Download presentation
Presentation is loading. Please wait.

1
Achieving Equitable Outcomes: Collecting Socio-Demographic Patient Data in Health Care Settings Joseph R. Betancourt, M.D., M.P.H. Director, The Disparities Solutions Center Senior Scientist, Institute for Health Policy Director for Multicultural Education, Massachusetts General Hospital Associate Professor of Medicine, Harvard Medical School

2
Outline Disparities in Health and Health Care Collecting Patient Demographics Case Study of Mass General Hospital –Collecting Race/Ethnicity Data –Measuring and Monitoring Equity –Developing Interventions

3
Diabetes-Related Death Rate, 2010 Deaths per 100,000 population

4
What causes these Racial/Ethnic Disparities in Health? Social Determinants Access to Care Health Care?

5
Racial/Ethnic Disparities in Health Care In patients with insurance… –Disparities based on race for: Influenza vaccination (Gornick et al.) Lung Ca Surgery (Bach et al.) Renal Transplantation (Ayanian et al.) Treatment of chest pain, cardiac catheterization, angioplasty, bypass (Harris et al, Ayanian et al., Peterson et al., Johson et al.) Referral to cardiology specialist care (Schulman et al.) Treatment of HIV/AIDS (Shapiro et al.) Pain management (Todd et al.)
 Lung Ca Surgery (Bach et al.) Renal Transplantation (Ayanian et al.) Treatment of chest pain, cardiac catheterization, angioplasty, bypass (Harris et al, Ayanian et al., Peterson et al., Johson et al.) Referral to cardiology specialist care (Schulman et al.) Treatment of HIV/AIDS (Shapiro et al.) Pain management (Todd et al.)")
6
Disparities in Health Care 2002 Racial/Ethnic disparities found across a wide range of health care settings, disease areas, and clinical services, even when various confounders (SES, insurance) controlled for. Many sources contribute to disparities—no one suspect, no one solution Provider-Patient Communication Stereotyping Mistrust

7
IOM’s Unequal Treatment www.nap.edu Recommendations Increase awareness of existence of disparities Address systems of care –Support race/ethnicity data collection, quality improvement, evidence- based guidelines, multidisciplinary teams, community outreach –Improve workforce diversity –Facilitate interpretation services Provider education – Health Disparities, Cultural Competence, Clinical Decisionmaking Patient education (navigation, activation) Research –Promising strategies, Barriers to eliminating disparities
 Research –Promising strategies, Barriers to eliminating disparities")
8
Quality Health Care Health care should be –Safe –Effective –Patient-centered –Timely –Efficient –Equitable

9
Case Study: Achieving Equity Massachusetts General Hospital

10
MGH Disparities Committee 2003 Underlying Principle While data specific to disparities at MGH important, not necessary to begin to take action given IOM Report documented issue nationally Charge Identify and address disparities in health and health care wherever they may exist at MGH –Subcommittees: Quality, Pt Experience, Education/Awareness –Present plan and results to Board, Executive Council and other hospital leadership regularly

11
Case Study: Achieving Equity at MGH Data Collection

12
Perceived Challenges Collection of information is illegal Patients won’t want to provide information Registrars won’t want to collect information (have history of just deciding patient info) Process will take too long, impede registration Adapting IT systems to collect info costly Uncertain how information will be used
 Process will take too long, impede registration Adapting IT systems to collect info costly Uncertain how information will be used")
13
Data Collection: Timeline Prior to 2003 Collected R/E data in 5 basic categories and preferred language Registrars asked basic questions Little training or quality assurance No preamble to collection of data No campaign to inform patients of purpose Information not linked to quality data

