Download presentation
Presentation is loading. Please wait.

1
Normal Postparutm Period
Lecturer: Eman Abu-Alfawaris

2
Objectives By the end of this session, the student should be able to:
Define postpartum period. Enumerate characteristics of PPP. Describe physiological changes during PPP. Explain psychological changes during PPP. Assess woman for uterine involution, lochia, perineum, uterine consistency.

3
Definition of puerperium:
The first 6 weeks "40 days" following the birth of an infant are known as the post partum period or puerperium, in which maternal body in general and genital organs in particular return to nearly pre-pregnancy state. Puerperium is divided into immediate postpartum (first 24 hours), early postpartum (first week), and late postpartum "from second week till end of six weeks".
, early postpartum (first week), and late postpartum from second week till end of six weeks .")
4
Characteristics of PPP:
Involution: of the reproductive organs or regressive changed. Lactation: is initiated. Recovery: from physiological effort & emotional symptoms “Recuperation”.

6
Post Partum Physiological Changes:
Endometrial regeneration is completed by about 3 weeks except for the placental site, where regeneration is not complete until 6 weeks. A. Reproductive system: 1. Involution of the uterus:- Involution refers to the changes that reproductive organs, especially the uterus, under go after childbirth to return to their nearly pre-pregnancy size and condition. The involution occurs by two processes: Involution rate: Immediately following delivery, the size of uterus as large grapefruit and can be palpated midway between the symphysis pubis and umbilicus, Within an hour, the fundus rises to the level above the umbilicus and should remain at this level for about 24 hours the uterus now weighs approximately 1000 gm. After 24 hours, the fundus begins to descend by approximately 1cm, or one fingerbreadth, per day, so that by the 10th day it is in the pelvic cavity and cannot be palpated abdominally.

7
Objectives

8
Characteristics of PPP:
Factors that enhance involution include: Uncomplicated labor and birth. Breast-feeding. Early, frequent ambulation. Factors that slow uterine involution include: Prolonged labor. Incomplete separation and expulsion of placenta. Previous labors. Distended (full) bladder. Anesthesia.
 bladder. Anesthesia.")
10
Assessment of involution of uterus after childbirth– 2 days after childbirth

11
Lochia: It is the uterine discharge coming through the vagina during the first 3-4 weeks or the post partum. It is alkaline in reaction; the amount is more than the menstrual flow, with fleshy odor. It contains blood, fibrin, leucocytes, dead decidual tissue, vaginal cells, peptone, cholesterol, and numerous nonpathogenic bacteria.

12
types of Lochia Type Dases Colors Componants Lochia rubra:
Lasts from the 1st post partum days, to the 4th day Red in color fair amount of blood shreds of the deciduas amount of chorion, aminiotic fluid, lanugo hair, vernix caseosa fatty epithelial cells, leukocyte Lochia serosa: 4-9 days Pinkish yellow discharge containing less blood and more serum leukocyte , microorganism Lochia alba: 10th day until 2-6 weeks postpartum . Creamy or white colored leucocytes and mucus , epithelial cells, microorganism .lochia serosa has strong odor

13
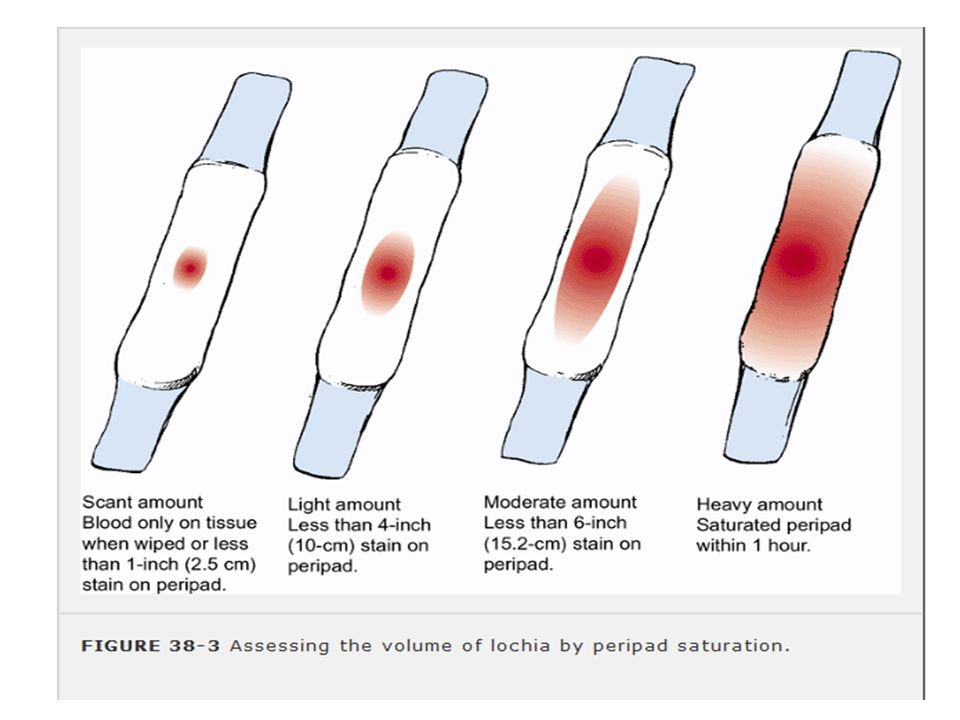
according to the amount the lochia classify to
scant lochia: less than 2-5 cm blood on the perineal pad light or mild lochia: less than 10cm blood on the perineal pad\hrs moderate lochia: less than 15cm stain perineal pad\hrs heavy lochia: 1 saturated pad\hrs sever lochia : more than 1 saturated pad \hrs

