Download presentation
Presentation is loading. Please wait.

1
National Center for Health Statistics DCC CENTERS FOR DISEASE CONTROL AND PREVENTION NAMCS/NHAMCS WORKSHOP Catharine W. Burt Susan M. Schappert Nghi Ly Division of Health Care Statistics

2
I. Introduction Learn how to use NAMCS and NHAMCS public use microdata for analyzing ambulatory care utilization

3
Workshop objectives Describe major survey variables Determine if an estimate is reliable Identify some cautions when using the data List ways of obtaining the data Use SETS Navigate our website Calculate sampling variance Manipulate visit files to get drug files

4
Workshop agenda 8:30 I. Introduction 8:50 II. Some technical considerations 9:10 III. Using SETS 9:30 IV. Navigating our website 10:10 * * Break * * 10:30 V. Using raw data files 11:15 VI. Advanced topics 12:00 VII. Summary & Adjourn

5
Overview Ambulatory care encounter data Physician offices Hospital outpatient departments Hospital emergency departments SEs rates percents drugs providers visits sample records

6
How are NAMCS/NHAMCS data used? To understand health care practice and find inequities To identify and track problems To decide what programs get funded To establish national priorities To serve as comparison points for states To measure Healthy People objectives

8
Data users Over 100 journal publications in last 2 years Medical associations Government agencies Health services researchers University and medical schools Broadcast & print media

9
Recent media headlines “Fewer Antibiotics Are Prescribed to Children”… Washington Post, June 19, 2002 “Picture of Health as America Ages” … New York Times, June 18, 2002 “ Doctors prescribing more medications” ….Washington Post, July 10, 2001

10
Vocabulary Patient record form (PRF) Induction interview form Provider-visit-patient-drug characteristics Drug mentions Reason for visit Classification (RVC) ICD-9-CM First-listed vs. Any-listed Sampling error Non-sampling error

11
POP QUIZ!! Multiple choice NAMCS/NHAMCS encounter data can be used to a. Make disease prevalence estimates b. Determine cost-effectiveness of treatment c. Estimate the most frequent medications prescribed for various diseases. d. Compare utilization rates across states

12
Section II – Some Technical Considerations with NAMCS and NHAMCS Data Section III – Using SETS Section IV – Navigating Our Website

13
Some NAMCS Considerations NAMCS samples physicians and their visits, not patients or ambulatory care settings We can’t make estimates of incidence, prevalence, state-level estimates, volume of visits to providers who are not office-based physicians, volume of visits to each type of in- scope location We may only sample one physician from a group practice May not capture same types of visits to solo practitioners and group practices

14
Items Collected Patient characteristics - age, sex, race Visit characteristics Source of payment, continuity of care, reason for visit, diagnosis, treatment Provider characteristics Physician specialty, hospital ownership Drug characteristics – class, composition, control status, ingredients, Rx or OTC

15
A few words about item validity Counseling items from NAMCS and OPD are often used as analytic variables in research papers Medical records are accurate in reflecting diagnostic services, but not health habit counseling (Stange et al. 1998) Our surveys may be underestimating counseling services especially where data are abstracted
 Our surveys may be underestimating counseling services especially where data are abstracted.")
16
Sample Weight Each NAMCS record contains a single weight, which we call Patient Visit Weight Same is true for OPD records and ED records This weight is used for both visits and drug mentions

17
Reliability Criteria Estimate must be based on at least 30 sample records For estimates based on at least 30 records, relative standard error may not exceed 30 percent

18
How Good are the Estimates? Depends on what you are looking at. In general, OPD estimates tend to be somewhat less reliable than NAMCS and ED. This may change with 2001 sampling improvements. 1999 and 2000 reports for NAMCS, OPD, and ED include standard errors in every table so it is easy to compute confidence intervals around the estimates.

19
Reliability of Estimates in NAMCS Estimate of office visits by white persons was 710.8 million in 2000, with a relative standard error of 4 percent – range of 649-773 million visits Estimate of office visits by black persons was 76 million in 2000 with a relative standard error of 9 percent – range of 63-89 million visits

20
Reliability of Estimates in NHAMCS OPD = 9% and 10% RSE for visits by white persons vs. visits by black persons ED = 5% and 7% RSE for visits by white persons vs. visits by black persons A higher RSE means that an estimate has a wider confidence interval and is less reliable.

