Download presentation
Presentation is loading. Please wait.

1
Meaningful Use Last Updated: September 23, 2011

2
Year 1, Stage 1 MU Information contained in this presentation pertains only to Year 1, Stage 1 of Meaningful Use Information was obtained from the CMS website and the IHS website All information is based on the Final Rule. ( http://edocket.access.gpo.gov/2010/pdf/2010-17207.pdf) http://edocket.access.gpo.gov/2010/pdf/2010-17207.pdf

3
Today’s Objectives Meaningful Use EHR Certification Eligible Professionals & Eligible Hospitals Incentives/Penalties Patient Volume Performance Measures Clinical Quality Measures MU Resources MU Reports CMS Incentive Program Registration Contacts

4
Electronic Health Record (EHR) Incentive Program Overview
 Incentive Program Overview")
5
MEANINGFUL USE

6
What is Meaningful Use? Meaningful Use is using certified EHR technology to: Improve quality, safety, efficiency, and reduce health disparities Engage patients and families in their health care Improve care coordination Improve population and public health All the while maintaining privacy and security

7
MEDICARE EHR Incentive Program MEDICAID EHR Incentive Program Implemented by the Federal Government and started January 3, 2011 Voluntary for States to implement - Most are expected to start by late summer 2011 Program ends in 2016 Must initiate participation by 2014 Must participate by 2012 to receive the maximum incentive payment Program ends in 2021 Must initiate participation by 2016 Must participate by 2016 to receive the maximum incentive payment Medicare payment reductions begin in 2015 for EH/EPs who do not demonstrate MU of certified EHR technology No Medicaid payment reductions Must demonstrate MU in Year 1 over a consecutive 90-day report period A/I/U option for Year 1 No patient volume requirementMust meet patient volume thresholds

8
Meaningful Use: Definition of A/I/U Adopt: Acquire, purchase, or secure access to certified EHR technology Implement: Install or commence utilization of certified EHR technology capable or meeting MU requirements Upgrade: Expand the available functionality of certified EHR technology capable of meeting MU requirements at the practice site, including staffing, maintenance, and training or upgrade from existing EHR technology to certified EHR technology per the ONC EHR certification criteria

9
Meaningful Use: State Options May add 4 additional core performance measures: Generate lists of patients by specific conditions for quality improvement, reduction of disparities, research, or outreach (can specify particular conditions) Reporting to immunization registries Reportable lab results Syndromic surveillance (can specify for their providers how to test the data submission and to which specific destination) May propose a different Patient Volume method is used instead of or in addition to the CMS-defined methods NOTE: CMS must review and approve all performance measure and patient volume changes
 Reporting to immunization registries Reportable lab results Syndromic surveillance (can specify for their providers how to test the data submission and to which specific destination) May propose a different Patient Volume method is used instead of or in addition to the CMS-defined methods NOTE: CMS must review and approve all performance measure and patient volume changes")
10
Meaningful Use: Stages of Meaningful Use 3 stages of Meaningful Use Requirements will increase over time…more work lies ahead Stage 1 2011-2012 Stage 2 2013-2014 Stage 3 2015+

11
EHR CERTIFICATION

12
EHR Certification: Process Creates EHR Certification Test Creates EHR Certification Requirements Creates MU Requirements Authorized Testing and Certification Body

13
EHR Certification: Key Points A certified EHR is required to demonstrate meaningful use EHR Certification demonstrates that the EHR is standardized and interoperable RPMS-EHR was certified by InfoGard on April 1, 2011 The certified version RPMS-EHR was released in June 2011 Further enhancements ongoing. The EHR certification number can be obtained at: http://onc-chpl.force.com/ehrcert http://onc-chpl.force.com/ehrcert

14
Name Space Package or ApplicationVersionPatchRelease Date AGPatient Registration7.1912/3/10 APCLExport3.02711/10/10 APSPPharmacy MOD-ePrescribing (eRx)7.010104/29/11 BGPClinical Reporting System (CRS)11.036/22/11 BJMDC321.016/24/11 BJPCPCC Mgmt Reporting2.066/2/11 BMCReferred Care Information System (RCIS) 4.075/12/11 BQIiCare2.13/11/11 BRNRelease of Information (ROI)2.034/13/11 BYIMImmunization Exchange Message2.0012/24/11 BGOElectronic Health Record (EHR)1.1806/10/11 LRLab5.21027 or 372 or 33412/07/10 PXRMEHR Reminders1.510074/13/10 BPHRPersonal Health Record (PHR)1.06/22/11 Central Ensemble2009.1.6921.0.104142011 GuardianEdge/ Symantec8.03/31/11 IPSEC (Windows)2010 VanDyke (AIX)2010 WinHasher1.62011 Universal Client or HIE Viewer The URL to access the application is http://ditdev4.d1.na.ihs.gov:9090/DocViewer http://ditdev4.d1.na.ihs.gov:9090/DocViewer 1.04/27/11
 /29/11 BGPClinical Reporting System (CRS)11.036/22/11 BJMDC /24/11 BJPCPCC Mgmt Reporting2.066/2/11 BMCReferred Care Information System (RCIS) 4.075/12/11 BQIiCare2.13/11/11 BRNRelease of Information (ROI)2.034/13/11 BYIMImmunization Exchange Message2.0012/24/11 BGOElectronic Health Record (EHR)1.1806/10/11 LRLab or 372 or 33412/07/10 PXRMEHR Reminders /13/10 BPHRPersonal Health Record (PHR)1.06/22/11 Central Ensemble GuardianEdge/ Symantec8.03/31/11 IPSEC (Windows)2010 VanDyke (AIX)2010 WinHasher Universal Client or HIE Viewer The URL to access the application is /27/11")
15
EHR Certification: EHR Certification Number* Inpatient Certification #: 30000002ELL6EAI Ambulatory Certification #: 0000002EJKDEAI *The number will be entered during CMS registration and attestation

