Download presentation
Presentation is loading. Please wait.

1
Current Trends and Updates on Diagnosis and Management of GERD
Jeraldine S. Orlina, MD Grand Rounds January 11, 2006

2
Pathophysiology Lower esophageal sphincter Intrinsic muscle of distal esophagus Sling fibers of cardia Diaphragm Transmitted pressure of abdominal cavity Reflux occurs when the high-pressure zone in distal esophagus is too low or when sphincter with normal pressure undergoes spontaneous relaxation The lower esophageal sphincter has the primary role of preventing reflux of the gastric contents into the esophagus. The sphincter is a unique physiologic entity, as opposed to an anatomic structure, that is located just cephalad to the gastroesophageal junction and is clearly identifiable as a zone of high pressure during manometric evaluation. Several factors contribute to the high-pressure zone. The first is the intrinsic musculature of the distal esophagus which are unique from those in other areas of the esophagus in that they are in a state of tonic contraction. They normally relax with initiation of a swallow and then return to a state of tonic contraction. The second contributing factor to LES pressure is the sling fibers of the cardia. These fibers are at the same anatomic depth of the circular muscle fibers of the esophagus but are oriented in a different direction. They run diagonally from the cardia-fundus junction to the lesser curve. The third contributing factor to the maintenance of the high-pressure zone in the distal esophagus is the diaphragm. The last component of the pressure generated at the lower esophageal high-pressure zone is the transmitted pressure of the abdominal cavity. The abdominal compartment has a relatively higher pressure than does the thoracic cavity. A gastroesophageal junction that is firmly anchored in the abdominal cavity will be exposed to a greater transmural pressure than one that is in the posterior mediastinum. Gastroesophageal reflux may occur when the high-pressure zone in the distal esophagus is too low to prevent gastric contents from entering the esophagus or when a sphincter with normal pressure undergoes spontaneous relaxation, not associated with a peristaltic wave in the body of the esophagus. Although both conditions may lead to abnormal amounts of reflux, some degree of reflux is present in most individuals.

3
GERD is often associated with a hiatal hernia
GERD is often associated with a hiatal hernia. Although any type of hiatal hernia may give rise to the classic symptoms of reflux, the most common is the type I hernia also called a sliding hiatal hernia. A type I hernia is present when the gastroesophageal junction is not maintained in the abdominal cavity by the phrenoesophageal ligament, thus allowing the cardia to migrate back and forth between the posterior mediastinum and the peritoneal cavity. Although the presence of a small sliding hernia does not necessarily imply an incompetent cardia, the larger its size, the greater the risk of abnormal gastroesophageal reflux. A type II hernia (in B), also called a rolling or paraesophageal hernia, occurs when the gastroesophageal junction is anchored in the abdomen but the hiatal defect, which is usually large, provides space for viscera to migrate into the mediastinum. The relatively negative pressure in the thorax facilitates visceral migration. Most commonly, the fundus of the stomach migrates into the mediastinum; however, the colon and spleen are also occasionally identified. This is discussed in more detail in the second part of this chapter in the discussion of paraesophageal hernias. A type III hernia (seeC) is a combination of the first two, in which the gastroesophageal junction and the fundus (or other viscera) are free to move into the mediastinum. A hiatal hernia is neither necessary nor sufficient to make the diagnosis of GERD, and having a hernia does not constitute an indication for operative correction. The theoretical implications of a type I and type III hiatal hernia being present is that the cardia and distal esophagus have the potential to be exposed to the negative pressure of the thoracic cavity. This would have the effect of lowering the pressure at the LES, thereby allowing reflux to occur more readily. Many patients with hiatal hernias do not have symptoms and do not require treatment.
, also called a rolling or paraesophageal hernia, occurs when the gastroesophageal junction is anchored in the abdomen but the hiatal defect, which is usually large, provides space for viscera to migrate into the mediastinum. The relatively negative pressure in the thorax facilitates visceral migration. Most commonly, the fundus of the stomach migrates into the mediastinum; however, the colon and spleen are also occasionally identified. This is discussed in more detail in the second part of this chapter in the discussion of paraesophageal hernias. A type III hernia (seeC) is a combination of the first two, in which the gastroesophageal junction and the fundus (or other viscera) are free to move into the mediastinum. A hiatal hernia is neither necessary nor sufficient to make the diagnosis of GERD, and having a hernia does not constitute an indication for operative correction. The theoretical implications of a type I and type III hiatal hernia being present is that the cardia and distal esophagus have the potential to be exposed to the negative pressure of the thoracic cavity. This would have the effect of lowering the pressure at the LES, thereby allowing reflux to occur more readily. Many patients with hiatal hernias do not have symptoms and do not require treatment.")
4
Absite Question An operation is the primary initial management for:
A) Achalasia B) a large sliding esophageal hiatal hernia C) an epiphrenic esophageal diverticulum D) gastroesophageal reflux E) a paraesophageal hiatal hernia The most common structure to herniate through the esophageal hiatus is the fundus of the stomach. Occasionally, the fundus of the stomach will rotate toward the right pleural cavity along the organoaxial axis defined by the phrenoesophageal membrane at the hiatus and the retroperitoneal attachment of the first portion of the duodenum. This results in what has been referred to as an upside-down stomach. Other structures that may be located in the hernia sac include the spleen, colon, and omentum. After repeated episodes of the viscera entering the hernia sac, adhesions between the wall of the sac and the structures may form, thus preventing the structures from returning to their position in the peritoneal cavity. The natural history of these large hernias is a matter of debate. Rarely, the herniated contents will become strangulated, causing an emergent condition that requires immediate operative intervention. Because of these risks most for decades have recommended repair of these hernias when detected regardless of symptoms. Recent evidence, however, suggests that the risk of acute strangulation is around 1% per year. Therefore we, and many others, recommend surgical intervention only for younger patients (<60 years) and those with significant symptoms.
 Achalasia. B) a large sliding esophageal hiatal hernia. C) an epiphrenic esophageal diverticulum. D) gastroesophageal reflux. E) a paraesophageal hiatal hernia. The most common structure to herniate through the esophageal hiatus is the fundus of the stomach. Occasionally, the fundus of the stomach will rotate toward the right pleural cavity along the organoaxial axis defined by the phrenoesophageal membrane at the hiatus and the retroperitoneal attachment of the first portion of the duodenum. This results in what has been referred to as an upside-down stomach. Other structures that may be located in the hernia sac include the spleen, colon, and omentum. After repeated episodes of the viscera entering the hernia sac, adhesions between the wall of the sac and the structures may form, thus preventing the structures from returning to their position in the peritoneal cavity. The natural history of these large hernias is a matter of debate. Rarely, the herniated contents will become strangulated, causing an emergent condition that requires immediate operative intervention. Because of these risks most for decades have recommended repair of these hernias when detected regardless of symptoms. Recent evidence, however, suggests that the risk of acute strangulation is around 1% per year. Therefore we, and many others, recommend surgical intervention only for younger patients (<60 years) and those with significant symptoms.")
5
Symptoms Symptom Predominance (%) Heartburn 80 Regurgitation 54
Abdominal Pain 29 Cough 27 Dysphagia for solids 23 Hoarseness 21 Belching 15 Aspiration 14 Wheezing 7 Globus 4 The most common presentation of patients with GERD includes a long-standing history of heartburn and a shorter history of regurgitation.

6
Symptoms -- Heartburn Epigastric and retrosternal
Caustic or stinging sensation Does not radiate to the back, is not pressurelike Can be confused with symptoms of PUD, bilary colic, or CAD Heartburn, when typical, is a very reliable symptom. Heartburn should be confined to the epigastric and retrosternal areas. It should be identified as a caustic or stinging sensation. It does not radiate to the back and is not characteristically described as a pressure sensation. It is best to ask the patient to describe in detail the sensation he or she is experiencing. Sometimes the symptoms will be more characteristic of peptic ulcer disease, cholelithiasis, or coronary artery disease.

7
Symptoms -- Regurgitation
Indicates progression of disease Distinguish between digested and undigested food The presence of regurgitation indicates progression of the disease. Some patients will be unable to bend over without experiencing the unpleasant event. A distinction between regurgitation of undigested and digested food should be made. Undigested food in the regurgitant is indicative of a different pathologic process, such as an esophageal diverticulum or achalasia.

8
Diagnostic Studies Empirical Therapy
Upper Gastrointestinal Endoscopy (EGD) Upper Gastrointestinal Fluoroscopy with Barium 24-hour pH testing Esophageal Manometry If the patient’s history is typical for uncomplicated GERD, and initial trial of empirical therapy including lifestyle modification is appropriate. Further diagnostic modalities can be used in the evaluation of patients who did not respond to medical therapy, patients with alarm symptoms suggesting complicated disease (such as dysphagia, odynophagia, bleeding, weight loss, or anemia), and when patients have a sufficient duration of symptms to put them at risk for Barrett’s esophagus. These include…
 Upper Gastrointestinal Fluoroscopy with Barium. 24-hour pH testing. Esophageal Manometry. If the patient’s history is typical for uncomplicated GERD, and initial trial of empirical therapy including lifestyle modification is appropriate. Further diagnostic modalities can be used in the evaluation of patients who did not respond to medical therapy, patients with alarm symptoms suggesting complicated disease (such as dysphagia, odynophagia, bleeding, weight loss, or anemia), and when patients have a sufficient duration of symptms to put them at risk for Barrett’s esophagus. These include…")
9
EGD Allows examination of the esophageal mucosa
Identifies presence of esophagitis and grading of severity Can identify other pathology, such as diverticula, hiatal hernia, webs, rings, or strictures Tissue biopsies to screen for Barrett’s esophagus EGD allows for examination of the esophageal mucosa. It is useful in identifying the presence of esophagitis or Barrett’s esophagus which is essentially diagnostic of GERD. It can also identify other pathology such as diverticula, hiatal hernia, webs, rings, or strictures. Tissue biopsies should also be obtained in order to screen for Barrett’s esophagus.

