Download presentation
Presentation is loading. Please wait.

1
Immunisation Against Human Papilloma Virus David Green – Immunisation Co- ordinator and Infection Control Nurse

2
Contents Epidemiology and pathology of infection Conditions caused by HPV HPV Vaccine Consent The DH immunisation campaign Results Future challenges

3
Brain Teaser What is the connection between this moth and the HPV vaccine? Cabbage looper or Trichoplusia ni

4
HPV infection Human papilloma virus (HPV) is a small DNA virus. It infects the deeper layers of the skin and internal lining of organs such as the vagina and mouth. HPV is often asymptomatic. There are more than 100 types, of which 40 infect the genital area. HPV infections normally resolve spontaneously - 90% do so within two years. Persistent HPV infection causes the cell changes that eventually lead to cancer.

5
HPV Transmission HPV is spread by direct physical contact Any genital contact is important, not just sexual intercourse. Hand to genital contact may cause some infections. Anyone who is sexually active is at risk. The risk of acquiring HPV increases with the number of sexual partners.

6
Epidemiology of genital HPV infection HPV infection is common – at least half of all sexually active women will be infected by a strain of genital HPV strain in their lifetimes. The rate of genital HPV infection increases from age 14. Women are most likely to be infected in their late teens and early twenties. 15% of 20 to 24-year-old women were recently infected with HPV 16 or 18.

7
Effects of HPV infection The HPV virus infects cells and then integrates its DNA in to the DNA of the host cell. Persistent infection leads to cells becoming damaged and abnormal. Eventually cancer - abnormal uncontrolled growth of tissues – occurs after many years. HPV infections can’t be treated but abnormal changes can be detected by screening and removed.

8
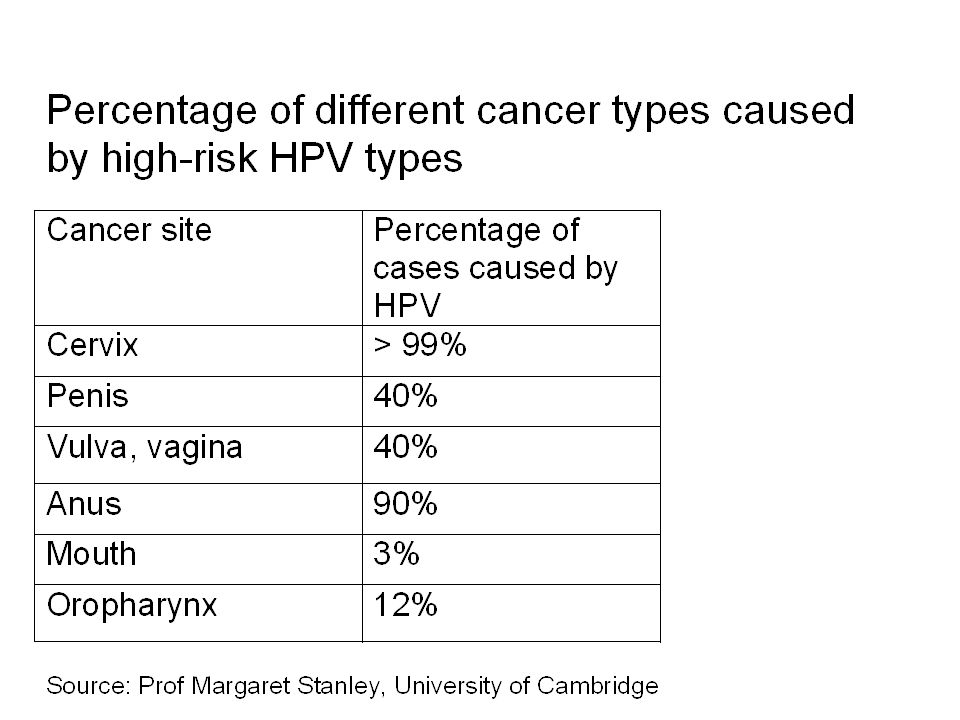
Categories of genital HPV infection Genital HPV types are categorised as either: –high-risk (oncogenic) types - that cause cervical intraepithelial neoplasia and invasive cancer, and –low-risk types - that cause genital warts. 99% of all cervical cancer cases are caused by HPV infection. Two high-risk types, HPV 16 and 18, cause over 70% of cervical cancers. Other HPV types can also cause cervical cancer.