16
EHR Certification: Vendor Letter Request Vendor Letter on the IHS MU website at http://www.ihs.gov/meaningfuluse/index.cfm?module=steps_request_letter http://www.ihs.gov/meaningfuluse/index.cfm?module=steps_request_letter Enter information in each of the fields on the webpage Click the “Submit” button IHS will process the request for each facility IHS will issue a letter to the requesting practice within 10 business days of the initial request The facility will receive the signed IHS EHR Vendor Letter via email The letter will be emailed to the individual that made the request

17
ELIGIBLE PROFESSIONALS

18
Eligible Professionals: Medicare & Medicaid Comparison Medicare-only Eligible Professionals Could be eligible for both Medicare & Medicaid incentives Medicaid-only Eligible Professionals Professionals may be eligible for both Medicare & Medicaid, but can only participate in one program at a time

19
Eligible Professionals: Overview Must choose the Medicare OR Medicaid incentive program; not eligible for both Payments for Eligible Professionals are based on a calendar year Incentives are based on the individual, not the practice Hospital-based EPs are NOT eligible for incentives 90% or more of their covered professional services in either an inpatient or emergency room (Place of Service codes 21 or 23) of a hospital Eligibility determined by law EPs may switch programs anytime prior to first payment After an EP receives a payment they may switch one time before 2015
 of a hospital Eligibility determined by law EPs may switch programs anytime prior to first payment After an EP receives a payment they may switch one time before 2015")
20
Eligible Professional: Incentive Program Timeline CY 2011CY 2012 01/01/11First day of calendar & EHR reporting year01/01/12 09/30/11 LAST day to establish clean-date for the Medicare Incentive Program 09/30/12 10/03/11 LAST day to begin 90-day reporting period for the Medicare Incentive Program 10/01/12 12/31/11Last day of calendar & EHR reporting year12/31/13 02/29/12 LAST day to register & LAST day to attest 02/28/13

21
ELIGIBLE PROFESSIONALS & MEDICAID

22
Eligible Professionals & Medicaid: Participation Requirements Year One A/I/U Meet patient volume threshold (previous year) Year Two+ Meet MU Requirements Meet patient volume threshold (previous year) Note: Medicare does not have a patient volume threshold
 Year Two+ Meet MU Requirements Meet patient volume threshold (previous year) Note: Medicare does not have a patient volume threshold")
23
Eligible Professionals & Medicaid: Patient Volume Threshold Eligible Professional (EP) If EP does not practice predominantly at FQHC/RHC: Minimum Medicaid patient volume thresholds If EP does practice predominantly at FQHC/RHC*: Minimum needy individual patient volume thresholds Physicians30% - Pediatricians20%30% Dentists30% Certified Nurse- Midwives 30% NPs30% PAs practicing at an FQHC/RHC that is led by a PA N/A30% * All Tribal clinics are deemed FQHC/RHC for the CMS incentive program
 If EP does not practice predominantly at FQHC/RHC: Minimum Medicaid patient volume thresholds If EP does practice predominantly at FQHC/RHC*: Minimum needy individual patient volume thresholds Physicians30% - Pediatricians20%30% Dentists30% Certified Nurse- Midwives 30% NPs30% PAs practicing at an FQHC/RHC that is led by a PA N/A30% * All Tribal clinics are deemed FQHC/RHC for the CMS incentive program")
24
Eligible Professionals & Medicaid: Medicaid Encounter For calculating Medicaid patient volume, a “Medicaid encounter” means services rendered to an individual on any one day where Medicaid (or a Medicaid demonstration project approved under section 1115 of the Act) paid for all or part of: The service; or Their premiums, co-payments, and/or cost-sharing Patient volume calculation options include: Individual EP Group Practice Patient panel*
 paid for all or part of: The service; or Their premiums, co-payments, and/or cost-sharing Patient volume calculation options include: Individual EP Group Practice Patient panel*")
25
Eligible Professionals & Medicaid: Needy Patient Encounter For calculating needy individual patient volume, a “needy patient encounter” means services rendered to an individual on any one day where: Medicaid or CHIP (or a Medicaid or CHIP demonstration project approved under section 1115 of the Act) paid for all or part of: The service; or Their premiums, co-payments, and/or cost-sharing; or The services were furnished at no cost; or The services were paid for at a reduced cost based on a sliding scale determined by the individual’s ability to pay Patient volume calculation options include: Individual EP Group Practice Patient panel*
 paid for all or part of: The service; or Their premiums, co-payments, and/or cost-sharing; or The services were furnished at no cost; or The services were paid for at a reduced cost based on a sliding scale determined by the individual’s ability to pay Patient volume calculation options include: Individual EP Group Practice Patient panel*")
26
ELIGIBLE PROFESSIONALS INCENTIVES

27
Eligible Professionals: Summary of Medicare & Medicaid Incentives MEDICAREMEDICAID Incentives Start CY 2011 Incentives End CY 2016 (max. 5 years, must start by 2014) 2021 (max. 6 years, must start by 2016) Incentive Amount Up to $44,000 total per provider Based on % Medicare claims Additional 10% bonus for EP’s in HPSAs Up to $63,750 total per provider Reimbursement Reduced CY 2015No penalties
 2021 (max. 6 years, must start by 2016) Incentive Amount Up to $44,000 total per provider Based on % Medicare claims Additional 10% bonus for EP’s in HPSAs Up to $63,750 total per provider Reimbursement Reduced CY 2015No penalties.")
28
Eligible Professionals: Medicare Incentive Payments Incentive amount based on 75% Fee-for-Service allowable charges Maximum incentive is $44,000 over 5 years Extra 10% bonus amount available for practicing predominantly in a Health Professional Shortage Area (HPSA) HPSA identifies, by zip code or county, areas lacking sufficient clinicians to meet primary care needs Incentives decrease if starting after 2012 Must begin by 2014 to receive incentive payments Last payment year is 2016 Receive one (1) incentive payment per year
 HPSA identifies, by zip code or county, areas lacking sufficient clinicians to meet primary care needs Incentives decrease if starting after 2012 Must begin by 2014 to receive incentive payments Last payment year is 2016 Receive one (1) incentive payment per year")
29
Eligible Professionals: Medicare Incentive Payment Example Amount of Payment Each Year of Participation Calendar Year EP Receives a Payment CY 2011CY 2012CY 2013CY2014 CY 2015 and later CY 2011$18,000 CY 2012$12,000$18,000 CY 2013$8,000$12,000$15,000 CY 2014$4,000$8,000$12,000 CY 2015$2,000$4,000$8,000 $0 CY 2016$2,000$4,000 $0 TOTAL$44,000 $39,000$24,000$0