10
Absite Question Four hours following upper esophagogastric endoscopy for gastroesophageal reflux, a 62 year-old man returns to the emergency room with chills, chest pain, and dyspnea. Cardiac work-up is normal, but esophagography shows a distal esophageal perforation. The most appropriate management is A) nasogastric suction and TPN B) reinforced primary esophageal repair C) drainage and esophageal diversion D) esophagectomy with gastric pull-through E) fluoroscopic esophageal stent placement
 nasogastric suction and TPN. B) reinforced primary esophageal repair. C) drainage and esophageal diversion. D) esophagectomy with gastric pull-through. E) fluoroscopic esophageal stent placement.")
11
Absite Question A 60 year-old otherwise healthy man has symptomatic GERD that has not responded to medical therapy, including PPIs. Esophagoscopy shows moderately severe esophagitis. Multiple biopsies of the esophageal mucosa in the area of esophagitis show columnar epithelium replacing the normal squamous epithelium. As the patient’s treatment is being planned, a biopsy report shows high-grade dysplasia.

12
(cont) Treatment should be
Continued medical treatment with yearly esophagoscopy and biopsies Laparoscopic Nissen fundoplication Photodynamic therapy Esophagectomy Laser ablation of normal mucosa Although most patient’s with Barrett’s esophagus can be treated adequately eith an antireflux procedure, patients withhigh grade dysplasia should be treated much more aggressively. At least one third of patients with high grade dysplasia already have onvasive carcinoma in the dyplastic area. Between a third and a half will show evidence pf carcinoma wothin five years. Esophagectomy with gatric or colonic reconstruction is the only effective therapy. Ablative therapy with electrosurgery, laser, or photodynamic therapy is used in patients with low-grade dysplasia, but should not replace p[eration in patients with high-grade dysplasia.

13
24-hour pH test Gold Standard for presence of pathologic reflux
Parameters measured include: total # of reflux episodes, duration of longest reflux episode, percentage of time pH is less than 4 The gold standard for diagnosing and quantifying acid reflux is the 24-hour pH test. It helps to confirm reflux in patients with persistent symptoms (both typical and atypical) without evidence of mucosal damage on EGD when a trial of acid suppression has failed. It may also be used to monitor the control of reflux in patients with continued symptoms on therapy. The study is performed by placing a thin catheter containing one or more solid-state electrodes in the esophagus. The electrodes are spaced 5 to 10 cm apart and are capable of sensing fluctuations in the pH between 2 and 7. The electrodes are connected to a data recorder that the patient wears for the period of observation. There is a digital clock displayed on the recorder. When the patient has an event (like heartburn, chest pain, eructation), he or she is to record the event in a diary, noting the time on the recorder. A large amount of information may be gleaned from the study: total number of reflux episodes (defined by pH <4), longest episode of reflux, number of episodes lasting longer than 5 minutes, extent of reflux in the upright position, and extent of reflux in the supine position. An overall score is obtained with the use of a formula that assigns a weight to each item according to its capacity to cause esophageal injury. This value, known as the DeMeester score, should be less than A simpler way to determine whether abnormal reflux is occurring is to estimate the total percent of time the pH is below 4 in the proximal and distal channel. In the proximal esophagus (15 cm above the LES), acid exposure normally occurs less than 1% of the time; in the distal esophagus (5 cm above the LES), it normally occurs less than 4%. The patient’s symptom diary should be correlated with episodes of reflux. The correlation of heartburn or chest pain with a drop in the pH has significant clinical value because it helps to confirm a cause-and-effect relationship.
 without evidence of mucosal damage on EGD when a trial of acid suppression has failed. It may also be used to monitor the control of reflux in patients with continued symptoms on therapy. The study is performed by placing a thin catheter containing one or more solid-state electrodes in the esophagus. The electrodes are spaced 5 to 10 cm apart and are capable of sensing fluctuations in the pH between 2 and 7. The electrodes are connected to a data recorder that the patient wears for the period of observation. There is a digital clock displayed on the recorder. When the patient has an event (like heartburn, chest pain, eructation), he or she is to record the event in a diary, noting the time on the recorder. A large amount of information may be gleaned from the study: total number of reflux episodes (defined by pH <4), longest episode of reflux, number of episodes lasting longer than 5 minutes, extent of reflux in the upright position, and extent of reflux in the supine position. An overall score is obtained with the use of a formula that assigns a weight to each item according to its capacity to cause esophageal injury. This value, known as the DeMeester score, should be less than A simpler way to determine whether abnormal reflux is occurring is to estimate the total percent of time the pH is below 4 in the proximal and distal channel. In the proximal esophagus (15 cm above the LES), acid exposure normally occurs less than 1% of the time; in the distal esophagus (5 cm above the LES), it normally occurs less than 4%. The patient’s symptom diary should be correlated with episodes of reflux. The correlation of heartburn or chest pain with a drop in the pH has significant clinical value because it helps to confirm a cause-and-effect relationship.")
14
Ambulatory pH testing – Recent Advances
Combined impedance and acid testing Allows for the measurement of both acid and nonacid (volume) reflux. Important in pt with persistent symptoms despite an adequate medical trial Impedance testing depends upon measurement of changes in resistance (in Ohms) to alternating electrical current when a bolus passes by a pair of metallic rings mounted on a catheter. In an empty tubular organ (ie, esophagus or small intestine) the electrical current between the two rings is conducted by the few ions present in and on the esophageal mucosa. Liquid containing boluses with an increased number of ions have a higher conductivity and when entering the impedance measuring segment will lower the impedance to a nadir value. The impedance stays at its nadir as long as the bolus is present in the segment, returning to baseline once the bolus is cleared by a contraction. The contraction produces a slight increase in impedance above the baseline due to a decrease in luminal cross-section. Gas passing transiently by the impedance measuring segments will produce a rapid rise in the impedance since they have poor electrical conductance. Measuring impedance at multiple sites (multichannel) allows for determination of direction of bolus movement based upon temporal differences in bolus entry and exit (ie, bolus entries progressing from proximal to distal indicate antegrade bolus movement while bolus entries progressing from distal to proximal indicate retrograde bolus movement) (show figure 3). Combined with manometry (multichannel intraluminal impedance and manometry; MII-EM) it provides information about both pressures and bolus transit within the esophagus. Combined with pH (multichannel intraluminal impedance and pH; MII-pH) it permits detection of both acid and non-acid gastroesophageal reflux.
 reflux. Important in pt with persistent symptoms despite an adequate medical trial. Impedance testing depends upon measurement of changes in resistance (in Ohms) to alternating electrical current when a bolus passes by a pair of metallic rings mounted on a catheter. In an empty tubular organ (ie, esophagus or small intestine) the electrical current between the two rings is conducted by the few ions present in and on the esophageal mucosa. Liquid containing boluses with an increased number of ions have a higher conductivity and when entering the impedance measuring segment will lower the impedance to a nadir value. The impedance stays at its nadir as long as the bolus is present in the segment, returning to baseline once the bolus is cleared by a contraction. The contraction produces a slight increase in impedance above the baseline due to a decrease in luminal cross-section. Gas passing transiently by the impedance measuring segments will produce a rapid rise in the impedance since they have poor electrical conductance. Measuring impedance at multiple sites (multichannel) allows for determination of direction of bolus movement based upon temporal differences in bolus entry and exit (ie, bolus entries progressing from proximal to distal indicate antegrade bolus movement while bolus entries progressing from distal to proximal indicate retrograde bolus movement) (show figure 3). Combined with manometry (multichannel intraluminal impedance and manometry; MII-EM) it provides information about both pressures and bolus transit within the esophagus. Combined with pH (multichannel intraluminal impedance and pH; MII-pH) it permits detection of both acid and non-acid gastroesophageal reflux.")
15
Ambulatory pH testing – Recent Advances
Tubeless method– Bravo System Allows a radiotelemetry capsule to be attached to the esophageal mucosa Decreases patient discomfort, allows for longer (48h) monitoring, and may improve accuracy by allowing the patient to carry out their usual activities The Bravo System is designed to minimize the discomfort associated with transnasal catheters. Bravo is the world's first catheter-free pH system that replaces the catheter in the esophagus with a small capsule containing a radiotransmitter that is attached to the esophageal mucosa. Patients using the Bravo system can participate in their everyday activities during the pH study period. The study results obtained with a Bravo system are more representative of a patient's normal day, and because 48 hours of a data can be recorded, more data is available to the physician. The system consists of (1)The Bravo pH Receiver an ambulatory data recorder that is the size and weight of a conventional pager. The Receiver is lightweight and compact, and it clips easily onto a belt, or a pocket allowing the patient to carry the Receiver throughout the study period. The second part of the system is (2) The Bravo capsule. The miniature Bravo pH capsule is approximately the size of a gel cap.
 monitoring, and may improve accuracy by allowing the patient to carry out their usual activities. The Bravo System is designed to minimize the discomfort associated with transnasal catheters. Bravo is the world s first catheter-free pH system that replaces the catheter in the esophagus with a small capsule containing a radiotransmitter that is attached to the esophageal mucosa. Patients using the Bravo system can participate in their everyday activities during the pH study period. The study results obtained with a Bravo system are more representative of a patient s normal day, and because 48 hours of a data can be recorded, more data is available to the physician. The system consists of (1)The Bravo pH Receiver an ambulatory data recorder that is the size and weight of a conventional pager. The Receiver is lightweight and compact, and it clips easily onto a belt, or a pocket allowing the patient to carry the Receiver throughout the study period. The second part of the system is (2) The Bravo capsule. The miniature Bravo pH capsule is approximately the size of a gel cap.")
16
The capsule is temporarily inserted by means of a customized delivery system, and is often placed during an endoscopy. Once the capsule is in place, the delivery system is removed. Data is transmitted to a receiver which is worn by the patient .