15
2. Cervix: Small tears or lacerations may be present, and the cervix is often edematous. Rapid healing takes place, and the end of the first week the cervix feels firm and the external so is the width of a pencil. The internal os closes as nearly before pregnancy, but the shape of the external os is permanently changed. It remains slightly open and appears slit-like rather than round, as in the nulliparous women. Complete cervical involution may take 3-4 months and child birth result in a permanent change in an cervical OS from round to elongated.

16
3. Vagina: The vagina diminishes in size, but not as the pregravida state. Rugea reappears in the third week. These are small skin folds in the lower part, dark red in color. The vagina and vaginal introitus are greatly stretched during birth to allow passage of the fetus. Soon after childbirth, the vaginal walls appear edematous, and multiple small lacerations may be present. The hymen is permanently torn and heals with small, irregular tag of tissue visible at the vaginal introitus.

17
the site of placental attachment require 6-7 weeks to heal
the site of placental attachment require 6-7 weeks to heal. In process called Exfoliation 4. Vulva: Edema, minute or frank laceration may be seen immediately after labor. Edema disappears gradually in a few days while lacerations, if not properly mended by sutures, may lead to the formation of a post partum ulcer.

18
5. Perineum: The appearance of the perineum will vary greatly, depending on the type and extent of the episiotomy or laceration. Commonly the soft tissues of the perineum are edematous and bruised. Ecchymosis due to rupture of surface capillaries.

19
Resumption of Ovulation and Menstruation:
Most non-nursing mothers resume menstruation within 7 to 9 weeks after childbirth. In lactating mothers, menstruation usually reappears not earlier then 3-4 months, and some times as late as 24 months. The first period is generally profuse and prolonged. It should be mentioned that ovulation can commence in the absence of menstruation, and another pregnancy can occur.

20
B. Cardiovascular System:
Body weight: Loss of weight is observed during the first l0 days particularly in the non-lactating mothers. There is about a 4 – 5 kg loss of body weight (sometimes 8 kg) due to evacuation of uterine contents and diuresis. B. Cardiovascular System: 1. Cardiac out put: Despite the blood loss and transient increase in the maternal cardiac output occurs following childbirth. This increase is caused by Increased flow of blood back to the heart when blood from the uteroplacental unit returns to central circulation. Mobilization of excess extracellular fluid into the vascular compartment. The rise in cardiac output, which persists for about 48 hours after childbirth. Decreases gradually and return to normal level by 12 weeks after childbirth.
 due to evacuation of uterine contents and diuresis. B. Cardiovascular System: 1. Cardiac out put: Despite the blood loss and transient increase in the maternal cardiac output occurs following childbirth. This increase is caused by Increased flow of blood back to the heart when blood from the uteroplacental unit returns to central circulation. Mobilization of excess extracellular fluid into the vascular compartment. The rise in cardiac output, which persists for about 48 hours after childbirth. Decreases gradually and return to normal level by 12 weeks after childbirth.")
21
2. Blood volume: Following delivery, despite 300 to 500 ml of blood loss during normal vaginal delivery, and ml is lost in cesarean births, excess blood volume, which was necessary during pregnancy, remains in the intravascular compartment and in interstitial spaces.

