Download presentation
Presentation is loading. Please wait.

1
Reflections on the Use of Qualitative Research with Users – Benefits, Barriers and New Opportunities Jenny Ure

2
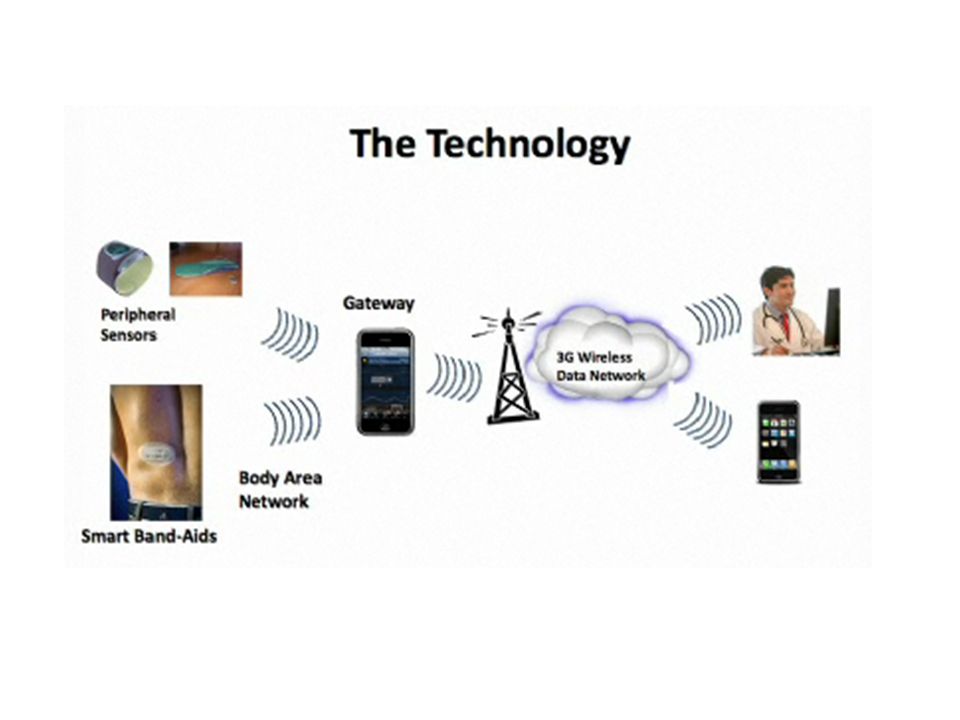
Care is now provided in an extended, digitally mediated environment where the problems and the opportunities are often unseen adn unreported qualitative research with users is increasingly needed to inform large scale clinical trials and service developments

3
I will present a few vignettes of how I have used qualitative and collaborative action research in different eHealth and Telehealth projects, highlighting theory and practice I will highlight some of the things that can go wrong in a qualitative research project, (which I which I had known at the start of my career!) and some of the strategies I have seen successful researchers adopt to avoid them
 and some of the strategies I have seen successful researchers adopt to avoid them")
4
CollectingCodingCommunicating Research in theory Research in the wild

5
1.Issues Collecting and Combining Data eHealth/HealthGrid Example

6
Patient Data integration across sites (horizontal) across scales (vertical …think Google Earth)
 across scales (vertical …think Google Earth)")
7
Seven HealthGrid projects PsyGrid NeuroGrid BIRN NeuroBase CARMEN DGEMap EMAGE P3G Observatory https://wikis.ac.uk/mod/Main_Page

8
Genes

9
1.sampling 2. collecting3. coding4. cleaning5. linkage6. analysis 7.use Recurring problem: solution scenarios at different stages the human process the technical process

10
Sampling, collecting scenarios Different populations Different collection protocols Different contexts and criteria for collection

11
Format?

12
Different study designs and procedures

13
Different Questionnaires

14
A 46:36 waist/hip ratio reading – is it an input error or just a typical sample from West Lothian Standardisation Strategies Do Not Ensure the Quality of Data Collection

15
Different Disease Effects or Different Scanner Calibration? Adapted from Keator et al (2006) Presentation to the UK-BIRN workshop
 Presentation to the UK-BIRN workshop.")
16
Strategies include... Wireless notepads for data collection Provenance metadata Links to original data Local QA/ethics/linkage committees Error trawls and spot checks combined with error-trapping software

17
Harmonising different tools and platforms? Microarray In situ hybridisation Scanners

18
Shared protocols? Trace a line around the region of interest in all subjects Compare differences in area across control and experimental groups Unambiguous?

19
A vision mediated by ´standard´ thresholds and protocols

20
…there are known unknowns; that is to say we know there are some things we do not know. But there are also unknown unknowns - - the ones we don't know we don't know.

21
The vision of seamless data sharing! Reliability of technology? Reliability of transmission? Usability of interfaces/kit? Patient factors? Local Factors? Unknown unknowns.....

22
Missing data i.e. data that was known but was not filled in Incomplete data - the patient ID specified but not the issuer of the patient ID Incorrect data - the patient's name being entered as "brain" Incorrectly formatted data Data in the wrong field - the series being described as “knee” Inconsistent data within a single file - patient's age inconsistent with scan date minus birth date. 30% Collection Errors ?

23
Effect or Artefact? Different equipment Different populations Different raters Different contexts Different protocols Different coding Different metadata

24
1.sampling 2. collecting3. coding4. cleaning5. linkage6. analysis 7.use Ethical/Legal Issues in Data Collection/Linkage. New technical infrastructures can outstrip the development of social governance structures the human process the technical process

25
Data linkage enhances knowledge discovery in relation to disease in relation to patients and their families DeCODE Different solutions cost, risk, benefit in different ways

26
Options - Role Based Access The de facto standard Persistent linked datasets more likely Getting access is easier Monitoring misuse is hard

27
An additional layer? Checking for risks arising from linkage between particular datasets

28
An additional human layer Linkage assessment panel Also combines ethical and quality roles Existing roles and responsibilities support effective intervention to enhance security and quality

