Download presentation
Presentation is loading. Please wait.

1
Antibacterials Review
November 6, 2009

2
Cell-wall active agents
Penicillins Narrow spectrum: penicillinase susceptible penicillinase resistant Broader spectrum Cephalosporins Narrow spectrum (1° generation) Broader spectrum (2-4° generations) Carbapenems Aztreonam Vancomycin
 Broader spectrum (2-4° generations) Carbapenems. Aztreonam. Vancomycin.")
3
Penicillins All derived from 6-aminopenicillanic acid and have b-lactam ring Vary in resistance to stomach acid, polar, not metabolized easily usually excreted unchanged in urine both via glomerular filtration and tubular secretion (latter is inhibited by Probenicid) Ampicillin and nafcillin also excreted in bile Procaine/benzathine forms of penicillin G injected i.m. to give long half-life, otherwise plasma half life is short (30-60 min) Most only cross blood brain barrier when meninges are inflamed.
 Ampicillin and nafcillin also excreted in bile. Procaine/benzathine forms of penicillin G injected i.m. to give long half-life, otherwise plasma half life is short (30-60 min) Most only cross blood brain barrier when meninges are inflamed.")
4
Penicillins Bactericidal Targets (peptidoglycan synthesis)
Penicillin binding proteins (PBPs) Transpeptidase Activate some autolytic enzymes Resistance usually due to b-lactamases (esp. Staph and many Gram-negatives) Resistance also known via changing PBPs (methicillin-resistance in Staph (PenG resistance in pneumococcus) Porins mutations in Pseudomonas may allow resistance
 Transpeptidase. Activate some autolytic enzymes. Resistance usually due to b-lactamases. (esp. Staph and many Gram-negatives) Resistance also known via changing PBPs. (methicillin-resistance in Staph. (PenG resistance in pneumococcus) Porins mutations in Pseudomonas may allow resistance.")
5
Clinical use of penicillins
Narrow spectrum, penicillinase-susceptible drugs penicillin G (parenteral – unstable in stomach acid) penicillin V (given orally) Used for streptococci, meningococcus, Gram-positive bacilli (Bacillus), Spirochetes (Treponema) Resistance reported for most Staph aureus, many Neisseria gonorrhoeae many Strep pneumoniae
 penicillin V (given orally) Used for streptococci, meningococcus, Gram-positive bacilli (Bacillus), Spirochetes (Treponema) Resistance reported for. most Staph aureus, many Neisseria gonorrhoeae. many Strep pneumoniae.")
6
Clinical use of penicillins (cont.)
Very narrow spectrum, penicillinase-resistant agents (methicillin) nafcillin oxacillin Primarily used for infections by Staph. aureus and Staph. epidermidis Resistance seen with MRSA and with some organisms making ESBLs
 nafcillin. oxacillin. Primarily used for infections by Staph. aureus and Staph. epidermidis. Resistance seen with MRSA and with some organisms making ESBLs.")
7
Clinical use of penicillins (cont.)
Broader spectrum, penicillinase-susceptible agents Ampicillin and amoxicillin Used for PenG susceptible agents and for enterococci, Listeria, E. coli, Proteus, Haemophilus influenzae, Moraxella catarrhalis Used in combination with penicillinase inhibitors (e.g. clavulanic acid) Synergy shown with aminoglycosides for Listeria and enterococci
 Synergy shown with aminoglycosides for Listeria and enterococci.")
8
Clinical use of penicillins (cont.)
Broader spectrum, penicillinase-susceptible agents (cont.) Piperacillin and ticarcillin Active against several Gram-negative rods Pseudomonas, Enterobacter, some Klebsiella Synergistic with main glycosides Often used with penicillinase inhibitors
 Piperacillin and ticarcillin. Active against several Gram-negative rods. Pseudomonas, Enterobacter, some Klebsiella. Synergistic with main glycosides. Often used with penicillinase inhibitors.")
9
Toxicity of penicillins
Nausea, diarrhea are fairly common, especially with oral penicillins Allergy (including anaphylaxis or induction of Type II and III reactions). Persons with allergy may be desensitized if necessary using a ~3-4 h rapid desensitization protocol Methicillin may cause nephritis Nafcillin may cause neutropenia Ampicillin often causes a maculopapular rash. This can be very pronounced if ampicillin is given to someone with mononucleosis (EBV) when this reaction is almost diagnostic for infective mononucleosis.
. Persons with allergy may be desensitized if necessary using a ~3-4 h rapid desensitization protocol. Methicillin may cause nephritis. Nafcillin may cause neutropenia. Ampicillin often causes a maculopapular rash. This can be very pronounced if ampicillin is given to someone with mononucleosis (EBV) when this reaction is almost diagnostic for infective mononucleosis.")
10
Cephalosporins Most administered parenterally
Many partly metabolized by liver but still usually excreted in urine (like penicillins) But cefoperazone & ceftriaxone (mainly via bile) Most 1° and 2 ° generation do not enter CSF (even if meninges inflamed) Targets same as penicillins – i.e, bactericidal drugs Tendency to be more resistant than penicillins to b-lactamases, but not to all. Note: MRSA is resistant to cephalosporins
 But cefoperazone & ceftriaxone (mainly via bile) Most 1° and 2 ° generation do not enter CSF (even if meninges inflamed) Targets same as penicillins – i.e, bactericidal drugs. Tendency to be more resistant than penicillins to b-lactamases, but not to all. Note: MRSA is resistant to cephalosporins.")
11
1st generation cephalosporins
Cefazolin (parenteral) and cephalexin (oral) Used for Gram-positive cocci Many E. coli and Klebsiella pneumoniae NOT for Gram-neg cocci enterococci MRSA, most Gram-neg rods
 and cephalexin (oral) Used for Gram-positive cocci. Many E. coli and Klebsiella pneumoniae. NOT for. Gram-neg cocci. enterococci. MRSA, most Gram-neg rods.")
12
Second generation cephalosporins
Extended coverage of Gram-negatives Less coverage of Gram-positives Diverse activity shown by different members Cefotetan, cefotoxin (Bacteroides fragilis - anaerobe) often resistant to ESBLs Cefomandole, cefuroxime, cefaclor (H. influenzae. M. cattharalis)
 often resistant to ESBLs. Cefomandole, cefuroxime, cefaclor. (H. influenzae. M. cattharalis)")
13
Third generation cephalosporins
Extended coverage of Gram-negatives Enter CSF (except cefoperazone and cefiximine) Resistance associated with extended spectrum beta-lactamases (ESBLs in Klebsiella and E. coli especially) Active against several Gram-neg including Neisseria ceftriaxone parenteral and cefiximine oral for gonococcus) cefoperazone & ceftazidime active against Pseudomonas One injection of ceftriaxone (~ 8h half life) usually effective for acute otitis media
 Resistance associated with extended spectrum beta-lactamases (ESBLs in Klebsiella and E. coli especially) Active against several Gram-neg including Neisseria. ceftriaxone parenteral and cefiximine oral for gonococcus) cefoperazone & ceftazidime active against Pseudomonas. One injection of ceftriaxone (~ 8h half life) usually effective for acute otitis media.")
14
Fourth generation cephalosporins
Cefepime Expands coverage of 3rd generation to include activity against Gram+ found in 1st generation cephalosporins Used for penicillin-resistant pneumococci and for several b-lactamase producing Gram-negatives including Enterobacter

