Download presentation
Presentation is loading. Please wait.

1
WV HFMA Spring Revenue Cycle Meeting March 26, 2013 Presented by: Linda Fotheringill, Esq. Principal & Co-Founder of Washington & West, LLC Role of Patient Access in Denial Prevention and Intervention

3
Discussion Objectives: 1. The Role of Patient Access in prevention of Lack of Authorization denials 2. Best Practice concepts for denial prevention 3. The Role of Patient Access in prevention of Medicare Denials 4. CMS Ruling No.: CMS-1455-R

4
Denials – Some Top Reasons 1. The claim was filed Late. 2. The Insurance Company Lost the Claim, and then the Claim Expired 3. Lack of Preauthorization / Authorization 4. The Patient Didn’t acquire a Referral from a Physician 5. You Provided Two Services in One Day 6. You Ran Out of Authorized Sessions 7. The Authorization Expired 8. The Patient Changed His or Her Insurance Plan 9. The Patients' Out-of-network Benefits Differ from In-network Benefits 10. The Service was Already Rendered 11. The Patient has an Out-of-State Insurance Plan 12. The Patient Lost His or Her Insurance Coverage 13. The Patient was Late to pay Their COBRA 14. Claim sent to the Wrong Managing Company 15. The Provider doesn’t participate with the Insurance Company 16. Services Were Rendered at the Wrong Location

5
Lack of Authorization Denials A 2009 study by the United States Government Accountability Office found the following rate of lack of authorization denials in four states: Ohio 2009 11 % across all insurers licensed in the state Connecticut 2009 14 % across 21 managed care organizations licensed in the state Maryland 2007 16 % across 41 insurers licensed in the state California 24 % across six of the largest managed care organizations licensed in the state

6
Lack of Authorization – what does this denial really mean? Accountable Dept/Entity 1. Payer 2. Patient Access, UM 3. UM, Payer, Attending Physician 4. UM, Payer, Attending Physician 5. UM, Attending Physician 6. Payer Refined Code Examples 1. Auth Obtained/Erroneously denied 2. Adm. Scheduled/Hosp. failed to contact payer/obtain Auth 3. Additional days requested/auth approval for lower level of care 4. Additional days requested/auth refused 5. Additional days not requested/stay exceeded auth 6. Auth not obtained but not required

7
Track accurate & meaningful data Accurate & Meaningful Data Includes: Refined denial/variance codes linked to accountable Departments, individuals (i.e., Coders & Physicians), and entity Denial/variance codes linked to Contract provisions and/or DRG, CPT, etc. Detailed denial/audit database & feedback tool

8
Best Practice Denial Prevention Maximize Opportunities with Appeal Team Intervention/Appeal Track Purpose: To prevent retraction or obtain full payment Methodology: To pursue all appeal levels until payment received or appeal and dispute resolution procedure exhausted. Prevention Track Purpose: To prevent future denials & ensure compliance. Methodology: Provide appropriate feedback to Hospital Department & staff Track all denials by Department/Physician Educate & respond according to data Monitor & Measure Response

9
If I Knew Then What I Know Now… The information that is obtained during the admitting process is crucial to prevent and fight denials Almost all technical denials can be challenged Facts State and federal laws Contract provisions Registration and Admitting staff should have access to key contract provisions and laws Prevention of denials Obtain critical facts