21
Calculating Variance with NAMCS/NHAMCS Estimates In the past, data users calculated standard errors with curve coefficients from generalized variance curves produced by NCHS. Sample design variables are needed to compute most precise variances, but these are restricted to the public because of confidentiality issues. We now have masked design variables on public use files from 1997-2000. Allows users to run SUDAAN and similar software to do more sophisticated analysis!

22
Examples of RSEs based on GVC, SUDAAN (true), SUDAAN (masked) Visits by Age GVC SUD– T SUD-M All ages 5.54.24.5 <15 6.06.97.2 15-246.56.56.2 25-445.85.45.5 45-645.84.85.0 65-746.25.25.6 75+6.25.75.5
, SUDAAN (masked) Visits by Age GVC SUD– T SUD-M All ages <")
23
Comparison of RSEs Produced Using GVC, SUDAAN-T, and SUDAAN-M

24
Comparisons of RSEs for Patient Race Variances for clustered items (like race, diagnosis, type of provider) are predicted less accurately using the GVC. If you use the GVC, use p =.01, not.05

25
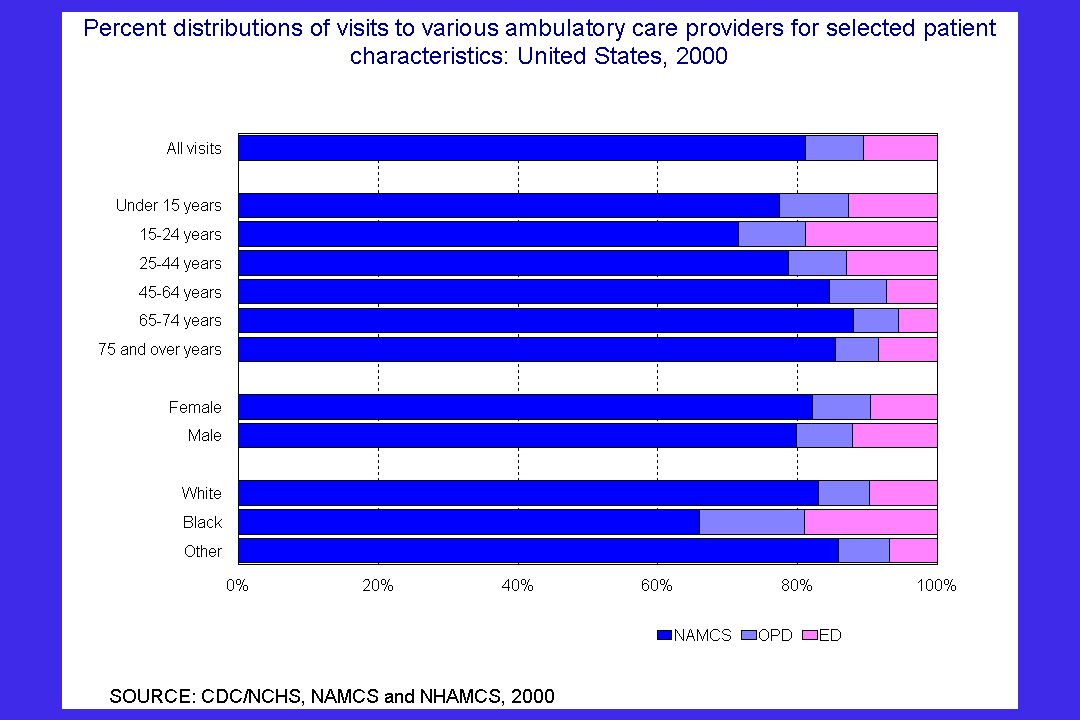
NAMCS vs. NHAMCS Consider what types of settings are best for a particular analysis Persons of color are more likely to visit OPD’s and ED’s than physician offices Persons in some age groups make disproportionately larger shares of visits to ED’s than offices and OPDs

26
When Combining NAMCS and NHAMCS Data… You can use the SUBFILE and DEPT variables to identify the ambulatory care setting In SAS… if subfile = 1 then settype = 1; else if subfile = 2 and dept = 2 then settype = 2; else if subfile = 2 and dept = 1 then settype = 3;

