Download presentation
Presentation is loading. Please wait.

2
Tehran university of medical science Baharlou hospital

3
MD,M.pouradineh N.azarakhshi

4
Ms. Leila Asgari /32 years old/ married She has 3 babies JOB: home keeper Source of information : patient (reliable) Time of admission in the ward: 93/07/10
 Time of admission in the ward: 93/07/10.")
5
spotting Abdominal pain vertigo and headache Fatigue urine incontinency and fecal incontinency

6
Methyldopa Folic acid vitamins

7
3 NVD delivery which last one was 4 days before Brain tumor surgery (lipoid cyst) 10 years ago HTN ovarian cyst surgery 8 years ago
 10 years ago HTN ovarian cyst surgery 8 years ago")
8
: ecchymosis in hands

9
Peripheral vascular sys : From 1 month ago she experienced edema which got worth when she came to hospital. as you see it seems 3+

10
mmHg130/80BP: RR:18 Temprature:36 Height:163 cm weight:80 Kg PR: 62

11
ecchymosis in hands skin :icteric Sclera :icteric Generalized edema (+4)
")
12
DATEWBCRBCHb HCT 7/1016.25.0715.548.3 7/11 18.33.8312.338.7 7/1218.63.029.531.2 7/1321.43.3310.232.8 7/14163.139.831.6

13
DATEMCVMCHMCHC PLATELET 7/1098.432.533.1117 7/1110132.1 102 7/12103.330.829.876 7/1398.530.631.388 7/1410131.33175

14
DATE NEUTROPHIL LYMPHOCYTE MONOCYTEEUSINOPHIL 7/10801532 7/11851221 7/12871021 7/13851221 7/14811421

15
*PT control time : 12 s DATE PT PATIENTINRPTT PATIENT TIME 7/10 ---------------- ------------------------------- 7/1115.71.740 7/1219.12.437 7/13182.338 7/14161.838

16
DATEFBSUREACreatinineUric acid 7/10---------- ----------------------------------------------------- 7/11 -------------- 451.68.4 7/12100621.88.3 7/13119681.58.5 7/14108561.15.3

17
DATESGOTSGPTALPNAK 7/10 ---------------------------------------------------------- 7/11135267988--------2.9 7/1283143673141---------- 7/1357517781384.4 7/1447506071384.4

18
DATETotal bilirubinDirect bilirubinLDH 7/10--------------------- ----------------------------------------- 7/119.15.8780 7/129.65.8788 7/137.13.2820 7/14 ---------------------------------------------------------------------

20
The acronym HELLP was coined by Weinstein in 1982 to describe a syndrome consisting of Hemolysis, Elevated liver enzymes and Low platelet count.

21
HELLP Syndrome - 0.2 to 0.6% of all pregnancies.

22
The findings of this multisystem disease are attributed to- Abnormal vascular tone Vasospasm Coagulation defects This vasculopathy either limited to hepatic segment or diffusely throughout liver. More commonly involves smaller terminal arterioles yielding a characteristic histological features

24
HELLP SyndromePre Eclampsia ParityMultiparousNulliparous Age> 25yrs 45 yrs Other relevant history White race H/O Poor pregnancy outcome Family history of PIH Chronic hypertension Diabetes mellitus Multifetal gestation Less Antenatal visit