10
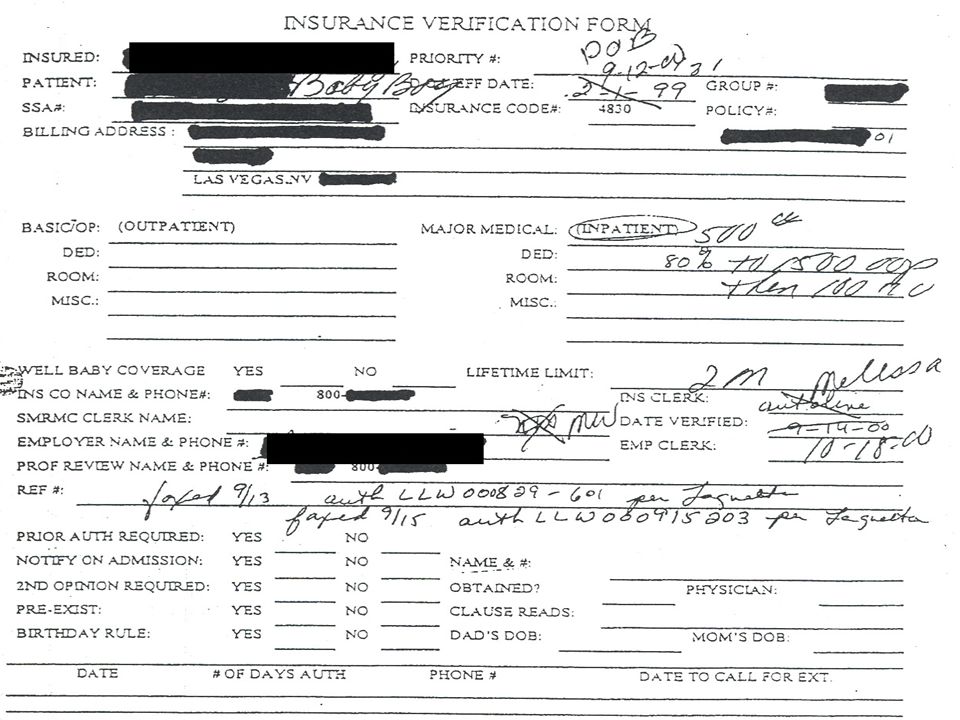
Insurance Verification Process Just asking the right questions can prevent denials Elicit information that is not routinely provided Specific policy exclusions Pre-existing conditions Opportunity to correct potential benefit problems Early registration Lapses in coverage during admission/patient involvement Documentation is the key to fight denials Misverification of benefits/eligibility

11
There are state and federal laws on the following denial management issues: Authorization Modification of authorization, delivery/newborn, emergency services Claims submission Minimum time frames Prompt payment Definition of clean claim, payment time frames, interest penalty Misverification of benefits Internal/External Appeals Subrogation Retroactive denials/ Retractions Notice prejudice Lien laws Workers compensation, Third Party Liability Pre-existing conditions Emergency Services State law definitions, EMTALA Continuation of Benefits ERISA Coordination of benefits Automatic newborn coverage Experimental treatment

12
WVC §33-45-2 Minimum fair business standards contract provisions required; processing and payment of health care services; provider claims… (6) Every insurer shall pay a clean claim if the insurer has previously authorized the health care service or has advised the provider or enrollee in advance of the provision of health care services that the health care services are medically necessary and a covered benefit, unless: (A) The documentation for the claim provided by the person submitting the claim clearly fails to support the claim as originally authorized; or (B) The insurer's refusal is because: (i) Another payor or party is responsible for the payment; (ii) The provider has already been paid for the health care services identified on the claim; (iii) The claim was submitted fraudulently or the authorization was based in whole or material part on erroneous information provided to the insurer by the provider, enrollee, or other person not related to the insurer; (iv) The person receiving the health care services was not eligible to receive them on the date of service and the insurer did not know, and with the exercise of reasonable care could not have known, of the person's eligibility status; (v) There is a dispute regarding the amount of charges submitted; or (vi) The service provided was not a covered benefit and the insurer did not know, and with the exercise of reasonable care could not have known, at the time of the certification that the service was not covered.
 Every insurer shall pay a clean claim if the insurer has previously authorized the health care service or has advised the provider or enrollee in advance of the provision of health care services that the health care services are medically necessary and a covered benefit, unless: (A) The documentation for the claim provided by the person submitting the claim clearly fails to support the claim as originally authorized; or (B) The insurer s refusal is because: (i) Another payor or party is responsible for the payment; (ii) The provider has already been paid for the health care services identified on the claim; (iii) The claim was submitted fraudulently or the authorization was based in whole or material part on erroneous information provided to the insurer by the provider, enrollee, or other person not related to the insurer; (iv) The person receiving the health care services was not eligible to receive them on the date of service and the insurer did not know, and with the exercise of reasonable care could not have known, of the person s eligibility status; (v) There is a dispute regarding the amount of charges submitted; or (vi) The service provided was not a covered benefit and the insurer did not know, and with the exercise of reasonable care could not have known, at the time of the certification that the service was not covered.")
13
WVC §33-45-2 (continued) (2) Each insurer shall maintain a written or electronic record of the date of receipt of a claim. The person submitting the claim shall be entitled to inspect the record on request and to rely on that record or on any other relevant evidence as proof of the fact of receipt of the claim. If an insurer fails to maintain an electronic or written record of the date a claim is received, the claim shall be considered received three business days after the claim was submitted based upon the written or electronic record of the date of submittal by the person submitting the claim.

