Download presentation
Presentation is loading. Please wait.

1
Demography Prof Iain Crombie

2
Demography Study of populations
size and density, growth, age distribution, fertility, mortality,, migration and vital statistics the interaction of all these with social and economic conditions.

3
Our focus size growth age distribution fertility vital statistics
births deaths IMR PYLL DALY Population size and structure has important implications for patterns of health and disease

4
Population size World population estimates: 2008: 6.7 billion
Of 78 million people added to the world every year, 95% live in less developed countries

5
Growth in population by region

6
% population in urban areas

7
Population size Interplay of births, deaths and migration
P2 = P1 + Births – Deaths + Net migration

8
Scotland’s population:1855- 2002

9
Net migration and natural changes

10
Projecting the future

12
Scotland’s Population

13
Scotland’s Population: a spike

14
A wedge

16
A barrel

17
Scotland’s Population

18
Trends in births and birth rate

19
Infant mortality rates: Scotland

20
Scotland’s Population: a spike

21
Overall deaths and death rates

22
Trends in death rates among younger women

23
Trends in death rates among older women

24
A wedge

25
A barrel

26
Population pyramids a graphic presentation of the age and sex composition of the population types Spike: high birth rate, high death rate, low growth rate, in equilibrium Wedge: high birth rate, low death rate, high growth rate, in transition Barrel / beehive: low birth rate, low death rate, low growth rate, in equilibrium

27
Demographic transition
a theory/ model to explain shift from SPIKE to BARREL population pyramids transition from high birth and high death rates to low birth and low death rates often seen in change from rural (poor) to industrialized (wealthy) society Note: changes in birth rate and mortality in infancy and childhood are very important
 to industrialized (wealthy) society. Note: changes in birth rate and mortality in infancy and childhood are very important.")
28
Demographic transition
1. Population has high birth rates and high death rates (particularly at young ages) 2. Death rates begin to fall (improved environmental conditions) 3. Population increases rapidly 4. Birth rates begin to fall but population has increased greatly 5. Population has low birth and death rates
 2. Death rates begin to fall (improved environmental conditions) 3. Population increases rapidly. 4. Birth rates begin to fall but population has increased greatly. 5. Population has low birth and death rates.")
29
Reasons for mortality decline
improved nutrition and food distribution better environmental conditions and sanitation (public health movements of 19th Century) better housing, less overcrowding reduced infectious disease Note medical advances most marked after 1930
 better housing, less overcrowding. reduced infectious disease. Note medical advances most marked after")
30
Tuberculosis mortality over time

32
Dependency ratio the proportion of economically inactive (due to age)
Under 18 plus over 65 years Dependency Ratio* = population aged 18 – 64 years * minimum age varies from maximum age sometimes 60, may rise to 70 Is this a useful measure? Why?

33
Calculating the dependency ratio
Pakistan, which is a developing country, has 41% of its population <15, 4% over 65. 55% between the ages of 15 and 64. 41 + 4 55 Dependency ratio = = 81.8 New Zealand, a developed country, has 23% of its population <15 12% over 65 65% between 15 and 64. 23+12 65 Dependency ratio = = 53.8

34
Predicted changes in Age structure: Scotland 2003 - 2028

35
Predicted changes in factors influencing the dependency ratio

37
Exploring key death rates
Infant mortality rates Under five mortality rates Maternal mortality ratio

38
Infant mortality rate No of deaths of infants aged 0 –1 year
No. of live births for specific time period per 1,000 276 infant deaths * 1,000 55,147 live births in Scotland in 1999 Very useful measure in a population. Often used as an overall summary measure of the health status of a population and indicator of public health standards and consitions. Infant mortality rate 5.0 per 1,000

39
1841 1866 1891 1916 1941 1966 1991

40
Infant mortality rate measure of population’s state of health
general - food, sanitation, overcrowding quality of health care – especially when rates low international indicator UK turn of century: IMR = 140 Sub-Saharan Africa today: IMR = 100 Developed countries today: IMR = 5-10 Very useful measure in a population. Often used as an overall summary measure of the health status of a population and indicator of public health standards and consitions.

41
Comparing the health status of countries
Country Infant mortality rate Per capita health care expenditure (US$) Singapore 2.31 816 France 3.3 2109 UK 4.85 1835 Cuba 5.72 185 US 5.82 4887 Mexico 18.42 370 Morocco 36.88 59 Yemen 54.7 20 Ethiopia 80.8 3 Afghanistan 151.95 8 Angola 180.21 31 2001
 Singapore France UK Cuba US Mexico Morocco Yemen Ethiopia Afghanistan Angola")
42
An alternative measure: under-five mortality
Why is under-five mortality one of the Millenium Development Goals?

43
Millenium Development Goals for 2015
189 Countries – September 2000 – Declartion at the UN

44
Child mortality target: to reduce by two-thirds, between 1990 and 2015, the under five years old mortality rate, from 93 children of every 1,000 dying to 31 of every 1,000

45
% of under 5 deaths by region

46
Factors associated with Child Mortality

47
Evaluation of progress 2010
On track Insufficient progress No progress

48
Maternal mortality ratio
deaths during pregnancy or within 42 days of termination associated with or aggravated by pregnancy expressed per 100,000 live births per year - ratio What does the graph show?