15
Cephalosporins - Toxicity
Allergy (cross-reactivity within cephalosporins as group) Some cross-reaction with penicillins Pain at injection site Phlebitis after i.v. administration May increase nephrotoxicity of aminoglycosides Disulfuram reaction with some (e.g. cefoperaxzone, cefotetan, cefamandole)
 Some cross-reaction with penicillins. Pain at injection site. Phlebitis after i.v. administration. May increase nephrotoxicity of aminoglycosides. Disulfuram reaction with some (e.g. cefoperaxzone, cefotetan, cefamandole)")
16
Other b-lactams Aztreonam (a monobactam. Acts on PBP3)
No activity on Gram-positive bacteria or anaerobes Resistant to b-lactamases produced by many Gram-negative rods including Klebsiella and Pseudomonas but not resistant to ESBLs. Synergistic with aminoglycosides Prolonged half-life in renal failure No significant cross-allerginicity with penicillin

17
Other b-lactams Imipenem, meropenem (carbapenems)
Wide activity against Gram positive cocci, Gram-negative rods, and anaerobes Used with aminoglycoside for Pseudomonas infection Resistant to ESBLs Imipenem is administered with cilastin to prevent inactivation by renal dehydropeptidase CNS toxicity at high concn

18
Vancomycin Bactericidal glycoprotein inhibiting cell wall formation
Binds D-Ala-D-Ala pentapeptide side chain to prevent transpeptidation in growing peptidoglycan Resistance in VRE and VRSA is due to change of one D-ala to D-lactate Narrow spectrum of use Mainly for MRSA, penicillin-resistant pneumococcus and C. difficile Eliminated unchanged in urine. Not absorbed from gut so only used orally for C. difficile Nephrotoxic, ototoxic, RED MAN syndrome with rapid infusion