25
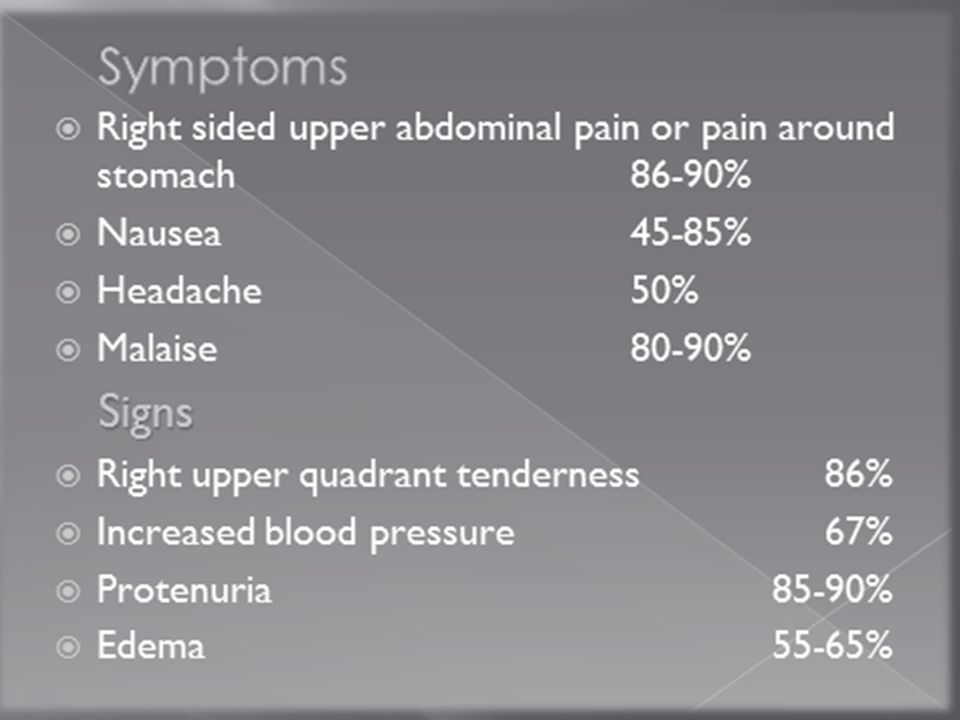
Young, White woman ≥25yrs Multiparous Heavy with severe generalized edema 2 nd or 3 rd trimester c/o Rt. Upper quadrant pain since few days for which she might be taking antacids. c/o malaise since few days, which may be out of proportion to the discomfort expected by the stage of pregnency Blood pressure is only slightly raised. Edema & proteinuria may or may not be present

26
So, any pregnant woman presenting in OPD with malaise or viral like illness in 2 nd or 3 rd trimester should be evaluated with CBC and Liver function tests

27
Thrombocytopenia occurs first followed by raised liver enzymes and last is hemolysis. Laboratory criteria for diagnosis — 1. Low platelets - < 100,000/µL 2. Elevated liver enzymes – AST > 70 IU/L - LDH > 600 IU/L 3. Hemolysis – Abnormal peripheral smear - Total bilirubin > 1.2mg%

28
Leukocytosis Coagulation factors If DIC is not present – PT, aPPT, S. Fibrinogen will be normal If fibrinogen < 300 mg/dl along with other lab abnormality – DIC is suspected Positive D-dimer test is more sensitive indicator of sub clinical coagulopathy and may be positive before other coagulation studies are abnormal. Proteinuria S. uric acid – raised Hypogycemia- persistent, profound hypoglycemia inspite of repeated glucose transfusion is peculiar to advanced HELLP syndrome.

29
1. Diseases related to pregnancy Benign thrombocytopenia of pregnancy Acute fatty liver of pregnancy (AFLP) 2. Infectious and inflammatory diseases, not specifically related to pregnancy: Virus hepatitis Cholangitis Cholecystitis Upper urinary tract infection Gastritis Gastric ulcer Acute pancreatitis
 2. Infectious and inflammatory diseases, not specifically related to pregnancy: Virus hepatitis Cholangitis Cholecystitis Upper urinary tract infection Gastritis Gastric ulcer Acute pancreatitis.")
30
3. Thrombocytopenia Immunologic thrombocytopenia (ITP) Folate deficiency Systemic lupus erythematosus (SLE) Antiphospholipid syndrome (APS) 4. Rare diseases that may mimic HELLP syndrome Thrombotic thrombocytopenic purpura (TTP) Haemolytic uremic syndrome (HUS)
 Folate deficiency Systemic lupus erythematosus (SLE) Antiphospholipid syndrome (APS) 4. Rare diseases that may mimic HELLP syndrome Thrombotic thrombocytopenic purpura (TTP) Haemolytic uremic syndrome (HUS).")
31
Maternal complications Eclampsia Abruptio placentae DIC Acute renal failure Severe ascites Cerebral oedema Pulmonary oedema Wound hematoma/infection

32
Subcapsular liver hematoma Liver rupture Hepatic infarction Recurrent thrombosis Retinal detachment Cerebral infarction Cerebral Haemorrhage Maternal death