49
Under-5 mortality rate 1970-2013
Lancet, Wang et al 2014

50
Fact sheet 2010 350,000 women die annually from complications during pregnancy or childbirth 99 per cent — in developing countries maternal mortality rate is declining only slowly the vast majority of deaths are avoidable Risk sub-Saharan Africa -1 in 30 developed regions - 1 in 5,600

52
More population measures
fertility rate life expectancy healthy life expectancy PYLL DALY

53
Fertility rates live births per 1,000 women per year
aged 15 – 44 years aged 15 – 49 years age specific fertility rates total period fertility rate

54
Scotland fertility rate 1861-2001

55
Age specific fertility rates E&W 2004
per 1000 Age group

56
Fertility rates in Scotland
Two main findings?

57
Total Period Fertility Rate (TPFR)
the average number of children that would be born to a woman over her lifetime assumes that a woman has the same fertility as the population on average lives beyond the maximum age of giving birth UK: 1.84 TPFR > 2.1 population increasing TPFR < 2.1 population decreasing } why?

58
Age-specific fertility rate per 1,000 women
Calculating TPFR Age Age-specific fertility rate per 1,000 women Rate x 5 years < 20 26.9 134.5 20-24 73.3 366.5 25-29 98.6 493 30- 34 99.4 497 35-39 48.9 244.5 40+ 10.4 52.0 1787.5 1,787.5 per 1000 women TPFR=1.78 (per woman)
")
60
Round the world TPFR Hong Kong 1.02 Japan 1.21 Cuba 1.61 China 1.79
United States 2.05 Ecuador 2.51 Ghana 3.68 Sierra Leone 5.88 Niger 7.75

61
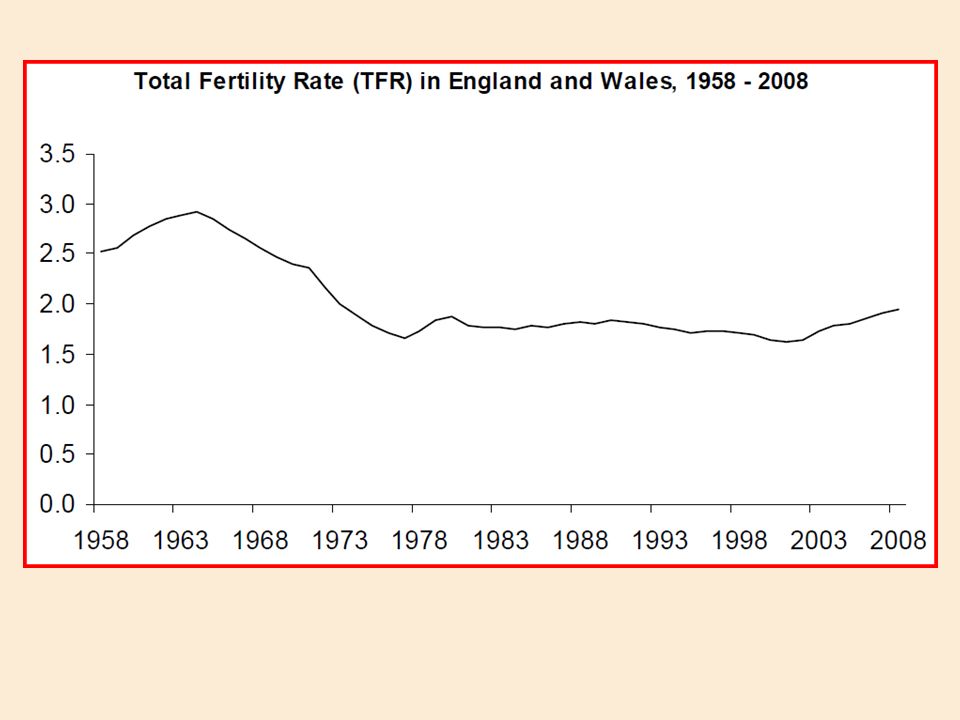
Total period fertility rates

62
Factors associated with high fertility
Poverty Extended family structure Pastoral / agrarian economy Religion Low socio-economic status Ignorance Early marriage Pro-natalist policies

63
Factors associated with low fertility
Affluence Nuclear family structure Industrial economy Religion High socio-economic status Education Deferred marriage Anti-natalist policies

65
Expectation of life at birth: 1861-2001

66
Life expectancy the number of years a baby born today can be expected to live IF it experienced the current age-specific mortality rates an average for the whole population some people will live longer other less apply age specific mortality rates 0-1, 1-4, 5-9, in sequence to a population of 100,000 add up the total number of years lived / 100,000 the calculation is not examinable

67
Male life expectancy Russian Fed 59.4 Belarus 62 Ukraine 62.6 Slovenia 71.9 Chile 72.5 SCOTLAND 72.8 Costa Rica 73.4 Cuba 73.7 England 75.4 Iceland 77.1 Sweden 77.3 Japan 77.5

68
UK Life expectancy 2006 What do these data show? At birth At age 65
Male Female England 77.2 81.5 17.2 19.9 Wales 76.7 81.7 16.9 19.6 Scotland 74.8 79.7 16.0 18.7 Northern Ireland 76.2 81.2 16.8 19.7 What do these data show?