30
Eligible Professionals: Medicaid Incentive Payments Maximum incentive is $63,750 over 6 years The first year payment is $21,250 No extra bonus for health professional shortage areas available Incentives are same regardless of start year Must begin by 2016 to receive incentive payments Incentives available through 2021 Receive one (1) incentive payment per year
 incentive payment per year")
31
Eligible Professionals: Medicaid Incentive Payment Example Amount of Payment Each Year if Continues Meeting Requirements 1 st Calendar Year EP Receives a Payment CY 2011CY 2012CY 2013CY 2014CY 2015CY 2016 CY 2011$21,250 CY 2012$8,500$21,250 CY 2013$8,500 $21,250 CY 2014$8,500 $21,250 CY 2015$8,500 $21,250 CY 2016$8,500 $21,250 CY 2017$8,500 CY 2018$8,500 CY 2019$8,500 CY 2020$8,500 CY 2021$8,500 TOTAL$63,750

32
Eligible Professionals: Incentive Payments IHS EP’s must re-assign incentive payments to their facility; Tribal EPs should consult with their Tribal/facility leadership EP’s who achieve MU by combining services from multiple sites or states, may only assign their payment to one entity in one state Medicare payments, in the first year of demonstrating MU, a payment will be made when the EP reaches his/her minimum allowable charges or the end of the year, whichever comes first Medicaid payments, in the first year, will be issued within 5 months after registering

33
ELIGIBLE PROFESSIONALS PERFORMANCE MEASURES & CLINICAL QUALITY MEASURES

34
Eligible Professionals: Meaningful Use Requirements STAGE 1: Meaningful Use Requirements 20 total Performance Measures 15 core performance measures* 5 performance measures out of 10 from menu set* 6 total Clinical Quality Measures 3 core or alternate core clinical quality measures 3 clinical quality measures out of 38 from menu set * Most measures require achievement of a performance target