33
Perinatal death IUGR Preterm delivery Neonatal thrombocytopenia RDS

34
Spontaneous rupture of a Subcapsular liver haematoma in pregnancy is a rare, but life threatening complication. Occurs 1 in 40,000 to 1 in 250,000 deliveries and about 1% to < 2% of the cases with the HELLP syndrome. Rupture most often occurs in the right liver lobe. The symptoms are sudden-onset severe pain in the epigastric and right upper abdominal quadrant radiating to the back, right shoulder pain, anaemia and hypotension. The condition may be diagnosed by ultrasound, CT or magnetic resonance imaging (MRI) examination. Hepatic rupture may also occur in the post-partum period.
 examination. Hepatic rupture may also occur in the post-partum period..")
35
Identification - clinical features - lab findings - D/D from other condition Admission to hospital S tabilization IV line,Cross match Catheterization Respi assessment Fetal assessment (NST,BPP,Color doppler ) Transport to tertiary care centre or latency for 24- 48 hrs Termination of pregnancy Conservative approach for 48-72 hrs (<32wks POG, Partial HELLP,Tertiary health cenre) Rebound / Resolution ● Monitor by lab Ix ● Stop MgSO4 24 hrs of delivery ● Continue antihypertensive & steroid
 Transport to tertiary care centre or latency for hrs Termination of pregnancy Conservative approach for hrs (<32wks POG, Partial HELLP,Tertiary health cenre) Rebound / Resolution ● Monitor by lab Ix ● Stop MgSO4 24 hrs of delivery ● Continue antihypertensive & steroid")
36
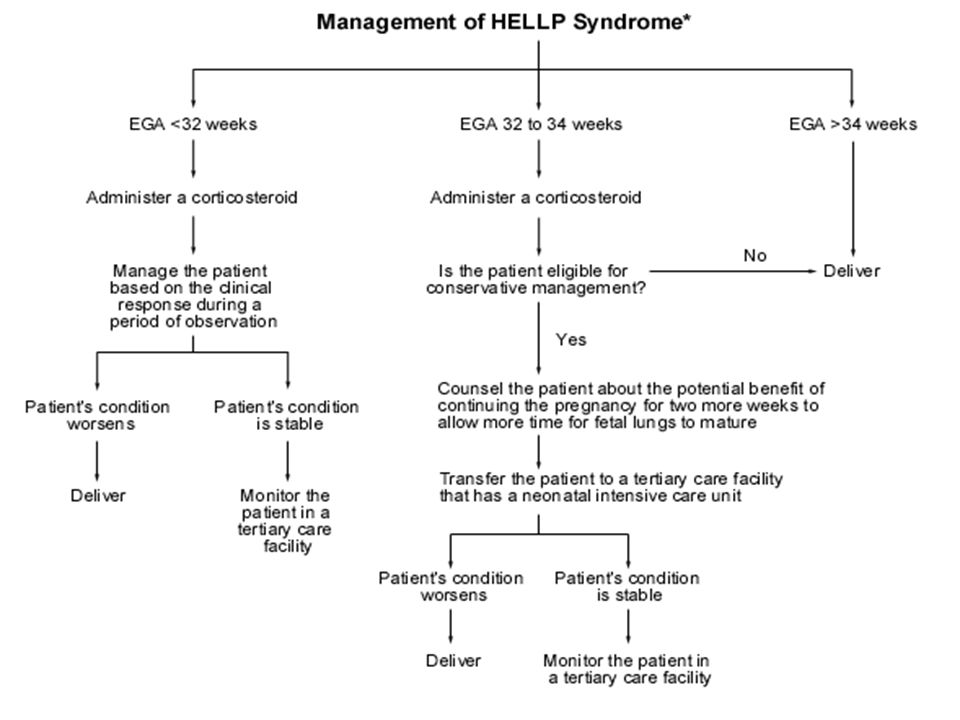
In general, there are three major options for the management of women with severe preeclampsia and HELLP syndrome These include: 1) Immediate delivery which is the primary choice at 34 weeks' gestation or later. 2) Delivery within 48 hours after evaluation, stabilization of the maternal clinical condition and Steroid treatment. At 27 to 34 weeks of gestation, this option appears appropriate and rational for the majority of cases. 3) Expectant (conservative) management for more than 48–72 hours may be considered in pregnant women before 27 weeks' gestation. In this situation, Steroid treatment is often used, but the regimens vary considerably.
 Delivery within 48 hours after evaluation, stabilization of the maternal clinical condition and Steroid treatment. At 27 to 34 weeks of gestation, this option appears appropriate and rational for the majority of cases. 3) Expectant (conservative) management for more than 48–72 hours may be considered in pregnant women before 27 weeks gestation. In this situation, Steroid treatment is often used, but the regimens vary considerably..")
37
34wks ↓ ↓ ↓ Admit & conservative Mx Steroids Deliver ↓ ↓ No Manage Pt based on Is pt eligible for conservative Mx ? Clinical response during ↓ Yes Period of observation Counsel pt abt benefit of continuing of pregnency for ≥2 wks for lung maturity ↓ Worsens Stable Transfer pt to tertiary care centre ↓ ↓ Deliver Monitor pt in tertiary care centre