14
WVC §33-25A-8d Coverage of emergency services (1) Every insurer shall provide coverage for emergency medical services, including prehospital services, to the extent necessary to screen and to stabilize an emergency medical condition. The insurer shall not require prior authorization of the screening services if a prudent layperson acting reasonably would have believed that an emergency medical condition existed. Prior authorization of coverage shall not be required for stabilization if an emergency medical condition exists. Payment of claims for emergency services shall be based on the retrospective review of the presenting history and symptoms of the covered person. (E) "Medical screening examination" means an appropriate examination within the capability of the hospital's emergency department, including ancillary services routinely available to the emergency department, to determine whether or not an emergency medical condition exists; and..
 Medical screening examination means an appropriate examination within the capability of the hospital s emergency department, including ancillary services routinely available to the emergency department, to determine whether or not an emergency medical condition exists; and...")
17
Authorization Process Obtaining an authorization number for an admission is only half the battle What does the authorization number cover? Tracking number Our facility - transfers/direct admissions Inpatient vs. outpatient Number of days authorized Documentation of name, phone & department of person providing authorization Insurer’s refusal to authorize admission Participating facility/lower level of care Where should the patient be admitted to?

19
What is the Must Have Contract Provision for Lack of Authorization Denials? “Insurer shall not deny or reduce payment for any Medically Necessary Covered Services based on Hospital’s failure to comply with any administrative or notification requirements as set forth in this Agreement and/or the Provider Manual insofar as such services would have been authorized as Medically Necessary if the notification had been provided in the appropriate time.”

20
What about Medicare?

21
CMS 2011 Financial Report Medicare & Medicaid payments represent: 53 cents of every $ spent on nursing homes 49 cents of every $ received by hospitals 31 cents of every $ spent on physicians Source: U.S. Treasury$ in billions

22
Economic Reality CMS 2012 Financial Report estimates c omplete exhaustion of Medicare Part A trust funds by 2024 GAO’s simulations continue to illustrate that the long-term fiscal outlook is unsustainable. … health care spending seen as the culprit. (80 million Americans will become eligible for Social Security retirement benefits over the next two decades—an average of more than 10,000 per day) GAO reports $28.8 billion in improper payments in FY 2011 President’s Remarks to Joint Session of Congress: “…we’ve estimated that most of this plan [PPACA] can be paid for by finding savings within the existing health care system, a system that is currently full of waste and abuse.” CMS committed to “aggressive corrective actions”
 GAO reports $28.8 billion in improper payments in FY 2011 President’s Remarks to Joint Session of Congress: …we’ve estimated that most of this plan [PPACA] can be paid for by finding savings within the existing health care system, a system that is currently full of waste and abuse. CMS committed to aggressive corrective actions .")
23
United States Government Accountability Office (GAO) http://www.gao.gov/assets/590/589681.pdf
")
24
Aggressive Corrective Action? ZPIC RAC MAC MIC QIO CERT OIG DOJ FBI

25
The current landscape….. “The OIG believes … healthcare providers have an ethical and legal duty to ensure the integrity of their dealings with these programs. This duty includes an obligation to take measures, such as instituting a compliance program, to detect and prevent fraudulent, abusive and wasteful activities. It also encompasses the need to implement specific procedures and mechanisms to examine and resolve instances of non-compliance with program requirements.”

26
Mandatory Compliance Program under PPACA 1.PPACA Sec. 6102 applies to Medicare & Medicaid SNFs 8 core elements of mandatory program 2.PPACA Sec. 6401 applies to all Medicare & Medicaid providers DHHS required to promulgate “core elements” with effective date (but no deadline yet) Sept 2010 HHS proposed rule indicates similar core elements to SNF & elements of U.S. Federal Sentencing Guidelines
 Sept 2010 HHS proposed rule indicates similar core elements to SNF & elements of U.S. Federal Sentencing Guidelines.")
27
Does your current Compliance Program adequately detect and prevent fraudulent, abusive and wasteful activities? Does your current Compliance Program adequately implement specific procedures and mechanisms to examine and resolve instances of non-compliance?

