Download presentation
Presentation is loading. Please wait.

1
Cholesterol Metabolism

2
Objectives Define cholesterol as the most important animal steroid.
Know The structure of cholesterol. Discuss the Synthesis of cholesterol. Identify the Regulation of cholesterol. Describe the Excretion of cholesterol. Define Hypercholesterolemia.

3
CHOLESTEROL METABOLISM
Overview: Cholesterol is the most important animal steroid Brain & egg yolk is very rich sources. The liver, kidney and red meat are rich sources. Average diet supplies about g /day.

4
Cholesterol is an extremely important biological molecule that has roles in membrane structure as well as being a precursor for the synthesis of the steroid hormones and bile acids and vit D3 Both dietary cholesterol and that synthesized de novo are transported through the circulation in lipoprotein particles. The same is true of cholesteryl esters, the form in which cholesterol is stored in cells.

5
The synthesis and utilization of cholesterol must be tightly regulated in order to prevent over-accumulation and abnormal deposition within the body Such deposition, eventually leading to atherosclerosis, is the leading contributory factor in diseases of the coronary arteries.

6
Most plasma cholesterol is in an esterified form , w is more hydropobic than free cholesterol.
Cholesteryl esters (CE) are not found in membranes CE are normally present in low levels in most cells Choesterol & CE must be transported in association with protein in LP or solubilized by phospholipids and bile salts in the bile
 are not found in membranes. CE are normally present in low levels in most cells. Choesterol & CE must be transported in association with protein in LP or. solubilized by phospholipids and bile salts in the bile.")
8
Cholesterol: is a sterol (with 8 carbons at C17,= bet 5&6)
Sterols: are steroids with 8-10 carbon atoms in the side chain at C-17 & OH at C-3 Cholesterol is the major sterol in animal tissues Plant sterols as B-sitosterol are poorly absorbed by humans, it blocks the absorption of dietary cholesterol Dietary intake of plant steroid esters (trans fatty acid –free margarine ) helps in reduction of plasma cholesterol
 helps in reduction of plasma cholesterol.")
9
Structure of cholesterol and its ester.
Plant sterols block the absorption of dietary cholesterol.

10
PLASMA CHOLESTEROL Plasma cholesterol level is 150 –
200 mg/dl (average 175 mg/dl) Types: 30% of plasma cholesterol are free and 70% are esterified with polyunsaturated fatty acids (PUFA)
 Types: 30% of plasma cholesterol. are free and 70% are esterified. with polyunsaturated fatty acids. (PUFA)")
11
Biosynthesis of Cholesterol

12
Cholesterol synthesis by all tissues esp
Cholesterol synthesis by all tissues esp.: liver, intestine ,adrenal cortex,& reproductive tissues It occurs in the cytoplasm with enzymes in both the cytosol and the membrane of the endoplasmic reticulum Synthesis begins with the transport of acetyl-CoA from the mitochondrion to the cytosol It needs reducing equivalents in form NADPH & energy from hydrolysis of the high-energy thioester bond of acetyl CoA