19
Tetracyclines: Mode of Action
Reversible binding to 30S ribosome subunit blocking aminoacyl-tRNA access to acceptor site (A site) X
 X.")
20
Tetracyclines Drugs usually given orally and absorbed from small intestine BUT Interference of uptake by food, divalent and trivalent cations (Ca++, Mg++, Fe++, Bi +++, Al+++ ) in antacids, dairy products. Active against many Gram + and Gram – bacteria including anaerobes, rickettsiae, chlamydiae, mycoplasmae. Tigecycline has wider range. Must be given i.v. MRSA included, but NOT Pseudomonas nor Proteus Some tetracyclines act against protozoa and those filarial nematodes that have endosymbiotic bacteria (e.g. doxycyline: Entamoeba and Plasmodium falciparum)
 in antacids, dairy products. Active against many Gram + and Gram – bacteria including anaerobes, rickettsiae, chlamydiae, mycoplasmae. Tigecycline has wider range. Must be given i.v. MRSA included, but NOT Pseudomonas nor Proteus. Some tetracyclines act against protozoa and those filarial nematodes that have endosymbiotic bacteria. (e.g. doxycyline: Entamoeba and Plasmodium falciparum)")
21
Tetracyclines Enter all body fluids well except CSF
(~10-20% plasma level) Actively excreted in bile and into feces some enterohepatic circulation Also excreted in urine But NOT doxycycline nor tigecycline
 Actively excreted in bile and into feces. some enterohepatic circulation. Also excreted in urine. But NOT doxycycline nor tigecycline.")
22
Tetracyclines toxicity
Allergies Minor effects on liver Vestibular toxicity Occasional photosensitivity Kidney excretion means doses need to be watched in renal failure Special effect on growing bones Enter breast milk and cross placenta Chelation with calcium causes binding to growing bones/teeth - damage

23
Tigecycline (Tygacil)
Became available 2005 Has very broad spectrum of activity including MRSA, VRSA, VISA, and coagulase-neg Staph Penicillin resistant and susceptible streptococci Enterococci (including VRE) Gram-positive rods Enterobacteriaceae Acinetobacter (multidrug resistant) Anaerobes (Gram + and -) Chlamydiae, rickettsiae, Legionella, fast growing mycobacteria NOT effective against Pseudomonas or Proteus where the efflux pump is effective at removing it thereby causing intrinsic resistance.
 Gram-positive rods. Enterobacteriaceae. Acinetobacter (multidrug resistant) Anaerobes (Gram + and -) Chlamydiae, rickettsiae, Legionella, fast growing mycobacteria. NOT effective against Pseudomonas or Proteus where the efflux pump is effective at removing it thereby causing intrinsic resistance.")
24
Macrolides – block transpeptidylation

25
Macrolides Erythromycin, azithromycin, clarithromycin
Oral bioavailability Active against Campylobacter, Mycoplasma, Legionella, Gram-pos cocci, some Gram-negs Erythromycin widely used for community acquired pneumonia

26
Macrolides Azithromycin Clarithromycin
Concn in tissues and phagocytes higher than plasma. Slow release allows once a week dosing (half life 2-4 days). Especially useful for chlamydial infections Clarithromycin Used for Mycobacterium avium
. Especially useful for chlamydial infections. Clarithromycin. Used for Mycobacterium avium.")
27
Aminoglycosides Broad spectrum Gentamicin Amikacin Tobramycin
Netilmicin Those with limited clinical application Streptomycin Neomycin Kanamycin Do not work alone on serious infections by enterococci or streptococci but can increase antimicrobial activity of other drugs when used in combination for these infections

28
Mistranslation – one effect of aminoglycosides
Gentamicin in major groove of RNA at site where aa-tRNA interacts with mRNA. Distortion of ribosomal site by antibiotic causes misreading of codons. Interaction is within the 30S subunit puglisi.stanford.edu/research.html

29
Aminoglycosides Highly charged (polycations) and poor lipid solubility
Do not penetrate human cell cytoplasm well. Generally given by i.v. or i.m. injection. Mainly excreted in urine Action independent of microbial concentration so very useful for intrabdominal infections Persistent suppression of microbial growth after dropping to non-lethal level (post antibiotic effect) High dose once a day is more effective and less toxic than same amount split and administered in 3 doses per day Toxicity largely depends on time the drug remains above a toxic concentration
 High dose once a day is more effective and less toxic than same amount split and administered in 3 doses per day. Toxicity largely depends on time the drug remains above a toxic concentration.")
30
Aminoglycosides - Toxicity
Neuromuscular blockade binding calcium in presynaptic region – reversible with calcium gluconate Nephrotoxicity interference with tubular function including excess loss of Mg and Ca: increased toxicity in combination with vancomycin, amphotericin B, diuretics, several others. Generally reversible Ototoxicity (auditory and vestibular) non-reversible
 non-reversible.")
31
Novel uses in the works for aminoglycosides
Treatment of genetic disease in humans when caused by premature stop codon in gene.

