Download presentation
Presentation is loading. Please wait.

1
Poisons and Drugs Prof. Monzir S. Abdel-Latif Chemistry Department Islamic University of Gaza http://www.monzir-pal.net

2
Areas of Toxicology

3
Mechanistic Toxicology A mechanistic toxicologist is concerned with identifying and understanding the mechanisms by which chemicals exert toxic effects on living organisms. For example, the relative toxic potential of organophosphate insecticides in humans, rodents, and insects can be accurately predicted on the basis of an understanding of common mechanisms (inhibition of acetylcholinesterase). A mechanistic toxicologist is concerned with identifying and understanding the mechanisms by which chemicals exert toxic effects on living organisms. For example, the relative toxic potential of organophosphate insecticides in humans, rodents, and insects can be accurately predicted on the basis of an understanding of common mechanisms (inhibition of acetylcholinesterase).
. A mechanistic toxicologist is concerned with identifying and understanding the mechanisms by which chemicals exert toxic effects on living organisms. For example, the relative toxic potential of organophosphate insecticides in humans, rodents, and insects can be accurately predicted on the basis of an understanding of common mechanisms (inhibition of acetylcholinesterase)..")
4
Descriptive Toxicology A descriptive toxicologist is concerned directly with toxicity testing, which provides information for safety evaluation and regulatory requirements. The appropriate toxicity tests in cell culture systems or experimental animals are designed to yield information to evaluate risks posed to humans and the environment from exposure to specific chemicals. Toxicologists in the chemical industry, however, must be concerned not only with the risk posed by a company ’ s chemicals (insecticides, herbicides, solvents, etc.) to humans but also with potential effects on fish, birds, and plants, as well as other factors that might disturb the balance of the ecosystem. A descriptive toxicologist is concerned directly with toxicity testing, which provides information for safety evaluation and regulatory requirements. The appropriate toxicity tests in cell culture systems or experimental animals are designed to yield information to evaluate risks posed to humans and the environment from exposure to specific chemicals. Toxicologists in the chemical industry, however, must be concerned not only with the risk posed by a company ’ s chemicals (insecticides, herbicides, solvents, etc.) to humans but also with potential effects on fish, birds, and plants, as well as other factors that might disturb the balance of the ecosystem.
 to humans but also with potential effects on fish, birds, and plants, as well as other factors that might disturb the balance of the ecosystem. A descriptive toxicologist is concerned directly with toxicity testing, which provides information for safety evaluation and regulatory requirements. The appropriate toxicity tests in cell culture systems or experimental animals are designed to yield information to evaluate risks posed to humans and the environment from exposure to specific chemicals. Toxicologists in the chemical industry, however, must be concerned not only with the risk posed by a company ’ s chemicals (insecticides, herbicides, solvents, etc.) to humans but also with potential effects on fish, birds, and plants, as well as other factors that might disturb the balance of the ecosystem..")
5
Regulatory Toxicology A regulatory toxicologist has the responsibility for deciding, on the basis of data provided by descriptive and mechanistic toxicologists, whether a drug or other chemical poses a sufficiently low risk to be marketed for a stated purpose and the subsequent human or environmental impacts resulting from its use. A regulatory toxicologist has the responsibility for deciding, on the basis of data provided by descriptive and mechanistic toxicologists, whether a drug or other chemical poses a sufficiently low risk to be marketed for a stated purpose and the subsequent human or environmental impacts resulting from its use.

6
Some Regulatory Bodies in USA In the USA, the Food and Drug Administration (FDA) is responsible for allowing drugs, cosmetics, and food additives to be sold in the market according to the Federal Food, Drug and Cosmetic Act (FFDCA). The U.S. Environmental Protection Agency (EPA) is responsible for regulating most other chemicals according to the Federal Insecticide, Fungicide and Rodenticide Act (FIFRA), the Toxic Substances Control Act (TSCA), the Resource Conservation and Recovery Act (RCRA), the Safe Drinking Water Act, and the Clean Air Act. In 1996, the U.S. Congress passed the Food Quality Protection Act (FQPA) which fundamentally changed the pesticide and food safety laws under FIFRA and FFDCA requiring stricter safety standards particularly for infants and children, who were recognized as more susceptible to health effects of pesticides. In the USA, the Food and Drug Administration (FDA) is responsible for allowing drugs, cosmetics, and food additives to be sold in the market according to the Federal Food, Drug and Cosmetic Act (FFDCA). The U.S. Environmental Protection Agency (EPA) is responsible for regulating most other chemicals according to the Federal Insecticide, Fungicide and Rodenticide Act (FIFRA), the Toxic Substances Control Act (TSCA), the Resource Conservation and Recovery Act (RCRA), the Safe Drinking Water Act, and the Clean Air Act. In 1996, the U.S. Congress passed the Food Quality Protection Act (FQPA) which fundamentally changed the pesticide and food safety laws under FIFRA and FFDCA requiring stricter safety standards particularly for infants and children, who were recognized as more susceptible to health effects of pesticides.
 is responsible for regulating most other chemicals according to the Federal Insecticide, Fungicide and Rodenticide Act (FIFRA), the Toxic Substances Control Act (TSCA), the Resource Conservation and Recovery Act (RCRA), the Safe Drinking Water Act, and the Clean Air Act. In 1996, the U.S. Congress passed the Food Quality Protection Act (FQPA) which fundamentally changed the pesticide and food safety laws under FIFRA and FFDCA requiring stricter safety standards particularly for infants and children, who were recognized as more susceptible to health effects of pesticides. In the USA, the Food and Drug Administration (FDA) is responsible for allowing drugs, cosmetics, and food additives to be sold in the market according to the Federal Food, Drug and Cosmetic Act (FFDCA). The U.S. Environmental Protection Agency (EPA) is responsible for regulating most other chemicals according to the Federal Insecticide, Fungicide and Rodenticide Act (FIFRA), the Toxic Substances Control Act (TSCA), the Resource Conservation and Recovery Act (RCRA), the Safe Drinking Water Act, and the Clean Air Act. In 1996, the U.S. Congress passed the Food Quality Protection Act (FQPA) which fundamentally changed the pesticide and food safety laws under FIFRA and FFDCA requiring stricter safety standards particularly for infants and children, who were recognized as more susceptible to health effects of pesticides..")
7
Other Areas of Toxicology Forensic toxicology is a hybrid of analytic chemistry and fundamental toxicological principles. It is concerned primarily with the medicolegal aspects of the harmful effects of chemicals on humans and animals. The expertise of forensic toxicologists is invoked primarily to aid in establishing the cause of death and determining its circumstances in a postmortem investigation. Forensic toxicology is a hybrid of analytic chemistry and fundamental toxicological principles. It is concerned primarily with the medicolegal aspects of the harmful effects of chemicals on humans and animals. The expertise of forensic toxicologists is invoked primarily to aid in establishing the cause of death and determining its circumstances in a postmortem investigation.

