Download presentation
Presentation is loading. Please wait.

1
Perry chapter 13 and Nield-Gehrig chapter 21
Periodontal Surgery Perry chapter 13 and Nield-Gehrig chapter 21

2
Historical Perspective
Originally, surgery was for removing damaged tissues that were thought to be diseased

3
Belief Today Modern belief is that surgery is part of an integral part of most aspects of dental care As severity of periodontitis increases, controlling the disease becomes more difficult Need for periodontal surgery as part of comprehensive patient care becomes more likely Used to support other aspects of care

4
Surgery as Supportive Care
Enhancing restorative procedures Improving patient appearance Preparing a patient for implant-supported prosthesis

5
Indications for Periodontal Surgery

6
Indications Surgery is necessary when the periodontium is unhealthy and cannot be repaired with nonsurgical treatment

7
Indications Provide access for improved root surface debridement
Reduce pocket depths Provide access for treatment of periodontal osseous defects Resect or remove tissues

8
Indications Regenerate periodontium lost because of disease
Graft bone or bone-stimulating materials into osseous defects Improve appearance of the periodontium Enhance prosthetic dental care Allow for placement of a dental implant

9
Provide Access for Improved Instrumentation of Root Surfaces
The deeper the probe depth, the more difficult it is to instrument root surfaces

10
Reduce Pocket Depth Pocket depth can be too deep for adequate daily self-care Plaque thrives in the deeper pockets Surgery reduces pocket depths, making it easier for patients to maintain

11
Provide Access to Osseous Defects
Osseous defect is a deformity in alveolar bone As disease advances, bone loss can change the shape of alveolar bone Surgery can modify the bone level or shape

12
Resect or Remove Tissue
Enlarged gingival tissues are unsightly and can inhibit good oral hygiene Surgery can remove and reshape enlarged gingiva

13
Regenerate Periodontium Lost Because of Disease
Regenerate implies growing back lost cementum, periodontal ligament, and alveolar bone Lost bone and tissue can be regenerated through sophisticated periodontal surgical techniques

14
Graft Bone Into Osseous Defects
Bone or bone-stimulating materials can be grafted into osseous defects Grafting bone does not imply regeneration

15
Improve Appearance of Periodontium
Some gingival levels or contours result in an unattractive smile Surgery can improve the appearance of gingiva

16
Enhance Prosthetic Dental Care
Altering alveolar ridge contours Crown lengthening Augmenting amount of gingiva present Enhancing restorative dentistry Many types of surgery are involved

17
Allow for Placement of Dental Implant
Surgery prepares the site for the implant Implant must be surrounded by sound alveolar bone Edentulous sites are often deficient in bone Some bone augmentation may be necessary before placement of implant

18
Contraindications for
Periodontal Surgery

19
“Relative” Contraindications
Most contraindications for periodontal surgery are relative, meaning each patient is different from all others: Systemic diseases or conditions Totally noncompliant with home care High risk for dental caries Unrealistic expectations for surgical outcomes

20
Systemic Diseases and Conditions
Recent history of heart attack Uncontrolled hypertension Uncontrolled diabetes Certain bleeding disorders Kidney dialysis History of radiation to the jaws HIV infection

21
Totally Noncompliant with Self-Care
Outcomes of many types of surgery depend on the level of patient’s efforts with plaque control Poor self-care can cause an unacceptable periodontal surgical outcome

22
High Risk for Dental Caries
Periodontal surgery can expose portions of tooth roots Patients at risk for dental caries can be devastated with rampant root caries

23
Unrealistic Expectations for Surgical Outcomes
Surgical correction of damage to diseased tissues does not always result in a perfectly restored periodontium Patients have to develop realistic expectations for surgical outcomes

24
Terms Four terms used to describe healing of periodontium after surgery: Repair Reattachment New attachment Regeneration

25
Healing by Repair Healing of a wound by formation of tissue that does not truly restore the original architecture or original function of the body part

26
Healing by Repair Example of repair is a scar
Healing is complete, but the tissue is not completely the same in appearance or function Example of repaired periodontium is healing that takes place after instrumentation Results in a long junctional epithelium

27
Healing by Reattachment
Reattachment is reunion of connective tissue and root that was separated by incision or injury, not disease Moving healthy tissue on a tooth may be necessary to access damaged tissue on an adjacent tooth The healing from this type of incision is reattachment

28
Healing by New Attachment
New attachment describes union of pathologically exposed root with connective tissue or epithelium Occurs when epithelium and connective tissues are newly attached to root where periodontitis previously destroyed the attachment

