Download presentation
Presentation is loading. Please wait.

1
TUMOURS OF NASAL CAVITY & PARANASAL SINUSES
Col Shoaib Ahmed Consultant ENT Head & Neck Surgeon MBBS (Honours) FCPS(Pakistan) FRCS(Glasgow)
 FCPS(Pakistan) FRCS(Glasgow)")
2
Review of Anatomy Paranasal sinuses are air filled cavities that communicate with the nasal cavity There are close anatomical relations with orbit & skull base Cranial nerves 1st, 2nd, 3rd ,4th , 5th and 6th are in close vicinity

3
Unique Features of Sinonasal Tumours
Relatively rare of head & neck tumours Present late Large air filled sinuses with no vital structure in immediate vicinity → remain clinically silent Highly non specific early symptoms – (rhinorrhea & nasal obstruction) → receive scant attention Wide variety of pathological lesions Extension to anatomically critical areas Generally advanced disease with poor clinical outcome
 → receive scant attention. Wide variety of pathological lesions. Extension to anatomically critical areas. Generally advanced disease with poor clinical outcome.")
4
Classification BENIGN Inverted papilloma Non epithelial Fibroma
Chondroma Hemangioma Nerve sheath tumour

5
Classification contd. MALIGNANT Squamous cell carcinoma Non epithelial
Adenocarcinoma Adenoid cystic carcinoma Mucoepidermoid carcinoma Olfactory neuroblastoma / Esthesioneuroblastoma Non epithelial Sarcomas Lymphoma Giant cell tumour

6
Environmental Factors associated with sinonasal malignancy
Wood dust Nickel Hydrocarbons Chromium Organic oils Isopropyl oil

7
Clinical Features EARLY Nasal obstruction Rhinorrhea LATE Epistaxis
Proptosis Facial pain / swelling Cranial nerve dysfunction Trismus

8
How to identify early on ?
Can be readily mimicked by common respiratory conditions (e.g. Sinusitis ) ↓ Unilaterality of symptoms & signs Persistent & progressive symptoms No improvement with antibiotics / anti histamines Unilateral facial pain / numbness / fullness Short span of symptoms suggests a malignant tumour
 ↓ Unilaterality of symptoms & signs. Persistent & progressive symptoms. No improvement with antibiotics / anti histamines. Unilateral facial pain / numbness / fullness. Short span of symptoms suggests a malignant tumour.")
9
Clinical Examination Thorough ENT head & neck examination ↓ Trismus
Orbit Neurological exam (cranial nerves 1st to 6th) Cervical lymph nodes
 Cervical lymph nodes.")
10
Diagnosis Always done after imaging Clinical
Imaging (X rays, CT , MRI , PET ) Biopsy Always done after imaging (highly vascular lesion, or intra cranial) Generally under LA
 Biopsy. Always done after imaging. (highly vascular lesion, or intra cranial) Generally under LA.")
11
Radiological Imaging Plain X rays have lesser value !
45 degrees Occipitomental projection – “X ray PNS”

12
Plain X- rays - Findings
Unilateral findings Opaque sinus Gross bone destruction

13
CT scans Initial investigation of choice Shows bony details
Areas of bone destruction Extension into adjacent areas

14
Normal CT scan Frontal sinus Ethmoid sinuses

15
CT scan Unilateral sinonasal mass
Bony erosion of lateral nasal wall and skull base

16
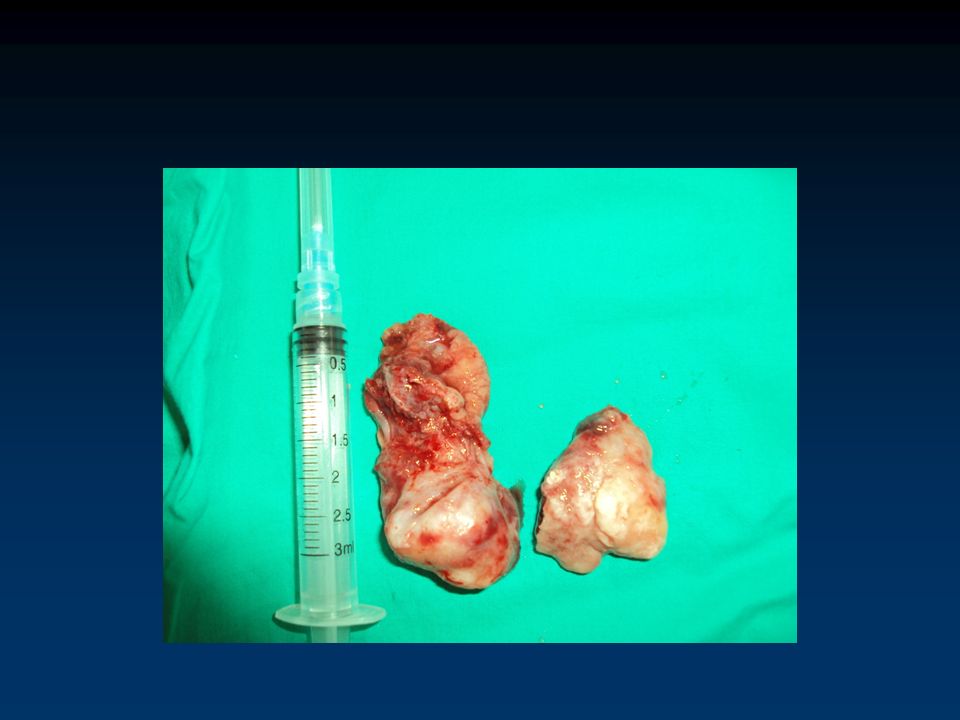
Inverted papilloma

17
Olfactory neuroblastoma in a 14 year old

18
MRI Better soft tissue detail Useful to detect intracranial extension
Able to distinguish nasal secretions from tumour Indicates extension into dural venous sinuses

19
Positron Emission Tomography (PET scan)
Routine evaluation for recurrent disease after primary tumour Mainly used for squamous cell carcinoma Very expensive modality

20
TREATMENT OPTIONS Palliation Surgery Radiotherapy
Combined surgery & radiotherapy Chemotherapy Palliation Lymphomas

21
Olfactory Neuroblastoma in a young lady

29
CONCLUSION These are rare tumours with poor survival & are generally advanced at presentation Comprise of several histologic types with varying biological behaviour Early diagnosis requires being alert for any persistent unilateral symptoms Diagnosis is based on CT, MRI and biopsy For cure, extensive mutilating surgery followed by reconstruction is often required

30
DEPARTMENT OF ENT HEAD & NECK SURGERY COMBINED MILITARY HOSPITAL RAWALPINDI

31
Any Questions ?

Similar presentations


















Primary Tumours: Benign Glomus tumour Malignant Carcinoma,sarcoma 2)Secondary Tumours: a) From adjacent areas like.>")