8
Clinical toxicology designates an area of professional emphasis in the field of medical science that is concerned with disease caused by or uniquely associated with toxic substances Clinical toxicology designates an area of professional emphasis in the field of medical science that is concerned with disease caused by or uniquely associated with toxic substances

9
Environmental toxicology focuses on the impacts of chemical pollutants in the environment on biological organisms. Although toxicologists concerned with the effects of environmental pollutants on human health fit into this definition, it is most commonly associated with studies on the impacts of chemicals on nonhuman organisms such as fish, birds, animals, and plants. Environmental toxicology focuses on the impacts of chemical pollutants in the environment on biological organisms. Although toxicologists concerned with the effects of environmental pollutants on human health fit into this definition, it is most commonly associated with studies on the impacts of chemicals on nonhuman organisms such as fish, birds, animals, and plants.

10
Local versus systemic effects Adverse effects may be local or systemic. Local effects occur at the site of exposure of the organism to the potentially toxic substance. Corrosives always act locally. Irritants frequently act locally. Most substances that are not highly reactive are absorbed and distributed around the affected organism causing general injury at a target organ or tissue distinct from the absorption site.

11
The target organ is not necessarily the organ of greatest accumulation. For example, adipose (fatty) tissue accumulates organochlorine pesticides to very high levels but does not appear to be affected by them. Some substances produce both local and systemic effects. For example, tetraethyl lead damages the skin on contact, and is then absorbed and transported to the central nervous system where it causes further damage. Accumulation Site and Affected Organ
 tissue accumulates organochlorine pesticides to very high levels but does not appear to be affected by them. Some substances produce both local and systemic effects. For example, tetraethyl lead damages the skin on contact, and is then absorbed and transported to the central nervous system where it causes further damage. Accumulation Site and Affected Organ.")
12
Effects of a chemical can accumulate even if the chemical itself does not. There is some evidence that this is true of the effects of organophosphate pesticides and other neurotoxins on the nervous system. This may lead to poor functioning of the nervous system in humans in old age. Because of the time difference between exposure and effect, establishing the relationship between such delayed effects and the toxin is often difficult.

13
Adverse effects related to allergies appear to be increasing. Allergy (hypersensitivity) is the name given to disease symptoms following exposure to a previously encountered substance (allergen) that would otherwise be classified as harmless. Essentially, an allergy is an adverse reaction of the altered immune system. The process, which leads to the disease response on subsequent exposure to the allergen, is called sensitization. Allergy
 is the name given to disease symptoms following exposure to a previously encountered substance (allergen) that would otherwise be classified as harmless. Essentially, an allergy is an adverse reaction of the altered immune system. The process, which leads to the disease response on subsequent exposure to the allergen, is called sensitization. Allergy.")
14
Another important aspect of adverse effects to be considered is whether they are reversible or irreversible. For the liver, which has a great capacity for regeneration, many adverse effects are reversible, and complete recovery can occur. For the central nervous system, in which regeneration of tissue is severely limited, most adverse effects leading to morphological changes are irreversible and recovery is, at best, limited. Carcinogenic effects are also irreversible, but suitable treatment may reduce the severity of such effects Regenerative Versus Non-regenerative Tissue

15
CHARACTERISTICS OF EXPOSURE To characterize fully the potential hazard of a specific chemical agent, we need to know not only what type of effect it produces and the dose required to produce that effect but also information about the agent, the exposure, and its disposition in the subject. Two major factors that influence toxicity as it relates to the exposure situation for a specific chemical are the route of exposure, the duration, and frequency of exposure. To characterize fully the potential hazard of a specific chemical agent, we need to know not only what type of effect it produces and the dose required to produce that effect but also information about the agent, the exposure, and its disposition in the subject. Two major factors that influence toxicity as it relates to the exposure situation for a specific chemical are the route of exposure, the duration, and frequency of exposure.