29
New Attachment vs. Reattachment
New attachment must occur in an area formerly damaged by disease Reattachment occurs when tissues are separated in the absence of disease

30
Healing by Regeneration
Regeneration is a biologic process by which architecture and function of lost tissue are completely restored Tissues look exactly the same as before Reforming of lost cementum, periodontal ligament, alveolar bone

31
Overview of Common Types of Periodontal Surgery
Chapter 21: Periodontal Surgical Concepts for the Dental Hygienist Section 3 Overview of Common Types of Periodontal Surgery

32
Historical Perspectives
Surgery was recommended mainly to remove what was thought to be dead or infected tissue in the periodontium Early procedures were mainly resective

33
Modern Periodontal Surgical Techniques
Resective surgery has limited use Resective surgery is no longer recommended as part of modern periodontal therapy Refinement of goals and techniques for periodontal surgery has taken place Emphasis has shifted from resective surgery to surgical procedures that attempt to regenerate lost periodontal tissues

34
Types of Surgery Periodontal flap Bone replacement graft
Guided tissue regeneration Apically positioned flap with osseous surgery Mucogingival plastic surgery Crown lengthening Dental implant placement Gingivectomy Gingival curettage

35
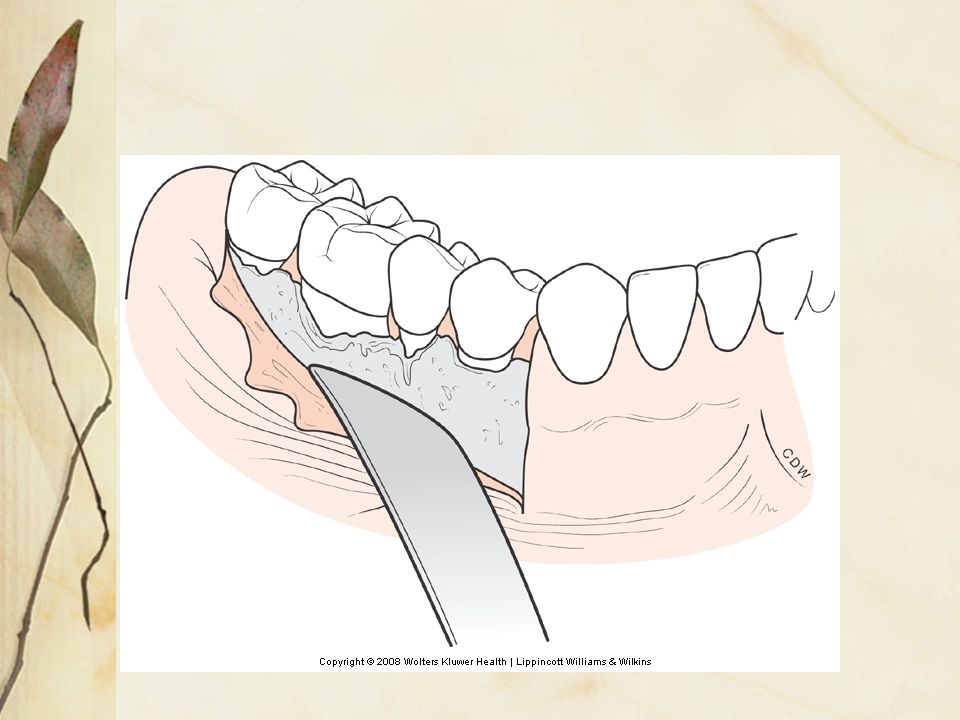
Periodontal Flap for Access

36
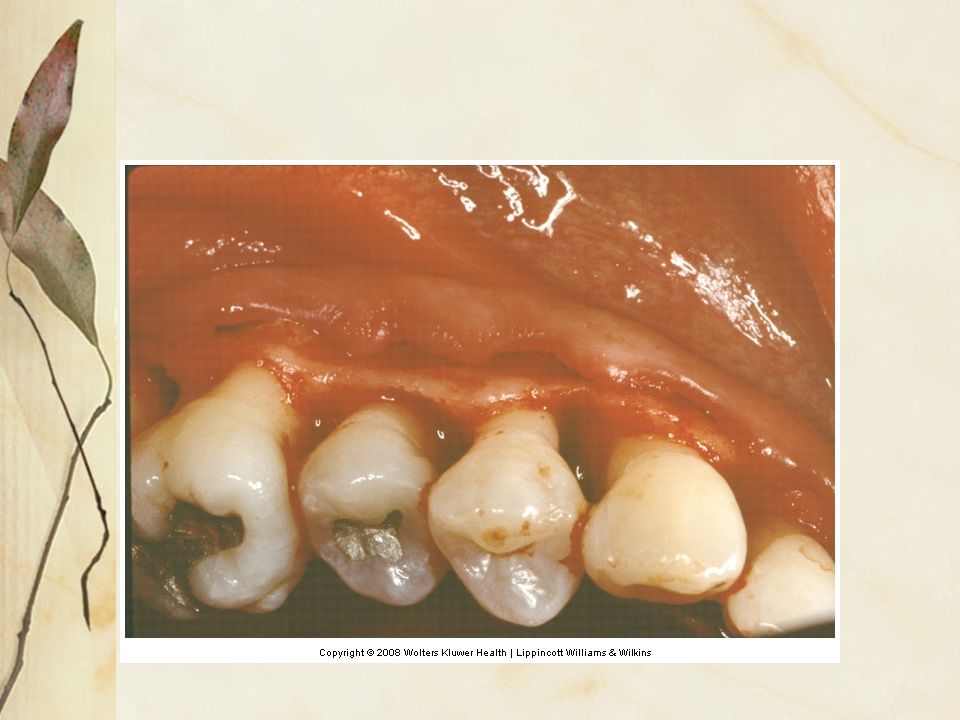
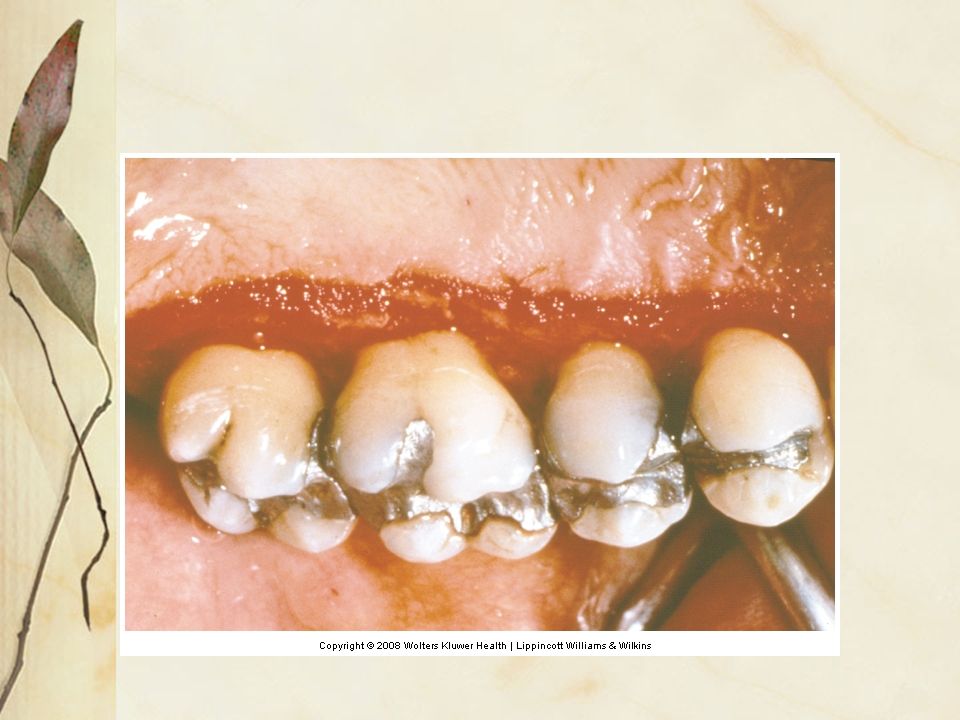
Periodontal Flap Incisions are made in gingiva around necks of teeth
Underlying soft tissues are elevated from tooth roots and bone

37
Indications for Periodontal Flap Surgery
Most periodontal surgical procedures require a flap Performed to provide access for treatment of tooth roots or bone Flap can be elevated for periodontal instrumentation Flap can be elevated to access bone to reshape or fill defects

41
Description of Procedure
Also called modified Widman flap surgery Provides access to tooth roots for improved root preparation Tissue is lifted long enough for procedure After completion of procedure, tissue is replaced at original position Sutured in place

43
Healing After Flap Surgery
Healing by repair Involves formation of long junctional epithelium Can be maintained by patient and professional care

44
Special Considerations for the Dental Hygienist
Pocket depths deeper than 5 to 7 mm Flap for access surgery allows more efficient instrumentation of root surfaces