13
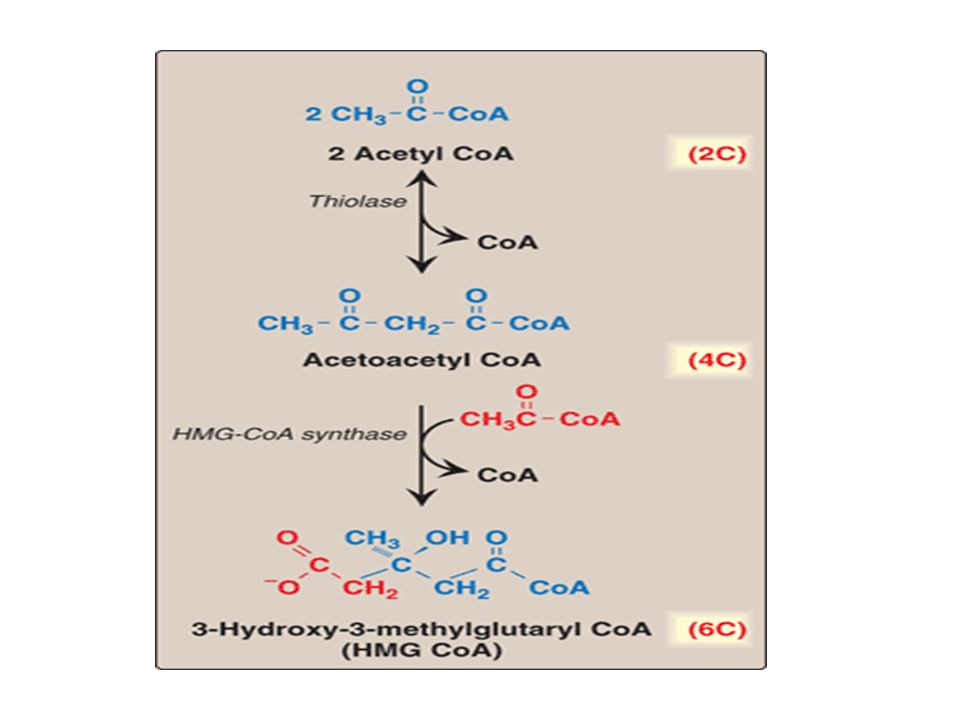
The rate limiting step occurs at the 3-hydroxy-3-methylglutaryl-CoA (HMG-CoA) reductase, HMGR catalyzed step. The phosphorylation reactions are required to solubilize the intermediates in the pathway. After dephosphorylation the intermediates require intracellular sterol carrier protein to keep them soluble Release of pyrophosphate in the condensation steps make the reactions irreversible

14
Liver parenchymal cells contain two isoenzymes of HMGCoA synthhase The cytolsolic enzyme participates in cholesterol synthesis & the mitochondrial enzyme for ketone bodies synthesis HMGCoA synthase is an intrinsic membrane protein of the endoplasmic reticulum with the enzyme catalytic domain projecting into the cytosol

16
Squalene monooxygenase
6C 5C C30 to C27 Removal of CH3 at C4 = migration from C8 to C5 Reduction of= bet C24&C25 10C 15C NADPH NADP Squalene synthase O2+NADPH+H Cyclization CYCLE 1ST 27C Squalene monooxygenase

17
Regulation of Cholesterol Synthesis

18
1.Sterol-dependent regulation of gene expression:↑Cholesterol – transcription factor
2.Sterol-independent phosphorylation/dephosphorylation 3.Hormonal regulation 4.Inhibition by drugs: simvastatin, lovastatin &mevastatin