28
Using raw data files File structure Transforming data Creating new variables Making a drug file Using sample design variables

29
Ambulatory Care Data Structure

30
File Structure Flat ASCII files for each setting and year Use file layout to read the data Download data and layout from website http://www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm

31
Visit File Layout Patient information Sex, age, race, ethnicity Visit information Reason for visit, diagnosis Expected source of payment, referral status Diagnostic services Therapeutic services – Counseling/education – Medication therapy (drug name, generic name, ingredients, therapeutic class, etc.)
")
32
Visit File Layout Outcome measures Visit disposition (no followup planned, return, refer, admit to hospital) Provider information Specialty, region, urban, solo practice, ownership Sample design variables Stratum, psum, subfile, prostrat…etc.
 Provider information Specialty, region, urban, solo practice, ownership Sample design variables Stratum, psum, subfile, prostrat…etc.")
33
File reading exercises SAS exercises: A-E Open SAS

34
Advanced topics Calculate sampling variance Creating measures Combining multiple files Multiple years for greater reliability Multiple years for analyzing trends Multiple settings

35
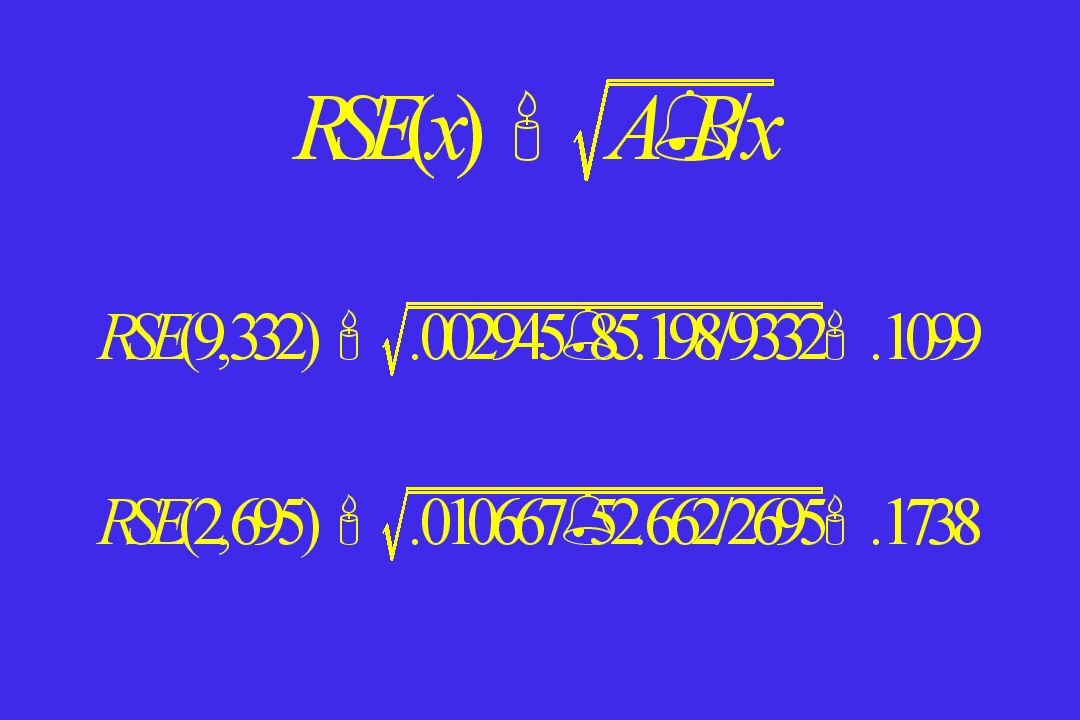
Calculate RSE’s for estimates of interest Using the variance curve to calculate RSE’s RSE(x)= A + B/x Refer to blue book for A & B coefficients x is the estimate of interest Calculate the standard error from the RSE SE(x) = x * RSE Examples: Calculate the RSE for the number of office visits for asthma. Calculate the RSE for the number of asthma visits to pediatricians.