32
Spectinomycin Similar structure to aminoglycosides
Target is on 30S ribosome Used to treat penicillin-resistant Neisseria gonorrhoeae

33
Others (all act on 50S subunit)
Chloramphenicol Wide spectrum of activity. Significant toxicities. Inactivated by liver (liver action has low activity in newborn) Aplastic anemia (gray baby syndrome) Restricted uses (e.g. serious rickettsial infections) Clindamycin (a lincomycin) MLSB resistance known Works like macrolides Bacteroides, several anaerobes Increased danger of Clostridum difficile colitis Quinupristin-dalfopristin MLSB resistance known Mixture of streptogramins VRE if Enterococcus faecium (but not E. faecalis) Linezolid VRSA, MRSA, VRE (both E. faecium and E.faecalis) May cause mild thrombocytopenia and bone marrow suppression
 Aplastic anemia (gray baby syndrome) Restricted uses (e.g. serious rickettsial infections) Clindamycin (a lincomycin) MLSB resistance known. Works like macrolides. Bacteroides, several anaerobes. Increased danger of Clostridum difficile colitis. Quinupristin-dalfopristin MLSB resistance known Mixture of streptogramins. VRE if Enterococcus faecium (but not E. faecalis) Linezolid. VRSA, MRSA, VRE (both E. faecium and E.faecalis) May cause mild thrombocytopenia and bone marrow suppression.")
34
Drugs affecting nucleic acid synthesis
Folate inhibitors Sulfonamides (derivatives of sulfanilamide structural analog of p-aminobenzoic acid) Trimethoprim, pyrimethamine DNA gyrase inhibitors Quinolones
 Trimethoprim, pyrimethamine. DNA gyrase inhibitors. Quinolones.")
35
Purine and pyrimidine synthesis

36
Spectrum of sulfonamides
Gram-positives and gram-negatives Nocardia Chlamydia Some protozoa Note: Sulfonamides stimulate rickettsial growth. Poor activity against anaerobes

37
Adverse reactions of sulfonamides
Allergies Photosensitivity Nausea and diarrhea Fever and skin rashes, exfoliative dermatitis Steven-Johnson syndrome (<1% treatment courses) Inactivation in part in liver Crystalluria, hematuria (drugs and inactivated forms excreted in urine and precipitate at acid pH) Hematopoietic reactions Hemolytic anemia or aplastic anemia Granulocytopenia, thrombocytopenia, leukemoid Glucose-6-DH deficiency – enhanced hemolytic reactions If given in late pregnancy Kernicterus (brain damage due to excess jaundice)
 Inactivation in part in liver. Crystalluria, hematuria (drugs and inactivated forms excreted in urine and precipitate at acid pH) Hematopoietic reactions. Hemolytic anemia or aplastic anemia. Granulocytopenia, thrombocytopenia, leukemoid. Glucose-6-DH deficiency – enhanced hemolytic reactions. If given in late pregnancy. Kernicterus (brain damage due to excess jaundice)")
38
Trimethoprim (TMP) Mainly excreted in urine
Good absorption orally. Lipid solubility enhances distribution (more than sulfamethoxazole - SMX) including into CSF Extended use gives similar side effects to sulfonamides Reduces length of sulfonamide treatment time when used in combination with the sulfonamide E.g. TMP-SMX for UTIs and Pneumocystis prophylaxis Pyrimethamine-sulfadiazine for Toxoplasma
 including into CSF. Extended use gives similar side effects to sulfonamides. Reduces length of sulfonamide treatment time when used in combination with the sulfonamide. E.g. TMP-SMX for UTIs and Pneumocystis prophylaxis. Pyrimethamine-sulfadiazine for Toxoplasma.")
39
Quinolones Interfere with DNA gyrase and DNA topoisomerase IV

40
Activity of fluoroquinolones
Excellent activity against Gram-negatives Lesser activity against Gram-positives but some newer agents better (e.g. ciprofloxacin maintained for anthrax) Bactericidal and have a post antibiotic effect
 Bactericidal and have a post antibiotic effect.")
41
Uptake of Quinolones Oral agents
Uptake inhibited up to 80% by coadministration with Al and Mg-containing antacids. Some inhibition by calcium and ferrous ions. Most also available for i.v. administration Excreted in urine except ciprofloxacin with 50% bile and 50% urine