22
The body rids itself of the excess fluids by two methods
1.Diuresis: “increased excretion of urine” is facilitated by a decline in the adrenal hormone aldosterone, which is increased during pregnancy to counteract the salt-wasting effect of progesterone. urinary output of 3000 ml per day is not common for the first few days of the post partum period. 2. Diaphoresis “profuse perspiration” also rids the body of excess fluids through skin "sweating often occurs at night"

23
3. Coagulation: During pregnancy, plasma fibrinogen necessary for coagulation increased as a protection against post partum hemorrhage. As a result, the mother’s body has a great ability to form clots and thus prevent excessive bleeding. 4. Blood values: The white blood cells count increasing /mm up to or even /mm during postpartum A moderate increase in the fibrinogen and sedimentation rate occurs during the first postpartum period, and then gradually gets back to normal values.

24
HB% also diminishes, but not proportionately, decrease in the homatocrit occurs during the plasma increases and thus dilutes the concentration of blood cells and other substances carried by the plasma. In the absence of complications and with proper diet and hygiene, RBC count and content, and the blood constituents, usually return to the non-pregnant levels in 4-6 weeks. If the patient is Rh negative, evaluate her need for RhO(D) immune globulin (RhoGAM). If indicated, administer the RhoGAM within 72 hours of delivery
 immune globulin (RhoGAM). If indicated, administer the RhoGAM within 72 hours of delivery.")
25
5. Vital signs: at least twice daily and more frequently if indicated: temperature : may increase in the first 24 hrs reach to 38 c after delivery ,because of the dehydration during labor so encourage fluid intake . pulse : decrease pulse rate during the 1st week to beat\mint(24-48 hrs), if increase you should think of hemorrhage, anxiety, excitement.pain, visitor Blood pressure : should be unchanged , if BP >140\90mmhg may indicate postpartum hemorrhage. Respiratory rate: unchanged . Respiratory function Returns to normal by approximately 6 to 8 weeks postpartum
, if increase you should think of hemorrhage, anxiety, excitement.pain, visitor. Blood pressure : should be unchanged , if BP >140\90mmhg may indicate postpartum hemorrhage. Respiratory rate: unchanged . Respiratory function. Returns to normal by approximately 6 to 8 weeks postpartum.")
26
Constipation may be present as a result of: Intestinal atony.
C. Gastrointestinal System: Thirst is present due to the marked fluid loss through sweat and urine. Tendency to atony of the gastrointestinal tract, with flatulence and constipation. Constipation may be present as a result of: Intestinal atony. Anorexia after labor. Loss of body fluids. Laxity of the abdominal wall. Hemorrhoids, perineal trauma and episiotomy. Reflex inhibition enema in labor.

27
Normal bowel function returns approximately 2 to 3 days postpartum
Gall bladder contractility increases to normal, allowing for expulsion of small gallstones. -After cesarean section, bowel tone returns in few days and flatulence causes abdominal discomfort

28
D. Urinary system The bladder of the postpartum woman has an increased capacity and has lost some of its muscle tone. During childbirth the urethra, bladder, and tissue around the urinary meatus may become edematous and traumatized. This often results in diminish sensitivity to fluid pressure, and many mothers have no sensation of needing to void even when the bladder is distended. Urinary retention and over distention of the bladder may cause two complications: 1.Urinary tract infection Post partum hemorrhage.

29
Changes in composition of urine:-
Mild proteinuria may occur as a result of the breakdown of uterine cells. common for 1 to 2 days after delivery in 50% of postpartum women. The urine may also test positive for acetone / ketonuria resulting from dehydration during a prolonged labor. Lactoseuria may occur in breast-feeding woman as a result of the lactation process. Bladder tone returns between 5 and 7 days

30
E. Musculoskeletal system:
Muscles and joints: During the first few days, levels of the hormone relaxin gradually subside. Ligaments and cartilage of the pelvis begin to return to their pre-pregnancy position. This can cause hip or joint pain that interferes with ambulation and exercise. Good body mechanics and correct posture are important during this time to prevent low back pain and injury to the joint