35
1.>30%: Computerized physician order entry (CPOE): 2. >40%: E-Prescribing (eRX) 3.Yes/No: Report ambulatory clinical quality measures to CMS or States 4.Yes/No: Implement one clinical decision support rule 5.>50%: Provide patients with an electronic copy of their health information, upon request 6.>50%: Provide clinical summaries for patients for each office visit 7.Yes/No: Implement drug-drug and drug-allergy interaction checks during the entire EHR reporting period 8.>50%: Record demographics 9.>80%: Maintain an up-to-date problem list of current & active diagnoses 10.>80%: Maintain active medication list 11.>80%: Maintain active medication allergy list 12.>50%: Record and chart changes in vital signs 13.>50%: Record smoking status for patients 13 years or older 14.Yes/No: Capability to exchange key clinical information (Test Performed) 15. Yes/No: Conduct or review a security risk analysis Eligible Professionals: 15 Core Performance Measures
 3.Yes/No: Report ambulatory clinical quality measures to CMS or States 4.Yes/No: Implement one clinical decision support rule 5.>50%: Provide patients with an electronic copy of their health information, upon request 6.>50%: Provide clinical summaries for patients for each office visit 7.Yes/No: Implement drug-drug and drug-allergy interaction checks during the entire EHR reporting period 8.>50%: Record demographics 9.>80%: Maintain an up-to-date problem list of current & active diagnoses 10.>80%: Maintain active medication list 11.>80%: Maintain active medication allergy list 12.>50%: Record and chart changes in vital signs 13.>50%: Record smoking status for patients 13 years or older 14.Yes/No: Capability to exchange key clinical information (Test Performed) 15. Yes/No: Conduct or review a security risk analysis Eligible Professionals: 15 Core Performance Measures.")
36
1.Yes/No: Implement drug-formulary checks for entire EHR reporting period 2.>40%: Incorporate clinical lab test results as structured data 3.Yes/No: Generate lists of patients by specific conditions 4.>10%: Use certified EHR technology to identify patient-specific education resources and provide to patient, if appropriate 5.>50%: Medication reconciliation at transitions of care 6.>50%: Summary of care record for each transition of care/referrals 7.Yes/No: Capability to submit electronic data to immunization registries/systems* (Test Performed) 8.Yes/No: Capability to provide electronic syndromic surveillance data to public health agencies* (Test Performed) 9.>20%: Send reminders to patients per patient preference for preventive/follow up care 10.>10%: Provide patients with timely electronic access to their health information (within 4 business days) *At least 1 public health measure must be selected Eligible Professionals: 10 Menu Performance Measures (Pick 5)
 8.Yes/No: Capability to provide electronic syndromic surveillance data to public health agencies* (Test Performed) 9.>20%: Send reminders to patients per patient preference for preventive/follow up care 10.>10%: Provide patients with timely electronic access to their health information (within 4 business days) *At least 1 public health measure must be selected Eligible Professionals: 10 Menu Performance Measures (Pick 5)")
37
Eligible Professionals: Clinical Quality Measures Core Set: If denominator = 0, must report on the Alternate Core measures NQF Measure Number & PQRI Implementation Number Clinical Quality Measure Title NQF 0013Hypertension: Blood Pressure Measurement NQF 0028Preventive Care and Screening Measure Pair: a) Tobacco Use Assessment, b) Tobacco Cessation Intervention NQF 0421 PQRI 128 Adult Weight Screening and Follow-up NQF Measure Number & PQRI Implementation Number Clinical Quality Measure Title NQF 0024Weight Assessment and Counseling for Children and Adolescents NQF 0041 PQRI 110 Preventive Care and Screening: Influenza Immunization for Patients 50 Years Old or Older NQF 0038Childhood Immunization Status Alternate Core Set
 Tobacco Use Assessment, b) Tobacco Cessation Intervention NQF 0421 PQRI 128 Adult Weight Screening and Follow-up NQF Measure Number & PQRI Implementation Number Clinical Quality Measure Title NQF 0024Weight Assessment and Counseling for Children and Adolescents NQF 0041 PQRI 110 Preventive Care and Screening: Influenza Immunization for Patients 50 Years Old or Older NQF 0038Childhood Immunization Status Alternate Core Set")
38
Eligible Professionals: 38 Additional Clinical Quality Measures (Choose 3) Diabetes: (9) Heart Failure (HF): (3) Coronary Artery Disease (CAD): (3) Pneumonia Vaccination Status for Older Adults Anti-depressant medication management: (2) Primary Open Angle Glaucoma (POAG): Optic Nerve Evaluation Asthma: (3) Appropriate Testing for Children with Pharyngitis Cancer Prevention and/ or Oncology: (6) Smoking and Tobacco Use Cessation,(3) Ischemic Vascular Disease (IVD): (3) Initiation and Engagement of Alcohol and Other Drug Dependence Treatment: (2) Prenatal Care: (2) Controlling High Blood Pressure Chlamydia Screening for Women Low Back Pain: Use of Imaging Studies
 Diabetes: (9) Heart Failure (HF): (3) Coronary Artery Disease (CAD): (3) Pneumonia Vaccination Status for Older Adults Anti-depressant medication management: (2) Primary Open Angle Glaucoma (POAG): Optic Nerve Evaluation Asthma: (3) Appropriate Testing for Children with Pharyngitis Cancer Prevention and/ or Oncology: (6) Smoking and Tobacco Use Cessation,(3) Ischemic Vascular Disease (IVD): (3) Initiation and Engagement of Alcohol and Other Drug Dependence Treatment: (2) Prenatal Care: (2) Controlling High Blood Pressure Chlamydia Screening for Women Low Back Pain: Use of Imaging Studies")
39
Eligible Professionals: Meaningful Use Summary MedicareMedicaid Year 1 (Stage 1): AIU to a certified EHR AND demonstrate MU for a 90 day consecutive period Year 2+: demonstrate MU for the entire year Year 1: AIU to a certified EHR Year 2 (Stage 1): demonstrate MU for a 90 day consecutive period Year 3+ (Stage 1): demonstrate MU for the entire year For Stage 1, report on a total of 20 performance measures 15 core measures and 5 measures from menu set of 10 Note: There are performance targets on most measures For Stage 1, report on a total of 6 clinical quality measures 3 core/alternate core measures and 3 menu set If the denominator for any of the 3 core measures is zero, must report on the 3 alternate core measures. If all 6 of the measures have a denominator of zero, the EP must still report on any 3 menu set measures shown in the menu set. Note: There are no performance targets

40
ELIGIBLE HOSPITALS

41
Hospitals only eligible for Medicare incentive Could be eligible for both Medicare & Medicaid (most hospitals) Hospitals only eligible for Medicaid incentive Eligible Hospitals: Medicare & Medicaid Comparison
 Hospitals only eligible for Medicaid incentive Eligible Hospitals: Medicare & Medicaid Comparison")
42
Eligible Hospitals: Overview IHS hospitals are eligible to participate in both the Medicare and Medicaid incentive programs Payments for Eligible Hospitals are based on the federal fiscal year Eligible IHS Hospitals include: Subsection-D/Acute Care Hospitals Critical Access Hospitals CMS recommends hospitals register for both programs Even if the hospital is unsure if the will meet the Medicaid patient volume requirements

43
Eligible Hospitals: Incentive Program Timeline FY 2011FY 2012 First day of calendar & EHR reporting year 10/01/11 06/30/11 LAST day to establish clean-date for the Medicare Incentive Program 06/30/12 07/03/11 LAST day to begin 90-day reporting period for the Medicare Incentive Program 07/01/12 09/30/11 Last day of calendar & EHR reporting year 09/30/12 11/30/11 LAST day to register & LAST day to attest 11/30/12

44
Eligible Hospitals: Medicare Program Requirements Medicare Program YearReporting periodMU Stage One90 dayS1-Y1 Two365 dayS1-Y2 Three365 dayS2- Y1 Four+365 dayS2- Y2

45
Eligible Hospitals: Medicaid Program Requirements Medicaid Program Participation Year Reporting periodMU Stage OneN/A (A/I/U)N/A Two90 dayS1-Y1 Three365 dayS1-Y2 Four+365 dayS2- Y1
N/A Two90 dayS1-Y1 Three365 dayS1-Y2 Four+365 dayS2- Y1")
46
Eligible Hospitals: Dual-Eligible Hospital Medicare & Medicaid (Same Year) YearMedicaid EHR Reporting period Medicare EHR Reporting period MU Stage OneA/I/U90 dayS1-Y1 Two365 day S1-Y2 Three365 day S2- Y1 Four+365 day S2- Y2
 YearMedicaid EHR Reporting period Medicare EHR Reporting period MU Stage OneA/I/U90 dayS1-Y1 Two365 day S1-Y2 Three365 day S2- Y1 Four+365 day S2- Y2")
47
Eligible Hospitals: Option Two Start Medicaid & Delay Medicare YearMedicaid EHR Reporting period Medicare EHR Reporting period MU Stage OneA/I/UDelayN/A Two90 day S1-Y1 Three365 day S1-Y2 Four+365 day S2- Y1