42
Indications for fluoroquinolones
b-lactam-resistant gonococcus Cystitis (where trimethoprim-sulfamethoxazole not useful) Complicated ascending UTIs (ureter/kidney) Prostatitis (drugs concentrate in prostatic tissue) Single dose for gonorrhea (but resistance developing) Pelvic inflammatory disease
 Complicated ascending UTIs (ureter/kidney) Prostatitis (drugs concentrate in prostatic tissue) Single dose for gonorrhea (but resistance developing) Pelvic inflammatory disease.")
43
Indications for quinolones
Respiratory tract infections Many uses but may be need in combination with b-lactams for severe pneumococcal pneumonia or with other drugs when Pseudomonas is likely (e.g. ventilators) Gastrointestinal infection Very useful for Shigella (1 dose), Salmonella (including typhoid), E. coli, cholera, Campylobacter (3-5 days). Resistance a concern
 Gastrointestinal infection. Very useful for Shigella (1 dose), Salmonella (including typhoid), E. coli, cholera, Campylobacter (3-5 days). Resistance a concern.")
44
Adverse reactions of quinolones
Nausea – vomiting - diarrhea Some cause Q-T interval prolongation May damage growing cartilage (not recommended in under 18 year olds) but the damage appears reversible and the drugs are likely safe for some uses Tendinitis (rare in adults – main >50 years) Usually starts in Achilles tendon - can lead to tendon rupture Probably should be avoided during pregnancy since safety not shown
 but the damage appears reversible and the drugs are likely safe for some uses. Tendinitis (rare in adults – main >50 years) Usually starts in Achilles tendon - can lead to tendon rupture. Probably should be avoided during pregnancy since safety not shown.")
45
Metronidazole (Flagyl®)
No net charge at physiological pH. Small molecule enters cells. Very good bioavailability, can be given orally Effective on most obligate anaerobic bacteria including Clostridium difficile, and Gardnerella vaginalis but NOT useful for most Actinomyces spp. and all Propionibacteria (e.g. P. acnes). Effective against anaerobic protozoa (Trichomonas, Giardia, Entamoeba) Activated after being reduced by ferredoxin Redox potential produced by aerobically growing bacteria not low enough to activate the drug.
. Effective against anaerobic protozoa (Trichomonas, Giardia, Entamoeba) Activated after being reduced by ferredoxin. Redox potential produced by aerobically growing bacteria not low enough. to activate the drug.")
46
Ferredoxinred Ferredoxinox Metronidazole Short-lived intermediates
R-NO2 + e- → R-NO2-● R-NO2-● + H+ → R-NO2H● 2R-NO2H● → R-NO2 + R-N(OH)2 R-N(OH)2 → R-NO + H2O R-NO + e- → R-NO-● R-NO-● + H+ → R-NOH● R-NOH● + R-NO2H● → R-NHOH + R-NO2 R-NHOH + 2e- + 2H+ → R-NH2 + H2O Free radicals (●) fragment DNA. The intermediates produced by reduction of the –NO2 group are the active form of the drug
2. R-N(OH)2 → R-NO + H2O. R-NO + e- → R-NO-● R-NO-● + H+ → R-NOH● R-NOH● + R-NO2H● → R-NHOH + R-NO2. R-NHOH + 2e- + 2H+ → R-NH2 + H2O. Free radicals (●) fragment DNA. The intermediates. produced by. reduction of the. –NO2 group are the. active form of. the drug.")
47
Antimicrobials Part II
Antimycobacterials Detecting resistance Probiotics