39
Whereas delivery is the mainstay of treatment for the HELLP syndrome, Steroid treatment is a possible addendum. Present alternatives for Steroid treatment are: 1) Standard steroid treatment on maternal HELLP. 2) High-dose dexamethasone treatment of the mother. 3) Treatment with repeated doses to reduce maternal morbidity and hastening recovery.
 Standard steroid treatment on maternal HELLP. 2) High-dose dexamethasone treatment of the mother. 3) Treatment with repeated doses to reduce maternal morbidity and hastening recovery..")
40
Benefit of steroid treatment for the HELLP syndrome was first reported in 1984. Mech. Of Action- Unknown Proposed mech - diminish oedema, inhibit endothelial activation and reduce endothelial dysfunction ↓ Prevention of thrombotic microangiopathic anaemia, Inhibition of cytokine production ↓ induce anti-inflammatory effects in the HELLP syndrome

41
IV steroid- appear to have more rapid onset of action than IM better outcome in improving urine output & laboratory values. Dose –increases platelet count when given in high doses Duration –Duration of action of this medication is limited. Patient may experience a worsening of their laboratory studies 48-72 hrs after dosing with steroid.– REBOUND PHENOMENON

42
For most of patient with HELLP syndrome- 10mg IV dexamethasone every 12 hrs until delivery & then 10 mg IV dexamethasone every 12 hrs for additional 3 doses post partum. For selected high risk cases with profound thrombocytopenia with CNS dysfunction. 20mg IV dexamethasone every 6hrs up to 4 doses

43
In first largest randomized double blind, placebo controlled (dexamethasone versus placebo) study of 132 women by Fonseca et al. reported shorter mean hospitalization but no significant differences were found in recovery of platelet counts or liver enzymes. A Cochrane analysis from 2004 concluded that steroid treatment did not affect maternal mortality and outcomes such as placental abruption, pulmonary oedema and liver complications.

44
Steroid is not curative but may create a WINDOW OF OPPORTUNITY for intervention before maternal condition may again deteriorate.

45
Platelet transfusion – is required eithr before or after delivery, in presence of bleeding from puncture site, wound and intra peritoneal bleeding. If platelet count <40,000/µL, 6 – 10 U of platelet is required. PCV and FFP – required if coagulopathy is present.

46
Antithrombin III transfusion- correct hypercoagulability, stimulate prostacyclin production, regulate thrombin-induced vasoconstriction, improve foetal status. In contrast to the use of heparin, antithrombin has not been shown to increase the risk of bleeding. The potential benefit from antithrombin treatment of women with HELLP syndrome might be a reasonable objective to be tested in future well designed multicenter studies.

47
In most women with a HELLP syndrome, the maternal PLT counts continue to decrease immediately post- partum with an increasing trend on the third day. About 30% of the HELLP syndromes develop after birth. The time of onset ranged from few hrs to 7 days; the majority within the first 48 hoursafter delivery. In post-partum HELLP syndrome, risk of renal failure and pulmonary oedema is significantly increased.

48
Since early post-partum administration of high-dose CS might accelerate recovery, its routine administration is highly advocated (10 mg of dexamethasone every 12 hours) However, a randomized study showed that adjunctive use of intravenous dexamethasone for postpartum patients with severe preeclampsia did not reduce disease severity or duration. There was no difference in maternal morbidity, duration of hospital stay, need for rescue scheme or the use of blood products between the groups. These findings did not support the use of dexamethasone in the puerperium for recovery of women with HELLP.

49
Sibai has shown that oral contraceptives are safe in women with a prior HELLP syndrome. Women with a history of the HELLP syndrome carry an increased risk of at least 20% (range 5–52%) that some form of gestational hypertension will recur in a subsequent gestation
 that some form of gestational hypertension will recur in a subsequent gestation.")
50
Women with a history of HELLP syndrome at or before 28 weeks' gestation during the index pregnancy are at increased risk for several obstetric complications (preterm birth, pregnancy-induced hypertension and increased neonatal mortality) in a subsequent pregnancy.
 in a subsequent pregnancy.")
51
HELLP Syndrome and its management still poses a problem in modern obstetrics Precise diagnosis and early treatment with non-mineral corticosteroides such as Dexamethasone may help achieve favorable maternal and perinatal results.

52
THANK YOU

Similar presentations


>")

