69
Life expectancy at birth, England and Wales, 1980-1982 to 2009-2011

70
Life expectancy at age 65, England and Wales, 1980-1982 to 2009-2011

71
Percentage Change in Life Expectancy, England and Wales 1980-1982 to 2009-2011

73
Healthy life expectancy
expected years of life in good or fairly good general health two types life expectancy in good general health disability-free life expectancy (no long term limiting illness) assumes current patterns of mortality and morbidity remain unchanged calculation similar to life expectancy
 assumes current patterns of mortality and morbidity remain unchanged. calculation similar to life expectancy.")
75
UK Health expectancies
Life expectancy Healthy life expectancy Disability-free life expectancy At birth Male 76.9 68.2 62.4 Female 81.3 70.4 63.0 At age 65 16.9 12.8 10.1 19.7 14.5 10.6 What do these data show?

77
Potential years of life lost: PYLL
a measure of the relative impact of various diseases and lethal forces on society. highlights the loss to society from early deaths. should live to 75 die at 40 lose 35 years JM Last

78
Calculating the PYLL the number of years of life "lost" when a person dies "prematurely" i.e. before age 75 dies at 25, loses 50 years dies at 57, loses 18 years calculate average number lost can use a different maximum age 65, 70 or 85 all causes or death or specific causes cardiovascular cancer

79
PYLL Index Deaths in male due to road traffic accidents in Tayside
: set maximum age at 70 years Age a) Remaining years d) Deaths a) x d) 0-4 67.5 5 337.5 5-9 62.5 3 187.5 10-14 57.5 4 230.0 - 65-69 2.5 10 25.0 Total 3380 Total pop = 192,500 PYLL = 3380 / 192,500 = 17.6 per 1,000
 Remaining. years. d) Deaths. a) x d) Total Total pop = 192,500. PYLL = 3380 / 192,500 = 17.6 per 1,000.")
80
PYLL data: US 2005

81
Disability-adjusted life years (DALYs)
measure of burden of disease extent to which disease reduces healthy years of life 1 DALY= 1 healthy year of life lost calculated for specific diseases

82
DALYs disability plus mortality disability mortality DALY
= incidence x duration x disability mortality years lost through early death DALY = years lost (death) plus years spent with disability (allowing for the amount of disability)
 plus years spent with disability (allowing for the amount of disability)")
83
Adjustment for DALYs example disputed
women lives for 10 years in moderate pain, disability weighting 0.4. Dies 5 years younger than life expectancy DALY= 0.4x = 9 disputed the adjustment for the amount of disability

84
Leading Causes of Mortality and Burden of Disease World, 2004
DALYs % Ischaemic heart disease Cerebrovascular disease Lower respiratory infections COPD Diarrhoeal diseases HIV/AIDS Tuberculosis Trachea, bronchus, lung cancers 2.3 Road traffic accidents Prematurity, low birth weight % Lower respiratory infections 6.2 Diarrhoeal diseases 4.8 Depression 4.3 Ischaemic heart disease 4.1 HIV/AIDS 3.8 Cerebrovascular disease Prematurity, low birth weight 2.9 Birth asphyxia, birth trauma 2.7 Road traffic accidents Neonatal infections and other 2.7 WHO. Global Burden of Disease 2004 Update

85
What you should know Population pyramids Dependency ratio
Infant mortality rate Fertility rates Life expectancies PYLL DALY what they are – definition what they mean – interpretation what influences them

86
No. of deaths from suicide
Mid Pt Years lost No. of deaths from suicide 0-14 yrs 7.5 67.5 3 15-24 yrs 20 55 90 25-34 yrs 167 35-44 yrs 138 45-54 yrs 93 55-64 yrs 70 65-74 yrs 47

87
No. of deaths from suicide
Mid Pt Years lost No. of deaths from suicide 0-14 yrs 7.5 67.5 3 202.5 15-24 yrs 20 55 90 4950 25-34 yrs 30 45 167 7515 35-44 yrs 40 35 138 4830 45-54 yrs 50 25 93 2325 55-64 yrs 60 15 70 1050 65-74 yrs 5 47 235 Total years lost = 21,067.5 Total pop = 5,120,000 PYLL = 21,067.5 ÷ 5,120,000 = 4.12 per 1000

88
Age-specific fertility rates
Rate x 5 < 20 43.0 215 20-25 97.2 486 25-29 112.9 564.5 30-34 118.3 591.5 35-39 55.6 278 40+ 14.4 72 Cumulative birth rate 2,207 per 1000 women TPFR = 2.2 (per woman)
")
Similar presentations