31
Abdominal wall: During pregnancy, the abdominal walls stretch to accommodate the growing of the fetus and muscle tone diminished. Many women, expecting that the abdominal muscles will return to the pre-pregnancy condition after labor, are dismayed to find the abdominal muscles weak, soft, and Flabby. The longitudinal muscles of the abdomen may also separate (diastasis recti) during pregnancy. The separation may be minimal or sever.
 during pregnancy. The separation may be minimal or sever.")
33
F. Integumentary system:
After birth, the skin gradually reverts back to pre-pregnancy state. The melanocyte-stimulating hormone (MSH) levels, which caused hyperpigmentation during pregnancy decreases rapidly after childbirth that result in disappear of chloasma and linea nigra by 6 week. Skin erythema, which may develop during pregnancy as a result of increased estrogen level, gradually disappear. Steria gnavidarum which develop on the abdomen, thighs, and breasts, gradually become silvery lines and less noticeable, but don’t disappear completely Hair loss can increase for the first 4 to 20 weeks postpartum and then re-growth will occur, although the hair may not be as thick as it was before pregnancy.
 levels, which caused hyperpigmentation during pregnancy decreases rapidly after childbirth that result in disappear of chloasma and linea nigra by 6 week. Skin erythema, which may develop during pregnancy as a result of increased estrogen level, gradually disappear. Steria gnavidarum which develop on the abdomen, thighs, and breasts, gradually become silvery lines and less noticeable, but don’t disappear completely. Hair loss can increase for the first 4 to 20 weeks postpartum and then re-growth will occur, although the hair may not be as thick as it was before pregnancy.")
34
G. Endocrine system: Following expulsion of the placenta, a fairly rapid decline occurs in placental hormones such as estrogen, progesterone, human placental lactogen, and human chronic gonadotrophin. Adrenal hormones, such as aldosterone, return to pre-pregnancy levels. FSH remains low for about 12 days then begin to rise to initiate new menstrual cycle, first cycle is frequently an ovulatorty.

35
Neurological function:
Discomfort and fatigue are common. Frontal and bilateral headaches are common and are caused by fluid shifts in the first week postpartum.

36
Physiology of lactation:
Lactation consists of two distinct processes: "Milk production After labor, sudden fall of estrogen and progesterone levels leads to marked rise of prolactin level. This hormone stimulates the alveolar cells leading to milk secretion. Milk ejection:Stimulation of the nipple and areola (by suckling), leads to increased production of oxytocin from posterior pituitary. This hormone acts on the myoepithelial cells which line the ducts causing its contraction. Milk is ejected into the lactiferous ducts and cysternae, where it is readily available to the suckling infant (Let down reflex" ) .
, leads to increased production of oxytocin from posterior pituitary. This hormone acts on the myoepithelial cells which line the ducts causing its contraction. Milk is ejected into the lactiferous ducts and cysternae, where it is readily available to the suckling infant (Let down reflex ) .")
37
"Nipple erection reflex" results also from stimulation of the nipple by suckling or tactile stimulation of the nipple. This is of great help to the baby during suckling.

38
Factors Affecting Milk Production
1- Regular complete breastfeeding. 2- Suckling abilities of newborn. 3- Maternal health, and Nutrition. 4- Psychological factors. 5-Hormones : Prolactin, Oxytocin, Thyroxin, Growth hormone, in addition to Progesterone and estrogen. Normal levels of these hormones are essential for initiation & maintenance of lactation.

39
Composition of Breast Milk:
There is a higher fat content at midday for example and in the hind milk white the fore milk always contains more water protein. BM is alkaline hued, bluish white in color. Average sample for 24hr is said to contain protein 1.5% fat 3.5% mineral salts 0.2% water 87.8% vitamins as in colostrums calorific value 80 kilo joules per 30ml.

40
Post Partum Psychological Changes:
After delivery, the woman may progress through Rubin's stages of taking in, taking hold, and letting go. Dependent or “ Taking –in phase. : It takes 2-3 days, Woman exhibits passive, dependent behavior. the mother's first concern is with her own needs Dependent – independent or “ Taking- hold “ phase. It starts the 3rd day postpartum & lasts about 10 days Openness to teaching on care of self and neonate. .

41
Interdependent or “ letting – go “ phase:
Mothering functions become more established there are two separations that the mother must accomplish. One is to realize and accept physical separation from the infant Second is to relinquish her former role as a childless person and accept the enormous implications and responsibilities other new situation. She must adjust her life to the relative dependency and helplessness other child.

42
Management of Postpartum Period
Early needs of the mother: 1- Observation and recording to: Vital signs Check vital signs 2 times daily "morning and evening". Observe for symptoms of hypovolemic shock and hemorrhage. A temperature of 38c or above, for two consecutive days after the first24hrs.is considered an early sign of puerperal infection Bradycardia is a normal physiological phenomenon

43
Uterus Palpate the uterus daily to assess firmness level of fundus, and the rate of involution of the uterus. It should be well contracted, central and involutes gradually at the rate of about 1cm daily during the first seven to ten days of the puerperium.