29
Introduction NeuroGRID www.neurogrid.ac.uk is a three- year, £2.1M project funded through the UK Medical Research Council to:-www.neurogrid.ac.uk develop a Grid-based research environment to facilitate the sharing of MR and CT scans of the brain and clinical patient data in the diagnosis of psychoses, dementia and stroke bring together clinicians, researchers and e- scientists at Oxford, Edinburgh, Nottingham and London create a toolset for image registration, analysis, normalisation, anonymisation, real-time acquisition and error trapping ensure rapid, reliable and secure access, authentication and data sharing Imaging Issues: Artefact or Actuality? Researchers use innovative imaging techniques to detect features that can refine a diagnosis, classify cases, track normal or often subtle physiological changes over time and improve understanding of the structural correlates of clinical features. Variance is attributable to a complex variety of procedures involved in image acquisition, transfer and storage, and it is crucial, but difficult, for true disease-related effects to be separated from those which are artifacts of the process Acknowledgements The authors would like to acknowledge the support of the UK Medical Research Council (Grant Ref no: GO600623 ID number 77729), the UK e-Science programme and the NeuroGrid Consortium. Data Quality Issues: The Social Life of Information Challenge: The large scale aggregation of diverse datasets offers both potential benefits and risks, particularly if the outputs are to be used with patients in a clinical context. Thus aggregating data is a key issue for e-Health, yet data is not independent of the context in which it is generated. Within small communities of practice a degree of shared and updated knowledge and experience allows judicious use of resources whose provenance is known and whose weaknesses are often already transparent. The same is not true of aggregated data from multiple sources. Approach: Early use of prototypes to provide a ‘sandpit’ for promoting both technical and inter- community dialogue and engagement, and start the process of identifying, sharing and updating knowledge of emerging issues. Early trials with known datasets aim to generate an awareness of the types of variance that can arise and ways in which it might be minimized, harmonized, or made transparent to users Socio-technical Issues Aligning Technical and Human Systems Conclusions In organic communities, the processes of structuring collaboration, coordination and control structures happens as a matter of course. NeuroGrid is employing an early prototype to generate engagement and dialogue, to enable early discussion of requirements for more complex services, compute capability and workflows, as well as data quality and configurational issues. In addition to ameliorating the recurring issue of requirements ‘creep’, late in the design process, it allows disparate groups to engage with the real issues, and possible solutions in a shared context. For further information For information on this and related projects contact Jenny.Ure@ed.ac.uk or go to www.neurogrid.ac.ukJenny.Ure@ed.ac.uk www.neurogrid.ac.uk Challenge: Integrating the technical work of system building, with the socio-political work of generating the governance of the new risks and opportunities they generate Approach: The creation of real and virtual ‘shared spaces’ (e.g. via Access Grid) and the use of an early prototype for engagement in areas of shared professional concern, to help this new hybrid community develop its own rules of engagement, and start making collective sense of local requirements in relation to common project goals. Semantic Issues Il nome della rosa Challenge: Multi-site studies raise issues such as different naming conventions for files, different coding and classification systems, different protocols, and different conceptualisations of domains. Approach: The project agreed on core and node specific metadata and will use an OWL-based ontology (logic-based domain map) to allow human and machine-readable searching and basic reasoning across the datasets. In this there is a trade-off between the benefits of share-ability and automated reasoning, on the one hand, and the formalisation of concepts and relationships that are evolving. Challenge: Aligning and representing datasets at different levels of granularity. While NeuroGrid uses MR and CT scans, other relevant datasets such as diffusion tensor imaging, genetic, proteomic datasets also contribute to an understanding of neurological processes. Approach: The project is adopting a two –pronged approach developing task specific ontologies developing a reference ontology based on the Foundational Model of Anatomy adopted by the BIRN Human Brain Project. This allows a degree of alignment between datasets and ontologies in future collaborations Designing for e-Health: Recurring Scenarios in Developing Grid-based Medical Imaging Systems Real or artefactual differences? Different scanners Different populations Different raters Different centres Different protocols The concept of the collaboratory is central to the e-Science vision, yet there has been limited concern with the generation of the community and coordination infrastructures which will coordinate and sustain it. Designing for e-Health: Recurring Scenarios in Developing Grid-based Medical Imaging Systems John Geddes a, Clare Mackay a, Sharon Lloyd b, Andrew Simpson b, David Powerb, Douglas Russell b, Marina Jirotka b, Mila Katzarova b, Martin Rossor c, Nick Fox c, Jonathon Fletcher c, Derek Hilld, Kate McLeish d, Yu Chen d, Joseph V Hajnal e, Stephen Lawrie f, Dominic Job f, Andrew McIntosh f, Joanna Wardlaw g, Peter Sandercock g, Jeb Palmer g, Dave Perry g, Rob Procter h, Jenny Ure h,[1], Mark Hartswood h, Roger Slack h, Alex Voss h, Kate Ho h, Philip Bath i, Wim Clarke i, Graham Watson i[1] a Department of Psychiatry, University of Oxford, b Computing Laboratory, University of Oxford, c Institute of Neurology, University College London, d Centre for Medical Image Computing (MedIC), University College London, e Imaging Sciences Department, Imperial College London, f Department of Psychiatry, University of Edinburgh, g Department of Clinical NeuroSciences, University of Edinburgh, h School of Informatics, University of Edinburgh, i Institute of Neuroscience, University of Nottingham [1][1] Corresponding Author: Jenny Ure, School of Informatics, University of Edinburgh, Jenny.Ure@ed.ac.uk
, the UK e-Science programme and the NeuroGrid Consortium. Data Quality Issues: The Social Life of Information Challenge: The large scale aggregation of diverse datasets offers both potential benefits and risks, particularly if the outputs are to be used with patients in a clinical context. Thus aggregating data is a key issue for e-Health, yet data is not independent of the context in which it is generated. Within small communities of practice a degree of shared and updated knowledge and experience allows judicious use of resources whose provenance is known and whose weaknesses are often already transparent. The same is not true of aggregated data from multiple sources. Approach: Early use of prototypes to provide a ‘sandpit’ for promoting both technical and inter- community dialogue and engagement, and start the process of identifying, sharing and updating knowledge of emerging issues. Early trials with known datasets aim to generate an awareness of the types of variance that can arise and ways in which it might be minimized, harmonized, or made transparent to users Socio-technical Issues Aligning Technical and Human Systems Conclusions In organic communities, the processes of structuring collaboration, coordination and control structures happens as a matter of course. NeuroGrid is employing an early prototype to generate engagement and dialogue, to enable early discussion of requirements for more complex services, compute capability and workflows, as well as data quality and configurational issues. In addition to ameliorating the recurring issue of requirements ‘creep’, late in the design process, it allows disparate groups to engage with the real issues, and possible solutions in a shared context. For further information For information on this and related projects contact or go to Challenge: Integrating the technical work of system building, with the socio-political work of generating the governance of the new risks and opportunities they generate Approach: The creation of real and virtual ‘shared spaces’ (e.g. via Access Grid) and the use of an early prototype for engagement in areas of shared professional concern, to help this new hybrid community develop its own rules of engagement, and start making collective sense of local requirements in relation to common project goals. Semantic Issues Il nome della rosa Challenge: Multi-site studies raise issues such as different naming conventions for files, different coding and classification systems, different protocols, and different conceptualisations of domains. Approach: The project agreed on core and node specific metadata and will use an OWL-based ontology (logic-based domain map) to allow human and machine-readable searching and basic reasoning across the datasets. In this there is a trade-off between the benefits of share-ability and automated reasoning, on the one hand, and the formalisation of concepts and relationships that are evolving. Challenge: Aligning and representing datasets at different levels of granularity. While NeuroGrid uses MR and CT scans, other relevant datasets such as diffusion tensor imaging, genetic, proteomic datasets also contribute to an understanding of neurological processes. Approach: The project is adopting a two –pronged approach developing task specific ontologies developing a reference ontology based on the Foundational Model of Anatomy adopted by the BIRN Human Brain Project. This allows a degree of alignment between datasets and ontologies in future collaborations Designing for e-Health: Recurring Scenarios in Developing Grid-based Medical Imaging Systems Real or artefactual differences. Different scanners Different populations Different raters Different centres Different protocols The concept of the collaboratory is central to the e-Science vision, yet there has been limited concern with the generation of the community and coordination infrastructures which will coordinate and sustain it. Designing for e-Health: Recurring Scenarios in Developing Grid-based Medical Imaging Systems John Geddes a, Clare Mackay a, Sharon Lloyd b, Andrew Simpson b, David Powerb, Douglas Russell b, Marina Jirotka b, Mila Katzarova b, Martin Rossor c, Nick Fox c, Jonathon Fletcher c, Derek Hilld, Kate McLeish d, Yu Chen d, Joseph V Hajnal e, Stephen Lawrie f, Dominic Job f, Andrew McIntosh f, Joanna Wardlaw g, Peter Sandercock g, Jeb Palmer g, Dave Perry g, Rob Procter h, Jenny Ure h,[1], Mark Hartswood h, Roger Slack h, Alex Voss h, Kate Ho h, Philip Bath i, Wim Clarke i, Graham Watson i[1] a Department of Psychiatry, University of Oxford, b Computing Laboratory, University of Oxford, c Institute of Neurology, University College London, d Centre for Medical Image Computing (MedIC), University College London, e Imaging Sciences Department, Imperial College London, f Department of Psychiatry, University of Edinburgh, g Department of Clinical NeuroSciences, University of Edinburgh, h School of Informatics, University of Edinburgh, i Institute of Neuroscience, University of Nottingham [1][1] Corresponding Author: Jenny Ure, School of Informatics, University of Edinburgh,")
30
2. Data Interpretation and Coding Example 2. Telehealth/Mobile Health