28
CMS RAC Appeals Update – June 2012 CLAIMS DENIALS OVERTURNED ON APPEALFY 2011 Number of claims with overpayment determinations 903,372 Number of claims where the provider appealed (any level) 56,620 Number of claims with appeal decisions in provider’s favor 24,548 Percentage of appealed claims with a decision in provider’s favor* 43.4% Number of claims where provider did not appeal 846,752 Percentage of claims overturned on appeal for all denials 2.7% * Often time Part B and DME claims are corrected through the appeals process, which means the reason for the denial is upheld but the provider is allowed to correct the claim and rebill using the appropriate code(s).
 56,620 Number of claims with appeal decisions in provider’s favor 24,548 Percentage of appealed claims with a decision in provider’s favor* 43.4% Number of claims where provider did not appeal 846,752 Percentage of claims overturned on appeal for all denials 2.7% * Often time Part B and DME claims are corrected through the appeals process, which means the reason for the denial is upheld but the provider is allowed to correct the claim and rebill using the appropriate code(s).")
29
Concerning Observations… Continuing problems with clear documentation of medical necessity. Physicians are often not demonstrating a clear understanding of Medicare’s criteria EHRs are often inadequate for establishing compliance with Medicare criteria Lack of resources and/or culture to focus on improper payment prevention Healthcare Providers/Hospitals are “reactive” rather than “proactive”

30
OIG Work plan - 2013 Hospitals—Inpatient and Outpatient Payments to Acute Care Hospitals We will review Medicare payments to hospitals to determine compliance with selected billing requirements. We will use the results of these reviews to recommend recovery of overpayments and identify providers that routinely submit improper claims. Prior OIG audits, investigations, and inspections have identified areas at risk for noncompliance with Medicare billing requirements. Using computer matching and data mining techniques, we will select hospitals for focused reviews of claims that may be at risk for overpayments. Using the same techniques, we will identify hospitals that broadly rank as least risky across compliance areas and those that broadly rank as most risky. We will then review the hospitals’ policies and procedures to compare the compliance practices of these two groups of hospitals. We will also survey or interview hospitals’ leadership and compliance officers to provide contextual information related to hospitals’ compliance programs.

31
The cost of failing to comply with Medicare criteria? Ultimately, will depend in part on whether deemed Fraud, Abuse, or an Improper Payment. Example: Civil penalty for False Claim liability is treble the amount of damages plus $5,000 to $10,000 for each claim!

32
How far back can the OIG go? (b) A civil action under section 3730 may not be brought— (1) more than 6 years after the date on which the violation of section 3729 is committed, or (2) more than 3 years after the date when facts material to the right of action are known or reasonably should have been known by the official of the United States charged with responsibility to act in the circumstances, but in no event more than 10 years after the date on which the violation is committed, whichever occurs last.
 A civil action under section 3730 may not be brought— (1) more than 6 years after the date on which the violation of section 3729 is committed, or (2) more than 3 years after the date when facts material to the right of action are known or reasonably should have been known by the official of the United States charged with responsibility to act in the circumstances, but in no event more than 10 years after the date on which the violation is committed, whichever occurs last..")
33
Per Medicare Learning Network “…there is no precise measure of health care fraud…” Fraud? Abuse? Improper Payment? Reasonable Minds can Differ?

34
What Is Medicare Fraud? Office of Inspector General: U.S. Department of Health and Human Services This Web page contains information about OIG's most-wanted health care fugitives. In all, we are seeking more than 170 fugitives on charges related to health care fraud and abuse. Click any of the photos below for more information about the fugitives or view captured fugitivesview captured fugitives Etienne Allonce Tarek Wehbe DOB: 06-28-1965 DOB: 11-29-1964 Height: UNK Height: 5’8” Weight: UKN Weight: 214 lbs Carlos Benitez Luis Benitez DOB: 08-03-1961 DOB: 06-06-1966 Height: 5'9“ Height: 5’11”http://oig.hhs.gov/fugitives/ Weight: 180 lbs Weight: 195 lbs

35
What Is Medicare Abuse? Practices that, either directly or indirectly, result in unnecessary costs to the Medicare Program. “Abuse appears quite similar to fraud except that it is not possible to establish that abusive acts were committed knowingly, willfully, and intentionally.” Examples of Medicare abuse may include: Misusing codes on a claim, Charging excessively for services or supplies, and Billing for services that were not medically necessary or services that do not meet professionally recognized standards. Both fraud and abuse can expose providers to criminal and civil liability.

36
Question….. Can billing Medicare for a knee replacement when the documentation does not support medical necessity per CMS criteria be considered fraud or abuse? What about when the denial is not appealed? If so, Providers are exposed to civil and criminal liability.

