries
Dislocations Rotator Cuff Damage Impingement Theory Subscapular Neuropathy Rotational Injuries Ectopic calcification Hardening of organic tissue through deposit of calcium salts in areas away from the normal sites

31
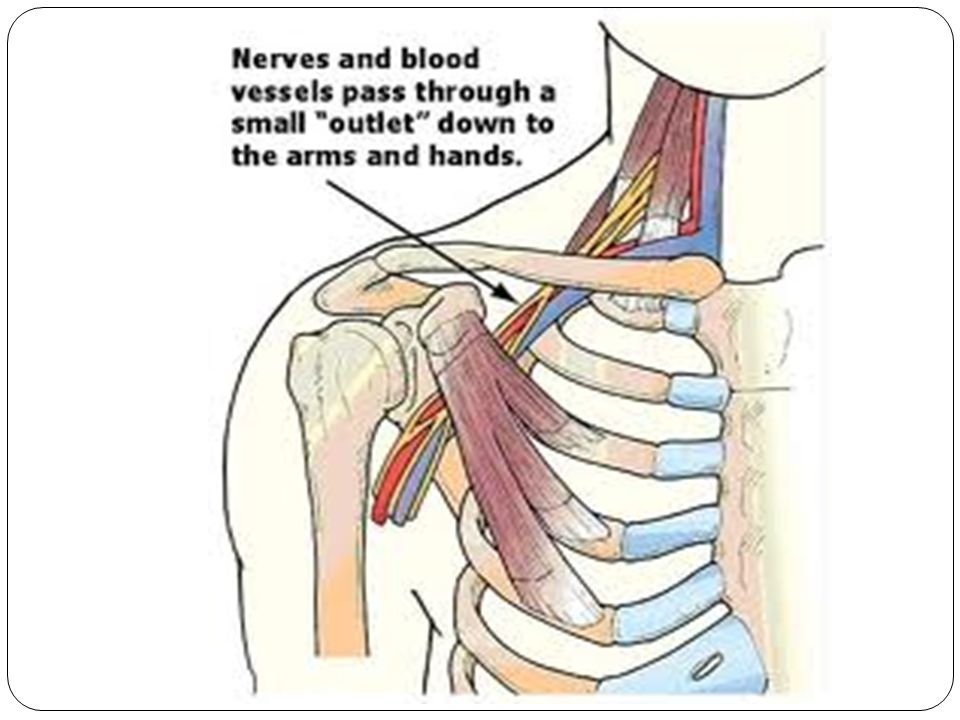
Subscapular Neuropathy
The typical patient is a young overhead athlete who reports vague posterior shoulder pain. Although, the athlete can have painless atropy presenting as supraspinatus and/or infraspinatus weakness, depending on the location of the suprascapular nerve. Because of the anatomy (see Functional Anatomy), more distal nerve injuries are often relatively painless. In particular, nerve injuries at the spinoglenoid notch that result in selective denervation of the infraspinatus muscle may be painless condition.. Based on anatomic considerations, athletes with more proximal lesions of the suprascapular nerve that affect both the supraspinatus and infraspinatus muscles are more likely to have pain and symptom- limited function.
, more distal nerve injuries are often relatively painless. In particular, nerve injuries at the spinoglenoid notch that result in selective denervation of the infraspinatus muscle may be painless condition.. Based on anatomic considerations, athletes with more proximal lesions of the suprascapular nerve that affect both the supraspinatus and infraspinatus muscles are more likely to have pain and symptom- limited function.")
32
Dislocations Loose structure of shoulder leads to extreme mobility = less stability It may be Posterior, Anterior or inferior dislocation Mechanism??//// Contact sports Glenohumeral capsular laxity Strengthening of shoulder musculature posterior dislocations that combines flexion, adduction, and internal rotation, such as falling on an outstretched arm. Ant.dislocation:abduction and external rotation forces .

33
Anterior dislocation

34
Elbow Articulations Humeroulnar Joint Humeroradial Joint
True elbow joint Strong bony configuration Hinge joint Humeroradial Joint Slides along capitulum Modified ball and socket joint Provides no ABD or ADD Proximal Radioulnar Joint Annular ligament Movements Interosseous membrane

35
Joint Capsule Anterior Posterior Medial Lateral Large, loose and weak
Reinforced by other ligaments

36
Loads on the Elbow Large loads generate by muscles that cross elbow during forceful pitching/throwing Also in weight lifting, gymnastics Extensor moment arm shorter than flexor moment arm Tricep attachment to ulna closer to elbow joint center than those of the brachialis on ulna an biceps on radius Moment arm also varies with position of elbow