44
Breast: The breasts are examined to note their tension and consistency, and the signs of infection. In breast-feeding mothers, the amount and flow of milk and the condition of the nipples and areola should be observed. Perineum Observe perineum and suture line if present, for redness, ecchymosis, and edema or gapping. Check healing and cleanliness During the examination haemorrids may be noted and appropriate treatment advised.

45
Lochia Check lochia for color, amount, odor, consistency and blood clots.

46
Urine out put The urine out put is usually recorded for the first 24 hours after delivery to ensure that the woman is passing and adequate amount of urine. Legs The midwife examines the patient's leg for pain and edema

47
Emotional state Phases of developing maternal role. Post partum blues. 2. Rest and sleep: Provide for sufficient periods of rest and sleep to maintain physical and mental health, as to promote lactation (8hrs nighttime sleep and 2hrs after noon-nap are needed).
.")
48
Provide diet high in proteins and calories to restore tissues.
A daily requirement of cal/day is needed in the form of a well balanced diet rich in 1st class proteins, calcium, iron, vitamins, thiamine, riboflavin and ascorbic acid Liberal amounts of fluids are required "the daily fluid intake should be liters" (e.g. milk, juice ….ect."

49
4. Hygiene: The women should be taken shower daily. The vulva and perineal care include washing or swabbing with warm water and antiseptic solution, the area must be kept clean and dry and free from infection. The perineum must be inspected daily if there are sutures to see that healing is taking place. Non-absorbable sutures are removed on the fifth or sixth day. Breast care should be done before and after feeding. The nurse teaches the mother the technique of breast care and encourages her to initiate breast-feeding.

50
5. Breast-feeding Advantages of Breast Feeding For baby: Immunological properties help prevent infections. Provides nutritional needs. Easily digested. Less sodium and protein than in cow's milk; puts less stress on newborn's kidneys. Calcium is better absorbed. Least allergenic food for infant. Promotes development of facial muscles, jaw, and teeth. Less likely to be overfed; less obesity. Has natural laxative effects. Fulfilling psychological needs.

51
For the mother: Oxytocin release aids uterine involution. Strong mother-infant relationship. Convenient; always available; no preparation. Cost effective. Less incidence of cancer breast. Natural contraception.

52
Breast feeding technique:
Clean the breast before and after feeding. Mother Clothes should not be tight over breast & clean. Wash hand before nursing her infant. The infant should be hungry, dry and warm. The mother should be in comfortable. Position either lying on her side or sitting up position.

53
Nursing role for promotion of breast-feeding:
1- Inform all pregnant women about the benefits and management of breast-feeding. 2- Help the mothers to initiate the breast-feeding within half-hour of birth. 3- Emphasize to mother the benefits of breast-feeding. 4- Teach mother the correct technique for .successful feeding. 5- Support them & their babies to adapt to new situation.

54
6- Give advice to proper diet, exercise, rest, and fluid intake, care of the breast, clothing and bathing. 7- Emphasize the role of father in sharing the rearing responsibility & providing support for the mother. 8- Raising awareness of the importance of child spacing for maternal & child health. 9- Arrange for close contact of mothers with their premature babies through encourage them to handle, or touch them. 10- Teach mothers how to express their milk with most hygiene for their pre-term baby. 11- Instruct mother about breast self examination & breast care. 12- The nurse should advice all mothers about the practice that help successful breast-feeding. 13- Instruct mothers about the contraceptive effect of breast-feeding.

55
Both supine and semi-sitting positions should be avoided.
14- The maternal child health care educator must help parents learn how to identity breast-feeding problems and how to manage it. 15- Practice rooming in-allow mothers and babies to remain together 24 hours a day 6. Proper positioning: During the first 8hrs.after labor, the mother is allowed to sleep in any comfortable position. After that, prone position or either lateral positions should be encouraged in order to facilitate involution and to help drainage of lochia. Sitting position is also recommended since it promotes contraction of the abdominal muscles, aids pelvic circulation, and helps drainage of lochia Knee-chest position is indicated in certain conditions because it prevents RVF of the uterus and hastens its involution Both supine and semi-sitting positions should be avoided.

56
Side-lying Football Position C Position Cradle Position

57
7. Ambulation: Encourage early ambulation to prevent blood stasis and deep venous thrombosis. Heavy activities are avoided to prevent complications. 8. Promote bladder and bowel function: Bladder Voiding should be encouraged within 6-8hrs after labor. If no urine is passed after 12 hrs. Initiate simple nursing measure to induce voiding. If failed, catheterization, under complete a septic technique is performed.

