Download presentation
Presentation is loading. Please wait.

1
MOVING FROM “WHAT’S THE MATTER WITH YOU” MEDICINE TO “WHAT MATTERS TO YOU”: A PARADIGM SHIFT IN PHILOSOPHY OF CARE.

2
BEING A GOOD PSYCHIATRIST – What I Was Taught As clinicians we are the ones responsible for whether people “get better” or not Relieving people of their voices, unusual beliefs, anxiety, and depression is the core of good clinical care and Good clinical care is the core of what it takes to foster recovery from severe mental illness

3
The Patient Over Outcome The “Zone of Delusion”

4
FROM DEFINED ROLES FOR DOCTOR AND PATIENT Power imbalance Clinician responsibility “What’s the matter with you” Compliance Constraint

5
TO A FOCUS ON BUILDING TRUST AND PARTNERSHIP Partnership Shared responsibility Health Behaviour “What matters to you” Liberation

7
12-18% of those with Long-Term Conditions (LTCs) are likely to have severe Mental Health & Addiction (MH&A) conditions which significantly contributes to poor health outcomes and increased service utilisation. On the other hand, people with severe MH&A conditions will die on average 15-20 years younger, mostly as a result of poorly managed LTCs – CVD, Diabetes, Cancer etc. The presence of a comorbid MH&A condition in people with LTCs increases risk of admission by up to 3x, increases LOS up to 2x, and increases use of Outpatient Services by up to 2x. The presence of unmet psychosocial and cultural needs further adds to poor outcomes and increased service utilization. Background

8
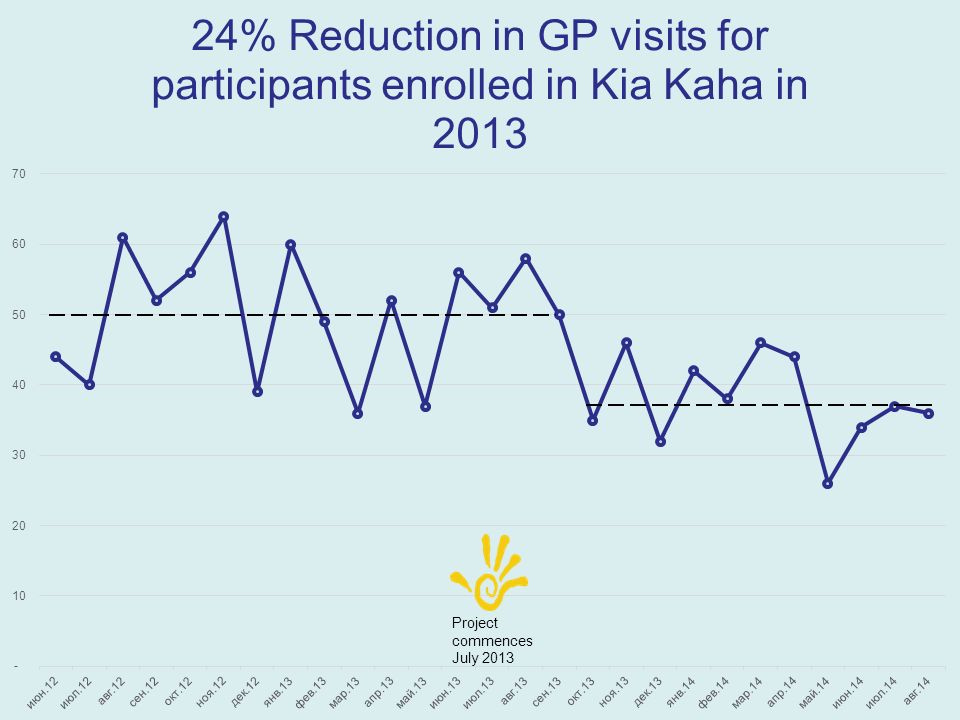
Research has clearly demonstrated that identifying and meeting this MH&A need, and any associated psychosocial or cultural need, results in much improved outcomes and significantly reduced health service (secondary/tertiary) utilization. Background (contd) Aims To achieve a 25% reduction in overall hospital and GP utilisation for 125-150 individuals with LTCs, and co-existing severe MH&A issues engaged by 1 July 2014. This will be achieved by identifying and meeting mental health, addiction, and psychosocial needs; and building self- management skills of these individuals and their whanau. We intend to do this by expanding our current Primary Mental Health service and introducing evidence-based interventions in an innovative way
 Aims To achieve a 25% reduction in overall hospital and GP utilisation for individuals with LTCs, and co-existing severe MH&A issues engaged by 1 July This will be achieved by identifying and meeting mental health, addiction, and psychosocial needs; and building self- management skills of these individuals and their whanau. We intend to do this by expanding our current Primary Mental Health service and introducing evidence-based interventions in an innovative way.")
10
Not all of the high users seen identified themselves as having a “mental health issue” What we identifed was high psychological distress and psychosocial complexity Many were current CMHC pts but not well engaged, no focus on physical healthcare needs Engagement was the biggest challenge (>50% fail rate) We trialed the use of peer support workers to engage with the most hard to reach patients Along the way, we recognised more and more the value of peer support as an “intervention” in itself Initial Findings
 We trialed the use of peer support workers to engage with the most hard to reach patients Along the way, we recognised more and more the value of peer support as an intervention in itself Initial Findings")
11
Some interesting themes emerged in the “stories” that sat behind these patients: Patient perspective – “no-one listens… sick of everyone telling me what to do… they don’t understand…” Clinic perspective – “no matter what we do they don’t change, they miss appointments – they don’t want to be well…” Most of these people are disempowered and feeling hopeless BUT want their lives to be better, want to be well, and have been so grateful to be heard, and provided help in a way that works for them.

13
Peer specialist pilot starts % making first appointment

15
OUTCOME: Activated patient - Activated Services

16
Total cohort to date n=69 46%54%

17
Total cohort to date n=69 Number of participants Age grouping

18
Total cohort to date n=69 Number of participants Ethnic group

21
Changes in GAD-7 score between initial assessment & exit from programme Number of patients

22
Changes in PHQ-9 score between initial assessment & exit from programme Number of patients

Similar presentations










 THW.>")