45
Bone Replacement Graft

46
Description of Procedure
Surgery used to encourage the body to rebuild alveolar bone lost from periodontal disease Involves: Elevation of a flap Cleaning granulation tissue from bone Treating roots as needed Placement of grafting material into defect

48
Materials Used for Bone Replacement
Harvested bone taken from the patient’s jaw Treated bone from cadavers and other species Artificial material that stimulates bone regrowth

49
Materials Used for Bone Grafts
Synthetic bone material Alloplast Treated cow bone Xenograft Taken from a cadaver Allograft Taken from patient’s body; jaw Autograft

50
Healing After Bone Grafting
Partial or complete rebuilding of alveolar bone Reformed bone may not actually be attached to cementum by periodontal ligament fibers

51
Special Considerations for the Dental Hygienist
Site of bone graft should not be disturbed for many months Do not probe until appropriate interval has lapsed Meticulous plaque control is critical to maintain health in the area

53
Guided Tissue Regeneration

54
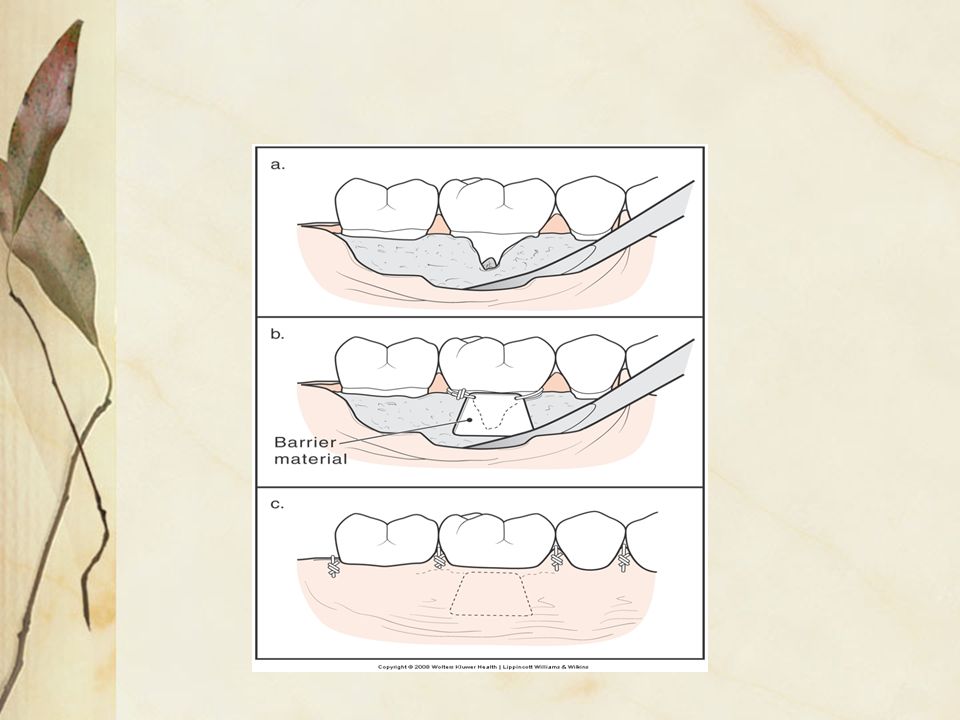
Description of Procedure
Surgical procedure that attempts to regenerate lost periodontal structures Widespread use