58
Bowel There may be no bowel action for a couple of days because the bowel has probably been emptied during labor. Glycerin suppository may be used to relieve constipation.

59
8. Post natal exercise: Encourage post partum exercise which promotes circulation. Lessen the possibility of venous thrombosis and restore the muscle tone of the abdominal wall and pelvic floor. Postnatal exercises help to give the patient a sense of well being. Certain patients, such as those suffering from heart lesions, should not be allowed to perform all the exercises, though even they may be encouraged, on medical advice to take gentle exercise. Deep breathing and free movements in the bed should be encouraged from the day of the delivery. On the second day the following exercises may be done provided the labor has been normal and the patient is in health. In prescribing exercises discretion must be used and the exercises must be adapted to the individual. In hospital the exercises will probably be directed by a physiotherapist.

60
Breathing exercises:
Deep-breathing exercises should be performed as described for antenatal period, with the patient lying flat in be stretch, stiffen and reflex the muscles of the right and let leg alternately.

61
Pelvic floor tone. Several exercises may be performed:
Lie flat on the back with body relaxed. Tighten the anus for ten seconds as though trying to control a loose motion or retain an enema. Repeat six times, and then rest for one minute. Carry out the same procedure eight times. Lie flat on the bed and forcely abduct the thighs against resistance (the nurse attempts to hold the thighs together while the patient pushes them apart. Repeat slowly six times. Later the same exercise may be carried out, but with the nurse holding the patient’s Knees together instead of the thighs. Lie flat upon the back with the hands upon the hips and elevate the feet alternately, counting one to six, up, and one to four, down. Lie flat with the hands resting lightly on the abdominal wall. Then slowly raise the head and shoulders. The patient must not push the chin forwards or the abdominal wall will be pushed outwards instead of contracting, nor must any weight be rested on the elbows. Sit up in bed with the hands clasped round the flexed knees and endeavor to touch the knees with the chain. The nearer the head and knees approach the greater the contraction of the abdominal muscles.

62
Strengthening the muscles generally:
The patient, sitting up in bed and bedding forward with legs outstretched places her hands on her ankles. The trunk is then stretched backwards and the arms drawn up and bent to imitate rowing, the knees are slightly flexed at the same time.

63
Late needs of the mother
Health education and counseling The midwife nurse plays an important role as health educator and counseling which should provide the woman health education and counseling about: Breast feeding, definite, technique and position. Resumption of sexual relations. Include information about when to expect menstruation.

64
Post natal exercise, hygiene, rest, sleep and nutrition.
The care of the baby which includes hygiene, prevention of infection, feeding and giving him love and sense of security feel her about the advantages of rooming in. Family planning methods for spacing of pregnancy. Stress the importance of post partum examination. Visits and follow up to assess involution, general health and well being of the mother before discharge.

65
Care of the newborn infant:
Observing the general condition. Checking the cord. Checking the infant's physical needs. Cleanliness, feeding, warmth, sleep, protection from unsuitable environment. Checking psychological needs: bonding and attachment. Carry out partial or complete bath to ensure cleanliness and comfort. Use proper clothing to keep the infant warm. Perform cord dressing. Encourage early breast-feeding. Ensure adequate hours of sleep. Protect from environmental hazards. Discuss infant care with mother. Cleanliness, handling, clothing, cord care, feeding, bonding, diapering, circumcision of male infant, immunization, weaning, and community resources. Encourage early skin to skin contact, bonding and attachment.

66
Postpartum visits The first visit : The visit is carried out 3-4 weeks after labor in order to assess the degree of involution of the body in general and of the genital tract in particular. General and local examination is performed. The client condition is evaluated through various medical and nursing activities that include: Measuring and recording of blood pressure. Estimation of the hemoglobin percentage, and aggressive treatment of anemia, if present.