19
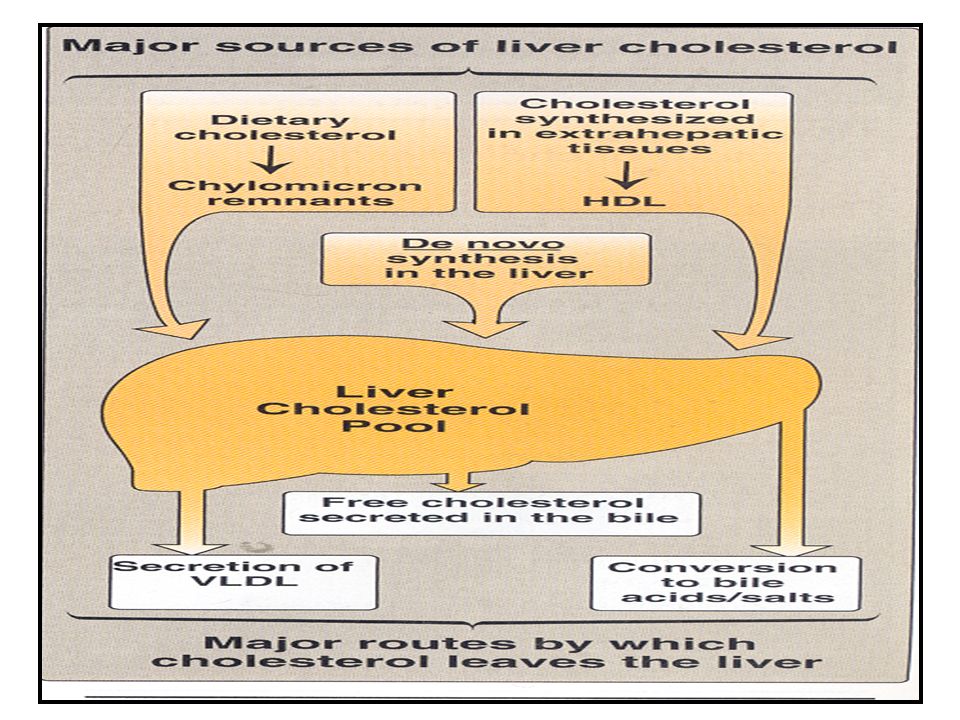
Cholesterol Degradation
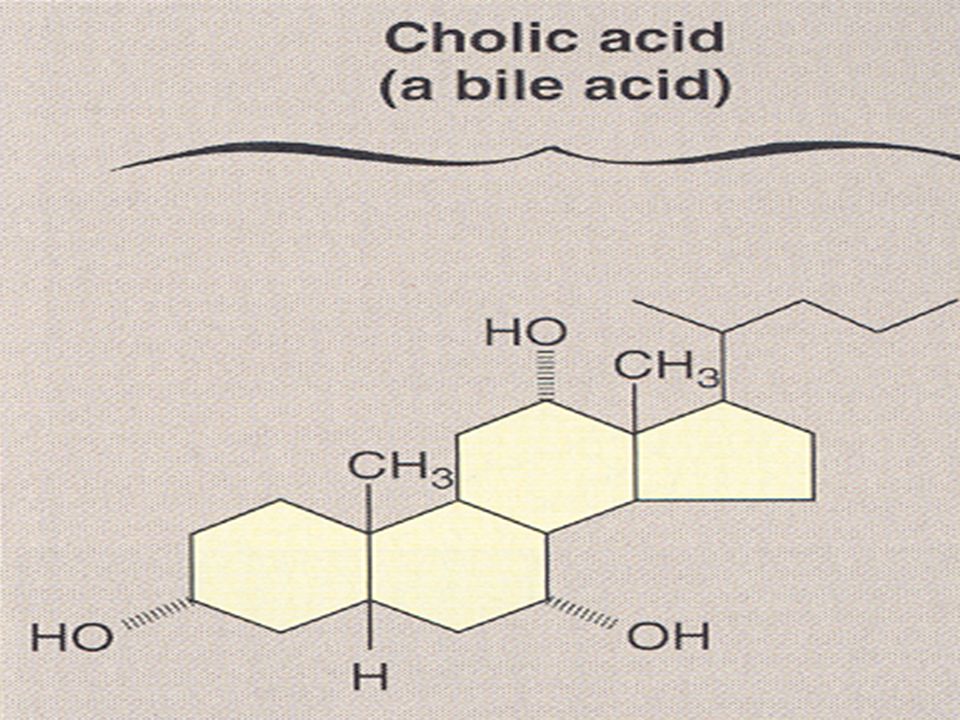
Ring of sterol can’t be metabolized to CO2 & H2O in humans Secretion as such in bile Conversion to bile acids Intest. Egested as such Modified by bacteria by reduction Coprostanol & cholestanol isomers )( Neutral sterols
( Neutral sterols.")
20
Bile acids & salts Bile consists of org. & inorg. watery mixture
Lecithin & bile salts are the most important org .quantitatively Bile liver duodenum stored in GB Bile salts are more effective detergents than bile acids b/c of their enhanced amphipathic structure