16
Route and Site of Exposure The major routes (pathways) by which toxic agents gain access to the body are the gastrointestinal tract (ingestion), lungs (inhalation), skin, and other parenteral (other than intestinal canal) routes. Toxic agents generally produce the greatest effect and the most rapid response when given directly into the bloodstream (the intravenous route). An approximate descending order of effectiveness for the other routes would be inhalation, intraperitoneal, subcutaneous, intramuscular, intradermal, oral, and dermal. The major routes (pathways) by which toxic agents gain access to the body are the gastrointestinal tract (ingestion), lungs (inhalation), skin, and other parenteral (other than intestinal canal) routes. Toxic agents generally produce the greatest effect and the most rapid response when given directly into the bloodstream (the intravenous route). An approximate descending order of effectiveness for the other routes would be inhalation, intraperitoneal, subcutaneous, intramuscular, intradermal, oral, and dermal.
. An approximate descending order of effectiveness for the other routes would be inhalation, intraperitoneal, subcutaneous, intramuscular, intradermal, oral, and dermal. The major routes (pathways) by which toxic agents gain access to the body are the gastrointestinal tract (ingestion), lungs (inhalation), skin, and other parenteral (other than intestinal canal) routes. Toxic agents generally produce the greatest effect and the most rapid response when given directly into the bloodstream (the intravenous route). An approximate descending order of effectiveness for the other routes would be inhalation, intraperitoneal, subcutaneous, intramuscular, intradermal, oral, and dermal..")
17
Duration and Frequency of Exposure Toxicologists usually divide the exposure of experimental animals to chemicals into four categories: acute, subacute, subchronic, and chronic. Toxicologists usually divide the exposure of experimental animals to chemicals into four categories: acute, subacute, subchronic, and chronic. Acute exposure is defined as exposure to a chemical for less than 24 hours. Whereas acute exposure usually refers to a single administration, repeated exposures may be given within a 24-hours period for some slightly toxic or practically nontoxic chemicals. Acute exposure by inhalation refers to continuous exposure for less than 24 hours, most frequently for 4 hours. Acute exposure is defined as exposure to a chemical for less than 24 hours. Whereas acute exposure usually refers to a single administration, repeated exposures may be given within a 24-hours period for some slightly toxic or practically nontoxic chemicals. Acute exposure by inhalation refers to continuous exposure for less than 24 hours, most frequently for 4 hours.

18
Repeated exposure is divided into three categories: subacute, subchronic, and chronic. Repeated exposure is divided into three categories: subacute, subchronic, and chronic. Subacute exposure refers to repeated exposure to a chemical for 1 month or less. Subacute exposure refers to repeated exposure to a chemical for 1 month or less. Subchronic exposure refers to repeated exposure to a chemical for 1 to 3 months, and Subchronic exposure refers to repeated exposure to a chemical for 1 to 3 months, and Chronic exposure refers to repeated exposure to a chemical for more than 3 months, although usually this refers to studies with at least 1 year of repeated dosing. Chronic exposure refers to repeated exposure to a chemical for more than 3 months, although usually this refers to studies with at least 1 year of repeated dosing.

19
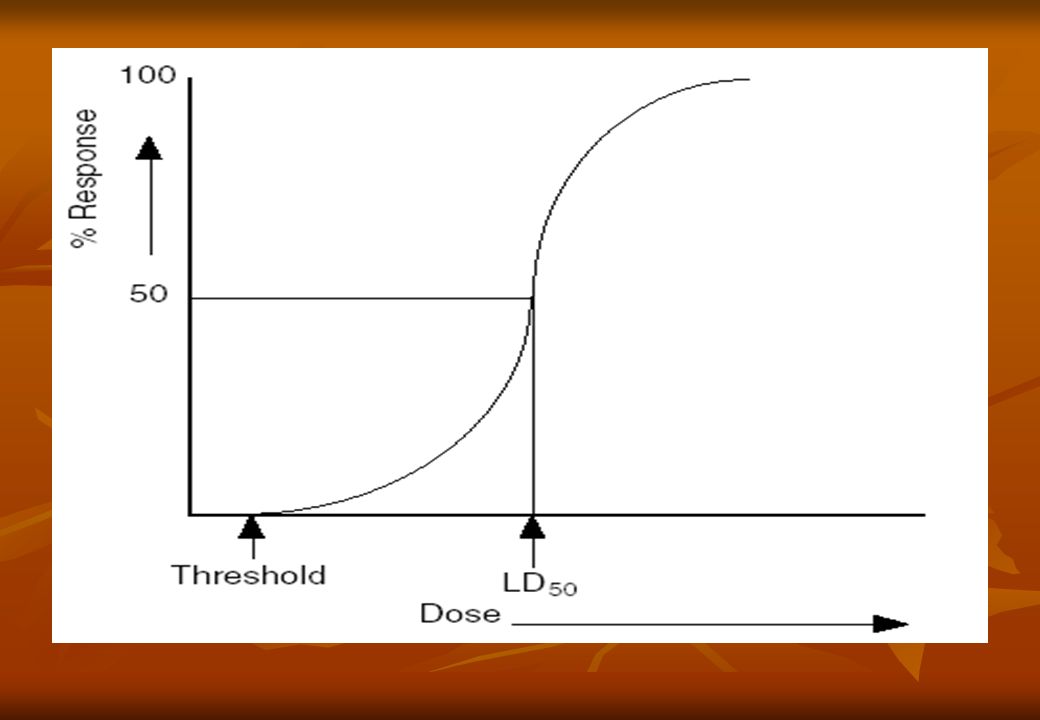
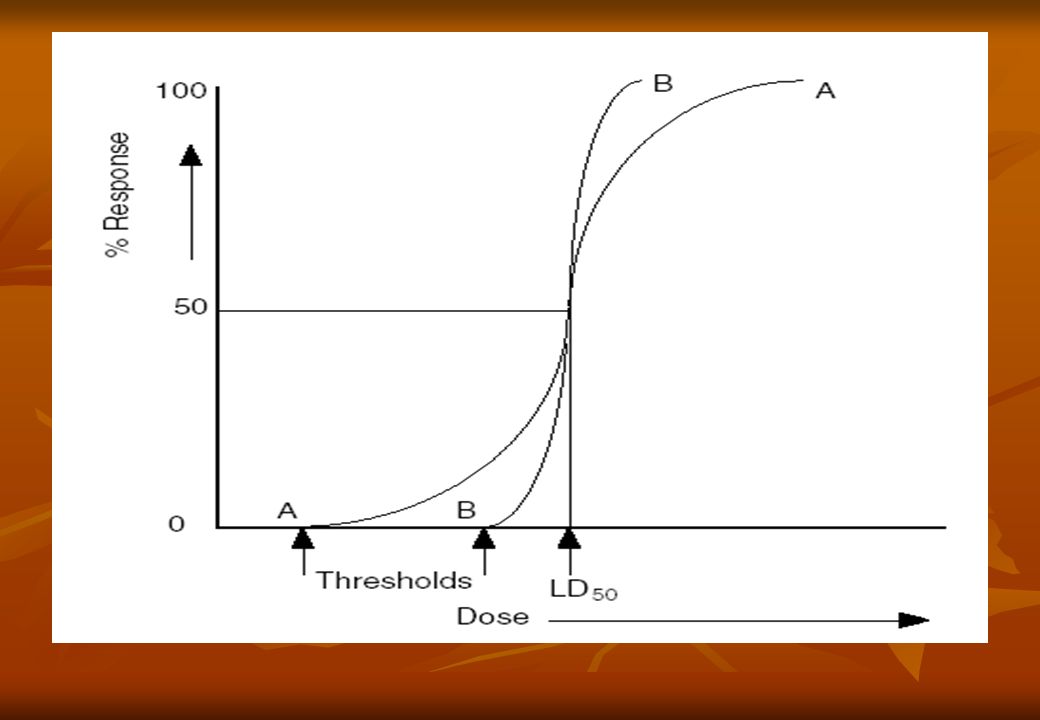
Toxicity testing Dose response and Concentration response A dose – response (concentration – response) relationship is defined as the association between dose (concentration) and the incidence of a defined biological effect in an exposed population, usually expressed as percentage. Historically the defined effect was death.