32
An accessible ‘living lab.’ for research on socio-technical systems The shaping of data passing through many hands The shaping and re-shaping of diagnosis as new data challenges current classifications, practices and policies The impact of local shaping (personal, contextual and technological) on the global vision for eHealth the impact of technology mediated access to data on the roles, risks and resources available to different actors The implications for representation of different actors in the process The implications of both access to data and access to representation in the design process can shape the care constituency.
 on the global vision for eHealth the impact of technology mediated access to data on the roles, risks and resources available to different actors The implications for representation of different actors in the process The implications of both access to data and access to representation in the design process can shape the care constituency.")
34
Qualitative Approaches

35
Evaluating tele-monitoring of COPD patients at home

36
Context telecare-monitoring centre

37
Grounded Theory Collaborative Action research Realistic Evaluation Ethnographic Observation

38
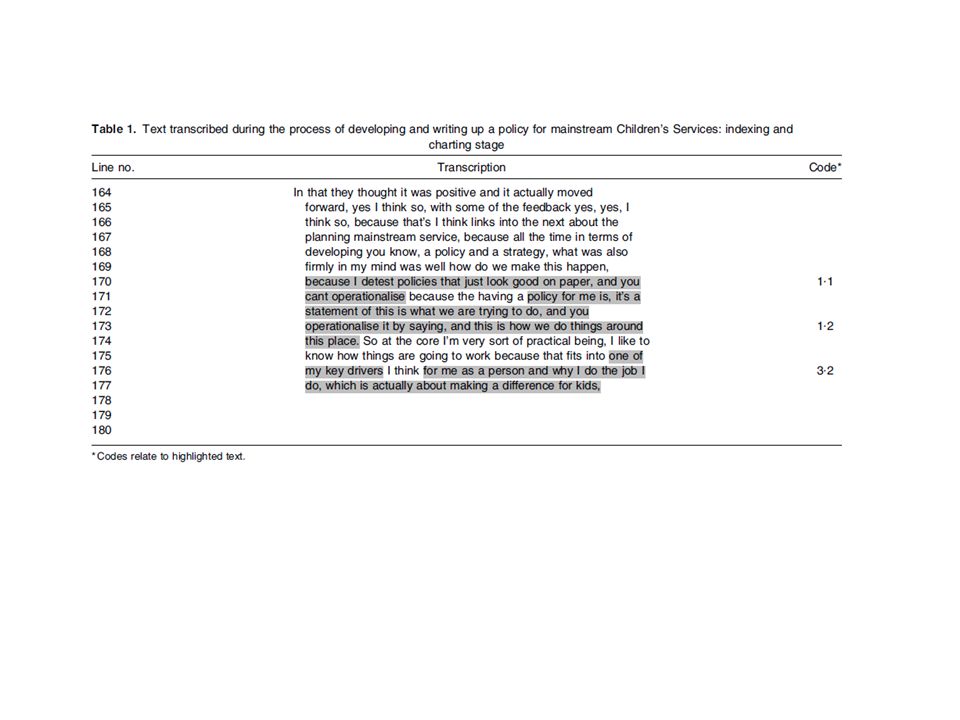
Grounded theory ‘The discovery of theory from data – systematically obtained and analysed in social research’ (Glaser & Strauss, 1967: 1) ‘The methodological thrust of grounded theory is toward the development of theory, without any particular commitment to specific kinds of data, lines of research, or theoretical interests... A style of doing qualitative analysis that includes a number of distinct features... and the use of a coding paradigm to ensure conceptual development and density’ (Strauss, 1987) Grounded theory38
 Grounded theory38.")
39
Two Variants Two main variants: 1.Strauss and Corbin’s (1990) book provides one coding paradigm (context, conditions, interactions, conditions and consequences) 2.Glaser’s (1978) book provides 18 coding ‘families’ giving many more options Glaser accused Strauss and Corbin of being too restrictive and of forcing data and concepts into a preconceived mould However the Strauss and Corbin (1990) variant is the most widely used Grounded theory39
 book provides one coding paradigm (context, conditions, interactions, conditions and consequences) 2.Glaser’s (1978) book provides 18 coding ‘families’ giving many more options Glaser accused Strauss and Corbin of being too restrictive and of forcing data and concepts into a preconceived mould However the Strauss and Corbin (1990) variant is the most widely used Grounded theory39")
44
www.telescot.orgwww.telescot.org http:// telehealthpilot.wikispaces.comhttp:// telehealthpilot.wikispaces.com