22
HYPERCHOLESTEROLEMIA
It is the increase of plasma cholesterol above 220 mg/dl. Hypercholesterolemia is associated with atherosclerosis, coronary heart disease (CHD), heart attacks, and stroke Causes: 1) Overfeeding of diet rich in cholesterol, Fats specially saturated FA ,or carbohydrates 2) Diabetes mellitus (D.M.) 3) Hypothyroidism: due to decreased conversion to bile acids 4) Obstructive jaundice: due to the obstruction no excretion of cholesterol or bile salts in the bile 5) Familial hypercholesterolemia
, heart attacks, and stroke. Causes: 1) Overfeeding of diet rich in cholesterol, Fats specially. saturated FA ,or carbohydrates. 2) Diabetes mellitus (D.M.) 3) Hypothyroidism: due to decreased conversion to bile acids. 4) Obstructive jaundice: due to the obstruction no excretion of cholesterol or bile salts in the bile. 5) Familial hypercholesterolemia.")
23
Treatment of Hypercholesterolemia
1- Diet: Decrease carbohydrate, saturated fatty acids and cholesterol in diet. Increase polyunsaturated fatty acids 2- Hypocholesterolemic drugs: Statin drugs e.g. Atorvastatin (Lipitor) and simvastatin (Zocor) are used to decrease plasma cholesterol levels in patients with hypercholesterolemia Statin drugs are competitive inhibitors of HMG CoA reductase
 and simvastatin (Zocor) are used. to decrease plasma cholesterol levels in patients with. hypercholesterolemia. Statin drugs are competitive inhibitors of HMG CoA. reductase.")
24
Lipoproteins Metabolism

25
Introduction Lipid compounds: Relatively water insoluble
Therefore, they are transported in plasma (aqueous) as Lipoproteins
 as Lipoproteins.")
26
Lipoproteins and Related Clinical Problems
Atherosclerosis and hypertension Coronary heart diseases Lipoproteinemias (hypo- and hyper-) Fatty liver
 Fatty liver.")
27
Lipoprotein Structure
Protein part: Apoproteins or apolipoproteins These proteins may be structural or transferred Lipid part: According to the type of lipoproteins Different lipid components in various combinations

28
Spherical molecules of lipids and proteins (apoproteins) = amphipathic molecules
Outer coat: - Apoproteins - Phospholipids - Cholesterol (Unesterified) Inner core: - TG - Cholesterol ester (CE) Lipoprotein Structure
 Inner core: - TG. - Cholesterol ester (CE) Lipoprotein Structure.")
29
Apoproteins Five major classes (A-E) divided by structure & function
Each class has subclasses as Apo A1, Apo CII Functions Some are required as structural proteins Some are activators, Some are recognition sites.

30
Types of Lipoproteins There are various types of lipoproteins:
They differ in lipid and protein composition and therefore, they differ in: - Size and density - Electrophoretic mobility

31
Chylomicrons Very low density Lipoprotein (VLDL) Low density
Lipoprotein (LDL) High density Lipoprotein (HDL) Types and Composition of Lipoproteins
 High density. Lipoprotein (HDL) Types and. Composition. of. Lipoproteins.")
32
Composition of LDL and HDL
Low density lipoprotein (LDL) Mostly free cholesterol High density lipoprotein (HDL) Mostly cholesterol ester More % protein More % phospholipids
 Mostly free cholesterol. High density lipoprotein (HDL) Mostly cholesterol ester. More % protein. More % phospholipids.")
33
Ultracentrifugation of Lipoproteins

34
Lipoprotein Electrophoresis

35
Plasma Lipoproteins For triacylglycerol transport (TG-rich):
- Chylomicrons: TG of dietary origin - VLDL: TG of endogenous (hepatic) synthesis For cholesterol transport (cholesterol-rich): LDL: Mainly free cholesterol HDL: Mainly esterified cholesterol
 synthesis. For cholesterol transport (cholesterol-rich): LDL: Mainly free cholesterol. HDL: Mainly esterified cholesterol.")
36
Chylomicrons Assembled in intestinal mucosal cells Lowest density
Largest size Highest % of lipids and lowest % proteins Highest triacylglycerol (dietary origin) Carry dietary lipids to peripheral tissues Responsible for physiological milky appearance of plasma (up to 2 hours after meal)
 Carry dietary lipids to peripheral tissues. Responsible for physiological milky appearance of plasma (up to 2 hours after meal)")
37
Type I hyperlipoprotemia
Apo E mediates uptake