20
The classic dose – response or concentration – response relationship is shown in the figure below. This is a theoretical curve and in practice such a curve is rarely found. Curves of this kind form the basis for the determination of the LD 50 or the LC 50 (the median lethal concentration). The LD 50 and LC 50 are specific cases of the generalized values LD n and LC n. The LD n is the dose of a toxicant lethal to n% of a test population. The LC n is the exposure concentration of a toxicant lethal to n% of a test population.
. The LD 50 and LC 50 are specific cases of the generalized values LD n and LC n. The LD n is the dose of a toxicant lethal to n% of a test population. The LC n is the exposure concentration of a toxicant lethal to n% of a test population..")
22
the LD 50 is the statistically derived single dose of a chemical that can be expected to cause death in 50% of a given population of organisms under a defined set of experimental conditions. Similarly, the LC 50 is the statistically derived exposure concentration of a chemical that can be expected to cause death in 50% of a given population of organisms under a defined set of experimental conditions.

23
Approximate Acute LD 50 s of Some Representative Chemical Agents LD 50, mg/kg ∗ agent 10000Ethyl alcohol 4000Sodium chloride 1500Ferrous sulfate 900Morphine sulfate 150Phenobarbital sodium 5Picrotoxin 2Strychnine sulfate 1Nicotine 0.10Tetrodotoxin 0.001Dioxin (TCDD) 0.00001Botulinum toxin
 Botulinum toxin")
24
Workplace Hazardous Materials Information System (WHMIS) D1A- Poisonous product that causes serious and immediate effects. Oral LD 50 < 50 mg/kg Oral LD 50 < 50 mg/kg Dermal LD 50 < 200 mg/kg Dermal LD 50 < 200 mg/kg Inhalation LC 50 < 2500 ppm 4 hours (gas) Inhalation LC 50 < 2500 ppm 4 hours (gas) Inhalation LC 50 2 times the LC 50 value. Inhalation LC 50 2 times the LC 50 value. Inhalation LC 50 < 0.5 mg/l or < 500 mg/m 3 4 hours (dust, mist, fume) Inhalation LC 50 < 0.5 mg/l or < 500 mg/m 3 4 hours (dust, mist, fume)
 Inhalation LC 50 < 2500 ppm 4 hours (gas) Inhalation LC 50 2 times the LC 50 value. Inhalation LC 50 2 times the LC 50 value. Inhalation LC 50 < 0.5 mg/l or < 500 mg/m 3 4 hours (dust, mist, fume) Inhalation LC 50 < 0.5 mg/l or < 500 mg/m 3 4 hours (dust, mist, fume).")