55
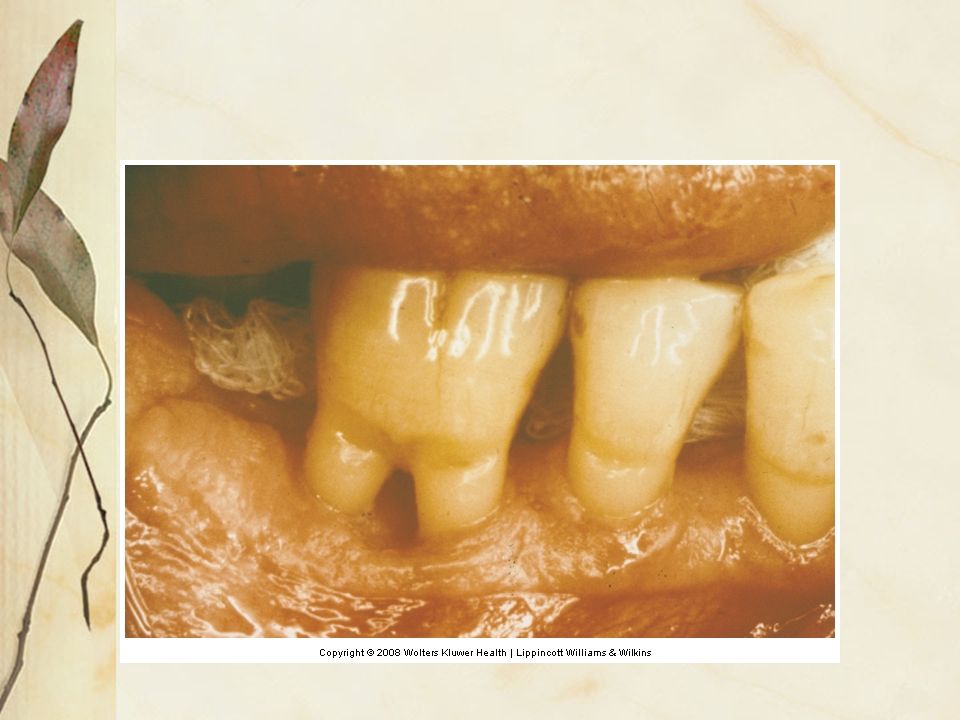
Description of Procedure
Involves: Elevation of flap Cleaning alveolar bone defects Treatment of roots Placement of barrier materials to control rapid growth of epithelium into wound Barrier materials require removal, necessitating a second surgery

56
Healing After Guided Tissue Regeneration
Connective tissue components from the periodontal ligament space provide the cells needed to regrow cementum, periodontal ligament, and alveolar bone Barrier materials prevent epithelial tissue from covering the tooth root too soon

58
Special Considerations for the Dental Hygienist
Effort is made during surgery to close the wound to cover barrier material During postsurgical visit, if part of barrier is exposed, minimize bacterial contamination May suggest topical antimicrobial Do not probe site for several months

59
Apically Positioned Flap

60
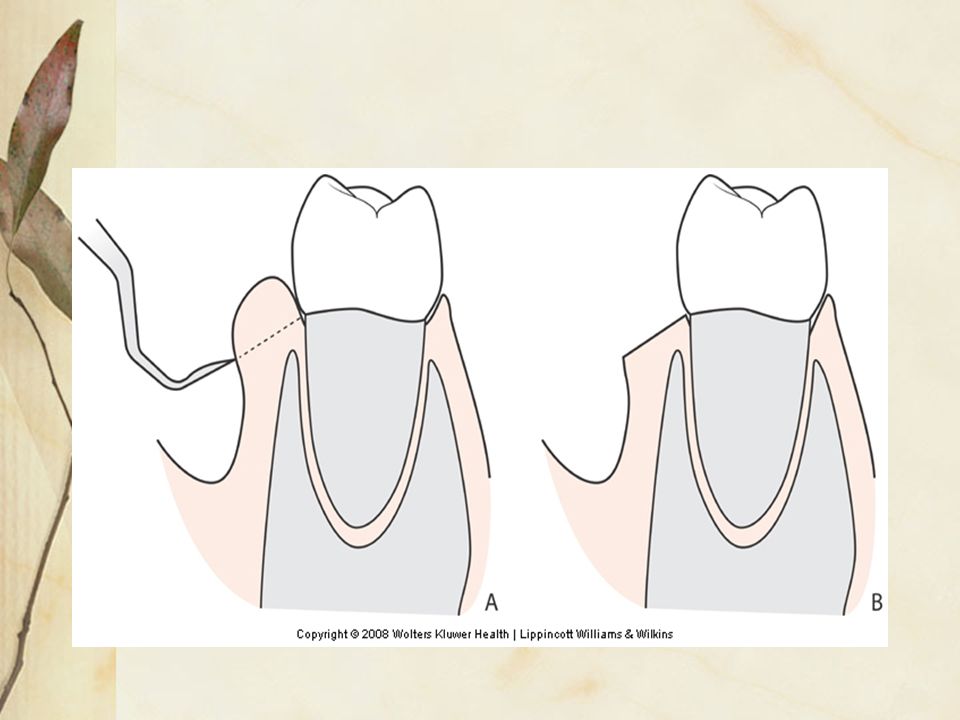
Description of Procedure
Designed to eliminate or minimize pocket depths Involves: Elevation of flap Removal of granulation tissue Treatment of roots Correction of bone contours to mimic healthy alveolar bone

61
Description of Procedure
Flap is sutured in a more apical position to its original level Ideal for minimizing pocket depth in patients with moderate periodontal disease

63
Healing of an Apically Positioned Flap
Results in a stable dentinogingival junction Outcome depends on meticulous home care by the patient combined with professional maintenance visits Final healing results in normal attachment at a more apical position on the root