38
Lipoprotein Lipase Extracellular enzyme anchored by heparan sulphate to the capillary walls of most tissue esp those of adipose tissue, cardiac & skeletal muscles Its synthesis & transfer to luminal surface of the capillary is stimulated by insulin Activated by apoC-II

39
Isomers of lipoprotein lipase have different kms for TAG :high km in the adipose enzyme
Low km in the heart enzymes is absent in adult liver which has hepatic lipase on the endothelial surface which assists in HDL metabolism mainly

40
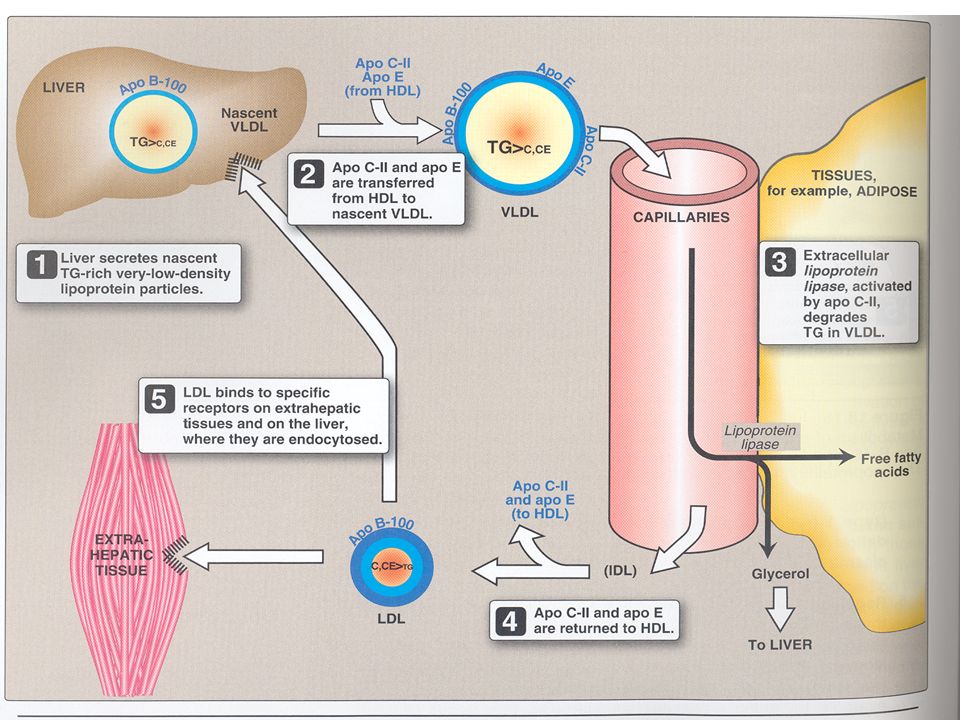
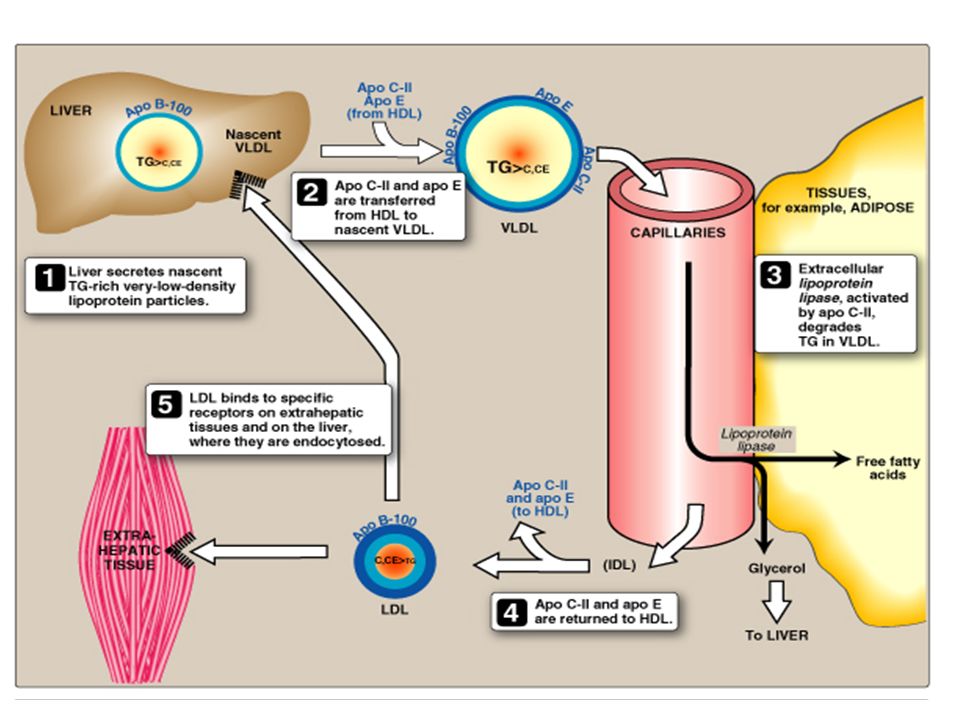
Metabolism of VLDL