48
Eligible Hospitals: Option Three Start Medicare & Opt-Out A/I/U Medicaid YearMedicaid EHR Reporting period Medicare EHR Reporting period MU Stage OneOpt-Out90 dayS1-Y1 Two365 day S1-Y2 Three365 day S2- Y1 Four+365 day S2- Y2

49
ELIGIBLE HOSPITALS & MEDICAID

50
Eligible Hospitals: Medicaid Patient Volume Requirement Eligible HospitalsMinimum Medicaid patient volume threshold Acute care hospitals, including Critical Access Hospitals 10% Note: Medicare does not have a patient volume threshold

51
Eligible Hospitals: Medicaid Patient Volume Calculation 1 main option for calculating patient volume Medicaid Encounters State picks can use this method or propose a new method for review and approval If CMS approves a method for one state, it may be considered an option for all states

52
Eligible Hospital: Medicaid Encounter Definition For calculating Medicaid patient volume, a “Medicaid encounter” means services rendered to an individual where Medicaid (or a Medicaid demonstration project approved under section 1115 of the Act) paid for part or all of: Service per inpatient discharges, Premiums, co-payments, and/or cost-sharing per inpatient discharge Service in an emergency department* on any one day, or, Their premiums, co-payments, and/or cost sharing in an emergency department* on any one day. *An emergency department must be part of the hospital under the qualifying CCN

53
HOSPITAL INCENTIVES

54
Eligible Hospitals: Medicare & Medicaid Incentive Summary MEDICAREMEDICAID Incentives Start FY 2011 Incentives End FY 2016 (max. 4 years, must start by 2015) 2021 (max. 6 years, must start by 2016) Incentive Amount Varies, depending on % Medicare inpatient bed days CAHs based on EHR costs & % Medicare inpatient bed days Varies, depending on % Medicaid inpatient bed days Reimbursement Reduced FY 2015No penalties
 2021 (max. 6 years, must start by 2016) Incentive Amount Varies, depending on % Medicare inpatient bed days CAHs based on EHR costs & % Medicare inpatient bed days Varies, depending on % Medicaid inpatient bed days Reimbursement Reduced FY 2015No penalties.")
55
IHS has created hospital incentive calculators Hospital Incentive Payment Estimator Eligible Hospitals: Incentive Calculators

56
ELIGIBLE HOSPITALS PERFORMANCE MEASURES & CLINICAL QUALITY MEASURES

57
Eligible Hospitals: Meaningful Use Requirements STAGE 1: Meaningful Use Requirements 19 total Performance Measures 14 core performance measures* 5 performance measures out of 10 from menu set* 15 total Clinical Quality Measures * Most measures require achievement of a performance target

58
1.>30%: Computerized physician order entry (CPOE): 2.Yes/No: Report hospital clinical quality measures to CMS or States 3.Yes/No: Implement one clinical decision support rule 4.>50%: Provide patients with an electronic copy of their health information, upon request 5.>50%: Provide patients with an electronic copy of their discharge instructions at time of discharge, upon request 6.Yes/No: Implement drug-drug and drug-allergy interaction checks during the entire EHR reporting period 7.>50%: Record demographics 8.>80%: Maintain an up-to-date problem list of current & active diagnoses 9.>80%: Maintain active medication list 10.>80%: Maintain active medication allergy list 11.>50%: Record and chart changes in vital signs 12.>50%: Record smoking status for patients 13 years or older 13.Yes/No: Capability to exchange key clinical information (Test Performed) 14.Yes/No: Conduct or review a security risk analysis Eligible Hospitals: 14 Core Performance Measures
: 2.Yes/No: Report hospital clinical quality measures to CMS or States 3.Yes/No: Implement one clinical decision support rule 4.>50%: Provide patients with an electronic copy of their health information, upon request 5.>50%: Provide patients with an electronic copy of their discharge instructions at time of discharge, upon request 6.Yes/No: Implement drug-drug and drug-allergy interaction checks during the entire EHR reporting period 7.>50%: Record demographics 8.>80%: Maintain an up-to-date problem list of current & active diagnoses 9.>80%: Maintain active medication list 10.>80%: Maintain active medication allergy list 11.>50%: Record and chart changes in vital signs 12.>50%: Record smoking status for patients 13 years or older 13.Yes/No: Capability to exchange key clinical information (Test Performed) 14.Yes/No: Conduct or review a security risk analysis Eligible Hospitals: 14 Core Performance Measures")
59
1.Yes/No: Implement drug-formulary checks for entire EHR reporting period 2.>40%: Incorporate clinical lab test results as structured data 3.Yes/No: Generate lists of patients by specific conditions 4.>10%: Use certified EHR technology to identify patient-specific education resources and provide to patient, if appropriate 5.>50%: Medication reconciliation at transitions of care 6.>50%: Summary of care record for each transition of care/referrals 7.Yes/No: Capability to submit electronic data to immunization registries/systems* (Test Performed) 8.Yes/No: Capability to provide electronic syndromic surveillance data to public health agencies* (Test Performed) 9.>50%: Record advanced directives for patients 65 years or older 10.Yes/No: Capability to provide electronic submission of reportable lab results to public health agencies* (Test Performed) *At least 1 public health measure must be selected Eligible Hospitals: 10 Menu Performance Measures (Pick 5)
 8.Yes/No: Capability to provide electronic syndromic surveillance data to public health agencies* (Test Performed) 9.>50%: Record advanced directives for patients 65 years or older 10.Yes/No: Capability to provide electronic submission of reportable lab results to public health agencies* (Test Performed) *At least 1 public health measure must be selected Eligible Hospitals: 10 Menu Performance Measures (Pick 5)")
60
Eligible Hospitals: 15 Clinical Quality Measures 1.Emergency Department Throughput – admitted patients Median time from ED arrival to ED departure for admitted patients 2.Emergency Department Throughput – admitted patients Admission decision time to ED departure time for admitted patients 3.Ischemic stroke – Discharge on anti-thrombotics 4.Ischemic stroke – Anticoagulation for A-fib/flutter 5.Ischemic stroke – Thrombolytic therapy for patients arriving within 2 hours of symptom onset 6.Ischemic or hemorrhagic stroke – Antithrombotic therapy by day 2 7.Ischemic stroke – Discharge on statins 8.Ischemic or hemorrhagic stroke – Rehabilitation assessment 9.VTE prophylaxis within 24 hours of arrival 10.Anticoagulation overlap therapy 11.Ischemic or Hemorrhagic stroke – Stroke Education 12.Intensive Care Unit VTE prophylaxis 13.Platelet monitoring on unfractionated heparin 14.VTE discharge instructions 15.Incidence of potentially preventable VTE