67
Urine analysis for sugar and albumen.
Thorough examination of breasts and nipples for early detection and treatment of abnormalities. Examination of abdominal muscles, perineum, perineal wounds and nature of lochia to asses the degree of involution of these parts, and to exclude the presence of infection. Careful and thorough examination of: size of the uterus, its position, tenderness, the condition of the cervix (such as laceration or erosions) as well as the condition of the pelvic floor. Management of any lesion should readily start.
 as well as the condition of the pelvic floor. Management of any lesion should readily start.")
68
The second visit: The visit is done at the end of the 6th postpartum week. It is carried out along the same lines as the postnatal visit with the institution of more active treatment for certain lesions: If retroversion flexion (RVF)is still present a pessary must be inserted Cervical erosion may call for cauterization. Subinovlution calls for more energetic treatment. Health teaching items at this time include advice in relation to:
is still present a pessary must be inserted. Cervical erosion may call for cauterization. Subinovlution calls for more energetic treatment. Health teaching items at this time include advice in relation to:")
69
Sexual intercourse, which should be prohibited during the six postpartum weeks.
Spacing of pregnancies and counseling about the appropriate contraceptive method, which should be prescribed and may be started at once? If the prolapsed of genital tract is present, it should be treated by pelvic floor muscle exercises and / or the insertion of a ring pessary. The patient should be advised to abstain from bearing down. Chronic cough and constipation should be treated for this purpose, however, operative treatment is not considered before the lapse of six months when total involution of the genital tract is established. Health education to puerperal women at this time should also include instructions related to the possibility of encountering menstrual irregularities during the following months. This irregularities range from complete amenorrhea to oligomenorrhea, hypomenorrhea or polymenorrhea. Bleeding is expected at the end of 6th puerperal week in the majority of patients. in non lactating mothers, however , menstruation usually appears after 6-8 weeks .

70
The third visit: This is performed at the end of 3 months by which time complete involution of the genital tract has occurred. General and local examinations are carried out, and any discovered lesion should be dealt with: Cervical erosions must be cauterized. Persistent RVF and / or prolapsed should be managed properly. If lactation amenorrhea is present, the client should be instructed that this is not a bar against another pregnancy, and suitable contraceptive measures should be instituted.

71
Minor Discomforts during the Postpartum Period
They are minor complaints felt by the parturient during postpartum period. Simple nursing measures (interventions) are needed to alleviate these complaints.
 are needed to alleviate these complaints.")
72
After-pains: It is a spasmodic colicky pain in the lower abdomen during the early postpartum, days due to vigorous contractions of the uterus. It is more common and more severe in multiparous due to weak muscle tone. Conditions with increased intra-abdominal pressure e.g. polyhydraminios, multiple pregnancy, large size infant. Predisposing factors: Presence of blood clots, piece of membranes or placental tissue. Breastfeeding increases after-pain.

73
Nursing management: Simple uterine Massage.
Reassurance and simple explanation of the cause. Proper positioning (prone, sitting). Offering warm drinks, Mild sedatives on doctor's orders (before feeding). Avoid full bladder. Encourage abdominal muscle exercises and pelvic floor muscle exercises. After-pains:
. Offering warm drinks, Mild sedatives on doctor s orders (before feeding). Avoid full bladder. Encourage abdominal muscle exercises and pelvic floor muscle exercises. After-pains:")
74
Urinary Retention It is the inability to excrete urine, i.e. urine is accumulated within the urinary bladder. A common complaint during the first few days after labor. Causes: Laxity of the abdominal muscles. Inability to micturate in the recumbent position. Reflex inhibition due to stitched perineum or bruised urethra. Atony of the bladder. Compression of the urethra by edema or haematoma.

75
Nursing management: Urine should be passed approximately 8-12 hrs after delivery. If not, the following measures should be attempted: Perineal care with warm water. Privacy and reassurance, Warm bedpan. listening to the sound of running water Hot-water bottle over the symphysis pubis If these measures fail, catheterization should be performed using complete aseptic technique.

76
Constipation An abnormal infrequent and difficult evacuation of feces may occur during the first few days postpartum. Nursing management: Health teaching should consider the following: Diet rich in roughage. Increase fluid intake. Milk before bedtime. Exercises. After 72 hrs a glycerin suppository, or mild laxative, may be administered as ordered.

77
Engorged Breast It is an accumulation of increased amounts of blood and other body fluids as well as milk in the breasts. This condition occurs frequently about the 3rd day postpartum, especially in primipara. It is due to lymphatic and venous engorgement, and is relieved when milk comes out. Causes: Inadequate and/or infrequent breast-feeding. Inhibited milk ejection reflex. Signs and symptoms: Breasts are firm, heavy (due to blocked ducts), swollen, tender and hot (37.8"C). Pain may be present leading to irritability and insomnia. The mother may refuse to nurse the infant.
, swollen, tender and hot (37.8 C). Pain may be present leading to irritability and insomnia. The mother may refuse to nurse the infant.")
78
Nursing management: Apply moist warm packs to the involved breast 2-3 minutes before each feeding Massage and manual expression of milk to relieve areola engorgement before feeding. This facilitates attachment. Cold application after feeding. A well-fitting bra should be used to provide support and comfort. Mild analgesics may be ordered. Syntocinon inhalation may be prescribed. In severe cases, administration of 2 doses of diuretic (as Lasix 40 mg) is effective
 is effective.")
79
Cracked Nipple Fissured nipple occurs in about half of the nursing mothers at one time or another. Nipple tenderness and soreness are usually the result of trauma and irritation. Causes: Improper antenatal care. Improper technique of breastfeeding. Unnecessary prolonged lactation. Flat or large size nipple--- excoriation. The use of irritating substances e.g. soaps, lotions. Conditions as candidiasis, and contact dermatitis. Engorgement of the breast. Signs and symptoms: Irritation of the nipple in the form of minute blisters or petechial spots. Persistent pain and tenderness. Bleeding. Inflammation signs.