14
Data Collection: Timeline 2003 Boston Mayor convenes Hosp CEO’s & Community Leaders –Agree to effort to address disparities in health and health care –Boston hospitals to be required to collect race/ethnicity 2004 Piloted new method of collection –3 models among 7000 patients (R/E, subgroup, language, education) –Metrics: Collects key info in timely fashion in way patients could understand Registrars receive intense training and QA Process –Includes preamble, methods to respond to questions City releases PR Poster Campaign MGH passes policy that all Quality Data will be stratified by race/ethnicity and language
 –Metrics: Collects key info in timely fashion in way patients could understand Registrars receive intense training and QA Process –Includes preamble, methods to respond to questions City releases PR Poster Campaign MGH passes policy that all Quality Data will be stratified by race/ethnicity and language")
15
Data Collection: Timeline 2006 MA Health Care Reform requires race/ethnicity, language, and highest level of education to be collected MGH begins preparation of Disparities Dashboard –Poster campaign series and website unveiled –Disparities questions incorporated in Quality Rounds –Patient Experience Survey Conducted –Multicultural Advisory Board Convened –Patient Satisfaction stratified by race/ethnicity, and language 2007 MGH develops first Disparities Dashboard Disparities found, interventions developed 2008 MGH begins public reporting via web

17
Case Study: Achieving Equity at MGH Measuring and Monitoring

18
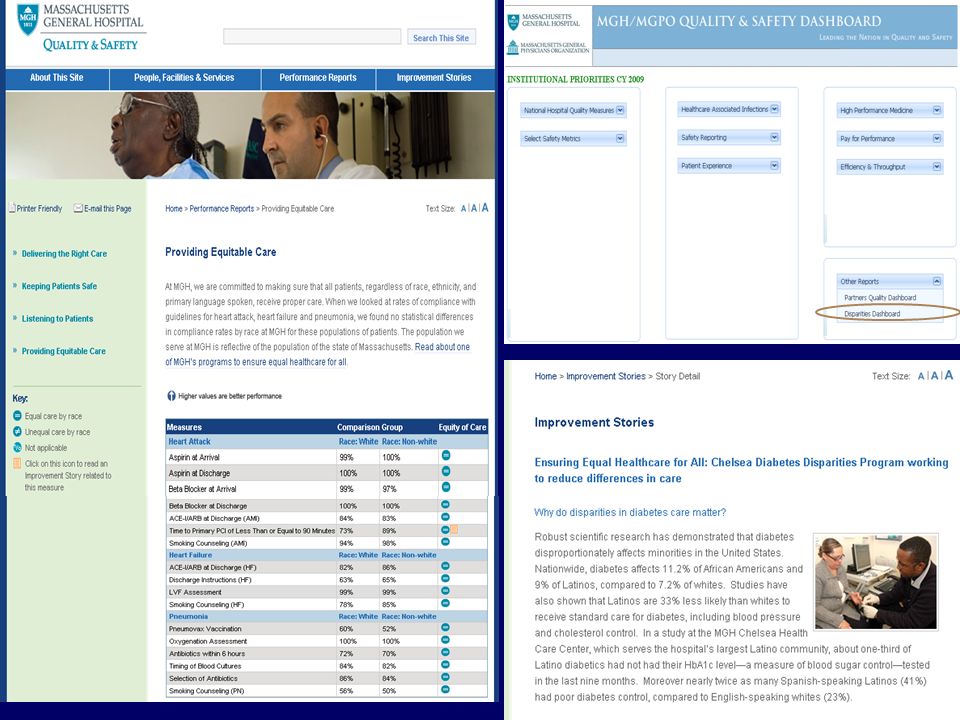
Initial Disparities Dashboard Welcome and Purpose –Definition of Disparities Focus on disparities in care –Purpose of Dashboard Annual Report Embedded into Q and S Reporting –Data and Measurement How race/ethnicity data collected –Process, categories Data Sources –IDX, PATCOM, TSI, H-CAHPS survey data, medical record review (Core/NHQM) Snapshot of diversity of MGH patients –Who they are and where they are seen
 Snapshot of diversity of MGH patients –Who they are and where they are seen")
19
Initial Disparities Dashboard Measures –Clinical quality indicators Inpatient: National Hospital Core Measures –AMI, CHF, CAP, SCIP Outpatient: HEDIS Measures –Mammogram, Pap, CRC Screening –Diabetes, Coronary Artery Disease –Physician, Practice Linkage –Patient Experiences with Care Press-Ganey Inpatient satisfaction by r/e Results of Quality Rounds Results of Minority Survey –Communication with LEP patients