45
A vision mediated by ´standard´ thresholds and protocols

46
Overview of the Lothian COPD Pilot Jenny Ure Edinburgh University www.telescot.org

47
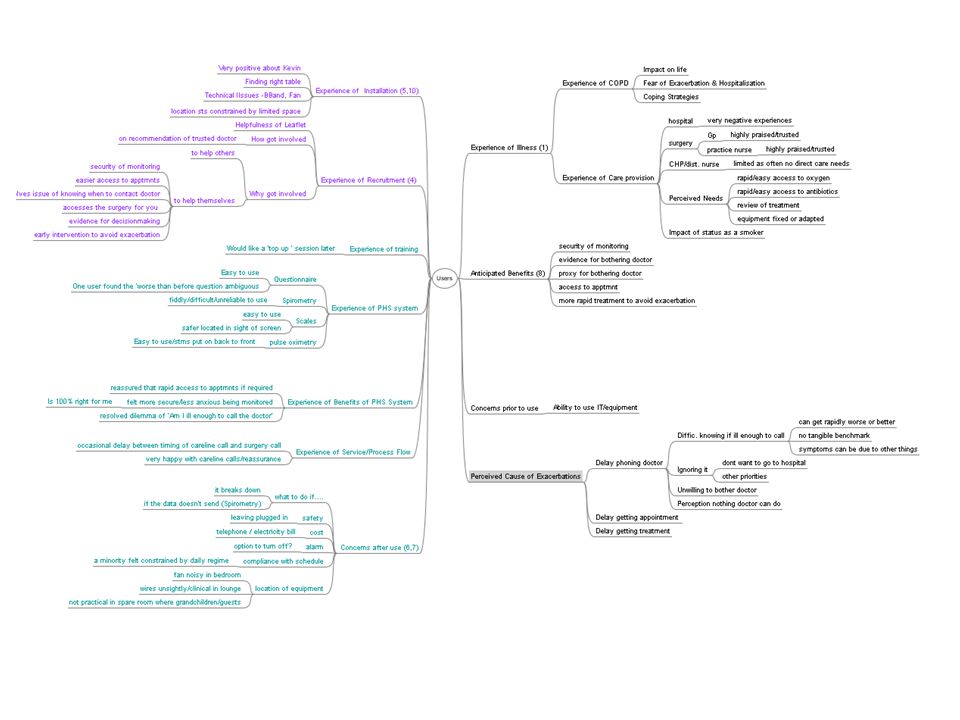
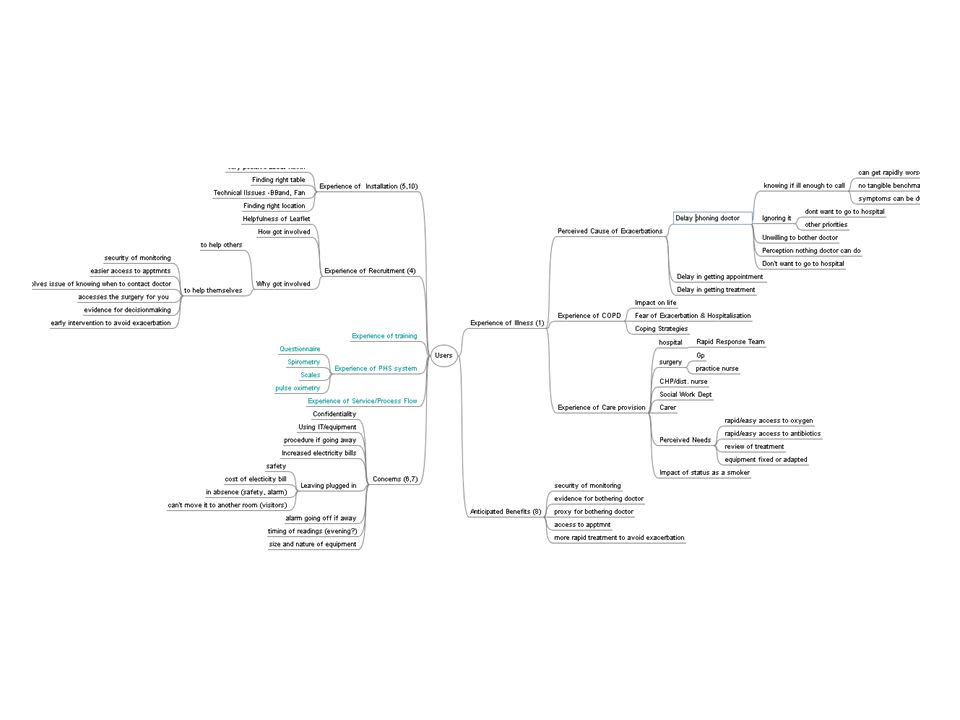
The home-monitoring vision The early vision of early detection to cut hospital admissions/costs The evolving scenarios as new opportunities and challenges arise The process of rethinking and reconfiguring roles, risks, resources and criteria for value

48
Hospital admissions Should I bother the GP?

49
Collaborative research and development with patients, GPs and nurses

50
Early vision was protocol driven

51
And team-based

52
Different Perspectives on This

53
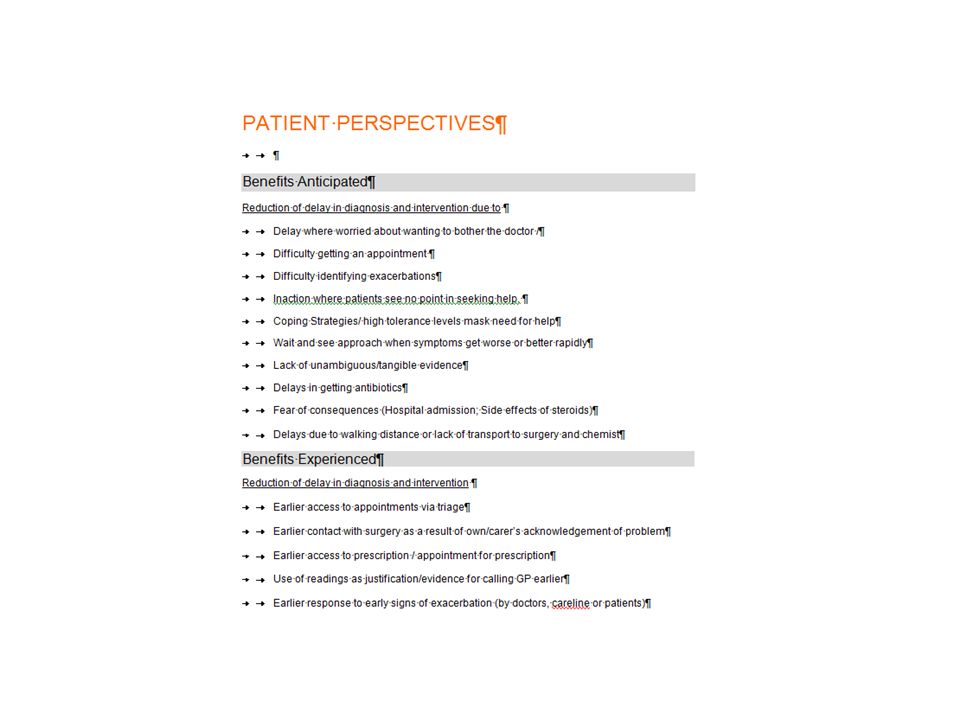
Patient Expectations Reduction in delays reporting an exacerbation or getting treatment