17
Esophageal Manometry Lower Esophageal Sphincter (LES) Esophageal Body
Mean resting pressure Total length Esophageal Body To determine effectiveness of peristalsis Amplitude of esophageal wave A significant amount of information about the function of the esophageal body and the LES may be obtained from stationary esophageal manometry. The manometry catheter is a flexible tube with pressure-sensing devices arranged at 5-cm intervals. The LES is analyzed for mean resting pressure and total length. Length includes the intra-abdominal length, and the location of the sphincter relative to the nares. The longer the length of the high-pressure zone and the longer the intra-abdominal component, the greater the barrier to reflux of gastric contents. The esophageal body is then assessed to determine the effectiveness of peristalsis. With the four channels located at 3, 8, 13, and 18 cm above the LES, the patient is given a series (at least 10) of 5-mL aliquots of water to swallow. The peristaltic activity is reported as the percentage of initiated swallows that are transmitted to each channel successfully. Normally, a patient should have greater than 80% peristalsis. The second characteristic of clinical importance is the amplitude of the peristaltic wave. The amplitude is simply the average of the pressures generated in the distal esophagus during effectively transmitted peristaltic waves. Ineffective esophageal motility (IEM) is defined as less than 60% peristalsis or distal esophageal amplitudes of less than 30 mm Hg and is often associated with significant GERD. This is particularly important in patients in whom antireflux surgery is being considered. It has been suggested that patients who have ineffective peristalsis may need to either avoid surgery or undergo an alternative procedure.
 of 5-mL aliquots of water to swallow. The peristaltic activity is reported as the percentage of initiated swallows that are transmitted to each channel successfully. Normally, a patient should have greater than 80% peristalsis. The second characteristic of clinical importance is the amplitude of the peristaltic wave. The amplitude is simply the average of the pressures generated in the distal esophagus during effectively transmitted peristaltic waves. Ineffective esophageal motility (IEM) is defined as less than 60% peristalsis or distal esophageal amplitudes of less than 30 mm Hg and is often associated with significant GERD. This is particularly important in patients in whom antireflux surgery is being considered. It has been suggested that patients who have ineffective peristalsis may need to either avoid surgery or undergo an alternative procedure.")
18
Esophagram Useful when operation is planned—shows anatomy of esophagus and proximal stomach Demonstrates presence and size of hiatal hernia if present The esophagram provides valuable information in the evaluation of patients with symptoms of GERD when an operation is contemplated or when the symptoms do not respond as expected. Often, spontaneous reflux during the examination will be demonstrated. Although reflux may be induced in patients who do not have the disease, the occurrence of spontaneous reflux lends support to the diagnosis of abnormal gastroesophageal reflux. The true value of the study is to determine the external anatomy of the esophagus and the proximal stomach. The presence and size of a hiatal hernia may be characterized . Although this neither confirms nor refutes the presence of disease, it is extremely beneficial in planning the operation. A mediastinal gastroesophageal junction that does not reduce into the peritoneal cavity during the study is a predictor of a more difficult operation that may require an esophageal lengthening procedure. Peptic esophageal strictures may also be found on an esophageal contrast study. The presence of a stricture will taint the interpretation of the 24-hour pH study, especially if it is tight enough to prevent reflux. Other anatomic abnormalities, such as diverticula, tumors, and unexpected paraesophageal hernias, will be discovered during an esophagogram. Figure 40-6 Upper gastrointestinal contrast material study shows a large hiatal hernia with the rugal folds of the stomach clearly transgressing the shadow of the left hemidiaphragm.

19
Treatment – Lifestyle Modification
May benefit many patients with GERD, although these changes alone are unlikely to control symptoms in the majority of patients Elevation of the head of the bed, decreased fat intake, cessation of smoking, avoiding recumbency for 3h postprandially, avoidance of certain foods (chocolate, EtOH, peppermint) No data reflecting the efficacy of these maneuvers
 No data reflecting the efficacy of these maneuvers.")
20
Treatment – Patient Directed Therapy
Antacids H2 receptor antagonists If symptoms persist, continuous therapy is required, or alarm symptoms/signs develop – pt should have additional evaluation and treatment Antacids and over-the-counter acid suppressants are options for patient directed therapy for heartburn and regurgitation. Then symptoms persist, continuous therapy is required, or alarm symptoms or signs develop, the patient should have additional evaluation and treatment.

21
Treatment – Acid Suppression
6-week course of acid-suppression therapy Double dose of a proton pump inhibitor Irreversible bind the proton pump in parietal cells of the stomach Maximal effect 4 days after initiation of therapy and lasts for the life of the parietal cell More effective than other antacid regimens Acid suppression in the mainstay of therapy for GERD. Proton pump inhibitors provide the most rapid symptomatic relief and heal esophagitis in the highest percentage of patients. These drugs act by irreversibly binding the proton pump in the parietal cells of the stomach, thus effectively stopping gastric acid production. The maximal effect occurs after approximately 4 days of therapy, and the effects will linger for the life of the parietal cell. Thus, the acid suppression will persist for 4 to 5 days after therapy has ended. For this reason, the patient should be off therapy for 1 week before being evaluated with pH monitoring. Compared with H2 blockers, proton pump inhibitors are more effective at healing esophageal ulceration secondary to acid exposure. The medications are relatively expensive but are well tolerated. The side effects may include headache, abdominal pain, and diarrhea.

22
Absite Question Proton pump inhibitors used in the treatment of GERD
Cause regression of Barrett’s epithelium Inhibit progression of dysplasia Increase squamous islands in Barrett’s segments Reverse intestinal metaplasia Are effective only if gastric acidity is normalized Although proton pump inhibitors increase the number of squamous epithelial islands within Barrett’s segments, biopsy specimens often show underlying intestinal metaplasia, indicating that even high doses of these drugs may not result in clinically significant regression of Barrett’s epithelium. Despite effective healing of injured esophageal mucosa, there is no evidence that these medications directly inhibit progression of abnormal epithelium to high-grade dysplasia. In fact, long-term gastric acid suppression may increase the risk of intestinal metaplasia of the esophagus as a result o bacterial overgrowth and a dramatic increase in the concentration of unconjugated bile salts in refluxed duodenal contents.

23
Treatment – Promotility Therapy
May be used as an adjunct to acid suppression therapy in patients with demonstrated defects in esophagogastric motility (LES incompetence, poor esophageal clearance, delayed gastric emptying) Promotility agents such as Reglan may be used in patients that demonstrate defects in gastroesophageal motilityas an adjunct to acid suppression. Domperidone is a dopamine receptor blocker that is not yet available in the US but unlike reglan does not easily cross the blood-brain barrier and therefore has little CNS effect.
 Promotility agents such as Reglan may be used in patients that demonstrate defects in gastroesophageal motilityas an adjunct to acid suppression. Domperidone is a dopamine receptor blocker that is not yet available in the US but unlike reglan does not easily cross the blood-brain barrier and therefore has little CNS effect.")
24
Absite Question Five years after a myocardial infarction, a 55 year-old woman with HTN and DM has symptomatic esophagogastric reflux. Medical treatment for the last year has not been successful. Her BMI is 55. Esophagoscopy shows severe esophagitis. Multiple biopsies show inflammatory changes but no columnar epithelium or cancer. The best treatment would be: Nissen fundoplication Gastric bypass procedure Gastric banding procedure Vertical banded gastroplasty Biliary-pancreatic diversion with duodenal switch As many as 50% of morbidly obese patients have some gastroesophageal reflux, and as many as 20% may have moderate or severe reflux requiring therapy. Whereas many surgeons will perform an antireflux procedure, there is some evidence that these procedures lead to a poor long-term result in the severely obese. A RYGB removes most of the stomach from contact with the esophagus and provides complete diversion of bile. It has results comparable to those seen with Nissen fundoplication in normal weight patients. It is not dependent of inducing weight loss to produce alleviation of symptoms. Any patient with severe or intractable GERD and a BMI > 35 should be considered for gastric bypass rather than a standard reflux procedure.