48
Treatment of mycobacterial diseases
Problems Waxy cell walls (inhibiting drug diffusion) Bacteria live both extracellular and intracellular Slow growth (drugs must be used for long periods) Many drugs only work for one or a few species Active disease should be treated using combination therapy with multiple drugs
 Bacteria live both extracellular and intracellular. Slow growth (drugs must be used for long periods) Many drugs only work for one or a few species. Active disease should be treated using combination therapy with multiple drugs.")
49
Tuberculosis All first line agents except ethambutol are all hepatotoxic and when used together have heightened hepatotoxicity Streptomycin (no longer first line because resistance is fairly common) is not hepatotoxic Treatment using first line agents becomes modified based on: Pre-existing hepatitis Pre-existing drug resistance
 is not hepatotoxic. Treatment using first line agents becomes modified based on: Pre-existing hepatitis. Pre-existing drug resistance.")
50
First line agents Isoniazid (INH)
Targets cell wall fatty acid synthesis Only for Mtb (not used for other mycobacteria) Requires activation by Mtb catalase-peroxidase Used alone in treatment of PPD-positive persons with latent TB infection (i.e., no active disease) Resistance when Mtb that have lost catalase gene Resistance shown by Mtb with altered INH targets Liver toxicity increases with age Other toxicities include peripheral neuropathy (often reversible by vitamin B6), lupus-like syndrome (~1% of persons though 20% develop anti-DNA)
 Requires activation by Mtb catalase-peroxidase. Used alone in treatment of PPD-positive persons with latent TB infection (i.e., no active disease) Resistance when Mtb that have lost catalase gene. Resistance shown by Mtb with altered INH targets. Liver toxicity increases with age. Other toxicities include peripheral neuropathy (often reversible by vitamin B6), lupus-like syndrome (~1% of persons though 20% develop anti-DNA)")
51
Other first line agents against Mtb
Rifampin (RIF) Good at inhibiting and killing bacteria Used for other mycobacteria including M. leprae Used for HIV-associated Mtb Induces acetylating enzymes in liver thus reducing its activity as treatment continues Hepatotoxicity, itching, and orange staining of secretions are most common side effects Significant drug interactions (including cyclosporine, contraceptives …) since it induces many cytochrome P450 isoforms. Can’t be used with AZT (zidovudine) since it upregulates the glucuronyl transferase that inactivates AZT. Also used for prophylaxis of contacts of children with active H. influenzae type b disease
 Good at inhibiting and killing bacteria. Used for other mycobacteria including M. leprae. Used for HIV-associated Mtb. Induces acetylating enzymes in liver thus reducing its activity as treatment continues. Hepatotoxicity, itching, and orange staining of secretions are most common side effects. Significant drug interactions (including cyclosporine, contraceptives …) since it induces many cytochrome P450 isoforms. Can’t be used with AZT (zidovudine) since it upregulates the glucuronyl transferase that inactivates AZT. Also used for prophylaxis of contacts of children with active H. influenzae type b disease.")
52
Other first line agents against Mtb
Pyrazinamide Most hepatotoxic of first line agents Good killing within macrophages and in caseous lesions Not effective at alkaline or neutral pH Deaminated in bacteria to make inhibitor of fatty acid synthase. M. bovis is resistant (amino acid substitution in deaminase) Polyarthraligia and hyperuricemia are main side effects Ethambutol Inhibits cell wall arabinogalactan formation No liver toxicity Significant toxicities include retrobulbar neuritis affecting visual acuity and severe skin reactions
 Polyarthraligia and hyperuricemia are main side effects. Ethambutol. Inhibits cell wall arabinogalactan formation. No liver toxicity. Significant toxicities include retrobulbar neuritis affecting visual acuity and severe skin reactions.")
53
Streptomycin One of numerous second line agents
Aminoglycoside works extracellularly only Toxicities include ototoxicity, circumoral parathesias Toxicity noted especially for Cranial nerve VIII Not hepatotoxic

54
Other mycobacteria Dapsone
sulfonamide-like inhibits folate synthesis Used in Multiple Drug Therapy to prevent resistance arising. Typically dapsone is used with rifampin and clofazimine in leprosy

55
Other mycobacteria Azithromycin or clarithromycin (macrolides)
Prophylaxis for M. avium when CD4<75/ml Azithromycin has elimination half life ~3 days (i.e. once-a week dosing is possible)
")
56
ANTIMICROBIAL SUSCEPTIBILITY TESTING