54
Not wishing to bother the GP I mean I was like days into an attack and it was only when I was really desperate that I thought maybe I should call out the doctor. I don’t like calling the doctor cos they’re very busy people I don’t know if I’m bad enough to go and see the doctor

55
Not being sure I think it’s the thought in case you’re..you know… mistaken, you know? And it doesn’t come to anything. I said ‘Well I’m really quite breathless but I don’t know if I’m bad enough to go and see the doctor’. Because if I have to clean my windows I can be breathless, but it doesnae mean.....

56
Not getting an appointment You cannae get a doctor so therefore it’s no my fault that (get breathless) and I get angry. And I can’t get a doctor. And it could have been prevented from getting to the stage that it is. To let you understand, just say I got up this morning and was awful bad, say I had a right bad lung infection, or whatever, and I phoned the surgery right now – no chance of an appointment the day. That’s the truth. I’d be lucky, maybe, to get one next week. I’d be very lucky.

57
See no point contacting GP I feel that quite often he leaves it a long time ……And I understand that because he says ‘ what else can they give me?’ He feels that he’s done everything, so what’s the point in going down?’ (Wife of patient, 72, pre-installation)
")
58
Avoidance / Denial I knew if I went to the surgery I would be in hospital. So I said ‘No.’. Ken what I mean?.’ I’ll just fight.’ But I was really bad. (Male patient,76, post-installation)
.")
59
Avoid difficulty of getting to surgery/chemist when ill Because it’s quite a wee bit of work getting to the doctor’s - it’s about 15 minutes walk - if we want to go to the doctor we’ve got to take two buses...You’ve got to wait, and then you come off, and then you’ve got the rest of the way to walk. It’s no problem walking if you’re OK, but if I’m having an attack there’s no way. ( Female Patient, 66,)
.")
60
Evidence to justify seeking help You’d think you would find it easy to tell when you’re ill but it’s only afterwards that you know you are not well. But this technology is really brilliant. The difference between no feeling well and being ill - she (practice nurse) said ‘It’s when you start no feeling well... no when you’re ill that you should come down.’ But I need to get the knowledge to separate the two. There’s a big difference - ken what I mean? Feeling unwell and being ill - it’s two different things.
 said ‘It’s when you start no feeling well... no when you’re ill that you should come down.’ But I need to get the knowledge to separate the two. There’s a big difference - ken what I mean. Feeling unwell and being ill - it’s two different things..")
61
Patient: perspectives Problem accessing an appointment Problem identifying an exacerbation from a bad day Fear of bothering doctors unnecessarily Getting to the surgery Getting antibiotics

62
Main Benefit Perceived? Best thing?.On the average I would think that the machine…it would get attention a lot quicker than you would normally. I’m just going on what you hear…where you wait 3 days for an appointment. Some people even said they had a week to wait. And I said – ‘Is that for a specific doctor? ‘ No, no, for a doctor. From that point of view, the machine’s a great asset. It would throw up to somebody right away that you need attention. You’re no getting blocked off by a receptionist.

63
Benefits Experienced

64
Reassurance You know if something was wrong I’d get a phone call from the surgery –saying-you know - tra la la - whatever it was. The way I look at it, if there was something wrong they’d write a prescription, and I’d get it sent to the chemist-..and then I’d get it delivered direct.because if I’m unwell that’s one thing I have to face is that long walk to X, because there’s no bus direct from here an you know, when I’m unwell, um, so I’m delighted with it, yeah. (Female patient, 66, post-installation)
.")
65
It’s actually quite comforting to know that they can see that every day, because before that I was getting rushed into hospital. Now with that they’re seeing it - they’re monitoring it. (Male patient/smoker 59, post-installation) Actually it made me more assured. In a way it was a relief thinking that I should ignore my own thoughts on getting a doctor or something like that. This organisation was going to get hold of a doctor if their readings showed I needed a doctor. They were going to get hold of a doctor and get one here. (Female patient, 47 with asthma and COPD)
 Actually it made me more assured. In a way it was a relief thinking that I should ignore my own thoughts on getting a doctor or something like that. This organisation was going to get hold of a doctor if their readings showed I needed a doctor. They were going to get hold of a doctor and get one here. (Female patient, 47 with asthma and COPD).")
66
Less anxiety / panic C: Since he’s been on that machine he’s never had anything like that. I: You’ve not had any attacks since you’ve had that machine? C: Oh no. Because you’re seen to right away now I: So you think you’ve been catching things earlier then P: Oh Aye C: He’d have been carted away in an ambulance because he hyperventilates at the start. Just before the machine went in. He panics. P: Ah panic… I was bad, and they took me into hospital on oxygen (Carer and patient with severe COPD, post-installation)
.")
67
Reassurance and information for carers And the readings are helpful for me, and I can physically see if her oxygen saturation is OK...and stuff like that so that’s reassuring for me. So I must say I like it... I think its a good thing for a carer to have. (Carer, female patient, 87)
.")
68
Faster access to GP Oh you were waiting weeks, and he was suffering all that time. And (now) any time the machine takes his reading and it’s not up to scratch, they’re on the phone right away. He’s (husband) fair pleased because he says at least it takes, you ken, the worry. Whenever you’re no well you can get them right away. Get on antibiotics and that. Cos he will say ‘you always leave it a wee bit too late. You wait till you’re gone and bad, you ken’. You must admit there was a big improvement, because it saves you begging for an appointment and things like that. Carer for 69 year old male patient
 any time the machine takes his reading and it’s not up to scratch, they’re on the phone right away. He’s (husband) fair pleased because he says at least it takes, you ken, the worry. Whenever you’re no well you can get them right away. Get on antibiotics and that. Cos he will say ‘you always leave it a wee bit too late. You wait till you’re gone and bad, you ken’. You must admit there was a big improvement, because it saves you begging for an appointment and things like that. Carer for 69 year old male patient.")
69
P: So I don’t need to have an appointment C: He just goes on to it straight away. They write a prescription and it goes straight to the chemist I: Did he have that before? C: No he didnae used to have that before.~ I: Do you see that as an advantage? C: Oh yeah, because normally..to get an appointment down here..it’s murder