9
HPV types that cause cervical cancer HPV type Percentage of cervical cancer cases caused by HPV type Cumulative percentage 1658.1% 1815.7%73.8% 334.4%78.2% 314.0%82.2% 452.9%85.1% 351.6%86.7% 581.2%87.9% 561.0%88.9% 520.6%89.5% 390.2%89.7% 510.2%89.9% 680.3%90.2% 590.1%90.3% Other1.4%91.7% No type identified8.3%100% Adapted from Smith JS et al., 2007; Int J Cancer. 121(3):621-32.
:")
11
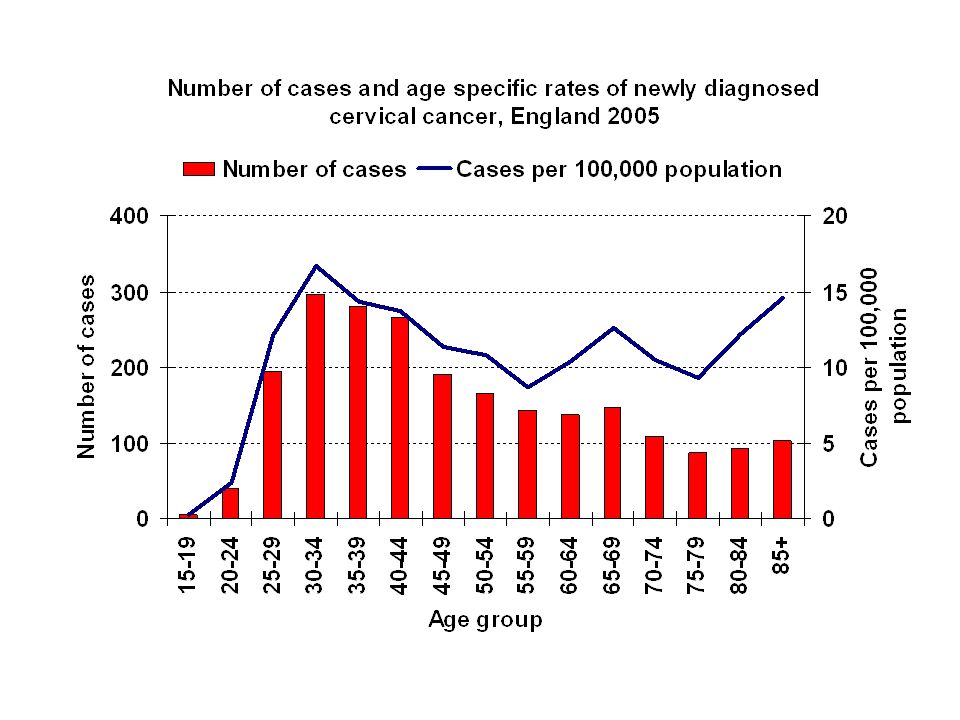
Epidemiology of cervical cancer 2253 cases of invasive cervical cancer were diagnosed in England in 2005. It is the second most common cancer of women worldwide. Most cases occur in women in their late 30s or in their 70s/80s (latter group were not screened when younger). In developed countries, most cases are prevented by cervical screening. In the UK, death rates are about 60% lower than 30 years ago, mainly due to screening.
. In developed countries, most cases are prevented by cervical screening. In the UK, death rates are about 60% lower than 30 years ago, mainly due to screening..")
13
HPV Immunisation

14
Cervarix Cervarix® is a bivalent vaccine manufactured by GlaxoSmithKline. Cervarix® protects against HPV types 16 and 18. Cervarix® was chosen after assessment of the two available vaccines against a wide range of criteria, such as the scientific data on vaccine effectiveness and cost- effectiveness Costs approx £80 per dose

15
Cervarix Controversy The competitor brand (Gardasil) protects against strains 6, 11, 16 and 18. Use of Cervarix rather than Gardasil has been called “short sighted” (Terrence Higgins Trust) and a “missed opportunity” (FPA). Prevention of cervical cancer is the primary purpose of the HPV vaccination programme.
 and a missed opportunity (FPA). Prevention of cervical cancer is the primary purpose of the HPV vaccination programme..")
16
The nature of Cervarix vaccine Proteins that coat the HPV virus are made using DNA recombinant technology in cells that have been infected by baculoviruses (insect viruses) which uses cells derived from Trichoplusia ni. These purified proteins assemble themselves into small spheres called virus-like particles (VLPs). VLPs cannot cause HPV infection or cancer. The VLPs produce immunity to HPV. Immunised individuals mount a rapid immune response when subsequently exposed to HPV.
. VLPs cannot cause HPV infection or cancer. The VLPs produce immunity to HPV. Immunised individuals mount a rapid immune response when subsequently exposed to HPV..")
17
Duration of immunity The immune response to HPV vaccination lasts at least six years (the current maximum length of post-vaccination follow-up). For at least five years post-vaccination, antibody levels have been shown to be higher from vaccination than from natural infection. At present there is no evidence for waning immunity, but important long-term follow-up studies are taking place to establish whether boosting will be necessary. Routine HPV vaccination will save the lives of around 400 women each year.