25
D1B- Toxic material that causes serious and immediate effects. Similar criteria is used as for the D1A. The criteria is as follows: Oral LD 50 > 50 mg/kg 50 mg/kg < 500 mg/kg Dermal LD 50 > 200 mg/kg 200 mg/kg < 1000 mg/kg Inhalation LC 50 > 1500 ppm 1500 ppm < 2500 ppm 4 hours (vapor) Inhalation LC 50 > 0.5 mg/l 500 mg/m 3 0.5 mg/l 500 mg/m 3 < 2500 mg/m 3 4 hours(Dust, Fumes or Mist(
 Inhalation LC 50 > 0.5 mg/l 500 mg/m mg/l 500 mg/m 3 < 2500 mg/m 3 4 hours(Dust, Fumes or Mist(.")
28
Another important value that may be derived from the relationship shown is the threshold dose or concentration, the minimum dose or concentration required to produce a detectable response in the test population. The threshold value can never be derived with absolute certainty and therefore the lowest observed effect level (LOEL) or the NOEL have normally been used instead of the threshold value in deriving regulatory standards.
 or the NOEL have normally been used instead of the threshold value in deriving regulatory standards..")
30
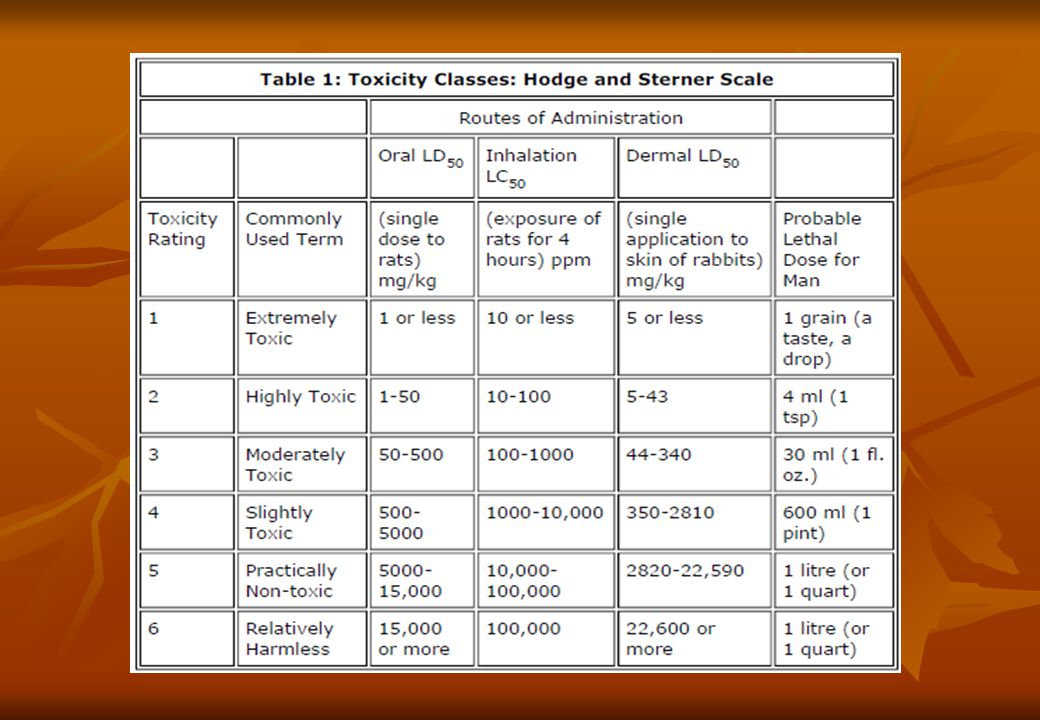
The use of the LD 50 in the classification of potentially toxic chemicals has been described; it must be emphasized that such a classification is only a very rough guide to relative toxicity. The LD 50 tells us nothing about sub lethal toxicity. Any classification based on the LD 50 is strictly valid only for the test population and conditions on which it is based and on the related route of exposure.

31
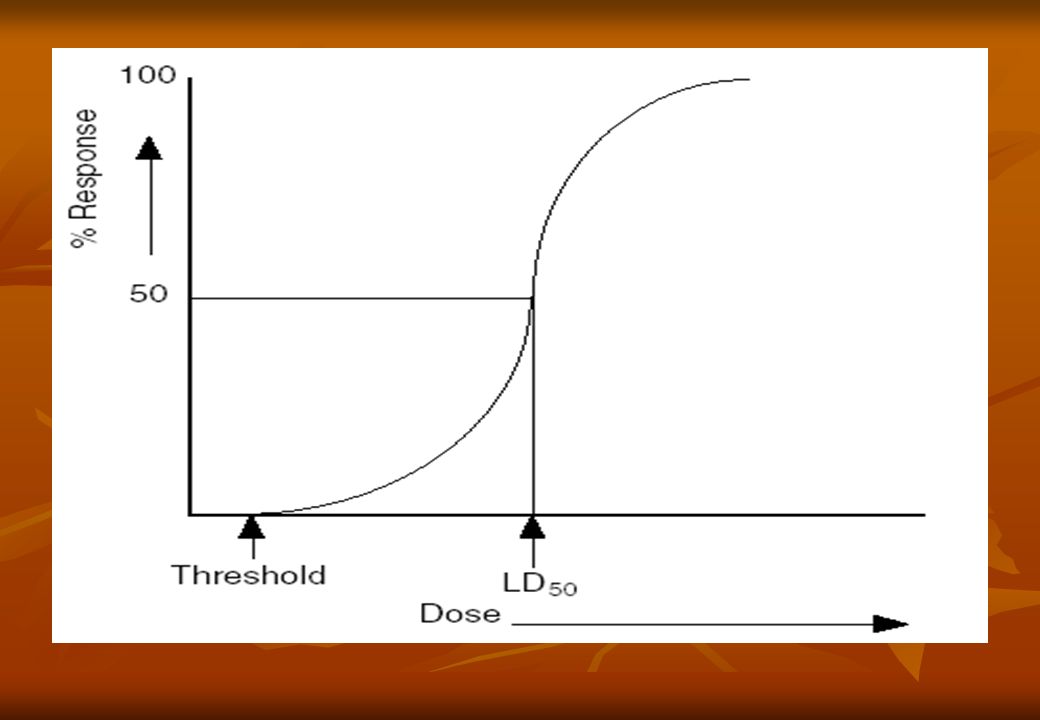
The LD 50 tells us nothing about the shape of the dose – response curve on which it is based. Thus, two chemicals may appear to be equally toxic since they have the same LD 50, but one may have a much lower lethal threshold and kills members of an exposed population at concentrations where the other has no effect LD 50 as a Measure of Toxicity

33
Fate of the LD 50 At their November meeting in 2001, the OECD Joint Meeting of the Chemicals Committee and Working Party on Chemicals, Pesticides and Biotechnolgy, agreed that the LD 50 for acute oral toxicity, known as OECD Test Guideline 401 and heavily criticised by the animal welfare protectorate shall be abolished and deleted from the OECD manual of internationally accepted Test Guidelines.