70
Earlier intervention Yes, a couple of times the doctors have caught it before it goes into an exacerbation...There’s a couple of times we’ve caught it before it got bad (Carer for female patient, 87, post- installation

71
Prompts patients to act I know myself if that wasn’t there I’d just keep puffin about. (Male patient 77 Well before I might have left it off for a week or two because I don’t like taking them (steroids).I don’t like the side effects. But I know when I have to take them now. (Female patient with / COPD and asthma, 47)
.I don’t like the side effects. But I know when I have to take them now. (Female patient with / COPD and asthma, 47).")
72
Reinforce lifestyle changes When I stopped smoking I could see the difference in the scores. I’ve noticed, even my peak flow. My peak flow will never be really high. There it was 105. Well, it’s usually about 80 or 90, ken? But since I’ve stopped smoking, I’m putting the weight on. I notice it on that scale.

73
Very positive perceptions Oh no – it’s a great help. There’s no two ways about it – it’s a good thing. Well I think its a good thing anyway, and the two boys that were there fae Intel – they asked that- and I said “I thought you were come to take it away!” And I said – ‘You’re no goin to take it away! You’ll need to get the FBI!’ (Male Patient)
.")
75
Emerging Opportunities In combination with pulmonary rehab. That would sell it. A combination, combined approach would be brilliant. I think if that was – if people who had COPD were offered this for monitoring their progress – just the fact that they are mentoring their progress every day GP

76
Usability

77
Installation

78
Care Team Perspectives

79
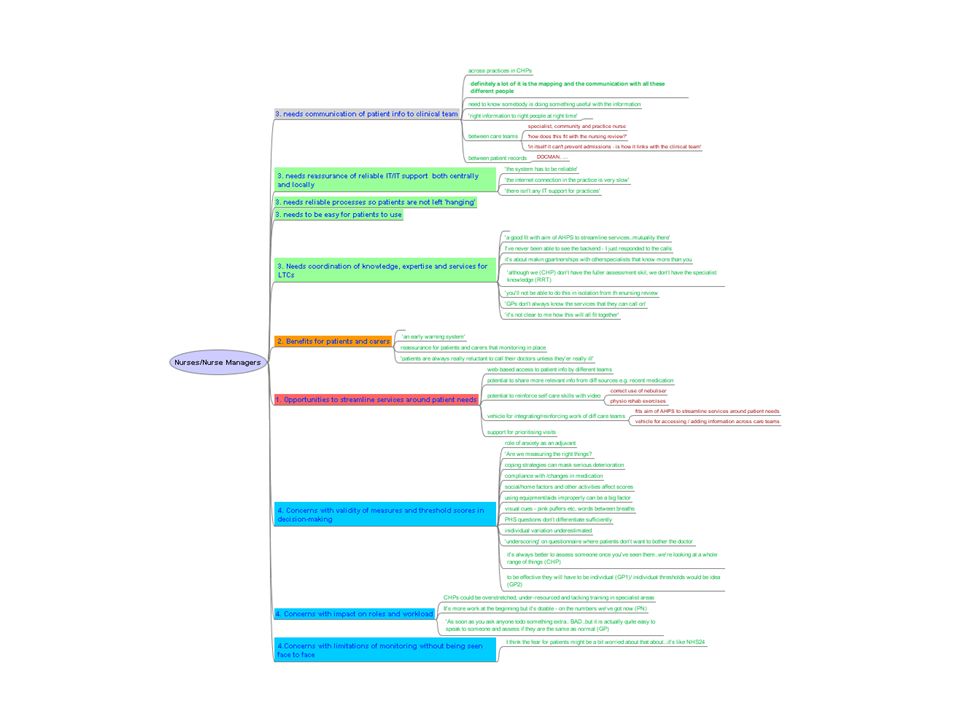
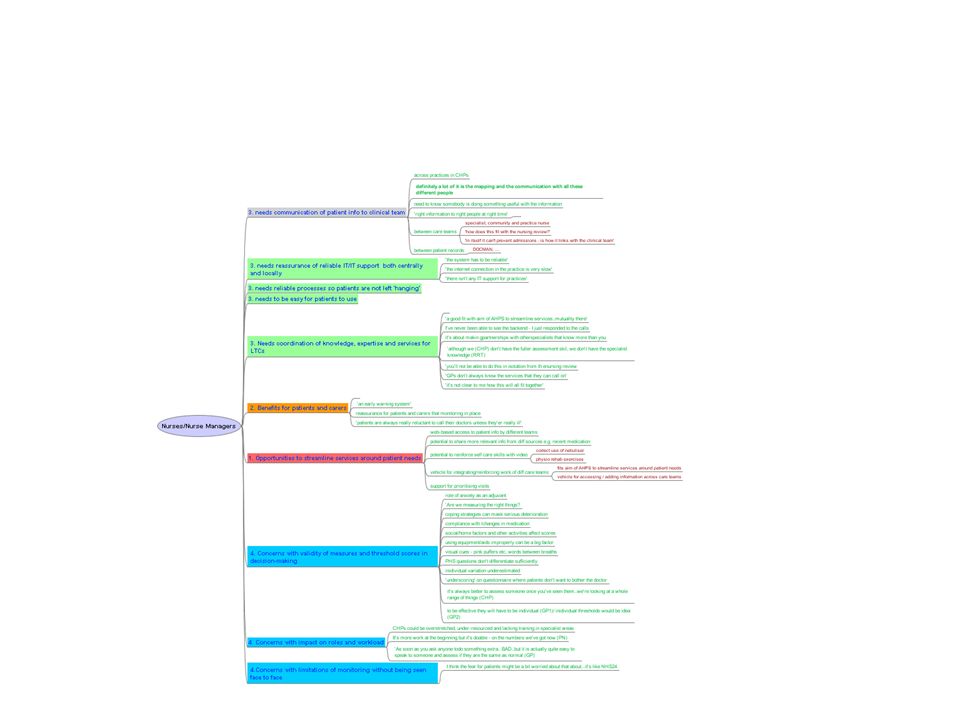
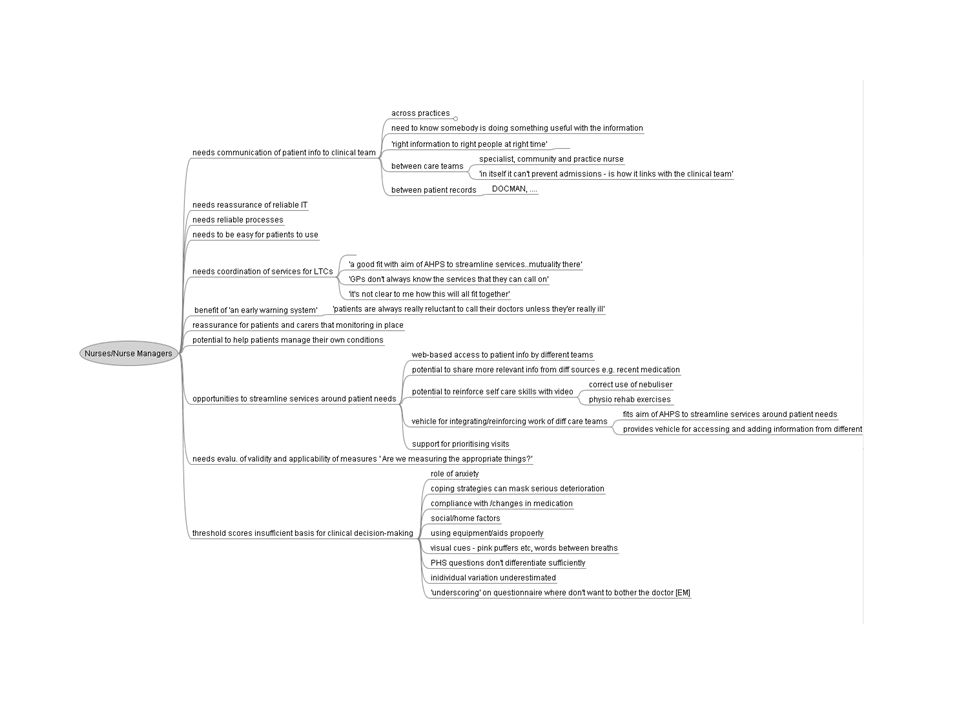
Nurses, Physiotherapists Core problem focus is the realisation of the intervention after monitoring Core problem issues (and opportunities) are – coordination of information and services of distributed care teams around patients needs – opportunity from virtual hub as vehicle for this here – limitations of standard threshold scores as a guide to care needs – Opportunity of video-conferencing facility to address this problem, and to extend reach of care services
 are – coordination of information and services of distributed care teams around patients needs – opportunity from virtual hub as vehicle for this here – limitations of standard threshold scores as a guide to care needs – Opportunity of video-conferencing facility to address this problem, and to extend reach of care services")
80
Risks raised by nurses I think the main thing is that when these people are picked up by the care team or the primary care team, that nurses know what to do with them - that they’re trained and they’re competent. That’s an area that we’re trying to develop. It is about being absolutely clear what these people need in the way of support, and of what exactly will help. For some of these people who…(pauses briefly)...the only thing that will help some people is more perfusion – getting their body on oxygen. Manager of distributed care services for patients at home
...the only thing that will help some people is more perfusion – getting their body on oxygen. Manager of distributed care services for patients at home.")
83
The early vision The barrier is patients’ unwillingness to bother the doctor in critical early phase The solution is telemetric monitoring triggering call to doctor for threshold readings and early intervention

