Download presentation
Presentation is loading. Please wait.

1
Dr Kirsten Windfuhr Senior Research Fellow & Senior Project Manager National Confidential Inquiry into Suicide and Homicide by People with Mental Illness (NCISH) Centre for Mental Health and Risk February 4 2015 Cheshire & Merseyside Suicide Reduction Summit Improving services, reducing suicide
 Centre for Mental Health and Risk February Cheshire & Merseyside Suicide Reduction Summit Improving services, reducing suicide")
2
Suicide prevention is an imperative

3
What are the causes of suicide? Suicidal Behaviour Biological factors Genes Neurodevelopment Clinical factors Mental illness Physical illness Previous suicidal behaviour Drugs and alcohol Treatment Psychological factors Problem solving Hopelessness Impulsivity Aggression Environmental factors Early life experience Life events Socio-economic conditions Societal attitudes Availability of methods (Adapted from Gunnell and Lewis 2005)
.")
4
UKEnglandWalesScotlandN. Ireland General population 100,32978,1705,47513,2353,449 NCISH In contact with MH services 26,216 (26%) 20,300 (26%) 1,260 (23%) 3,705 (28%) 951 (28%) Suicide in the UK; 1996/7-2012 UK_SUICIDE © National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved. Not to be reproduced in whole or part without the permission of the copyright holder.
 20,300 (26%) 1,260 (23%) 3,705 (28%) 951 (28%) Suicide in the UK; 1996/ UK_SUICIDE © National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved. Not to be reproduced in whole or part without the permission of the copyright holder..")
5
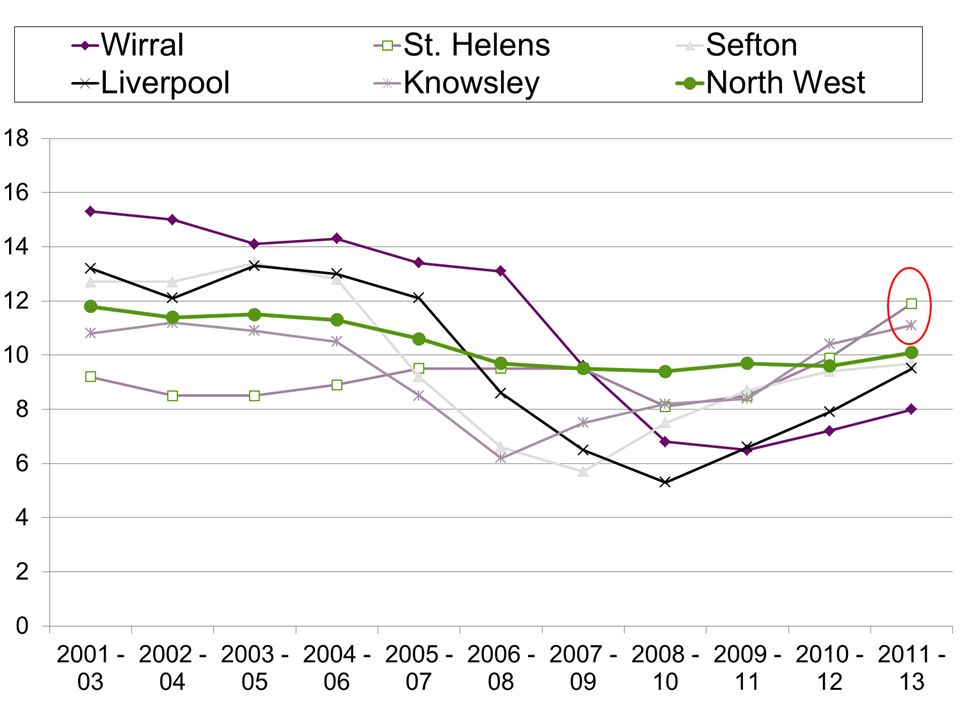
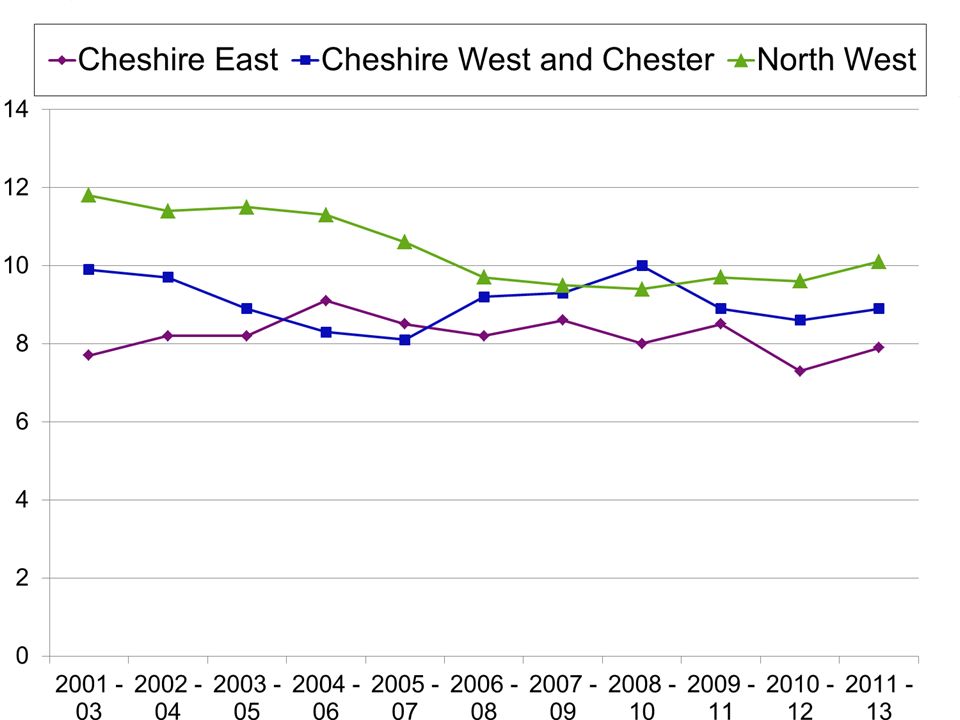
What are national and local trends?