34
The determination and use of the LD 50 are likely to decline in future as fixed dose testing (The Fixed Dose Procedure (FDP), proposed in 1984) becomes more widely used. In fixed dose testing, the test substance may be administered to rats or other test species at no more than four dose levels: the possible dose levels are preset legally to equate with a regulatory classification or ranking system. Dosing is followed by an observation period of 14 days. The dose at which toxic signs are detected is used to rank or classify the test materials.

35
FDM versus LD 50 The new OECD FDM (Test Guideline 420) departs from the conventional method (Test Guideline 401) in two principal ways: The new OECD FDM (Test Guideline 420) departs from the conventional method (Test Guideline 401) in two principal ways: 1. FDM considers non-lethal endpoints; and 2. it does not develop a quantitative relationship between dose and lethality. The method relies upon clear signs of toxicity ("evident toxicity"), a non-lethal endpoint as well as lethality, as the basis for acute oral toxicity assessment. The method relies upon clear signs of toxicity ("evident toxicity"), a non-lethal endpoint as well as lethality, as the basis for acute oral toxicity assessment.
, a non-lethal endpoint as well as lethality, as the basis for acute oral toxicity assessment. The method relies upon clear signs of toxicity ( evident toxicity ), a non-lethal endpoint as well as lethality, as the basis for acute oral toxicity assessment..")
36
Acute Oral Toxicity - Fixed Dose Procedure This Guideline is intended primarily for use with rat. Groups of animals of a single sex (normally females) are dosed in a stepwise procedure using the fixed doses of 5, 50, 300 and 2000 mg/kg (exceptionally 5000 mg/kg). The initial dose level is selected on the basis of a sighting study as the dose expected to produce some signs of toxicity without causing severe toxic effects or mortality. Further groups of animals may be dosed at higher or lower fixed doses, depending on the presence or absence of signs of toxicity or mortality. This procedure continues until the dose causing evident toxicity or death is identified, or when no effects are seen at the highest dose or when deaths occur at the lowest dose. The test substance is administered in a single dose by gavage using a stomach tube or a suitable intubation canula. Animals should be fasted prior to dosing. A total of five animals of one sex will normally be used for each dose level investigated. This Guideline is intended primarily for use with rat. Groups of animals of a single sex (normally females) are dosed in a stepwise procedure using the fixed doses of 5, 50, 300 and 2000 mg/kg (exceptionally 5000 mg/kg). The initial dose level is selected on the basis of a sighting study as the dose expected to produce some signs of toxicity without causing severe toxic effects or mortality. Further groups of animals may be dosed at higher or lower fixed doses, depending on the presence or absence of signs of toxicity or mortality. This procedure continues until the dose causing evident toxicity or death is identified, or when no effects are seen at the highest dose or when deaths occur at the lowest dose. The test substance is administered in a single dose by gavage using a stomach tube or a suitable intubation canula. Animals should be fasted prior to dosing. A total of five animals of one sex will normally be used for each dose level investigated.
 are dosed in a stepwise procedure using the fixed doses of 5, 50, 300 and 2000 mg/kg (exceptionally 5000 mg/kg). The initial dose level is selected on the basis of a sighting study as the dose expected to produce some signs of toxicity without causing severe toxic effects or mortality. Further groups of animals may be dosed at higher or lower fixed doses, depending on the presence or absence of signs of toxicity or mortality. This procedure continues until the dose causing evident toxicity or death is identified, or when no effects are seen at the highest dose or when deaths occur at the lowest dose. The test substance is administered in a single dose by gavage using a stomach tube or a suitable intubation canula. Animals should be fasted prior to dosing. A total of five animals of one sex will normally be used for each dose level investigated. This Guideline is intended primarily for use with rat. Groups of animals of a single sex (normally females) are dosed in a stepwise procedure using the fixed doses of 5, 50, 300 and 2000 mg/kg (exceptionally 5000 mg/kg). The initial dose level is selected on the basis of a sighting study as the dose expected to produce some signs of toxicity without causing severe toxic effects or mortality. Further groups of animals may be dosed at higher or lower fixed doses, depending on the presence or absence of signs of toxicity or mortality. This procedure continues until the dose causing evident toxicity or death is identified, or when no effects are seen at the highest dose or when deaths occur at the lowest dose. The test substance is administered in a single dose by gavage using a stomach tube or a suitable intubation canula. Animals should be fasted prior to dosing. A total of five animals of one sex will normally be used for each dose level investigated..")
37
Fixed Dose testing In this procedure the test substance is given at one of the four fixed-dose levels (5, 50, 300, and 2000 mg/kg) to five male and five female rats. The objective is to identify a dose that produces clear signs of toxicity but no mortality. Depending on the results of the first test, either no further testing is needed or a higher or lower dose is tested: If mortality occurs, retesting at a lower dose level is necessary (except if the original dose chosen is 5 mg/kg). If no signs of toxicity occur at the initial dose, it is necessary to retest at a higher dose level. The results are thus interpreted in relation to animal survival and evident toxicity and it becomes possible to assign the chemical to one of the OECD classification categories. In this procedure the test substance is given at one of the four fixed-dose levels (5, 50, 300, and 2000 mg/kg) to five male and five female rats. The objective is to identify a dose that produces clear signs of toxicity but no mortality. Depending on the results of the first test, either no further testing is needed or a higher or lower dose is tested: If mortality occurs, retesting at a lower dose level is necessary (except if the original dose chosen is 5 mg/kg). If no signs of toxicity occur at the initial dose, it is necessary to retest at a higher dose level. The results are thus interpreted in relation to animal survival and evident toxicity and it becomes possible to assign the chemical to one of the OECD classification categories.
. If no signs of toxicity occur at the initial dose, it is necessary to retest at a higher dose level. The results are thus interpreted in relation to animal survival and evident toxicity and it becomes possible to assign the chemical to one of the OECD classification categories. In this procedure the test substance is given at one of the four fixed-dose levels (5, 50, 300, and 2000 mg/kg) to five male and five female rats. The objective is to identify a dose that produces clear signs of toxicity but no mortality. Depending on the results of the first test, either no further testing is needed or a higher or lower dose is tested: If mortality occurs, retesting at a lower dose level is necessary (except if the original dose chosen is 5 mg/kg). If no signs of toxicity occur at the initial dose, it is necessary to retest at a higher dose level. The results are thus interpreted in relation to animal survival and evident toxicity and it becomes possible to assign the chemical to one of the OECD classification categories..")
38
Fixed dose testing (no mortality) The initial test dose level is selected with a view to identifying toxicity without mortality occurring. Thus, if a group of five male and five female rats is tested with an oral dose of 300 mg/ kg body weight and no clear signs of toxicity appear, the substance should not be classified in any of the defined categories of toxicity. If toxicity is seen but no mortality, the substance can be classed as ‘ harmful ’.