84
…there are known unknowns; that is to say we know there are some things we do not know. But there are also unknown unknowns -- the ones we don't know we don't know.

85
Data shaped by technical and social issues challenges the initial vision of monitoring Battery failure /poor transmission “You don’t want to be hippy and ‘over-score’ “ I know if I score high I’ll be carted off in an ambulance so….(laughs).” “You really need a sort of second layer (VC) to make sense of the scores, and decide if they need a visit. M’s scores are OK but I know.. because I spoke to her that she’s really bad. Others score high and they’re fine.

86
Scenario 1: A largely technical process Telemetric monitoring using standard symptom scores to trigger early intervention/reduce costly admissions Critical assumptions about the relationship between standard scores and the processes of diagnosis and intervention

87
Problem: ‘Standard’ scores not reliable index of how ill patients are in practice Local factors such as activity, anxiety, environment, affect breathlessness for example GPs and nurses need to get/use patient/context specific information to make sense of scores

88
Scenario 2: A two stage socio-technical process Stage 1 : Tele-monitoring to highlight potential risks Stage 2: GP/nurse uses video- conferencing facility to see patient in home environment to interpret the threshold scores in context, and negotiate an appropriate intervention with them

89
Problem: responding to much higher levels of at risk patients than expected Workload implications for GPs if scaled Clinical and legal risks/ implications where delays occur between patient, call centre, surgery Clinical issues as patients get antibiotics twice as often as a result of monitoring

90
Scenario 3: A socio-political process? Tele-monitoring to highlight potential risks but patient has responsibility for contacting surgery GP/nurse and patient video- conferencing session to interpret scores in context, and agree satisfactory diagnosis / intervention but rapid response nurse team have responsibility for responding quickly and appropriately

91
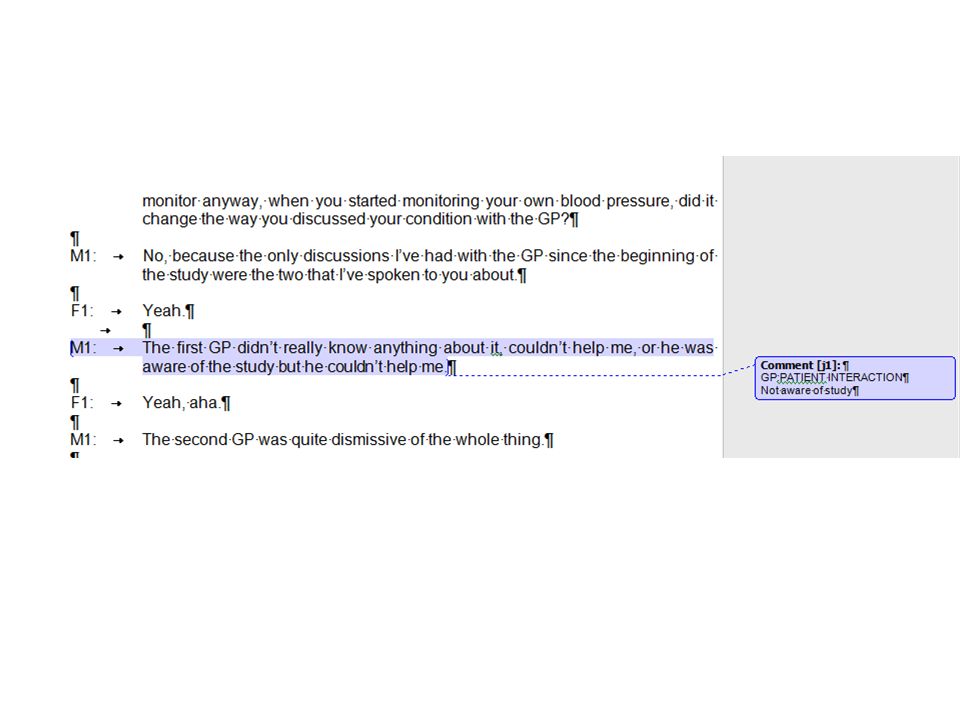
Critique of grounded theory Advantages: – It has intuitive appeal for novice researchers, since it allows them to become immersed in the data at a detailed level – It gets researchers analysing the data early – It encourages systematic, detailed analysis of the data and provides a method for doing so – It gives researchers ample evidence to back up their claims – It encourages a constant interplay between data collection and analysis – It is especially useful for describing repeated processes e.g. the communications processes between doctors and patients, or the communications processes between information systems analysts and users Grounded theory91