37
News Release, February 11, 2013 Departments of Justice and Health and Human Services announce record-breaking recoveries resulting from joint efforts to combat health care fraud Government Teams Recovered $4.2 Billion in FY 2012 Attorney General Eric Holder and Health and Human Services (HHS) Secretary Kathleen Sebelius report that for every dollar spent on health care-related fraud and abuse investigations in the last three years, the government recovered $7.90. This is the highest three-year average return on investment in the 16-year history of the Health Care Fraud and Abuse (HCFAC) Program.
 Program..")
38
OIG EDUCATIONAL STATEMENT- Not just after the big fish… False Claims Act cases are in the news and many involve large companies, such as drug and device manufacturers or pharmaceutical companies. “But there also are many cases involving smaller entities and individuals. For example, a recent FCA case involved a cardiologist who allegedly submitted claims to the Federal health care programs for services that were not supported by patient medical records and did not meet the billing criteria. Additionally, the physician allegedly billed separately for services that the government had already paid for as part of a bundled payment for a group of services. To resolve these allegations the doctor paid $435,000 and entered into a 5-year Integrity Agreement.”

39
OIG – 2013 Work Plan Recovery Audit Contractors—Identification and Recoupment of Improper and Potentially Fraudulent Payments and CMS’s Oversight and Response “We will determine the extent that Recovery Audit Contractors (RAC) identified improper payments, identified vulnerabilities, and made potential fraud referrals in 2010 and 2011. We will also review the activities that CMS performed to resolve RAC-identified vulnerabilities, address potential fraud referrals, and evaluate RAC performance in 2010 and 2011. (Affordable Care Act, § 6411.)”
 .")
40
Zone Program Integrity Contractors (ZPICs) ZPICZoneStates in Zone Safeguard Services1 California, Hawaii, Nevada, American Samoa, Guam, and the Mariana Islands AdvanceMed2 Washington, Oregon, Idaho, Utah, Arizona, Wyoming, Montana, N. Dakota, S. Dakota, Nebraska, Kansas, Iowa, Missouri, Alaska Cahaba3 Minnesota, Wisconsin, Illinois, Indiana, Michigan, Ohio, Kentucky Health Integrity4Colorado, New Mexico, Texas, Oklahoma AdvanceMed5 Arkansas, Louisiana, Mississippi, Tennessee, Alabama, Georgia, N. Carolina, S. Carolina, Virginia, W. Virginia Under Protest6 Pennsylvania, New York, Delaware, Maryland, D.C., New Jersey, Massachusetts, New Hampshire, Vermont, Maine, Rhode Island, Connecticut Safeguard Services7Florida, Puerto Rico, Virgin Islands ZPICs identify target areas based on: Investigations OIG and law enforcement instructions Congressional mandates Data Mining or “Predictive Modeling”

41
MAC “Provider Tracking System” (PTS) MACs must have a PTS Will identify all providers & track all contacts to correct “problems” such as medical necessity issues & repeated “billing abusers” Information coordinated with ZPIC Quarterly reassessments to see if behavior has changed Information shared with Administrative Law Judge when cases appealed
 MACs must have a PTS Will identify all providers & track all contacts to correct problems such as medical necessity issues & repeated billing abusers Information coordinated with ZPIC Quarterly reassessments to see if behavior has changed Information shared with Administrative Law Judge when cases appealed")
42
Administrative Law Judge Comment in Unfavorable ALJ Decision: “The Provider was unquestionably aware of the CMS regulations, manuals and rulings, CMS bulletins, past unfavorable CMS contractor actions and the lack of substantiating medical records. See 42 CFR Section 411.406(e) (knowledge presumed from experience and constructive notice of CMS publications).”
 (knowledge presumed from experience and constructive notice of CMS publications). .")
43
Alabama Medical Review of LCD A-03-03 (Replacement of Lower Extremity Joint) May 2005 – Error Rate 88.78% ($1,585,067 charges denied of 107 Claims reviewed for 49 Providers) Majority of denials because “documentation in the medical record did not provide sufficient justification for the services rendered” QIO did targeted education to improve compliance December 2005 – Error Rate increased to 91.25% ($1,034,375 charges denied of 100 Claims reviewed for 42 Providers)
 May 2005 – Error Rate 88.78% ($1,585,067 charges denied of 107 Claims reviewed for 49 Providers) Majority of denials because documentation in the medical record did not provide sufficient justification for the services rendered QIO did targeted education to improve compliance December 2005 – Error Rate increased to 91.25% ($1,034,375 charges denied of 100 Claims reviewed for 42 Providers)")
44
Sample Issue: DRG 470: Joint Replacement or Reattachment of Lower Extremity