64
Special Considerations for the Dental Hygienist
Surgery results in more root exposure in the oral cavity Patient may experience temporary root sensitivity

65
Mucogingival Surgery

66
Description of Surgery
Also called periodontal plastic surgery Designed to alter components of attached gingiva Restores gingiva to tooth surface as a result of disease or trauma Removes frenum to deepen vestibule May alter the appearance of the tissue

67
Types of Surgery Soft tissue graft Connective tissue graft
Covering roots because of excessive recession Connective tissue graft Harvesting donor connective tissue (palate) Free gingival graft Harvesting donor tissue that includes both surface epithelium and underlying connective tissue
 Free gingival graft. Harvesting donor tissue that includes both surface epithelium and underlying connective tissue.")
69
Healing After Mucogingival Surgical Procedures
Harvesting from a donor site creates two wounds that have to heal Expected new attachment of grafting material to the tooth root

70
Special Considerations for the Dental Hygienist
Donor site on palate can actually bother the patient more than wound at site Discuss postsurgical discomfort with the patient Do not disturb grafted sites during early stages of healing Encourage patient to maintain good plaque control

71
Crown Lengthening Surgery

72
Description of Procedure
Designed to create longer clinical crown Gingiva is removed from the tooth Alveolar bone is removed from necks of teeth Performed for aesthetics, restorative dental procedures

73
Description of Procedure
Involves: Elevating a flap Recontouring of the bone Suturing tissue back in place

74
Healing After Crown Lengthening Surgery
Similar to apically positioned flap with osseous surgery Results in a normal attachment at a position more apical on root

75
Special Considerations for the Dental Hygienist
Patient may experience some temporary dentinal hypersensitivity Institute measures to deal with sensitivity Encourage patient to maintain meticulous oral hygiene, especially during healing phase May be difficult because mechanical plaque control must be restricted after surgery

76
Dental Implant Placement

77
Description of Procedure
Artificial tooth root placed into alveolar bone to hold a replacement tooth Requires exposure of alveolar bone using flap surgery A precise hole is drilled into bone and metallic implant is inserted Some implants are covered by gingiva during healing

78
Healing Bone growth is in close proximity to implant surface
Implant must be stable enough to support a tooth or dental prosthetic appliance Implants are not surrounded by cementum and ligaments

79
Special Considerations for the Dental Hygienist
Patient self-care is critical After the implant site heals, gingiva can be maintained as usual

80
Gingivectomy

81
Description of Procedure
Surgery designed to remove gingival tissue

83
Indications for Gingivectomy
Use is limited to removing enlarged gingiva to improve esthetics or allow for better access during home care

84
Disadvantages Leaves large open connective tissue wound
Slower surface healing than other surgeries More discomfort for patient during healing Teeth appear longer

86
Healing After Gingivectomy
Normal attachment of the soft tissues to the tooth root Attachment is more apical in position than original level Teeth appear longer

87
Special Considerations for the Dental Hygienist
Healing phase can be very uncomfortable for patient Can be managed with a periodontal dressing over the wound Prescribe analgesics Dressing may need to be changed at several postsurgical visits until total epithelization has occurred

88
Gingival Curettage

89
Description of Procedure
Involves an attempt to scrape away lining of the periodontal pocket with a curette Benefits of this procedure are the same as periodontal instrumentation and meticulous plaque control No longer a recommended procedure

90
Management of the Patient Following Periodontal Surgery
Chapter 21: Periodontal Surgical Concepts for the Dental Hygienist Section 4 Management of the Patient Following Periodontal Surgery