92
HITS Hypertension Monitoring Study

93
Does monitoring change things? How does the process work on the ground? Changes in roles, risks, costs and benefits? Benefits and problems ? Barriers and enablers? Differences between practices/patients? We need more feedback from nurses!

94
Different perceptions Yes – well I was a bit alarmed when I got a phone call saying you know to come in. One thing that really was of good benefit was – I got a phone call from that lady there (nurse) that’s just been in saying em ‘We’ve been monitoring your BP and it’s a bit high - so we want you to come in’ - and that’s when they changed by medication
 that’s just been in saying em ‘We’ve been monitoring your BP and it’s a bit high - so we want you to come in’ - and that’s when they changed by medication.")
95
Personal Use: Using it as a prompt So I like having the machine there cos it prompts me, and it you know.... If it creeps up again I think ‘I’d better do something about this.’ It’s useful for the fact that it just there. I’ll just take a reading an see how I’m getting on. Yeah. It’s great. For me it’s a prompt for me to do something to get the blood pressure down. I or..eh..it’s there. I leave it on a shelf in the office where I work.It’s there as a constant reminder. It’s just a prompt. To be proactive rather than reactive.

96
Different Uses : Using it as evidence On occasions you know I’ve been into the doctor, and the readings have just been on a plateau, they didn’t seem to be going down and I took these in and I said ‘Look…these are my readings, and I’m concerned. Well I mean I was on two tablets, and I’m on three now so um it’s certainly helped communication. It’s given me more meaningful data to speak to the doctor rather than – ‘ I think the blood pressure’s gone up’.

97
I’ve done things like done some exercise and then taken my blood pressure to see if it makes a difference and it did…it does...s every time. If it creeps up again I think ‘I’d better do something about this.’ Or as evidence

98
Early findings highlight differences In use between patients and practices Some patients used it as a prompt to help them diet, exercise etc to reinforce effective approaches to better understand their own BP changes, and link these to their lifestyle as evidence to support more constructive discussions with nurse/GP

99
Early Findings: Nurses But the positive thing is it definitely gets patients more involved in their care In terms of compliance with their medication I think they are much more likely to comply, and they can see the effect I think it does give them more control There would be a workload thing about it, and that’s really the main thing, to find the time to...

100
Early Findings: Nurses I’ve had not one phone call from any of them, rather than seeing them every two weeks as we would normally do. So I don’t know. Did they understand their role in this?They seemed to tail off as well with their enthusiasm. I didn’t see a benefit to this..with this particular group of patients Time consuming going into the web-page and getting the average, and writing it into the patient records

101
Well I did the screening but was in the group that didn’t get a monitor, so I bought one on Amazon and I’ve been using that The unexpected!

102
Critique of grounded theory (2) Disadvantages: – First time users can get overwhelmed at the coding level – Open coding takes a long time – It can be difficult to ‘scale up’ to larger concepts or themes – Because it is a detailed method, it can be difficult to see the bigger picture – Tends to produce lower level theories only Grounded theory102
 Disadvantages: – First time users can get overwhelmed at the coding level – Open coding takes a long time – It can be difficult to ‘scale up’ to larger concepts or themes – Because it is a detailed method, it can be difficult to see the bigger picture – Tends to produce lower level theories only Grounded theory102")
103
Evaluating grounded theory studies Is there a clear chain of evidence linking the findings to the data? Are there multiple instances in the data which support the concepts produced? Has the researcher demonstrated that they are very familiar with the subject area or, as Glaser puts it, are steeped in the field of investigation (Glaser, 1978)? Has the researcher created inferential and/or predictive statements about the phenomena? Has the researcher suggested theoretical generalizations that are applicable to a range of situations? 103Grounded theory
. Has the researcher created inferential and/or predictive statements about the phenomena. Has the researcher suggested theoretical generalizations that are applicable to a range of situations. 103Grounded theory.")
104
Communicating

107
Extending... The reach of research at low cost The role of users as researchers and developers of health and other services PIMS using mobile services

110
Telescot www.telescot.org COPD http://www.telescot.org/uploads/4/5/9/4/4594120/telescot-copd-pilot-report.pdf mHealth http://telemed.wikispaces.com/ www.telescot.org http://www.telescot.org/uploads/4/5/9/4/4594120/telescot-copd-pilot-report.pdf http://telemed.wikispaces.com/ Jenny Ure Jenny.Ure@ed.ac.uk

111
Combining Qual. And Quant. Interviews followed by questionnaires Framework approach Research design: The Framework (Pope, Ziebland, and Mays, 2000) and explanatory account approaches (Stern & Kirmayer, 2004) is used to analyze the qualitative data and develop quantitative variables from qualitative data. Correlation analysis of qualitative variables with external constructs reveals consistent convergent/divergent pattern of associations— suggesting specific underlying structural constructs.
 and explanatory account approaches (Stern & Kirmayer, 2004) is used to analyze the qualitative data and develop quantitative variables from qualitative data. Correlation analysis of qualitative variables with external constructs reveals consistent convergent/divergent pattern of associations— suggesting specific underlying structural constructs..")
112
Academic Writing Skills Does it answer the question? Does it follow the required format? Does it provide evidence for the arguments? Do paragraphs have a keypoint sentence on which you enlarge? Does the Introduction say What, Why and How you are proceeding? Do you provide signposts?

113
so technical infrastructure needs community infrastructure to define.. frames of reference naming conventions ethical and legal conventions agreements on management of costs and risks and benefits

114
The eHealth Vision of seamless data sharing? Still more of a vision than a reality !

Similar presentations



 Gill Johnston, University of Sussex.>")
















 De Anza College 14 April 2011.>")