45
Medicare Newsletter – June 6, 2011 DRG 470: Joint Replacement or Reattachment of Lower Extremity In order to meet the criteria for a total knee replacement procedure, all of the following must be documented: Documentation of level of pain and worsening of pain Pain that is increased with activity Pain that is increased with weight bearing Pain that interferes with activities of daily living Pain with passive range of motion Limited range of motion Crepitus Joint effusion / swelling

46
Medicare Newsletter – June 6, 2011 DRG 470: Joint Replacement or Reattachment of Lower Extremity (con’t.) An x-ray must be obtained and must have at least two of the following findings: Subchondral cysts Subchondral sclerosis Periarticular osteophytes Joint subluxation Joint space narrowing Documentation must indicate continued symptoms after a trail of medication (i.e. NSAIDs) or the contraindication of medication due to the patient’s inability to tolerate. Documentation of physical therapy or external joint support 12 weeks or greater.
 or the contraindication of medication due to the patient’s inability to tolerate. Documentation of physical therapy or external joint support 12 weeks or greater..")
47
Billing for Part B Services After Part A Services are Denied Old Rule See the Medicare Benefit Policy Manual, Chapter 6, Hospital Services Covered Under Part B, Section 10. Interim Rule http://www.ofr.gov/(S(2yzxk55mcriryqcephbfo5gx))/OFRUpload/ OFRData/2013-06159_PI.pdf Proposed Rule https://www.federalregister.gov/articles/2013/03/18/2013- 06163/medicare-program-part-b-inpatient-billing-in-hospitals

48
Old Rule Hospitals could only receive reimbursement for “a limited set of largely ancillary inpatient services under Part B.” * These claims are considered “new claims subject to timely filing guidelines.” *Described in detail in the Medicare Benefit Policy Manual, Chapter 6, Hospital Services Covered Under Part B, Section 10.

49
Interim Rule CMS Ruling No.: CMS-1455-R Addresses CMS policy on Part B billing following the denial of a Part A inpatient hospital claim on the basis that the inpatient admission was determined not reasonable and necessary Effective March 13, 2013 Permits submission of a Part B claim for payment for payable services had the beneficiary been treated as an outpatient with no timely filing restrictions Exception: those services that require outpatient status, i.e. ED visits, office visits, observation services

50
Proposed Final Rule Published in the Federal Register on 3/18/13 Permits submission of a Part B claim for payment for payable services had the beneficiary been treated as an outpatient with a timely filing restriction Part B claim must be billed within one year of the DOS! ALJs/MACs in the future will not be permitted to issue a partially favorable decision and allow payment for Part B services

51
Recommendations of W&W Interim Rule Proposed Final Rule Continue to Appeal claims that you have billed appropriately. Review proposed rule to determine how it will affect your facility specifically Timely filing requirement Submit comments to CMS no later than 5 pm on 5/17/13!

52
In Summary…. 1. Emphasis on Denial Prevention 2. Education, Education, Education! 3. Follow Medicare, Medicaid & Managed Care/Commercial Rules 4. Collect accurate and meaningful data 5. Best Practice Appeal for all wrongfully denied cases 6. Contract Review for fair & appropriate terms 7. Ability & willingness to act on your data – Feedback & Enforcement to ensure that Physicians & Departments know & follow payer criteria & documentation requirements!!!

53
Linda Fotheringill, Esq. Washington & West, LLC One Olympic Place Suite 500 Baltimore, Maryland 21204 1- 800 -704 – 5574 www.washingtonwest.com l.fotheringill@washingtonwest.com Questions?

54
Copyright 2013 by Washington & West, LLC. All rights reserved. Washington & West, LLC is not a law firm. The information conveyed in this presentation is for general educational purposes and is not legal advice. The application and impact of laws can vary widely, based on the specific facts involved. Given the constantly changing nature of state and federal laws, there may be omissions or inaccuracies in the information you receive during this program. Accordingly, any information is provided with the understanding that the presenter is not rendering legal, accounting, or other professional advice and services. As such, any information obtained in this presentation should not be used as a substitute for consultation with legal counsel or other professional advisors specifically retained for that purpose. While Washington & West, LLC has made every attempt to ensure that the information contained in these materials is generally useful for educational purposes, Washington & West, LLC, RAC University and its agents & employees are not responsible for any errors or omissions or for the results obtained through the use of any information herein. Please Take Note!

Similar presentations




 May 6, 2014 John Rogers Manager, Eligibility Services>")

