61
MEANINGFUL USE RESOURCES

62
Meaningful Use Resources National Site Tracker For RPMS sites, can run it to see if you have complete Certified EHR installed MU Readiness Assessment Tool MU Action Plan MU Preparation Checklist MU Performance Measure Cheat Sheets EHR MU Guide

63
Compares a list of RPMS applications installed at a facility with the official certified RPMS list Determines which versions/patches are needed Automated tool Meaningful Use Resources: National Site Tracker

64
Meaningful Use Resources: Privacy & Security IT staff attend 90 minute Risk Analysis WebEx Training Obtain the OIT Security Risk Analysis (RA) template located at http://www.ihs.gov/meaningfuluse/index.cfm?module=rsrc_toolkit Complete the Risk Analysis Process Conduct risk analysis Implement Risk Management Ensure a sanction policy is adopted for the site. Review logs and incident reports Submit completed risk analysis Complete monthly Secure Fusion & Annual Risk Analysis survey Attest to Privacy & Security when generating the RPMS MU Performance Measure report. 09/30/11- Medicare Eligible Hospital deadline 12/31/11- Medicare Eligible Provider deadline

65
Meaningful Use Resources: MU Guide Objective Type of Measure Threshold RPMS MU Report Logic RPMS Configuration EHR Use RPMS roll & scroll screenshots GUI EHR screenshots http://www.ihs.gov/CIO/ EHR/index.cfm?module =preparing_documents

67
Resources: Websites

68
MEANINGFUL USE REPORTS

69
MU Reports: EP & EH Performance Measures Reports PCC Management Report All measures Some yes/no measures need to be answered by person running report MU tab in iCare Provides current progress (runs/generates report overnight) Shows performance on all MU measures that calculate a rate e.g., CPOE rate, demographic rate, e-prescribing rate, etc. Includes measures that require a yes/no answer e.g., performance of a test of facility’s ability to electronically exchange key clinical information Summary Report provides information needed to attest with CMS or the respective State to receive incentive payment

70
MU Reports: EP & EH Performance Measures Reports

71
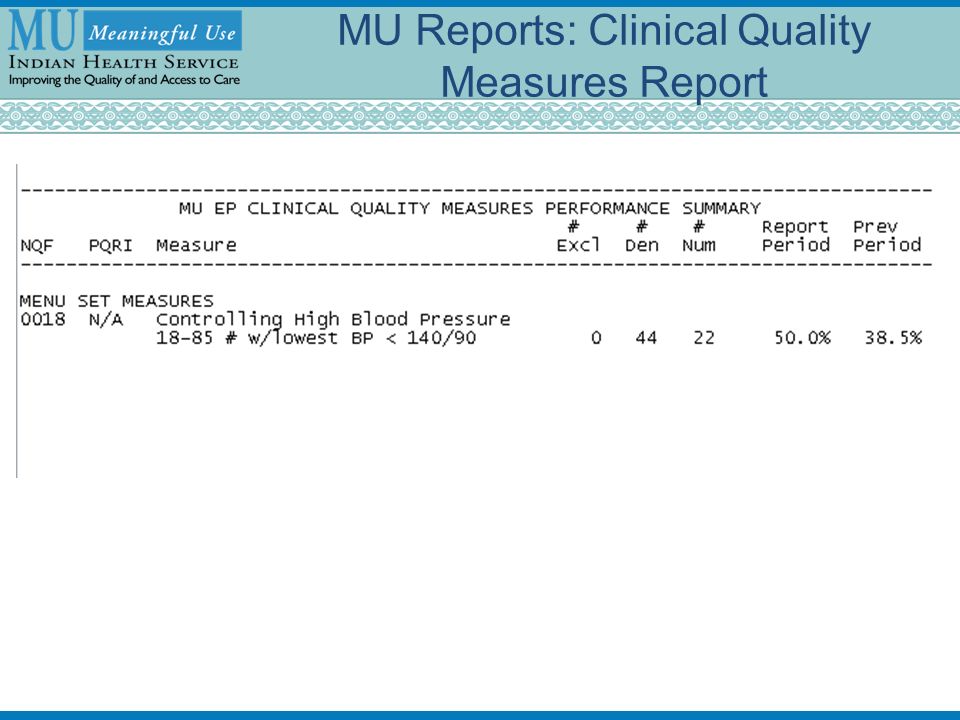
New MU tab in iCare RPMS Clinical Reporting System (CRS) 1st Release 9 EP measures 3 core/3 alternate core/3 menu set (breast cancer screening, cervical cancer screening, and colorectal cancer screening) CRS v11.0 Patch 2 2 nd Release All 15 hospital measures CRS v11.0 Patch 3 3rd Release Remaining 35 EP measures CRS v11.1. Patch 1 –Estimated release October 2011 MU Reports: Clinical Quality Measures Report