42
Choleteryl Ester Transfer Protein
VLDL CE PL ,TAG HDL Choleteryl Ester Transfer Protein

43
Composition of LDL and HDL
Low density lipoprotein (LDL) Mostly free cholesterol High density lipoprotein (HDL) Mostly cholesterol ester More % protein More % phospholipids
 Mostly free cholesterol. High density lipoprotein (HDL) Mostly cholesterol ester. More % protein. More % phospholipids.")
44
Low Density Lipoprotein
LDL carries about 70% of total plasma cholesterol High LDL-C level is well established risk factor for development of coronary heart disease The diagnosis of a primary defect is made after secondary defect causes have been ruled out

45
Low Density Lipoproteins (LDL)
Produced in the circulation as the end product of VLDLs Compared to VLDLs: It contains only apo B-100 Smaller size and more dense Less TG More cholesterol & cholesterol ester Transport cholesterol from liver to peripheral tissues Uptake of LDL at tissue level by LDL receptor-mediated endocytosis Recognized by apo B-100

47
LDL: Receptor-Mediated Endocytosis

48
Receptor-Mediated Endocytosis
LDL receptor: Cell surface glycoprotein High-affinity, tightly regulated LDL/Receptor binding and internalization of the complex by endocytosis Release of cholesterol inside the cells for: Utilization Storage as cholesterol ester Excretion Degradation of LDL: into amino acids, phospholipids and fatty acids Degradation or recycling of receptor

49
LDL Receptor-Mediated Endocytosis: Regulation
Down-regulation: High intracellular cholesterol content Degradation of LDL receptors Inhibition of recepotor synthesis at gene level Decrease No. of receptor at cell surface Decrease further uptake of LDL Decrease de novo synthesis of cholesterol Up-regulation: Low intracellular cholesterol content Recycling of LDL receptors Stimulation of recepotor synthesis at gene level Increase No. of receptor at cell surface Increase further uptake of LDL Increase de novo synthesis of cholesterol

50
Plasma LDL can be measured by ultracentrifugation, but this is not a practical technique
Calculated LDL: LDL-C= total cholesterol –[HDL-C]+ TAG/2.2) in case of mmol/L or 5 in case of mg/dL LDL exits in a range of sizes & densities which can be detected by electrophoresis. There is evidence that small dense LDL is atherogenic
 in case of mmol/L or 5 in case of mg/dL. LDL exits in a range of sizes & densities which can be detected by electrophoresis. There is evidence that small dense LDL is atherogenic.")
51
Coronary Heart Disease Risk Factors Determined by (Exclusive of LDL –C) NCEP ATP III
Positive Risk Factors: Age ≥ 45 y for men , ≥55 y for females or premature menopause Family history of premature CHD Current cigarette smoking Hypertension ( BP≥ 140/90 or taking antihypertensive drugs HDL-C concentration < 40 mg/dL ( < 1.0 mmol/L) Diabetes mellitus = CHD risk equivalent Metabolic syndrome (multiple metabolic risk factors Negative Risk Factors: HDL-C concentration ≥ 60 mg/ dL (≥ 1.6 mmol/L) ; its presence removes one risk factor from the total count
 Diabetes mellitus = CHD risk equivalent. Metabolic syndrome (multiple metabolic risk factors. Negative Risk Factors: HDL-C concentration ≥ 60 mg/ dL (≥ 1.6 mmol/L) ; its presence removes one risk factor from the total count.")
52
Categories of Risk for LDL Cholesterol Goals
LDL goal mg/dL < 100 <130 <160 Risk Category CHD & CHD risk equivalents Multiple (2+) risk factors 0-1 risk factor For cholesterol the molar concenteration can be changed to mass concentration by the formula: mg/dL =mmol/L x 38.7
 risk factors. 0-1 risk factor. For cholesterol the molar concenteration can be changed to mass concentration by the formula: mg/dL =mmol/L x")
53
HDL Metabolism PC = Phosphatidylcholine/Lecithin