39
If mortality occurs, retesting with a dose of 50 mg/ kg body weight is required. If no mortality occurs at the lower dose but signs of toxicity are detected, the substance would be classified as ‘ toxic ’. If mortality occurs at the lower dose, retesting at 5 mg/ kg body weight would be carried out and if signs of toxicity were detected and mortality occurred, the substance would be classified as ‘ very toxic ’.

40
Again: Fixed Dose Versus LD 50 In an international study involving 33 laboratories in 11 countries, the acute oral toxicity to the rat of 20 substances and preparations was evaluated using a fixed-dose procedure and the results compared with those obtained for the test materials using the classical LD 50 test. The study has shown that the fixed-dose approach to acute oral toxicity testing: (1) produces consistent results that are not substantially affected by inter-laboratory variations; (2) provides adequate information for risk assessment purposes on signs of toxicity, including their nature, time to onset, duration and outcome; (3) uses fewer animals than the current internationally agreed OECD procedure; (4) subjects animals to less pain and distress than the classical LD 50 test and causes less compound-related mortality. In an international study involving 33 laboratories in 11 countries, the acute oral toxicity to the rat of 20 substances and preparations was evaluated using a fixed-dose procedure and the results compared with those obtained for the test materials using the classical LD 50 test. The study has shown that the fixed-dose approach to acute oral toxicity testing: (1) produces consistent results that are not substantially affected by inter-laboratory variations; (2) provides adequate information for risk assessment purposes on signs of toxicity, including their nature, time to onset, duration and outcome; (3) uses fewer animals than the current internationally agreed OECD procedure; (4) subjects animals to less pain and distress than the classical LD 50 test and causes less compound-related mortality.
 produces consistent results that are not substantially affected by inter-laboratory variations; (2) provides adequate information for risk assessment purposes on signs of toxicity, including their nature, time to onset, duration and outcome; (3) uses fewer animals than the current internationally agreed OECD procedure; (4) subjects animals to less pain and distress than the classical LD 50 test and causes less compound-related mortality. In an international study involving 33 laboratories in 11 countries, the acute oral toxicity to the rat of 20 substances and preparations was evaluated using a fixed-dose procedure and the results compared with those obtained for the test materials using the classical LD 50 test. The study has shown that the fixed-dose approach to acute oral toxicity testing: (1) produces consistent results that are not substantially affected by inter-laboratory variations; (2) provides adequate information for risk assessment purposes on signs of toxicity, including their nature, time to onset, duration and outcome; (3) uses fewer animals than the current internationally agreed OECD procedure; (4) subjects animals to less pain and distress than the classical LD 50 test and causes less compound-related mortality..")
41
Workplace Hazardous Materials Information System (WHMIS) In order to apply this protocol to classification under WHMIS, the following interpretations should be applied: In order to apply this protocol to classification under WHMIS, the following interpretations should be applied: 1. Where mortality in the FDM is 50% at one of the fixed dose levels, it can be assumed that the LD 50 for the controlled product, when tested in accordance with OECD 401, would likely fall below that fixed dose level. Consequently, it follows that:

42
Where mortality in the FDM is 50% A. at a dose of 5 or 50 mg/kg b.w. one would classify the controlled product in D1A. B. at a dose of 500 mg/kg b.w. one would classify the controlled product in D1B, provided there was no data available to show that lethality at 50 mg/kg b.w. exceeded 50%. C. at a dose of 2000 mg/kg b.w., one would need to review test data at the next lower dose level (500 mg/kg) to determine if lethality at that level is 50%.
 to determine if lethality at that level is 50%..")
43
Where there is 100% survival with or without evident toxicity a. at a dose of 5 or 50 mg/kg b.w. one would need to review test data at the next highest dose level (50 or 500 mg/kg b.w.) to determine if lethality at that level is ³ 50%. b. at a dose of 500 or 2000 mg/kg b.w. the LD 5o is not very likely to be 500 mg/kg b.w., therefore the product would not be classified for acute oral toxicity under WHMIS Class D1. b. at a dose of 500 or 2000 mg/kg b.w. the LD 5o is not very likely to be 500 mg/kg b.w., therefore the product would not be classified for acute oral toxicity under WHMIS Class D1.
 to determine if lethality at that level is ³ 50%. b. at a dose of 500 or 2000 mg/kg b.w. the LD 5o is not very likely to be 500 mg/kg b.w., therefore the product would not be classified for acute oral toxicity under WHMIS Class D1. b. at a dose of 500 or 2000 mg/kg b.w. the LD 5o is not very likely to be 500 mg/kg b.w., therefore the product would not be classified for acute oral toxicity under WHMIS Class D1..")
44
3. Where mortality is 0% at one of the fixed dose levels, it can be assumed that in most cases, the LD 50 value for the substance, when tested in accordance with OECD 401, would fall above that fixed dose level. Consequently, it follows that:

45
Where mortality is 0% at one of the fixed dose levels a. at a dose of 5 mg/kg b.w. - one would need to review the lethality data for the next highest fixed dose (50 mg/kg) to determine the % lethality at that level. If mortality at the next fixed dose level is 50% the controlled product would be classified D1A.
 to determine the % lethality at that level. If mortality at the next fixed dose level is 50% the controlled product would be classified D1A..")
46
Where mortality is 0% at one of the fixed dose levels b. at a dose of 50 mg/kg b.w. - one would need to review the lethality data for the next highest fixed dose (500 mg/kg b.w.) to determine the % lethality at that level. If mortality at the next fixed dose level is ³ 50% the controlled product would be classified in D1B, as described in 1(b), above. However, if lethality at 50 mg/kg b.w. is 40% (i.e. if the data are pooled and 4/10 animals died, especially if the majority of them were of one sex) and no data are available at 500 mg/kg b.w., the conservative approach would be to assume that the LD 50 value for the substance might be below 50 mg/kg b.w., and consequently it would be prudent to classify in D1A.
 to determine the % lethality at that level. If mortality at the next fixed dose level is ³ 50% the controlled product would be classified in D1B, as described in 1(b), above. However, if lethality at 50 mg/kg b.w. is 40% (i.e. if the data are pooled and 4/10 animals died, especially if the majority of them were of one sex) and no data are available at 500 mg/kg b.w., the conservative approach would be to assume that the LD 50 value for the substance might be below 50 mg/kg b.w., and consequently it would be prudent to classify in D1A..")
47
Where mortality is 0% at one of the fixed dose levels c. at a dose of 500 mg/kg b.w. - if lethality at 500 mg/kg b.w. is 40% (i.e. 4/10 animals died) and no data are available at the next highest fixed dose (2000 mg/kg b.w.), the conservative approach would be to assume that the LD 50 value for the substance might be below 500 mg/kg b.w., and consequently it would be prudent to classify in D1B. If lethality at 500 mg/kg b.w. was lower than 40%, it would be reasonable to assume that the substance is not classified under WHMIS class D1. d. at a dose of 2000 mg/kg b.w. - not classified for acute oral toxicity under WHMIS Class D1.
 and no data are available at the next highest fixed dose (2000 mg/kg b.w.), the conservative approach would be to assume that the LD 50 value for the substance might be below 500 mg/kg b.w., and consequently it would be prudent to classify in D1B. If lethality at 500 mg/kg b.w. was lower than 40%, it would be reasonable to assume that the substance is not classified under WHMIS class D1. d. at a dose of 2000 mg/kg b.w. - not classified for acute oral toxicity under WHMIS Class D1..")
48
Acute Toxic Class Method The test consists of a stepwise procedure with the use of three animals of a single sex (normally females) per step. Absence or presence of compound-related mortality of the animals dosed at one step will determine the next step 1. 1. no further testing is needed, 2. 2. dosing of three additional animals, with the same dose 3. 3. dosing of three additional animals at the next higher or the next lower dose level. The starting dose level is selected from one of four fixed levels (5, 50, 300, and 2000) and it should be that which is most likely to produce mortality in some of the dosed animals. When there is no information on a substance to be tested, it is recommended to use the starting dose of 300 mg/kg. This procedure is reproducible, uses very few animals and is able to rank substances in a similar manner to the other acute toxicity testing methods.
 and it should be that which is most likely to produce mortality in some of the dosed animals. When there is no information on a substance to be tested, it is recommended to use the starting dose of 300 mg/kg. This procedure is reproducible, uses very few animals and is able to rank substances in a similar manner to the other acute toxicity testing methods..")
49
Acute Oral Toxicity: Up-and-Down Procedure The test consists of a single ordered dose progression in which animals of a single sex (normally females) are dosed, one at a time. The first animal receives a dose step below the level of the best estimate of the LD 50 (when no information is available to make a preliminary estimate of the LD 50, the suggested starting dose is 175 mg/kg). If the animal survives, the dose for the next animal is increased by a factor of 3.2 times the original dose; if it dies, the dose for the next animal is decreased by a similar dose progression. The preferred species is the female rat and the test substance is administered in a single dose by gavage (if not possible the dose may be given in smaller fractions over a period not exceeding 24 hours).
. If the animal survives, the dose for the next animal is increased by a factor of 3.2 times the original dose; if it dies, the dose for the next animal is decreased by a similar dose progression. The preferred species is the female rat and the test substance is administered in a single dose by gavage (if not possible the dose may be given in smaller fractions over a period not exceeding 24 hours)..")
Similar presentations





, the participant will interpret health hazard information.>")
 l DSN564-3520 X 7151 l COMM (757)>")