37
Estimating Variance You can use the generalized variance curve. We have variance curves for some 2-year combinations. This is the least accurate method. You can use public-use files with masked sample design variables to obtain more accurate variances using SUDAAN or other software. You can use restricted files at the NCHS Research Data Center.

38
Creating measures Drug utilization rate = drug mentions/pop’n Drug mention = health care provider’s entry of a pharmaceutical agent on the PRF Drug visit rate = drug visits/pop’n Drug visits=visit where a drug was provided or prescribed Drug mention rate = drug mentions/visit

39
Combining multiple files Multiple year combinations are best for subpopulation analysis Multiple year combinations for disease specific analysis Keep adding years until you have at least 30 raw cases in important cells. RSE improves incrementally with the number of years combined.

40
RSE improves incrementally with the number of years combined If SE=RSE*x then RSE = SE/x Example: Calculate the RSE for the percent of visits with diabetes by persons less than 21 years of age 1998 RSE =.08/.18 =.44 (44%) 1998 and 1999 RSE =.06/.18 =.33 (33%) 1998, 1999, and 2000 RSE =.05/.21 =.24 (24%)
 1998 and 1999 RSE =.06/.18 =.33 (33%) 1998, 1999, and 2000 RSE =.05/.21 =.24 (24%)")
41
Trend analysis – for NAMCS 1973 NAMCS began 1974 used 1973 PRF, data not released 1975-76 increased dx/rx checkboxes 1977-78 added referral, time since onset; separated and expanded dx/rx items 1979 added prior-visit status, 5 injury/product-related illness items 1980-81 medication item added, dropped injury/product related illness items

42
Trend analysis – for NAMCS 1985 source of payment added 1989-90 separated and expanded rx services 1995-96 cause of injury, surgical procedures 1997-98 providers seen, major reason for visit, managed care items added; disposition off 1999-00 disposition back

43
Trend analysis for NHAMCS (ED) 1992 NHAMCS began 1993-94 dropped major reason for visit (injury or illness initial or follow-up) 1995-96 time of visit, injury items added 1997-98 mode of arrival, pain level, immediacy, time seen by physician added, urgency dropped 1999-2000 no changes
 1992 NHAMCS began dropped major reason for visit (injury or illness initial or follow-up) time of visit, injury items added mode of arrival, pain level, immediacy, time seen by physician added, urgency dropped no changes")
44
Trend continued …. Be careful about trending diagnosis prior to 1980 because of ICDA (based on ICD-8) Even after 1980- be careful about changes in ICD-9-CM Number of medications varies over years 1980-81 – 8 medications 1985, 1989-94 – 5 medications 1995-2000 – 6 medications Diagnostic & therapeutic checkboxes vary Use spreadsheet for significance of trends
 Even after be careful about changes in ICD-9-CM Number of medications varies over years – 8 medications 1985, – 5 medications – 6 medications Diagnostic & therapeutic checkboxes vary Use spreadsheet for significance of trends.")
45
Multiple settings NAMCS, ED, and OPD can be combined in one or multiple years. Be sure to use variables that indicate survey type (NAMCS, ED or OPD) and year. OPD and NAMCS should be combined to get estimates of ambulatory physician care especially for African-American, Medicaid or adolescent subpopulations. Only NAMCS has physician specialty.
 and year. OPD and NAMCS should be combined to get estimates of ambulatory physician care especially for African-American, Medicaid or adolescent subpopulations. Only NAMCS has physician specialty..")
46
Summary How to use NAMCS/NHAMCS data files for analyzing ambulatory care utilization Use SAS to analyze data Familiarity of sample design variables to get SE’s for estimates Calculate RSE using the variance curve Create measures (ex. Rates) Combine multiple files for reliability or trends SPSS syntax for SAS exercises (handout) Questions and Answers
 Combine multiple files for reliability or trends SPSS syntax for SAS exercises (handout) Questions and Answers.")
47
Where to Get More Information www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm Call Ambulatory Care Statistics Branch at 301-458-4600

Similar presentations







 data Session 25 July 13, 2004 10:30-noon.>")

 to the National Hospital Medical Care Survey (NHAMCS) Centers for Disease.>")
 and National Hospital Ambulatory Medical Care Survey (NHAMCS) data for clinical.>")