37
Wrist and Hand Bones Wrist Scaphoid Lunate Triquetrium Pisiform
Trapezium Trapezoid Capitate Hamate

38
Wrist and Hand Bones Hand Metacarpals Phalanges 2-5 Proximal Middle
Distal Phalange 1 (Thumb)
")
39
Closer Look at the Carpal Tunnel
Structures within Tunnel FDS FDP FPL Median Nerve

40
Movements of the Wrist Sagittal and frontal plane movements
Rotary motion Flexion Extension and Hyperextension Radial Deviation Ulnar Deviation

41
Joint Structure of the Hand
Carpometacarpal (CM) Metacarpophalangeal (MP) Interphalangeal (IP)
 Metacarpophalangeal (MP) Interphalangeal (IP)")
42
Common Injuries of the Wrist and Hand
Sprains and strains fairly common, due to breaking a fall on hyperextended wrist Certain injuries characteristic of sport type Metacarpal fractures and football Ulnar collateral ligament and hockey Wrist fracture and skate/snowboarding Wrist in non-dominant hand for golfers Carpal Tunnel Syndrome

43
Swan neck deformity=== mallet finger Boutonniere deformity
Swan neck:t (DIP Phyperflexion with PIP hyperextension). BUTTONAIRE:way (PIP flexion with DIP hyperextension). It
. BUTTONAIRE:way (PIP flexion with DIP hyperextension). It.")
44
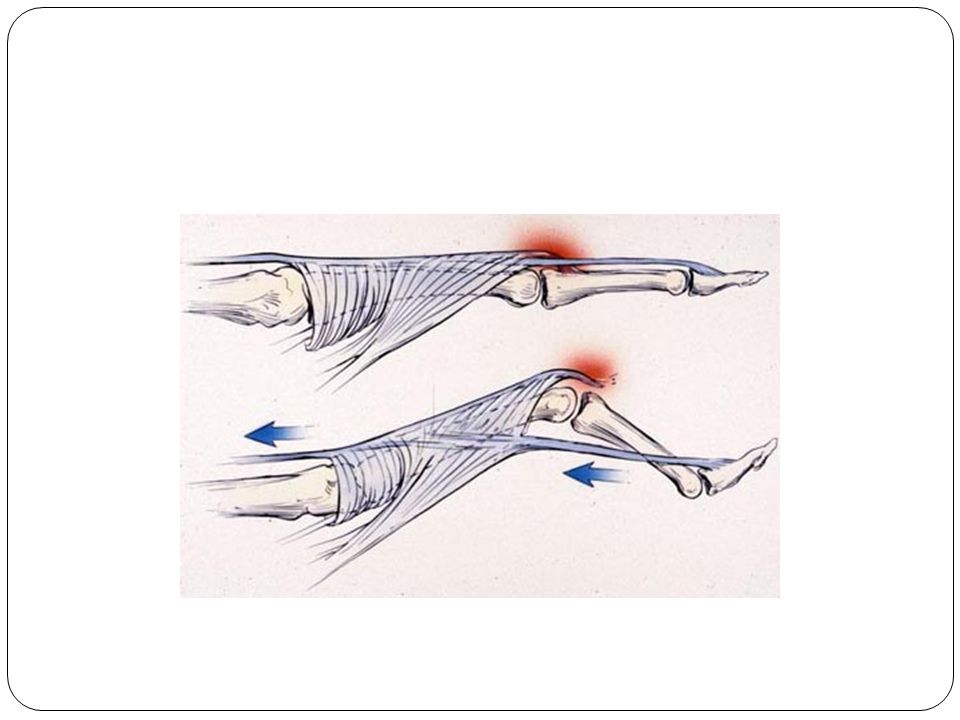
Mallet finger In medicine, mallet finger, also baseball finger,[1] dropped finger, dolphin finger, "Virgin Finger", "Hannan Finger" and (more generally) extensor tendon injury, is an injury of the extensor digitorum tendon of the fingers at the distal interphalangeal joint (DIP).[2] It results fromhyperflexion of the extensor digitorum tendon, and usually occurs when a ball (such as a softball,basketball, or volleyball), while being caught, hits an outstretched finger and jams it - creating a ruptured or stretched extensor digitorum tendon.
 extensor tendon injury, is an injury of the extensor digitorum tendon of the fingers at the distal interphalangeal joint (DIP).[2] It results fromhyperflexion of the extensor digitorum tendon, and usually occurs when a ball (such as a softball,basketball, or volleyball), while being caught, hits an outstretched finger and jams it - creating a ruptured or stretched extensor digitorum tendon.")
Similar presentations