18
Consent Consent is being asked for a course of treatment (all three doses) For year 8 girls (aged 12 and 13) the person with parental responsibility gives consent Year 13 (aged 17 and 18) girls give their own consent
 For year 8 girls (aged 12 and 13) the person with parental responsibility gives consent Year 13 (aged 17 and 18) girls give their own consent")
19
Vaccine schedule and administration Schedule for Cervarix ® : –first dose of 0.5ml HPV vaccine; –second dose of 0.5ml, at least one to two months after the first; and –a third dose of 0.5ml, at least six months after the first. HPV vaccination is normally given by the usual route, in the upper arm by IM injection

20
HPV Immunisation Program

21
Vaccination of boys and young women 18 and over The benefits of HPV vaccination are less for boys and JCVI has advised that vaccination of boys is not cost-effective. The vaccination of girls will reduce HPV infections in boys by a herd immunity effect. The DH are not currently planning to offer vaccine to those aged 18 and over as part of a national programme All young women will still be covered by the cervical screening programme and should still be actively promoted by HCWs.

22
The HPV routine and catch-up vaccination schedule for girls and young women in England, as of September 2008 School year 7 School year 8 School year 9 School year 10 School year 11 School year 12 Girls aged 17- 18 (school year 13) 2008/09 2009/10 2010/11 2011/12 Routine programme for Year 8 girls Catch-up programme for older girls
 2008/ / / /12 Routine programme for Year 8 girls Catch-up programme for older girls")
23
Implementation in Calderdale PCT A schools-based programme was used for those in school as it was likely that: –vaccine coverage will be higher in schools –costs would be lower than a GP-delivered model, and –using schools would be more acceptable to parents/pupils. –Opt out of school program available if necessary Offering vaccination in the summer term is problematic, so an early start in the school year was thought necessary.

24
Implementation in Calderdale Schools Dose one - Sept 08 (plus mop ups) Dose two – Nov 08 (plus mop ups) Dose three – March 09 (plus mop up) Those who miss mop up could attend their GP practice to receive outstanding dose(s)
 Dose two – Nov 08 (plus mop ups) Dose three – March 09 (plus mop up) Those who miss mop up could attend their GP practice to receive outstanding dose(s)")
25
Regional and National Comparison (Jan 09) DoseCalderdaleY&H Region (Average) England (Average) One (Yr 8)92%90%82% One (Yr 13)46%32% Two (Yr 8)89%78%73% Two (Yr 13)37%15%21%
 DoseCalderdaleY&H Region (Average) England (Average) One (Yr 8)92%90%82% One (Yr 13)46%32% Two (Yr 8)89%78%73% Two (Yr 13)37%15%21%")
26
Uptake in Calderdale (as of 31.3.09) Year 8 (12 and 13 years old) = Dose 1 = 94.4% Dose 2 = 91.6% Dose 3 = 81.5% Year 13 (17 and 18 year olds) = Dose 1 = 56.9% Dose 2 = 43.6% Dose 3 = 27.7%
 Year 8 (12 and 13 years old) = Dose 1 = 94.4% Dose 2 = 91.6% Dose 3 = 81.5% Year 13 (17 and 18 year olds) = Dose 1 = 56.9% Dose 2 = 43.6% Dose 3 = 27.7%")
27
Future challenges Year 8 - To bring uptake of doses 2 and 3 up to dose 1 level Year 13 – To achieve 90% uptake! To implement the new “accelerated” HPV immunisation campaign from Sept 09.

28
The Accelerated HPV Campaign School year 7 School year 8 School year 9 School year 10 School year 11 School year 12 Girls aged 17- 18 (school year 13) 2008/09 2009/10 2010/11 2011/12
 2008/ / / /12")
29
Questions?

Similar presentations


















>")