73
MU Reports : Patient Volume Report RPMS Third Party Billing (TPB) Developing software requirements/program logic EP individual and EH report released August 2011 EP group report anticipated October 2011 release Calculates EP Medicaid patient volume rates EP Needy Individual patient volume rates Group practice rates (Medicaid and Needy Individual) in lieu of calculating the rate for each individual EP Hospital Medicaid patient volume rates Relies on information stored in RPMS TPB; sites using a COTS Billing package will not be able to run this report
 Developing software requirements/program logic EP individual and EH report released August 2011 EP group report anticipated October 2011 release Calculates EP Medicaid patient volume rates EP Needy Individual patient volume rates Group practice rates (Medicaid and Needy Individual) in lieu of calculating the rate for each individual EP Hospital Medicaid patient volume rates Relies on information stored in RPMS TPB; sites using a COTS Billing package will not be able to run this report")
74
CMS INCENTIVE PROGRAMS REGISTRATION

75
CMS Incentive Program Registration: Overview MEDICARE hospitals & providers Only register on CMS incentive program website Https://ehrincentives.Cms.Gov/hitech/login.Action 3 rd party registration available for providers MEDICAID hospitals & providers Register on CMS incentive program website Https://ehrincentives.Cms.Gov/hitech/login.Action 3 rd party registration available for providers And Register on state Medicaid website Http://www.Cms.Gov/apps/files/medicaid-hit-sites/ Providers must self-register for Medicaid

76
CMS Incentive Program Registration: Eligible Hospitals Checklist CMS & Medicare Registration Identify registration coordinator and timeline for hospital registration Login to I & A at https://nppes.cms.hhs.gov/NPPES/IACreateLogin.dohttps://nppes.cms.hhs.gov/NPPES/IACreateLogin.do and Create “Certifying Official” and “End-User account Mail hospital copy of IRS Form CP-575 Obtain hospitals CMS Certification Number (CCN) Obtain hospital National Provider Identifier (NPI) Verify hospital has an enrollment record PECOS Identify the program(s) the hospital will participate in (should register for both) Identify state program hospital will participate in (MEDICAID ONLY) Identify type of hospital for Medicare & Medicaid hospital Obtain EHR certification number Obtain facility address from IRS form CP-575 Obtain facility work phone number Identify e-mail address to use for registration Print Submission Receipt Medicaid Registration Create a state account (account varies by state) Obtain state ID number Identify contact person for application questions Obtain IHS RPMS EHR Vendor Letter at http://www.ihs.gov/meaningfuluse/index.cfm?module=steps_request_letter http://www.ihs.gov/meaningfuluse/index.cfm?module=steps_request_letter Run hospital patient volume report Obtain cost report data for most recent 3-4 years
 Obtain hospital National Provider Identifier (NPI) Verify hospital has an enrollment record PECOS Identify the program(s) the hospital will participate in (should register for both) Identify state program hospital will participate in (MEDICAID ONLY) Identify type of hospital for Medicare & Medicaid hospital Obtain EHR certification number Obtain facility address from IRS form CP-575 Obtain facility work phone number Identify address to use for registration Print Submission Receipt Medicaid Registration Create a state account (account varies by state) Obtain state ID number Identify contact person for application questions Obtain IHS RPMS EHR Vendor Letter at module=steps_request_letter module=steps_request_letter Run hospital patient volume report Obtain cost report data for most recent 3-4 years")
77
CMS Incentive Program Registration: Eligible Professional Checklist CMS & Medicare Registration Identify who will register Medicare providers (third party registration or provider self registration) Login to I & A at https://nppes.cms.hhs.gov/NPPES/IACreateLogin.do and Create Third Party Registration User ID & Password (if applicable)https://nppes.cms.hhs.gov/NPPES/IACreateLogin.do Identify how the Medicaid providers will register (Providers must self register on Medicaid website) Obtain each provider’s National Provider Identifier (NPI) Verify each provider has an enrollment record in PECOS Identify the program the provider will be participating in Identify state program provider will participate in (MEDICAID ONLY) Identify type of provider’s profession (physician, optometrist, etc) Obtain EHR certification number Obtain facility Payee TIN & NPI (for reassignment of benefits to facility) Obtain facility address from IRS form CP-575 Obtain providers work phone number & email address Print Submission Receipt Medicaid Registration Create a state account (account varies by state) Obtain state Medicaid ID number Obtain Professional License number &issuing state (individual patient volume only) Obtain providers NPI and TIN information (group patient volume only) Identify contact person for application questions Obtain IHS RPMS EHR Vendor Letter at http://www.ihs.gov/meaningfuluse/index.cfm?module=steps_request_letter http://www.ihs.gov/meaningfuluse/index.cfm?module=steps_request_letter Run Individual/Group provider patient volume report
 Login to I & A at and Create Third Party Registration User ID & Password (if applicable) Identify how the Medicaid providers will register (Providers must self register on Medicaid website) Obtain each provider’s National Provider Identifier (NPI) Verify each provider has an enrollment record in PECOS Identify the program the provider will be participating in Identify state program provider will participate in (MEDICAID ONLY) Identify type of provider’s profession (physician, optometrist, etc) Obtain EHR certification number Obtain facility Payee TIN & NPI (for reassignment of benefits to facility) Obtain facility address from IRS form CP-575 Obtain providers work phone number & address Print Submission Receipt Medicaid Registration Create a state account (account varies by state) Obtain state Medicaid ID number Obtain Professional License number &issuing state (individual patient volume only) Obtain providers NPI and TIN information (group patient volume only) Identify contact person for application questions Obtain IHS RPMS EHR Vendor Letter at module=steps_request_letter module=steps_request_letter Run Individual/Group provider patient volume report")
78
Certifying Officials and Providers will use the NPPES/NPI web user account user name and password CMS Registration: Login Page