25
Surgical Therapy Indications
Pt w/ evidence of severe esophageal injury (ulcer, stricture, or Barrett’s) Incomplete resolution of symptoms or relapses while on medical therapy Long duration of symptoms Younger patients Ideal patient: more than 10-year life expectancy and are in need of lifelong therapy due to a mechanically defective sphincter The indications for surgical therapy have changed somewhat with the advent of proton pump inhibitors. Certainly, patients with evidence of severe esophageal injury (ulcer, stricture, or Barrett mucosa) and incomplete resolution of symptoms or relapses while on medical therapy are appropriate to consider for operative intervention. Other patients with a long duration of symptoms or those in whom symptoms persist at a young age should be considered for operative treatment initially. In these patients, operative therapy should be considered an alternative to medical therapy rather than a treatment of last resort. There are some patients who have absolutely no response of their symptoms to the use of proton pump inhibitors. They should be scrutinized further before offering surgical treatment, as opposed to being considered medical failures who need operative treatment. Because the proton pump inhibitors are so effective at decreasing the acid production of the stomach, the diagnosis of GERD in such patients should be questioned and must be demonstrated with objective testing. Since the application of minimally invasive techniques to the treatment of GERD, the cost and morbidity associated with operative treatment has decreased. This has changed the way in which surgical treatment is viewed. Considering the cost of proton pump inhibitor use and the cost of operative treatment with its accepted success rate, the length of time required for medical therapy to become more expensive than the operation is about 10 years. This assumes the patient uses the lowest dose of the medication. Therefore, in patients who have more than 10 years of life expectancy and are in need of lifelong therapy due to a mechanically defective sphincter, surgical therapy may be considered as the treatment of choice. That being said, there is still considerable controversy that exists over the long-term effectiveness of surgical intervention in GERD and whether it is equal or superior to chronic medical therapy.
 Incomplete resolution of symptoms or relapses while on medical therapy. Long duration of symptoms. Younger patients. Ideal patient: more than 10-year life expectancy and are in need of lifelong therapy due to a mechanically defective sphincter. The indications for surgical therapy have changed somewhat with the advent of proton pump inhibitors. Certainly, patients with evidence of severe esophageal injury (ulcer, stricture, or Barrett mucosa) and incomplete resolution of symptoms or relapses while on medical therapy are appropriate to consider for operative intervention. Other patients with a long duration of symptoms or those in whom symptoms persist at a young age should be considered for operative treatment initially. In these patients, operative therapy should be considered an alternative to medical therapy rather than a treatment of last resort. There are some patients who have absolutely no response of their symptoms to the use of proton pump inhibitors. They should be scrutinized further before offering surgical treatment, as opposed to being considered medical failures who need operative treatment. Because the proton pump inhibitors are so effective at decreasing the acid production of the stomach, the diagnosis of GERD in such patients should be questioned and must be demonstrated with objective testing. Since the application of minimally invasive techniques to the treatment of GERD, the cost and morbidity associated with operative treatment has decreased. This has changed the way in which surgical treatment is viewed. Considering the cost of proton pump inhibitor use and the cost of operative treatment with its accepted success rate, the length of time required for medical therapy to become more expensive than the operation is about 10 years. This assumes the patient uses the lowest dose of the medication. Therefore, in patients who have more than 10 years of life expectancy and are in need of lifelong therapy due to a mechanically defective sphincter, surgical therapy may be considered as the treatment of choice. That being said, there is still considerable controversy that exists over the long-term effectiveness of surgical intervention in GERD and whether it is equal or superior to chronic medical therapy.")
26
Trends in the use of surgery for gastroesophageal reflux disease in Ontario, 1988-2000
The initial decline and subsequent rise in GERD surgery over the past decade reflects 2 important trends in therapeutic approaches to GERD. First, the arrival of PPIs in the marketplace in the late 1980s was associated with a sharp decline in GERD surgery. Second, the increased use of GERD surgery after 1996 was probably related to the widespread use of laparoscopy. The increased popularity of GERD surgery over the last few years suggests that patients and physicians consider laparoscopic GERD surgery an improvement over conventional open surgery and an effective alternative to long-term medical therapy for GERD. Although the use of GERD surgery has increased, disagreement between surgeons and gastroenterologists persists regarding the role of surgery in patients with uncomplicated GERD. The predominant surgical perspective, that surgery is more effective than medical therapy and should be offered even to patients who respond well to PPIs, conflicts sharply with the medical perspective that surgery is ineffective or lacks durability in many patients and should be reserved for the rare patient who fails, or is unwilling to continue, drug therapy. Lack of consensus is not the result of a lack of prospective randomized trials; several have been conducted over the last 3 decades as both medical and surgical therapies have evolved. Conventional antireflux surgery proved far more effective than antacids and lifestyle modifications in 1975, modestly more effective than histamine type-2 receptor antagonists (H2RAs) in 1992. and perhaps marginally more effective than PPIs in The principal message from randomized trials is that, under ideal circumstances, modern surgical and medical management are both highly efficacious in the reduction of GERD symptoms. Urbach, D. R. et al. CMAJ 2004;170: Copyright ©2004 CMA Media Inc. or its licensors
 in and perhaps marginally more effective than PPIs in The principal message from randomized trials is that, under ideal. circumstances, modern surgical and medical management are both highly efficacious in the reduction of GERD symptoms. Urbach, D. R. et al. CMAJ 2004;170: Copyright ©2004 CMA Media Inc. or its licensors.")
27
Laparoscopic Nissen Fundoplication
Lafullarde T, Watson DI, Jamieson GG, Myers JC, Game PA, Devitt PG. Laparoscopic Nissen fundoplication: five-year results and beyond. Arch Surg Feb;136(2):180-4 87% of the 176 patients remained free of significant reflux. The long-term outcome was considered "good or excellent" by 90% of patients.
: % of the 176 patients remained free of significant reflux. The long-term outcome was considered good or excellent by 90% of patients.")
28
Laparoscopic Nissen Fundoplication
Success rate of greater than 90% Procedure of choice In the properly selected patient, laparoscopic antireflux surgery with a Nissen fundoplication has a success rate of greater than 90% in addressing the classic symptoms of reflux, specifically heartburn and regurgitation. I will describe the left crus approach to a (Nissen fundoplication), which should be the procedure of choice for the majority of patients. The left crus approach provides the advantage of a direct and early view of the short gastric vessels and the spleen. Once this obstacle is negotiated, there is little chance of injuring the spleen during the remainder of the procedure.
, which should be the procedure of choice for the majority of patients. The left crus approach provides the advantage of a direct and early view of the short gastric vessels and the spleen. Once this obstacle is negotiated, there is little chance of injuring the spleen during the remainder of the procedure.")
29
The patient is placed in a low lithotomy position
The patient is placed in a low lithotomy position. The surgeon stands between the patient’s legs, with the assistant on the left side of the patient. The five trocars are placed so that two equilateral triangles sharing a common medial angle are created. The surgeon operates through the two most cephalad ports. The assistant operates through the two closest caudad ports. The right-sided, caudad port is used for the liver retractor.

30
With the assistant first retracting the greater curve and then the omentum, the left crus and the greater curve are dissected by the surgeon. The short gastric vessels are taken early to mobilize the fundus.

31
With the fundus mobilized, the phrenoesophageal membrane over the left crus may be dissected until the crural fibers are identified. The entire length of the left crus is mobilized at this time.

32
Right crural dissection is then performed by opening the lesser omentum and mobilizing this to the phrenoesophageal membrane on the right. Anterior and posterior dissection of the right crus will reveal the previously dissected left crus. Care should be taken to preserve the anterior and posterior vagus nerves during this mobilization. Both will be contained by the wrap. A Penrose drain is placed around the esophagus to facilitate more proximal dissection and to assist with creation of the wrap.

33
Once the esophagus is mobilized, the crura are reapproximated posteriorly with heavy permanent sutures to allow the easy passage of a 52-French bougie

34
The posterior aspect of the fundus is then passed behind the esophagus from left to right. The wrap is created over a length of 2.5 to 3 cm with three or four interrupted permanent sutures. This repair should also allow the easy passage of a 52-French bougie . With the bougie removed, the wrap is anchored to the esophagus and the right crus at the hiatus. This helps prevent herniation and slipping. A similar suture is placed on the left. The wrap is anchored anteriorly and posteriorly to the crura with two additional sutures. The wrap is inspected. The suture line should lie just to the right of the middle of the esophagus. The posterior aspect of the wrap should not have redundant stomach, which would imply the wrap was made too far inferior, possibly with the body instead of the fundus.