91
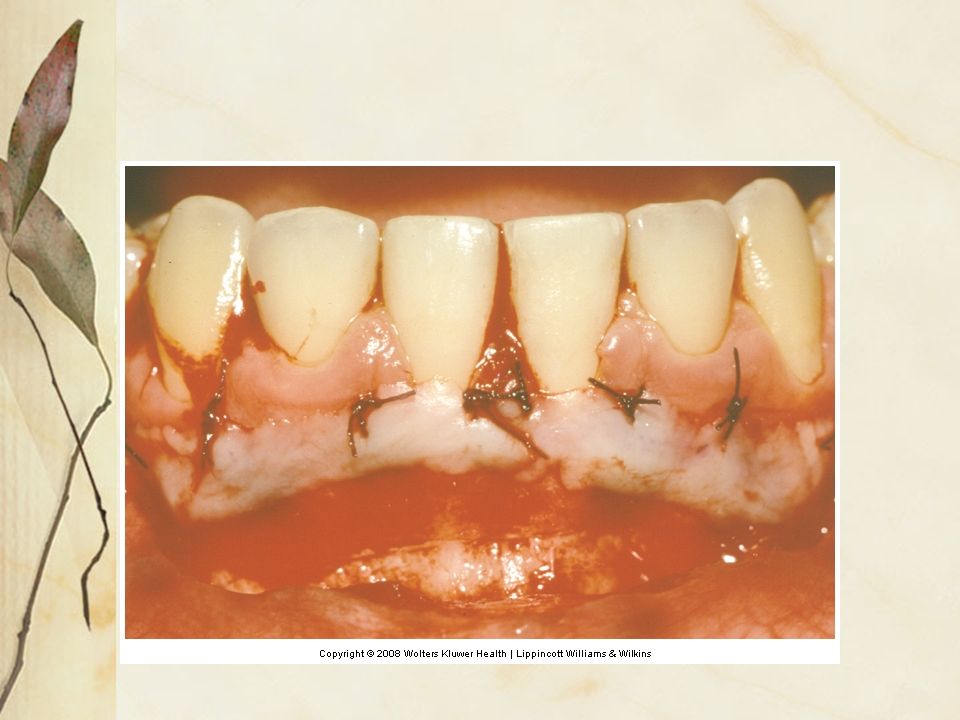
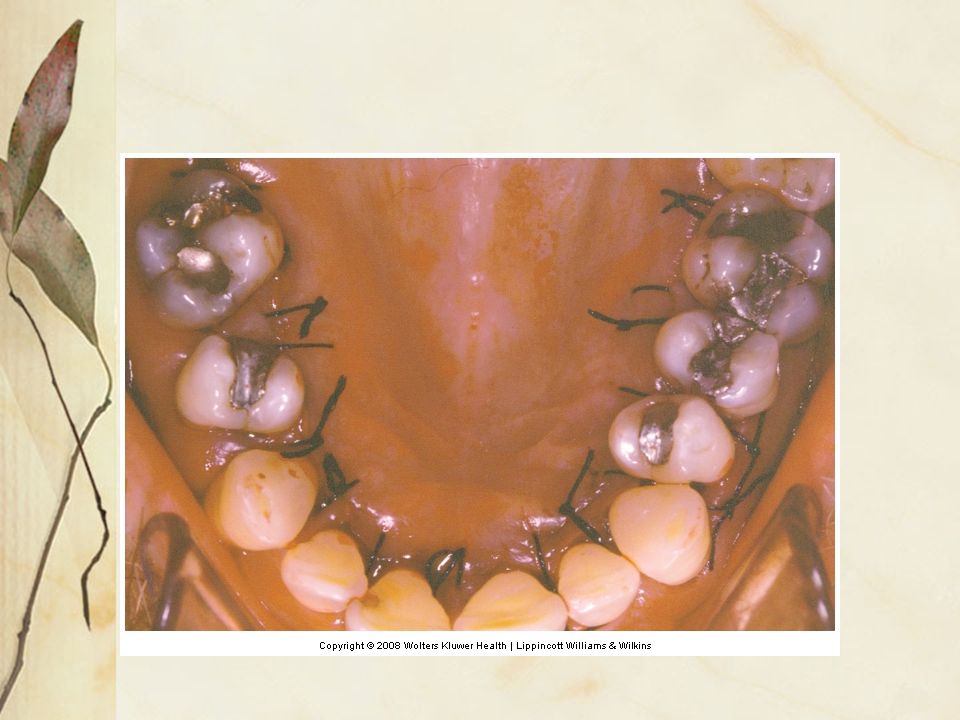
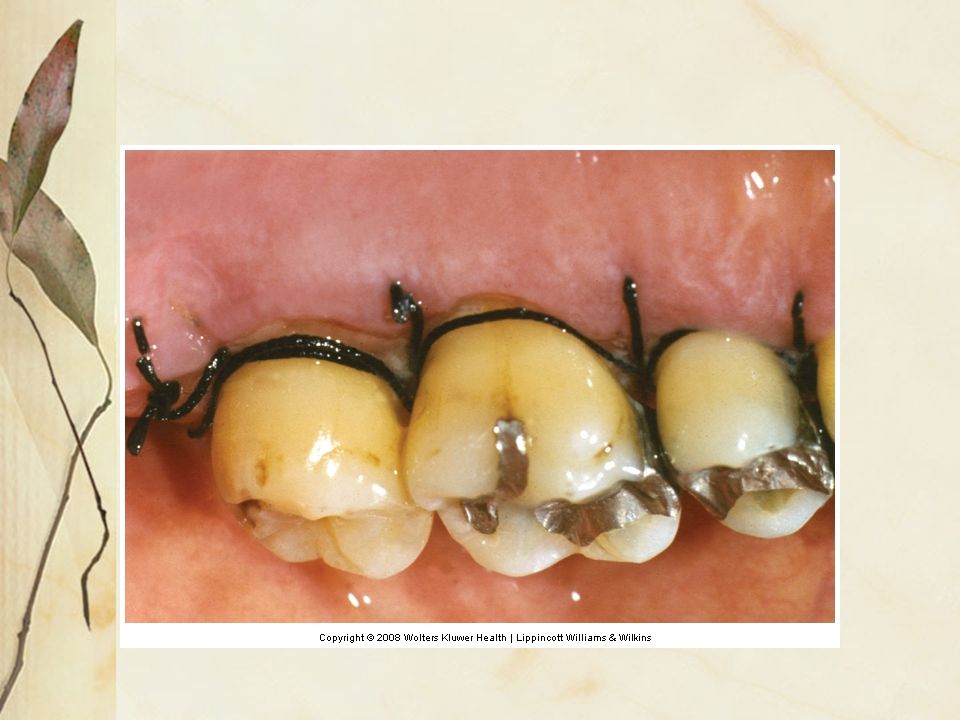
Suture Placement and Removal