79
One difference in registering is that hospitals must provide their CCN and pick an NPI. These must match the TIN as well. CMS Registration: Hospital Registration

80
Here EP or staff registering on their behalf select program type (state for Medicaid providers), provider type, and EHR # CMS Registration: EP Program Selection
, provider type, and EHR # CMS Registration: EP Program Selection")
81
Unlike EPs, some hospitals can pick Medicare, Medicaid, or both IMPORTANT: If a hospital is eligible for both programs, they should select both, even if they may not get an incentive for both in the 1 st year. CMS Registration: EH Program Selection

82
Hospitals/Providers will not receive email confirmations at this point in the program. It is important that providers print this page or record the information in some other way. Medicaid EPs and hospitals must continue with the State’s site to verify additional info. CMS Registration: Submission Receipt

83
Area MU Coordinators AreaMU Coordinator EmailPhone Number AberdeenCAPT Scott Anderson Scott.Anderson@ihs.gov (605) 335-2504 Alaska Richard Hall Kimi Gosney Erika Wolter rhall@anthc.org kgosney@anthc.org ewolter@anthc.org (907) 729-2622 (907) 729-2642 (907) 729-3907 AlbuquerqueJacque Candelaria (Acting) Jacque.Candelaria@ihs.gov (505)988-9821 Bemidji Jason Douglas Alan Fogarty Jason.Douglas@ihs.gov Alan.Fogarty@ihs.gov (218) 444-0550 (218) 444-0538 BillingsCAPT James Sabatinos James.Sabatinos@ihs.gov (406) 247-7125 CaliforniaMarilyn Freeman Marilyn.Freeman@ihs.gov (916) 930-3981, ext. 362 NashvilleRobin Bartlett Robin.Bartlett@ihs.gov (615) 467-1577 NavajoLCDR Andrea Scott Andrea.Scott@ihs.govAndrea.Scott@ihs.gov; (928) 292-0201 OklahomaAmy Rubin Amy.Rubin@ihs.gov (405) 951-3732 PhoenixCAPT Lee Stern Lee.Stern@ihs.gov (602) 364-5287 Portland CAPT Leslie Dye Donnie Lee, MD Leslie.Dye@ihs.gov Donnie.Lee@ihs.gov (503) 326-3288 (503) 326-2017 TucsonScott Hamstra, MD Scott.Hamstra@ihs.gov (520) 295-2532
 NavajoLCDR Andrea Scott (928) OklahomaAmy Rubin (405) PhoenixCAPT Lee Stern (602) Portland CAPT Leslie Dye Donnie Lee, MD (503) (503) TucsonScott Hamstra, MD (520)")
84
Area MU Consultants(contractors) AreaMU ConsultantsEmailPhone Number Team Lead (ABQ)JoAnne HawkinsJoanne.Hawkins@ihs.gov(505) 382-4228 Regional #1(TUC) Troy WhaleyTroy.Whaley@ihs.gov(520) 954-5025 Regional #2(NAS)Melissa AlfordMelissa.Alford@ihs.gov(615) 260-4076 Regional #3(ABQ)Bevin MoonBevin.Moon@ihs.gov AberdeenCarol SmithCarol.Smith3@ihs.gov(605) 484-7090 AlaskaKaren Sidell Audra Hill Karen.Sidell@ihs.gov Audrey.Hill@ihs.gov (907) 729-2624 (907) 729-2679 AlbuquerqueTroy Whaley – InterimTroy.Whaley@ihs.gov(520) 954-5025 BemidjiSusanna FrenkelSusanna.Frenkel@ihs.gov(218) 444.0551 BillingsMelissa Alford- InterimMelissa.Alford@ihs.gov(615) 260-4076 CaliforniaTim CampbellTim.Campbell@ihs.gov(707) 889-3009 NashvilleRobin KitzmillerRobin.Kitzmiller@ihs.gov(615) 467-1532 NavajoDonna NichollsDonna.Nicholls@ihs.gov(505) 205-9177 OklahomaUrsula HillUrsula.Hill@ihs.gov(405) 951-6036 PhoenixRick BowmanRichard.Bowman@ihs.gov(520) 603-6817 PortlandAngela BoechlerAngela.Boechler@ihs.gov(971) 221-8057 TucsonRick BowmanRichard.Bowman@ihs.gov(520) 603-6817
 AreaMU Consultants Phone Number Team Lead (ABQ)JoAnne Regional #1(TUC) Troy Regional #2(NAS)Melissa Regional #3(ABQ)Bevin AberdeenCarol AlaskaKaren Sidell Audra Hill (907) (907) AlbuquerqueTroy Whaley – BemidjiSusanna BillingsMelissa Alford CaliforniaTim NashvilleRobin NavajoDonna OklahomaUrsula PhoenixRick PortlandAngela TucsonRick")
85
IHS Meaningful Use: Contact Information Chris Lamer, MU Federal Lead, COTR, IHS (615) 669-2747 Chris.Lamer@ihs.gov Cathy Whaley, MU Project Manager, DNC (520) 622-2069 Catherine.Whaley@ihs.gov JoAnne Hawkins, MU Field Team Lead, DNC (505) 382-4228 JoAnne.Hawkins@ihs.gov
 Cathy Whaley, MU Project Manager, DNC (520) JoAnne Hawkins, MU Field Team Lead, DNC (505)")
86
Questions? Sign up for the MU Listserv! MeaningfulUseTeam@ihs.gov

Similar presentations












 Incentive Program Update OHCA Board Meeting December 9, 2010 Adolph Maren Jr., M.A. Senior Planning Coordinator.>")




 October 18, 2010 IHS Office of.>")