35
When esophageal motility is poor, then a partial fundoplication may be considered to prevent obstruction to bolus propagation in the esophagus. While this was thought mandatory in all patients with IEM (peristalsis <60% or distal esophageal amplitudes <30 mm Hg), this practice has been questioned in recent years. A total fundoplication can be performed in most patients with IEM (except perhaps those patients with absent peristalsis), without an increase in development of dysphagia. In fact, effective control of reflux with a total fundoplication usually improves premorbid dysphagia and often improves the esophageal motility. When needed, there are many types of partial fundoplications. Regardless of the type used, the initial dissection of the esophagus is the same. If an anterior wrap (Thal, Dor) is to be performed, there is no need to disrupt the posterior attachments of the esophagus (B). The Dor and Thal fundoplications are created with the fundus folded over the anterior aspect of the esophagus. They are anchored to the hiatus and esophagus as in the 360-degree wrap. The experience with these repairs is limited in patients being treated for gastroesophageal reflux. They are more commonly used in patients with achalasia after an anterior myotomy has been performed. If a posterior wrap (Toupet) is to be performed, the entire esophageal dissection is the same as for a 360-degree wrap, and the crura are reapproximated as well. The reconstruction of the posterior fundoplication is initiated by passing the posterior fundus behind the esophagus from left to right. The fundoplication is created by anchoring the posterior fundus to the crura and the esophagus. The most cephalad sutures of the wrap incorporate all three structures (fundus, crus, esophagus). The wrap is anchored posteriorly to the crura with two or three sutures. The fundus is then sutured to the esophagus along the anterolateral aspects, creating a 220- to 250-degree wrap (see C).
 is to be performed, there is no need to disrupt the posterior attachments of the esophagus (B). The Dor and Thal fundoplications are created with the fundus folded over the anterior aspect of the esophagus. They are anchored to the hiatus and esophagus as in the 360-degree wrap. The experience with these repairs is limited in patients being treated for gastroesophageal reflux. They are more commonly used in patients with achalasia after an anterior myotomy has been performed. If a posterior wrap (Toupet) is to be performed, the entire esophageal dissection is the same as for a 360-degree wrap, and the crura are reapproximated as well. The reconstruction of the posterior fundoplication is initiated by passing the posterior fundus behind the esophagus from left to right. The fundoplication is created by anchoring the posterior fundus to the crura and the esophagus. The most cephalad sutures of the wrap incorporate all three structures (fundus, crus, esophagus). The wrap is anchored posteriorly to the crura with two or three sutures. The fundus is then sutured to the esophagus along the anterolateral aspects, creating a 220- to 250-degree wrap (see C).")
36
Absite Question A 56 year-old man is seen 2 years after a laparoscopic Nissen fundoplication for GERD. His pre-operative work-up 2 years ago demonstrated normal esophageal motility, and pH probe testing showed that reflux was the cause of his symptoms. He now has recurrent symptoms of GE reflux. A Barium swallow is performed.

37
Which is not true about this patient?
A. Redo operation is as effective as primary antireflux operation for ameliorationg reflux symptoms Transabdominal laparoscopic redo operation is contraindicated Redo operation has an increased complication rate The cause is related to technical performance of the initial operation Manometry is helpful in planning operative therapy This patient has a slipped Nissen fundoplication, in which the fundoplication wrap slides down onto the proximal stomach. Approximately 10% of patients undergoing laparoscopic antireflux operation experience failure of some sort with a range of reported values from 3-30%. The most frequent post-op complaint is recurrent reflux, followed by dysphagia, then reflux and dysphagia together. Failures are usually related to technical problems with the original antireflux procedure or to poor patient selection when an esophageal motility disorder is not recognized pre-op with manometry. Pt’s with recurrent reflux post-op can be managed conservatively with medication. Operative intervention can be performed successfully via a laparoscopic approach, but the complication rate is higher than that of initial antireflux procedures (as high as 53%).
.")
38
Absite Question Four years ago, a 47 year-old woman had a laparoscopic fundoplication. It failed after three years and she had severe, recurrent gastroesophageal symptoms. Through a celiotomy incision, the surgeon performed a redo-fundoplication with a 360-degree, 2 cm wrap around a 56 Fr dilator. For the past three months she has had severe early satiety, postprandial epigastric pain, and weight loss. The most likely cause of these symptoms is: A. The wrap is too tight B. The wrap is too loose C. Vagal injury D. Irritable bowel syndrome E. Esophageal motor disorder With injury to the vagus, pts have gastric stasis resulting in retention of food within the stomach for several hours. This may be accompanied by a feeling of fullness and occasionally abdominal pain. In rarer cases, it may be associated with a functional gastric outlet obstruction.