20
Disparities Dashboard Evolution (V2, V3) H-CAHPS Inpatient satisfaction by race/ethnicity All-cause and ACS Admission by race/ethnicity CHF Readmissions by race/ethnicity Sentinel Measures –Mental Health –Pain Mgmt in the ED –Wait time for Renal Transplantation –Orbit time for CABG Patient Experience Summit –Interpreter Pilot Project Cross-Cultural Communication Training Report Public Reporting via external MGH Q/S Website
 H-CAHPS Inpatient satisfaction by race/ethnicity All-cause and ACS Admission by race/ethnicity CHF Readmissions by race/ethnicity Sentinel Measures –Mental Health –Pain Mgmt in the ED –Wait time for Renal Transplantation –Orbit time for CABG Patient Experience Summit –Interpreter Pilot Project Cross-Cultural Communication Training Report Public Reporting via external MGH Q/S Website")
21
Disparities Dashboard Executive Summary –Green Light: Areas where care is equitable National Hospital Quality Measures HEDIS Outpatient Measures (Main Campus) Pain Mgmt in the ED –Orange Light: National disparities, areas to be explored Mental Health, Renal Transplantation All cause and ACS Admissions (so far no disparities) CHF Readmissions (so far no disparities) Patient Experience (H-CAHPS subgroub differences) –Red Light: Disparities found, action being taken Diabetes at community health centers –Chelsea (Latino), Revere (Cambodian) Diabetes Project Colonoscopy screening rates –Chelsea CRC Navigator Program (Latinos)
 Pain Mgmt in the ED –Orange Light: National disparities, areas to be explored Mental Health, Renal Transplantation All cause and ACS Admissions (so far no disparities) CHF Readmissions (so far no disparities) Patient Experience (H-CAHPS subgroub differences) –Red Light: Disparities found, action being taken Diabetes at community health centers –Chelsea (Latino), Revere (Cambodian) Diabetes Project Colonoscopy screening rates –Chelsea CRC Navigator Program (Latinos)")
23
Case Study: Achieving Equity at MGH Developing Interventions

24
The MGH Chelsea Diabetes Program Chelsea: Large minority and immigrant community (Hispanic/Latino primarily, but also Bosnian, Somali) about 3 miles from hospital. MGH Chelsea Healthcare Center provides community based care MGH Chelsea Diabetes Program: A quality improvement / disparities reduction program with 3 primary components: Telephone outreach to increase rate of HbA1c testing Individual coaching to address patients’ needs and concerns regarding diabetes self-management to improve HbA1c Group education meeting ADA requirements

25
* Chelsea Diabetes Management Program began in first quarter of 2007; in 2008 received Diabetes Coalition of MA Programs of Excellence Award *

26
Monitoring Equity: Key Lessons Learned There may be initial resistance and concern –Appropriate messaging, explanation of disparities, description of “work in progress”, blame-free approach is key Not always as easy as it seems, but can be done –Some data systems not easily connected; begin incrementally, build the system step-by-step; perfect not enemy of good –Address basic methodological issues, don’t get bogged down by them Need to expand measure set over time, innovate –Sentinel measures; sub-group analysis of patient experience; errors Mainstreaming essential –Policies, champions make for success and culture change; needs to be owned by Quality and Safety; tailor to your needs

27
Looking towards the Future Building Equitable Systems and Incentives Race/ethnicity and other data collection is essential Need to measure and monitor 20/80 Rule: Conditions of Focus Asthma, Diabetes, CVD, CRC Screen, Mental Health –South Asians and First Nation populations Increase Capacity of Health Care Providers Foster cultural competence of health care providers Empower Patients Support coaching and navigation activities

28
Summary There is a significant body of evidence that has identified racial/ethnic disparities in health care Hospitals can play a major role in their elimination through quality improvement; monitoring equity is key Improving equity will improve the care not only of minorities, but of all patients

29
Thank You Joseph R. Betancourt, MD, MPH jbetancourt@partners.org www.mghdisparitiessolutions.org

Similar presentations