92
Purpose of Sutures Sutures stabilize the position of the soft tissues during early phases of healing A suture is a stitch taken to repair an incision, tear, or wound

93
Material Used Nonresorbable Resorbable
Does not dissolve in body fluids and must be removed by a clinician Resorbable Dissolves slowly in body fluids and does not need to be removed

97
Suture Removal Nonresorbable sutures placed during surgical procedures are removed as part of routine postsurgical visits Remnants of resorbable sutures are removed to avoid inflammation Sutures should be removed when they are loose in the tissues

98
Suture Removal Sutures are usually loose in the tissue 1 week after surgery Sutures should not be left in place longer than 2 weeks They become irritants if left in the tissue too long

99
Suture Removal Guidelines
Count the number of sutures placed and enter it in the treatment notes Assures the correct number is removed Write suture size in treatment notes: 3-0, 4-0, 5-0 3-0 is largest; 5-0 smallest

100
Suture Removal Guidelines
Sutures are removed by cutting material near the knot and grasping the knot with pliers Gently pull through the tissue Usually not painful for the patient

102
Periodontal Dressing Placement

103
Surgical Wound Dressing
Periodontal surgical wound dressing Material from two tubes is mixed together for a putty-like consistency Light-cured gel Does not stick to the tissue Is retained by pressing firmly interdentally

104
Surgical Wound Dressing
Use the least amount possible Just enough to cover the wound Should be no dressing on occlusals Take care not to trap sutures in dressing

106
Post Surgical Instructions

107
Postsurgical Instructions
Supplying the patient with both verbal and written instructions minimizes confusion Restrict mechanical plaque removal Encourage patient to take medications as prescribed

108
Postsurgical Instructions
Advise the patient to chew food in such a way that it does not disturb the surgical site Manage facial swelling Supply patient with an emergency number in case excessive bleeding occurs

109
Post Surgical Visits

110
Postsurgical Visits Patients are usually seen in 5 to 7 days for the first postsurgical visit It is the dentist’s responsibility to manage postsurgical problems The dental hygienist performs most of the postsurgical management

111
Step 1 Interview the patient about:
Pain experience and use of analgesics If antibiotic prescriptive instructions were followed Swelling Postsurgical bleeding Sensitivity to cold

112
Step 2 Take patient’s vital signs:
Blood pressure Pulse Temperature Elevated temperature may indicate a developing infection

113
Step 3 Remove periodontal dressing and examine surgical site
Rinse site with warm, sterile saline solution Use cotton-tipped applicator to remove debris adherent to teeth, soft tissue, or sutures Swelling or exudate indicates an infection

114
Step 4 Cut sutures and remove using sterile scissors

115
Step 5 Plaque accumulation is likely Remove plaque from surgical area

116
Step 6 Replace periodontal dressing, if indicated
Discontinue dressing as soon as patient is able to resume mechanical plaque control

117
Step 7 Instruct patient in self-care
Use brushes with extra soft bristles May introduce additional self-care aids

118
Step 8 Reappoint for second postsurgical visit
Usually 2 to 3 weeks after surgery

Similar presentations