39
Absite Question Barrett’s esophagus
A) will usually regress after Nissen fundoplication B) carries an increased risk of squamous cell carcinoma C) is an indication for esophagectomy D) should be followed by endoscopic surveillance E) is a contraindication to laparoscopic Nissen fundoplication Injured squamous cells in the distal esophagus can be replaced either by more squamous cells or, through the process of metaplasia, by columnar cells (Barrett’s esophagus). Chronic gastroesophageal reflux both injures the squamous epithelium and provides the abnormal esophageal environment that stimulates repair through columnar cell metaplasia. Up to three different types of columnar epithelia can be found in Barrett’s esophagus: (1) specialized intestinal metaplasia, which has a villiform surface and intestinal-type crypts lined by mucus-secreting columnar cells and goblet cells; (2) gastric fundic-type epithelium; and (3) junctional-type epithelium. Specialized intestinal metaplasia is the most common, and dysplasia and carcinoma in Barrett’s esophagus are almost invariably associated with specialized intestinal metaplasia. Diagnosis Barrett’s esophagus is more common in men than in women, with a 3:1 male predominance (the average age at diagnosis is 55 years). Barrett’s esophagus and severe GERD are uncommon in blacks. The prevalence of Barrett’s esophagus increases with age up to 70 years. Barrett’s esophagus often remains stable, and no conclusive evidence indicates that either ongoing severe reflux or effective treatment of reflux alters the progression of Barrett’s esophagus despite the association with cancer. The extent of intestinal metaplasia is related to the status of the LES and the degree of esophageal acid exposure.[205] Barrett’s esophagus can be found in 10% to 15% of patients who have endoscopic examinations for symptoms of GERD. Most patients with Barrett’s esophagus do not seek medical attention for esophageal symptoms and may have no symptoms of GERD. GERD associated with Barrett’s esophagus, however, often is severe, with esophageal ulceration, stricture, and hemorrhage. Barrett’s esophagus has been identified in approximately 1 in 10 persons with erosive esophagitis and 1 in 3 persons with a peptic esophageal stricture. In one study, small areas of specialized columnar epithelium with intestinal metaplasia were identified histologically in the region of the gastroesophageal junction in 18% of patients undergoing endoscopy. This finding indicates that “short segment Barrett’s esophagus” may be common in the general population. Whether short-segment Barrett’s esophagus represents a substantial risk factor for esophageal adenocarcinoma is not yet clear. Cancer registries in the United States document that the rate of increase in the frequency of adenocarcinoma of the distal esophagus and gastric cardia exceeds that for any other type of cancer. Most of these tumors arise from Barrett’s epithelium, a finding suggesting that the prevalence of specialized intestinal metaplasia that predisposes to adenocarcinoma is far more common in the general population than had been appreciated. Carcinogenesis in Barrett’s esophagus may involve activation of proto-oncogenes, dysfunction of tumor suppressor genes, or both. Molecular studies have shown that genomic abnormalities in Barrett’s esophagus result in the loss of heterozygosity in a variety of tumor suppressor genes including 17P (encoding p53), 5Q (APC, MCC), 18Q (DCC), and 13Q (RBI). Tumor suppressor genes (p53, P16), oncogenes (c-erbB-2, H-ras, K-ras, cyclin D1, and src), and growth factors or receptors (transforming growth factor-α, epidermal growth factor receptor) are implicated in the 1143 malignant transformation of Barrett’s esophagus and may soon serve as prognostic indicators. Notably, the degree of angiogenesis is not a significant prognostic indicator of esophageal cancer. Flow cytometry has also been used to detect aneuploidy in Barrett’s esophagus. True dysplasia in Barrett’s esophagus represents a neoplastic alteration of the columnar epithelium and is widely regarded as the precursor of invasive malignancy. Unfortunately, dysplasia is not an ideal biomarker of malignant potential in Barrett’s epithelium for several reasons. The histologic interpretation of dysplasia is largely subjective, and the natural history of dysplasia is not clear. Dysplastic Barrett’s mucosa often is indistinguishable from nondysplastic mucosa, and small foci of dysplasia can be easily missed. Despite limitations, dysplasia remains the best biomarker for evaluating malignancy in Barrett’s esophagus. Approximately one third of patients with high-grade dysplasia in Barrett’s esophagus either already have or will develop invasive cancer within several years. The prevalence of adenocarcinoma at the time of diagnosis of Barrett’s esophagus is approximately 8%. The high incidence of esophageal adenocarcinoma has led to the recommendation that all patients with Barrett’s esophagus undergo prospective screening for the development of dysplasia and carcinoma. Although this approach seems reasonable, the benefits of screening in Barrett’s esophagus have not been proven by a prospective clinical trial.
 will usually regress after Nissen fundoplication. B) carries an increased risk of squamous cell carcinoma. C) is an indication for esophagectomy. D) should be followed by endoscopic surveillance. E) is a contraindication to laparoscopic Nissen fundoplication. Injured squamous cells in the distal esophagus can be replaced either by more squamous cells or, through the process of metaplasia, by columnar cells (Barrett’s esophagus). Chronic gastroesophageal reflux both injures the squamous epithelium and provides the abnormal esophageal environment that stimulates repair through columnar cell metaplasia. Up to three different types of columnar epithelia can be found in Barrett’s esophagus: (1) specialized intestinal metaplasia, which has a villiform surface and intestinal-type crypts lined by mucus-secreting columnar cells and goblet cells; (2) gastric fundic-type epithelium; and (3) junctional-type epithelium. Specialized intestinal metaplasia is the most common, and dysplasia and carcinoma in Barrett’s esophagus are almost invariably associated with specialized intestinal metaplasia. Diagnosis. Barrett’s esophagus is more common in men than in women, with a 3:1 male predominance (the average age at diagnosis is 55 years). Barrett’s esophagus and severe GERD are uncommon in blacks. The prevalence of Barrett’s esophagus increases with age up to 70 years. Barrett’s esophagus often remains stable, and no conclusive evidence indicates that either ongoing severe reflux or effective treatment of reflux alters the progression of Barrett’s esophagus despite the association with cancer. The extent of intestinal metaplasia is related to the status of the LES and the degree of esophageal acid exposure.[205] Barrett’s esophagus can be found in 10% to 15% of patients who have endoscopic examinations for symptoms of GERD. Most patients with Barrett’s esophagus do not seek medical attention for esophageal symptoms and may have no symptoms of GERD. GERD associated with Barrett’s esophagus, however, often is severe, with esophageal ulceration, stricture, and hemorrhage. Barrett’s esophagus has been identified in approximately 1 in 10 persons with erosive esophagitis and 1 in 3 persons with a peptic esophageal stricture. In one study, small areas of specialized columnar epithelium with intestinal metaplasia were identified histologically in the region of the gastroesophageal junction in 18% of patients undergoing endoscopy. This finding indicates that short segment Barrett’s esophagus may be common in the general population. Whether short-segment Barrett’s esophagus represents a substantial risk factor for esophageal adenocarcinoma is not yet clear. Cancer registries in the United States document that the rate of increase in the frequency of adenocarcinoma of the distal esophagus and gastric cardia exceeds that for any other type of cancer. Most of these tumors arise from Barrett’s epithelium, a finding suggesting that the prevalence of specialized intestinal metaplasia that predisposes to adenocarcinoma is far more common in the general population than had been appreciated. Carcinogenesis in Barrett’s esophagus may involve activation of proto-oncogenes, dysfunction of tumor suppressor genes, or both. Molecular studies have shown that genomic abnormalities in Barrett’s esophagus result in the loss of heterozygosity in a variety of tumor suppressor genes including 17P (encoding p53), 5Q (APC, MCC), 18Q (DCC), and 13Q (RBI). Tumor suppressor genes (p53, P16), oncogenes (c-erbB-2, H-ras, K-ras, cyclin D1, and src), and growth factors or receptors (transforming growth factor-α, epidermal growth factor receptor) are implicated in the malignant transformation of Barrett’s esophagus and may soon serve as prognostic indicators. Notably, the degree of angiogenesis is not a significant prognostic indicator of esophageal cancer. Flow cytometry has also been used to detect aneuploidy in Barrett’s esophagus. True dysplasia in Barrett’s esophagus represents a neoplastic alteration of the columnar epithelium and is widely regarded as the precursor of invasive malignancy. Unfortunately, dysplasia is not an ideal biomarker of malignant potential in Barrett’s epithelium for several reasons. The histologic interpretation of dysplasia is largely subjective, and the natural history of dysplasia is not clear. Dysplastic Barrett’s mucosa often is indistinguishable from nondysplastic mucosa, and small foci of dysplasia can be easily missed. Despite limitations, dysplasia remains the best biomarker for evaluating malignancy in Barrett’s esophagus. Approximately one third of patients with high-grade dysplasia in Barrett’s esophagus either already have or will develop invasive cancer within several years. The prevalence of adenocarcinoma at the time of diagnosis of Barrett’s esophagus is approximately 8%. The high incidence of esophageal adenocarcinoma has led to the recommendation that all patients with Barrett’s esophagus undergo prospective screening for the development of dysplasia and carcinoma. Although this approach seems reasonable, the benefits of screening in Barrett’s esophagus have not been proven by a prospective clinical trial.")
40
Endoscopic Therapy Attempt to augment the LES by Suturing – EndoCinch
Radiofrequency energy – Stretta Plexiglass injection – polymethylmethacrylate Biocompatible polymer injection -- Enteryx Recently several endoscopic techniques have been developed for the treatment of GERD. These procedures have sparked significant interest, because they each promise a mechanical treatment for reflux with less invasion than a fundoplication. These techniques attempt to augment the LES by suturing (EndoCinch, Bard), radiofrequency energy (Stretta, Curon Medical), Plexiglas injection (polymethylmethacrylate), or biocompatiable polymer injection (Enteryx, Boston Scientific).
, radiofrequency energy (Stretta, Curon Medical), Plexiglas injection (polymethylmethacrylate), or biocompatiable polymer injection (Enteryx, Boston Scientific).")
41
Plication/Sewing Techniques
First developed in the mid ’80’s Allow placement of sutures into the gastric cardia, thereby augmenting the barrier effect of the GEJ Bard EndoCinch The first endoscopic suturing system was developed in the mid 1980’s and has undergone several subsequent modifications that allow the endoscopist to place sutures into the gastric cardia, thereby augmenting the barrier effect of the gastroesophageal junction. The first endoscopic sewing and plication instrument created is the Bard EndoCinch system.

42
The EndoCinch consists of a sewing capsule that is attached to the distal end of a gastroscope. The capsule has a hollow chamber through which esophageal tissue can be suctioned. A handle mounted to the biopsy port on the gastroscope then drives a hollow-core needle containing suture material through the tissue to create a stitch through the submucosa. A second gastroscope must be used to fasten the ends of the suture together.

43
EndoCinch Filipi CJ, Lehman GA, Rothstein RI et al. “Transoral, flexible endoscopic suturing for treatment of GERD: a multicenter trial.” Gastrointestinal Endoscopy 2001; 53: Suggested that endoscopic gastric plication is a safe procedure and, at a 6-month follow-up, that 2/3 of pts undergoing the procedure were successfully treated. A pivotal multicenter trial for the EndoCinch was published in 2001 and provided data for the FDA approval of the device for the treatment of GERD. The trial suggested that endoscopic gastric plication is a safe procedure and, at a 6-month follow-up, that 2/3 of pts undergoing the procedure were successfully treated.

44
EndoCinch (cont) Inclusion Criteria Exclusion Criteria
Three or more episodes of heartburn a week when off antisecretory meds Successful response to and reliance upon antisecretory meds for GERD Abnormal acid reflux on ambulatory pH monitoring Exclusion Criteria Dysphagia BMI greater than 40 GERD refractory to PPIs Hiatal hernia greater than 2 cm in length

45
EndoCinch (cont) Treatment success defined as a decrease in the heartburn severity score by 50% in addition to a reduction in the use of antireflux medications to fewer to 4 doses per month. 64 patients were enrolled 33 pts (52%) – gastroplication in a linear configuration 31 (48%) – gastroplication in a circumferential plication No difference in outcomes between the 2 groups
 – gastroplication in a linear configuration. 31 (48%) – gastroplication in a circumferential plication. No difference in outcomes between the 2 groups.")
46
Results: Mean heartburn scores fell from a preprocedure score of 62.7 to mean scores of 16.7 and 17 and 3 and 6 months postprocedure Percent total time the pH was < 4, total number of reflux episodes, and percent upright pH time was lower than 4 were all significantly improved, but none returned to normal range Regurgitation scores improved significantly Quality of life scores were improved for social functioning and bodily pain and 62% of pts at 3 and 6 month f/u were taking less than 4 doses of medication per month

47
Results (cont) No significant change found in LES resting pressure or length No significant effect on mucosal healing Adverse events included pharyngitis (31%), vomiting (14%), and abdominal pain (14%), and chest pain (16%) One patient experienced a suture microperforation that was treated conservatively with IV antibiotics and brief hospitalization
, vomiting (14%), and abdominal pain (14%), and chest pain (16%) One patient experienced a suture microperforation that was treated conservatively with IV antibiotics and brief hospitalization.")
48
EndoCinch (cont) Chen YK, Raijman I, Ben-Menachem T et al. “Long-term outcomes of endoluminal gastroplication: a U.S. multicenter trial.” Gastrointestinal Endoscopy : Prospective, multicenter trial which enrolled 85 patients to be treated with endoluminal gastroplication followed over 2 years Long term study

49
Results: Shortcomings of study
51% of patients had no or occasional GERD symptoms 73% and 69% were completely off PPIs or at 12 and 24 months postprocedure Reduction in the mean annual medication cost from $1564 per year preprocedure to $157 one year postprocedure (cost redux of 88%) Shortcomings of study Does not contain a nonplication sham group Trends toward increased symptoms over time suggestive of degradation of repair over time
 Shortcomings of study. Does not contain a nonplication sham group. Trends toward increased symptoms over time suggestive of degradation of repair over time.")
50
EndoCinch (cont) Schiefke I et al. “Long term failure of endoscopic gastroplication (EndoCinch)”. Gut 2005; 54: Evaluated prospectively long term outcome after EndoCinch 70 patients at a single referral center Patients interviewed with a standard questionaire regarding symptoms, medication use, in addition to f/u with endoscopy, 24h pH monitoring, and esophageal manometry