80
Nursing management: Proper technique of breast-feeding should be followed. Apply moist heat and massage before feeding (3-5 min). Frequent, short feedings. Air/sun exposure. Avoid engorged breast. Avoid irritating materials. Use supportive bra. Mild analgesic and panthenol ointment may be used. Treatment of candidiasis and dermatitis.

81
Insufficient milk supply:
Physiological variations in milk secretion are often perceived as milk insufficiency. Nursing management: Encourage the mother to follow frequent breast-feeding. Mother should drink more fluids. Reduce outside activities that are strenuous. Avoid supplementary hour feeds. Nurse the baby every hour if necessary. Nurse in a relaxed position. Try to avoid distracting or up setting situation while breast-feeding. Breast-feed just as the baby wakes up before he can begin crying from hunger. Have a warm or cool drink each time the baby is breast-fed.

82
Leaking of breast milk:
Women who have active ejection reflexes often find that breasts leak milk during the first few weeks after delivery. Nursing management: The mother should put clean pieces of gauze or cloth inside the bra to soak up the milk. Change the clothes frequently. Breast care frequently.

83
Mastitis: - Is an infection of the parenchyma of the mammary gland usually occurring within the first 2-3 weeks of postpartum. It may progresses to cause breast Abscess.

84
Nursing management: Instruct the mother about self-administration of antibiotics, analgesics and antipyretic. Instruct the mother about personal hygiene. Breast care with water not using soap. Intermittent exposure of the nipples to air and changing of breast pads when wet. Breast feeding should be continued or pumped emptying the affected side to relieve engorgement. If abscess develops drain it. If feeding is too painful, maintain lactation through expression and offering the baby milk by spoon and cup.

85
Soaks of magnesium sulphate compresses in case of edema.
Perineal Discomfort It usually occurs due to presence of tears, lacerations, episiotomy and edema. Nursing management: Frequent perineal care under aseptic technique, (the area should be kept clean and dry). Soaks of magnesium sulphate compresses in case of edema. Expose to dry heat (electric lamp) will help the healing process. Health education that includes: Perineal self care. Position (lateral with a pillow between thighs). Diet: rich in protein. Sources of strain such as coughing, constipation and carrying heavy objects should be avoided. Encourage pelvic floor muscle exercises. Avoid infection. The use of cotton underwear.
. Soaks of magnesium sulphate compresses in case of edema. Expose to dry heat (electric lamp) will help the healing process. Health education that includes: Perineal self care. Position (lateral with a pillow between thighs). Diet: rich in protein. Sources of strain such as coughing, constipation and carrying heavy objects should be avoided. Encourage pelvic floor muscle exercises. Avoid infection. The use of cotton underwear.")
86
Postpartum Blues (Depression)
Rev a Rubin defined postpartum blues as "the gap between the ideal and reality: the new mother's expectations may exceed her capabilities, resulting in cyclic feelings of Depression". This condition is usually temporary and may occur in the hospital. The condition is partly due to hormonal changes, and partly due to the ego adjustment that Accompanies role transition.

87
Predisposing factors:
Signs and symptoms: Disturbed appetite and sleeping patterns. Discomfort, fatigue and exhaustion. Episodes of crying for no apparent cause. The mother may experience a let down feeling accompanied by irritability and tears which often relieves the tension. Guilt feeling at being depressed. Predisposing factors: The first pregnancy or pregnancy in late childbearing age. Social isolation. Ambivalence toward the woman's own mother. Prolonged, hard labor. Anxiety regarding finances. Marital disharmony. Crisis in the family.

88
Nursing management: Reassurance, understanding, and anticipatory guidance will help the parents become aware that these feelings are a normal accompaniment to this role transition.

Similar presentations