57
Resistance limits usefulness of antimicrobials
Need to identify isolates and also test for resistance 1. Intrinsic resistance in some species (no target) 2. Development of resistance Blocking entry of antibiotic or upregulating export pumps Mutation or enzymatic modification of target Overexpressing target or upregulating alternative pathway bypassing target Modifying antibiotic directly to inactivate it Failing to activate antibiotic.
 2. Development of resistance. Blocking entry of antibiotic or upregulating export pumps. Mutation or enzymatic modification of target. Overexpressing target or upregulating alternative pathway bypassing target. Modifying antibiotic directly to inactivate it. Failing to activate antibiotic.")
58
MIC – a quantitative measure of susceptibility
Minimum inhibitory concentration (MIC) Measures concentration of drug that prevents growth in vitro (does not necessarily kill bacterium) when tested over a set period, usually 1 day. MIC is an intrinsic property of the bacterium. It stays the same regardless of site of infection (unless strain develops resistance). Therapy should be chosen to so the concentration of drug in the areas of infection exceeds the MIC
 Measures concentration of drug that prevents growth in vitro (does not necessarily kill bacterium) when tested over a set period, usually 1 day. MIC is an intrinsic property of the bacterium. It stays the same regardless of site of infection (unless strain develops resistance). Therapy should be chosen to so the concentration of drug in the areas of infection exceeds the MIC.")
59
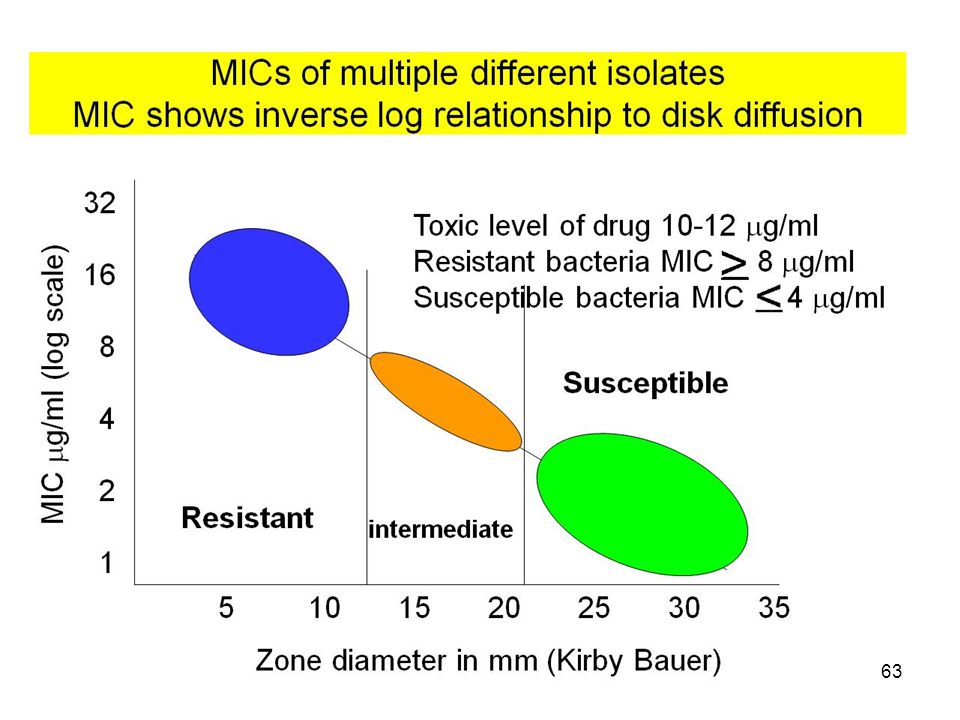
Significance of MIC for clinical practice
When the MIC for an antimicrobial is greater than safe therapeutic concentration, bacteria are resistant When the MIC is below the safe therapeutic level, bacteria are susceptible An increase in MIC points to resistance developing

60
MIC determination - Tube dilution assay Bacterium, growth medium and drug added to each tube incubated 24 h Susceptible isolate (Drug only toxic above 6 mg/ml) MIC = 1 mg/ml Concentration of drug in tube (mg/ml)
 MIC = 1 mg/ml Concentration of drug in tube (mg/ml)")
61
Tube dilution assay - resistant isolate Isolate is resistant because drug is toxic above 6 mg/ml)
MIC = 8 mg/ml Concentration of drug in tube (mg/ml)
")
62
MIC from antibiotic diffusion in agar
Inoculation of plate with clinical isolate. Antibacterial disks are placed on surface. Plates incubated ~24 h to allow bacteria to form a lawn Kirby-Bauer Zone around antibiotic disc showing no bacterial growth due to presence of antibacterial diffusing out of disk. Antimicrobial is most concentrated at disk A B C