54
High Density Lipoproteins (HDL)
Produced by intestine and liver Nascent HDL: Disk-shaped Contains apo A-I, C-II and E Contains primarily phospholipid (PC) Mature HDL (HDL2): First, the HDL3 collects cholesterol (C) Then, C is converted to CE (C- ester) The HDL2 is the spherical mature particle
 Mature HDL (HDL2): First, the HDL3 collects cholesterol (C) Then, C is converted to CE (C- ester) The HDL2 is the spherical mature particle.")
55
Functions of HDL Reservoir of apoproteins e.g., Apo C-II and E to VLDL
Uptake of cholesterol: From other lipoproteins & cell membranes (HDL is suitable for uptake of cholesterol because of high content of PC that can both solublizes cholesterol and acts as a source of fatty acid for cholesterol esterification) Esterification of cholesterol: Enzyme:PCAT/LCAT Activator: Apo A-I Substrate: Cholesterol, Co-substrate: PC Product: Cholesterol ester (& Lyso-PC) Reverse cholesterol transport
 Esterification of cholesterol: Enzyme:PCAT/LCAT Activator: Apo A-I Substrate: Cholesterol, Co-substrate: PC Product: Cholesterol ester (& Lyso-PC) Reverse cholesterol transport.")
56
Why Is HDL a Good Cholesterol carrier?
Inverse relation between plasma HDL levels and atherosclerosis …. How? Reverse cholesterol transport involves: Efflux of cholesterol from peripheral tissues and other lipoproteins to HDL3 Esterification of cholesterol & binding of HDL2 to liver and stroidogenic cells by scavenger receptor class B (SR-B1) Selective transfer of cholesterol ester into these cells Release of lipid-depleted HDL3
 Selective transfer of cholesterol ester into these cells. Release of lipid-depleted HDL3.")
57
Lp(a) Simulates LDL but apo(a) covalently linked to apo B-100
Competes with plasminogen to plasminogen activator Genetical element Estrogen decreases it while trans fats increases it

58
Abnormalities in lipoprotein metabolism
Type I hyperlipoproteinemia = F.lipoprotein lipase deficiency Due deficiency of lipoprotein lipase or apo C-II -> accumulate of triaryglycerol –rich lipoptn in plasma Type II hyperlipidemia = F.hypercholesterolemia -familial hyperbetalipoproteinalmia deficiency of functional LDL receptors -> elevation of plasma cholesterol but plasma TG remains normal There ie premature atherosclerosis Type III hyperlipoteinemia = F. dysbetalipoproteinemia or broad B disease Deficiency of apo E -> accumulation of chylomicron remnants in plasma . There’s hyperchloesterolemia with premature atherosclerosis

59
Abetalipoproteinemia defective triacyglycerol transfer protein
No chylomicrons ↓TG& ↑ TG in small intestine & liver No VLDL No VLDL no LDL ↓ cholesterol Hypobetalipoproteinanemia There ‘s ↓ apo B-100 synthesis ↓ VLDL ↓ TG & ↑ TG in liver ↓ LDL ↓ cholesterol Fatty liver : there’s imbalance between hepatic TG synthesis & secretion of VLDL Causes . hepatitis ,DM, chronic ethanol ingestin

Similar presentations












>")