51
Results: 18 months after EndoCinch 56/70 patients (80%) were considered treatment failures as their heartburn symptoms did not improve or PPI medication exceeded 50% of initial dose Endoscopy showed all sutures in situ in 12/70 (17%), while no sutures remained in 18/70 (26%) No significant changes in 24h pH monitoring or LES pressure
 were considered treatment failures as their heartburn symptoms did not improve or PPI medication exceeded 50% of initial dose. Endoscopy showed all sutures in situ in 12/70 (17%), while no sutures remained in 18/70 (26%) No significant changes in 24h pH monitoring or LES pressure.")
52
Conclusion: Long term outcome is disappointing probably due to suture loss in the majority of patients

53
Radiofrequency Thermal Therapy -- Stretta
Delivery of low-power, temperature-controlled radiofrequency energy to the GEJ Two mechanisms 1. mechanically altering the GEJ 2. inducing the ablation of nerves that trigger transient lower esophageal relaxation Another endoscopic approach involves the delivery of low-power, temperature-controlled radiofrequency energy to the GEJ, more specifically the muscularis propria. RF energy is thought to enhance LED function by two mechanisms -- the first of which is mechanically altering the GEJ. The thermocouple-controlled RF delivery results in the propagation of a circumscribed area of thermal coagulative necrosis that targets the smooth muscle at or near the GEJ and cardia. Tissue contraction and remodeling that results lead to eventual tightening and reduced compliance of the GEJ. The second mechanism by which RF delivery enhances LES function is by inducing the ablation of nerves that trigger transient lower esophageal sphincter relaxations.

54
Radiofrequency Thermal Therapy -- Stretta
The Stretta procedure is most commonly performed on an outpatient basis in the endoscopy inot or ambulatory surgery center with the use of conscious sedation. The Stretta catheter is comprised of a bougie tip,a balloon-basket assembly, and four electrode delivery sheaths positioned radially around the balloon. The catheter is placed transorally over a guidewire and positioned 1 cm above the GE junction. The balloon is then inflated to a low pressure and four nickel titanium needles are deployed 2) Temperature-controlled levels of radiofrequency (RF) energy is delivered to each electrode deployed in the submucosa while the overlying mucosa is cooled with irrigation. The target tissue temperature is 85 degrees Celsius. On average, 14 lesion sets are created in the region for 1 cm above to 2 cm below the GEJ. 3) When the lesions heal, the barrier function of the LES is improved.
 Temperature-controlled levels of radiofrequency (RF) energy is delivered to each electrode deployed in the submucosa while the overlying mucosa is cooled with irrigation. The target tissue temperature is 85 degrees Celsius. On average, 14 lesion sets are created in the region for 1 cm above to 2 cm below the GEJ. 3) When the lesions heal, the barrier function of the LES is improved.")
55
Stretta Wolfsen HC and Richards WO. “The Stretta Procedure for the Treatment of GERD: A registry of 558 patients.” Journal of Laparoendoscopic and Advanced Surgical Techniques 2002 558 patients, 33 institutions 6 months of follow-up Survey administered which assessed GERD severity, percentage of GERD symptom control, satisfaction, and antisecretory medication use

56
Results At baseline, the median percentage of GERD symptom control while on drugs was 50%, compared with 90% after Stretta Satisfaction with symptom control was 26% versus 77% after Stretta Median requirement at baseline was double dose of PPI versus antacids prn after Stretta Most subjects (90%) would recommend Stretta to a friend
 would recommend Stretta to a friend.")
57
Stretta Triadafilopolous et al: reported 6- and 12- month results of an open label trial of Stretta Prospective multicenter trial involving 118 patients who had chronic heartburn or regurgitation, abnormal esophageal acid exposure, hiatal hernia less than 2 cm, and mild esophagitis At 12 mo: improvement in heartburn score, GERD score, and quality of life. PPI use decreased from 88% to 30%. Esophageal acid exposure improved significantly, although no improvement in the incidence and severity of esophagitis In additian looked at objective outcomes such as acid exposure and esophagitis.

58
randomized, double-blinded, sham controlled trial of radiofrequency energy to the gastroesophageal junction for the treatment of GERD

59
Patient Criteria heartburn or acid regurgitation at least partially responsive to and requiring daily antacid medications age 18 years 24-hour pH study (off medications) showing abnormal esophageal acid exposure (4%) or a DeMeester score of 14.7 esophageal manometry showing normal esophageal peristalsis and sphincter relaxation EGD, on medications, showing no esophagitis worse than grade II (i.e., no substantial ulcerations), no hiatal hernia 2 cm long, and no Barrett’s esophagus no coagulation disorders, mechanical prostheses, prominent dysphagia, or unstable disorders.
 showing abnormal esophageal acid exposure (4%) or a DeMeester score of esophageal manometry showing normal esophageal peristalsis and sphincter relaxation. EGD, on medications, showing no esophagitis worse than grade II (i.e., no substantial ulcerations), no hiatal hernia 2 cm long, and no Barrett’s esophagus. no coagulation disorders, mechanical prostheses, prominent dysphagia, or unstable disorders.")
60
A total of 64 patients were randomized (35 to
active treatment and 29 to sham) between May 2000 and February 2001 (Figure 1).
 between May 2000 and. February 2001 (Figure 1).")
61
Active treatment significantly improved heartburn scores, GERD-specific quality of life scores, and general quality of life scores compared with sham treatment. At 6 months, active vs. sham patients had significantly improved heartburn scores (mean decrease, 1.6 vs. 0.6 and GERD HRQL scores (mean decrease 13 points vs. 3 points. Radiofrequency energy delivery did not significantly decrease medication use beyond that achievable with a sham procedure followed by a medication- withdrawal protocol. It also did not significantly decrease esophageal acid exposure at 6 months, suggesting that this procedure should not be used in patients with severe erosive esophagitis.

62
Stretta Patients were offered the Stretta procedure if they had documented GERD and did not have a hiatal hernia larger than 2 cm, LES pressure less than 8 mmHg, or Barrett’s esophagus. Patients with larger hiatal hernias, LES pressure less than 8 mmHg, or Barrett’s were offered LF. This study compares the Stretta with Laparoscopic Nissen Fundoplication

63
Results of 65 patients undergoing the Stretta procedure.
Complete response (CR) is defined as no longer needing to take PPIs, partial response (PR) is defined as a reduction in PPIs to once per day or less, and no response (NR) is defined as remaining on preoperative twice-daily doses of PPIs. CR was achieved in 58%, PR was achieved in 31%, and NR was seen in 11% of patients after Stretta.
 is defined as no longer needing to take PPIs, partial response (PR) is defined as a reduction in PPIs to once per day or. less, and no response (NR) is defined as remaining on preoperative. twice-daily doses of PPIs. CR was achieved in 58%, PR was achieved. in 31%, and NR was seen in 11% of patients after Stretta.")
64
Results of 75 patients undergoing laparoscopic fundoplication
(LF). CR was achieved in 97%, PR was achieved in 3%, and NR was not seen in any patient after LF.
. CR was achieved in 97%, PR was achieved in 3%, and NR was. not seen in any patient after LF.")
67
Stretta Conclusions – Although the incidence of complications is decreased compared with operative intervention, success of therapy does not approach that of surgical intervention After Stretta 30-50% of patients still require PPI therapy