64
E-TEST® agar diffusion MIC determination
Continuous scale - not just doubling dilutions. Expensive

65
Surrogate tests Numerous types: tests with one drug to predict response to another E.g. 30 mg cefoxitin disk for oxacillin-resistant Staph. aureus (i.e. MRSA) Cefoxitin induces mecA (PBP2a) more effectively than oxacillin in those MRSA that are not constitutive producers of PBP2a
 Cefoxitin induces mecA (PBP2a) more effectively than oxacillin in those MRSA that are not constitutive producers of PBP2a.")
66
Macrolide - Lincosamide - Streptogramin B resistance
Staphylococcus aureus Erythromycin R Clindamycin S This result could hide potential to express clindamycin resistance (MLSB pattern) due to methylase. Erythromycin far better inducer of methylase than is clindamycin If resistance to clindamycin induced by erythromycin (D-test), this points to MLSB resistance
 due to methylase. Erythromycin far better inducer of methylase than is clindamycin. If resistance to clindamycin induced by erythromycin (D-test), this points to MLSB resistance.")
67
Measuring bactericidal activity
MBC (minimum bactericidal concentration) – concentration needed to ensure all bacteria killed Specialty test, only occasionally used when patients lack residual immunity, or when infection may require bactericidal levels such as in endocarditis/osteomyelitis
 – concentration needed to ensure all bacteria killed. Specialty test, only occasionally used when patients lack residual immunity, or when infection may require bactericidal levels such as in endocarditis/osteomyelitis.")
68
Extended spectrum b-lactamases ESBLs
Over 340 different b-lactamases in Gram-negative rods. Some have very limited substrate activity e.g. the plasmid-mediated penicillinases with little activity against cephalosporins SHV-1- ~ 100% Klebsiella pneumoniae isolates (confers R to ampicillin+ticarcillin) TEM-1 - ~ 50% (currently ) E. coli isolates (confers R to ampicillin). Mutations in the genes for SHV-1 and TEM-1 → extended-spectrum b-lactamases (ESBLs) ESBLs have activity against ALL the penicillins, most cephalosporins, and aztreonam. Most common in Klebsiella pneumoniae, K. oxytoca, E. coli but also in other Gram-negatives
 TEM-1 - ~ 50% (currently ) E. coli isolates (confers R to ampicillin). Mutations in the genes for SHV-1 and TEM-1 → extended-spectrum b-lactamases (ESBLs) ESBLs have activity against ALL the penicillins, most cephalosporins, and aztreonam. Most common in Klebsiella pneumoniae, K. oxytoca, E. coli but also in other Gram-negatives.")
69
Many microbes exist in complex communities Therapeutic alterations to “microbiota”
Antibiotics Chemicals directly targeting (inhibiting/killing) microbes Prebiotics Non–digested ingredients that selectively stimulate one or a group of bacteria in the colon: e.g. lactulose used to reduce ammonia Probiotics Live organisms, which when administered in adequate amounts, confer a health benefit on the host
 microbes. Prebiotics. Non–digested ingredients that selectively stimulate one or a group of bacteria in the colon: e.g. lactulose used to reduce ammonia. Probiotics. Live organisms, which when administered in adequate amounts, confer a health benefit on the host.")
70
Targeted antibiotics Bacteriophages
Increasing interest in bacteriophages to attack biofilms and at other sites. Many are highly species-specific Many bacteria attacked by a large number of different bacteriophages suggesting several targets Rapid lysis of cell wall bright about by murein (peptidoglycan) hydrolases produced during infection (similar structures to bacterial peptidoglycan hydrolases)
 hydrolases produced during infection (similar structures to bacterial peptidoglycan hydrolases)")
71
Lysins produced during intracellular growth by bacteriophages
Lysins transferred to wall via pores (holins) produced by phage during infection. Pure lysins can act at outside of bacterial cell Hermoso et al., Current Opinion in Microbiology 2007, 10:
 produced by phage during. infection. Pure lysins can act at outside of. bacterial cell. Hermoso et al., Current Opinion in Microbiology 2007, 10:")
72
Potential problems of bacteriophage therapy
Narrow host range of most lytic phages Bacteria can become resistant Antibody responses may neutralize activity Pharmacokinetics not easy Potential to mobilize and transfer genes Use of phage lytic enzymes appears to avoid most of these problems. Resistance does not seem to develop

73
Probiotics “Live organisms, which when administered in adequate amounts, confer a health benefit on the host.” Bacteria must be able to adhere and colonize and work within context of a biofilm Indications suggest usefulness in halitosis and maybe caries (tooth decay) Strong evidence for value in pouchitis following ileal pouch-anal anastomosis
 Strong evidence for value in pouchitis following ileal pouch-anal anastomosis.")
74
Fecal flora therapy in relapsing Clostridium difficile colitis
5% of C. difficile colitis do not respond permanently to treatment with metronidazole or vancomycin and develop a relapse Fecal flora replacement with non-C. difficile donor has been reported effective More research needed

75
Microbial intestinal flora may prime for allergic responses
Antibiotic-treated and Candida colonized mice Cefoperazone 5 days ± Candida albicans orally antigen/spore lung challenge for 2-3 weeks Noverr et al. Infect. Immun. 2005;73:30-38

76
Candida in intestinal flora may prime for allergic responses in lung (response is IL-13 dependent)
Mice treated with cefoperazone Mice treated with cefoperazone for for 5 days No Candida days and colonized with C. albicans Challenge with Aspergillus spores 4 times in 12 days after Candida Ovalbumin 6 times in 21 days after Candida increased IgE, goblet cell metaplasia lung eosinophils Noverr et al. Infect. Immun. 2005;73:30-38

77
Antibiotics and asthma in humans
Antibiotic usage changes microbial flora in intestine and changes stay for significant time – More clostridia and Candida (stimulatory lipids) Less lactobacilli (butyrate, anti-inflammatory) Possibly allows increased chances of developing asthma Several papers suggest antibiotic use early in life is a risk factor for asthma Suggestion that probiotics given infant may reduce tendency to develop asthma (some data)
 Less lactobacilli (butyrate, anti-inflammatory) Possibly allows increased chances of developing asthma. Several papers suggest antibiotic use early in life is a risk factor for asthma. Suggestion that probiotics given infant may reduce tendency to develop asthma (some data)")
Similar presentations