68
While not all patients may have a complete response to
Stretta, it is an effective, less invasive therapy for GERD that does not burn any bridges. Stretta is a reasonable procedure to use in well-selected patients. It should not be used in patients with Barrett’s esophagus, LES pressure less than 8 mm Hg, or large hiatal hernia (2 cm). Patients with long segment Barrett’s have altered mucosal landmarks at the GE junction, making it difficult to identify the proper site of treatment. In addition, many of the Barrett’s patients have severe disease in which normalization of acid and non-acid refluxate should be achieved. The Stretta procedure does not normalize esophageal acid exposure in all patients; therefore, we believe it should be considered inadequate therapy for this population. Patients with small hiatal hernias will have some diaphragm around the area where the needle electrodes are positioned for treatment. This tissue barrier provides a safety zone, preventing RF thermal injury to vital structures in the mediastinum, so patients who have hiatal hernias larger than 2 cm are not offered the Stretta procedure. Patients with large hiatal hernias and inadequate LES barriers (LESP 8 mmHg) are better suited for LF, where the anatomic defect and the mechanical barrier to reflux can be restored. As better techniques of treatment using RF energy are developed, indications and patient selection may change. [It may have specific utility in morbidly obese patients, patients with previous gastric resection or gastric bypass, or after failed fundoplication. A number of obese patients simply do not want to undergo gastric bypass surgery but desire surgical treatment of their GERD. Morbidly obese patients have a higher rate of failure after fundoplication than do patients of normal weight. It has been speculated that abdominal pressure contributes to the breakdown of the repair and leads to recurrent reflux. Performance of the Stretta in a morbidly obese patient is no more time-consuming or technically demanding than in a patient with a normal BMI.]
. Patients with long segment Barrett’s have altered mucosal landmarks at the GE junction, making it difficult to identify the proper site of treatment. In addition, many of the Barrett’s patients have severe disease in which normalization of acid and non-acid refluxate should be achieved. The Stretta procedure does not normalize esophageal acid exposure in all patients; therefore, we believe it should be considered inadequate therapy for this population. Patients with small hiatal hernias will have some diaphragm around the area where the needle electrodes are positioned for treatment. This tissue barrier provides a safety zone, preventing RF thermal injury to vital structures in the mediastinum, so patients who have hiatal hernias larger than 2 cm are not offered the Stretta procedure. Patients with large hiatal hernias and inadequate LES barriers (LESP 8 mmHg) are better suited for LF, where the anatomic defect and the mechanical barrier to reflux can be restored. As better techniques of treatment using RF energy are developed, indications and patient selection may change. [It may have specific utility in morbidly obese patients, patients with previous gastric resection or gastric bypass, or after failed fundoplication. A number of obese patients simply do not want to undergo gastric bypass surgery but desire surgical treatment of their GERD. Morbidly obese patients have a higher rate of failure after fundoplication than do patients of normal weight. It has been speculated that abdominal pressure contributes to the breakdown of the repair and leads to recurrent reflux. Performance of the Stretta in a morbidly obese patient is no more time-consuming or technically demanding than in a patient with a normal BMI.]")
69
Injection/implantation techniques -- Enteryx
Injectable biocompatible solution consisting of 8% ethylene vinyl alcohol copolymer mixed in dimethyl sulfoxide When injected into the LES, the solution interacts with the surrounding fluid to become an inert spongy solid mass Mechanism: may impart an alteration in the compliance of tissues preventing sphincter shortening and improving the barrier function of the GEJ

70
Enteryx After routine upper endoscopy, a 24 gauge catheter is used to inject Enteryx solution at the squamocolumnar junctionby advancing the needle into the LES muscle. The solution is injected very slowly and 1 – 2 cc is placed in 4 quadrants around the LES. After injecting the Enteryx the needle is left in the injection site for 20 seconds thereafter to allow the solution to solidify and prevent leakage. The procedure is done in an outpatient setting and patients can be expected to experience some post-procedure discomfort that is typically amenable to po analgesics. Also because some patients may note transient dysphagia post-procedure, they are instructed to stay on a soft mechanical diet for a few days.

71
Enteryx Cohen LB, Johnson DA, Ganz RA et al “Enteryx implantation for GERD: expanded multicenter trial results and interim postapproval follow-up to 24 months.” Gastrointestinal Endoscopy May 2005 Open-label, international clinical trial conducted in 144 PPI—dependent patients with GERD with f/u at 6 and 12 months Primary outcome: PPI use Secondary outcome: GERD health-related quality of life and esophageal acid exposure

72
Results: At 12 months PPI use was reduced by greater than 50% in 84% of treated pts GERD health-related quality of life < 11% in 78% of patients Esophageal acid exposure was reduced by 31%

73
Enteryx However, since this study Enteryx has been recalled. The serious adverse events that forced this recall involve unrecognized transmural injections of ENTERYX® into structures surrounding the esophagus. This events occurred even though fluoroscopy was used throughout the procedure. Three weeks was the longest period that we know of in which a transmural injection went unrecognized by a physician. Accurate estimates of the number of adverse events associated with transmural injection of ENTERYX are not available. Reports received thus far suggest ENTERYX® has been injected into various sites outside the esophagus including the mediastinum, pleural space and the aorta. When injected into the aorta, ENTERYX® may migrate to and occlude blood vessels which supply other organs including the kidneys. One reported death was due to injection of the ENTERYX® into the wall of the aorta, which resulted in an aorto-enteric fistula. Another patient experienced a partial reduction in renal function due to partial embolization.

74
Conclusions on Endoscopic Mgmt of GERD
Techniques need to be further studied in sham-controlled protocol Long term follow-up suggest a declining effect of treatment with pts returning to PPI use -- more long term f/u studies necessary Future studies should improve targeting of which patients benefit, further elucidate the mechanisms of action, and provide detailed comparisons to alternative treatments. T

75
Future of Endoscopic Therapy
As a substitute for long-term medical therapy for the pt with mildly symptomatic GERD As adjuncts to ongoing pharmacologic treatment In patients with a failed surgical fundoplication

Similar presentations
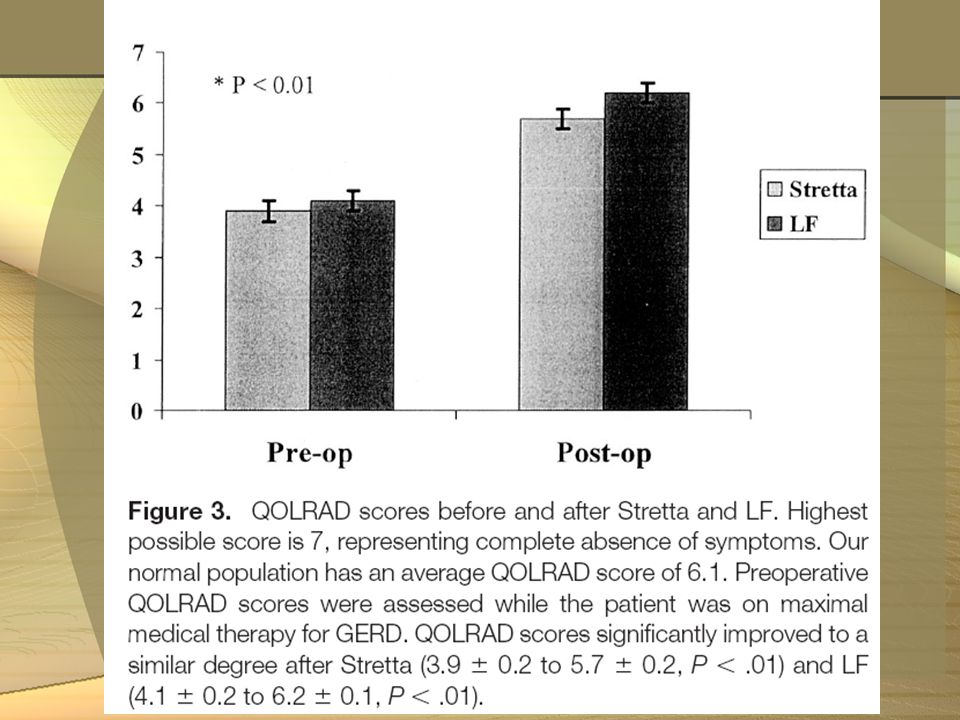
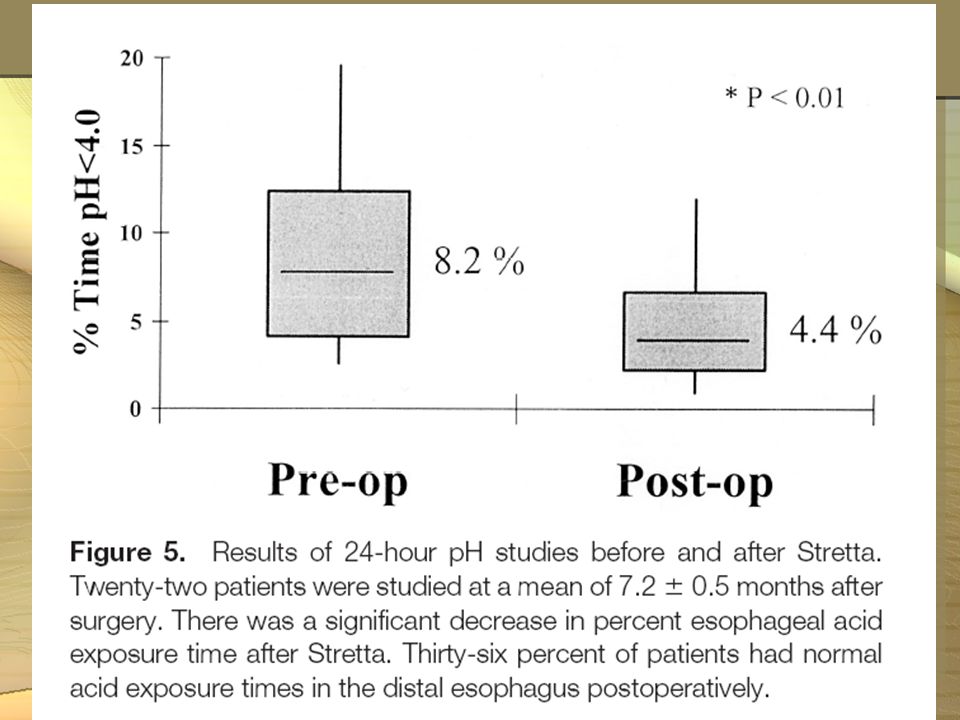

 has Barrett’s esophagus diagnosed on upper endoscopy. Which of.>")




 Rory Loveland Paramedic class ’08-’09.>")


 Joint Hospital Grand Round 25.1.2014 Prepared by Siu Yin Yu, Eva North District.>")





>")