6
Source: Public Health England; Health Profiles http://www.phoutcomes.info/profile/health-profiles/data#gid/1938132696/pat/6/ati/102/page/4/par/E12000002/are/E08000003

9
Suicide prevention and primary care

10
“GPs can make a big difference to overall suicide rates.” (DH, 2014) “Primary care services have a crucial role in addressing mental health problems and assessing suicide risk.” “The RCGP/RCPsych have issued a helpful factsheet on managing suicide risk in primary care.” “Research is essential to inform effective suicide prevention.”
 Primary care services have a crucial role in addressing mental health problems and assessing suicide risk. The RCGP/RCPsych have issued a helpful factsheet on managing suicide risk in primary care. Research is essential to inform effective suicide prevention.")
11
Why are GPs central to reducing suicide? 1.Majority of people present to their GP prior to losing their life to suicide

12
1: GP contact prior to suicide GP contact: month prior to suicide GP contact: year prior to suicide Luoma et al., 2002 Am J Psychiatry

13
Why are GPs central to reducing suicide? 1.Majority of people present to their GP prior to losing their life to suicide 2.A substantial proportion of people with mental illness are managed in primary care

14
Why are GPs central to reducing suicide? 1.Majority of people present to their GP prior to losing their life to suicide 2.A substantial proportion of people with mental illness are managed in primary care 3.Suicide risk is greater in the context of mental illness

15
3: Suicide risk and mental illness Year prior to suicide: mental health patient suicide deaths Pearson et al., 2009, BJGP Proportion of suicide deaths who had a mental illness prior to death Cavanagh et al., 2003, Psych Med

16
Study of attendance and clinical factors 10 years Case control study in primary care Clinical Practice Research Datalink (CPRD)
")
17
Attendance

18
Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide [number= 1,504 (63%)] Clinical time line 2,384 patients who died by suicide
![Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide [number= 1,504 (63%)] Clinical time line 2,384 patients who died by suicide](http://images.slideplayer.com/21/6252347/slides/slide_18.jpg "Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide [number= 1,504 (63%)] Clinical time line 2,384 patients who died by suicide")
19
Number of consultations in the 12 months prior to suicide 1,504

20
Risk and GP attendance frequency 12.3 7.8

21
Number of consultations in the time period prior to suicide

22
Risk and GP attendance frequency 12.3 7.8 1.67 Characteristics of non-attenders: male younger

23
Suicide risk in primary care Attendance –frequent attendance –increasing attendance –non-attendance

24
Diagnosis

25
Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide number= 1,504 (63%) Mental health diagnosis (any time) [number= 1,497 (63%)] Clinical time line 2,384 patients who died by suicide
![Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide number= 1,504 (63%) Mental health diagnosis (any time) [number= 1,497 (63%)] Clinical time line 2,384 patients who died by suicide](http://images.slideplayer.com/21/6252347/slides/slide_25.jpg "Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide number= 1,504 (63%) Mental health diagnosis (any time) [number= 1,497 (63%)] Clinical time line 2,384 patients who died by suicide")
26
Diagnosis Mental health diagnosis (at any time) –63% (v. 28% of living patients) –mainly depression Of patients with no diagnosis (37%) –male –35-44
 –mainly depression Of patients with no diagnosis (37%) –male –")
27
Suicide risk in primary care Attendance –frequent attendance –increasing attendance –non-attendance Diagnosis –under-recognition

28
Drug treatment

29
Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide number= 1,504 (63%) Mental health diagnosis (any time) number= 1,497 (63%) Psychotropic drug treatment within 12 months of suicide [number= 1,148 (48%)] Clinical time line 2,384 patients who died by suicide
![Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide number= 1,504 (63%) Mental health diagnosis (any time) number= 1,497 (63%) Psychotropic drug treatment within 12 months of suicide [number= 1,148 (48%)] Clinical time line 2,384 patients who died by suicide](http://images.slideplayer.com/21/6252347/slides/slide_29.jpg "Patients who died by suicide: consultation, diagnosis, treatment, and referral Face-to-face GP consultation within 12 months of suicide number= 1,504 (63%) Mental health diagnosis (any time) number= 1,497 (63%) Psychotropic drug treatment within 12 months of suicide [number= 1,148 (48%)] Clinical time line 2,384 patients who died by suicide")
30
Managing mental illness: suicide risk and multiple drug prescriptions 5x more likely to have psychotropic drugs prescribed 31% prescribed 2+ elevated risk with 4 or 5

31
Drug treatment Multiple drug types –Illness severity –Inherent risks with complex prescribing Risk

32
Suicide risk in primary care Attendance –frequent attendance –increasing attendance –non-attendance Diagnosis –under-recognition Drug prescriptions –multiple drug types

33
Key messages for services Markers of risk include –frequent attendance –increasing attendance –non-attendance –multiple drug prescriptions Markers could form basis of ‘flag’ alert in primary care records –further assessment, engagement Collaborative working with third sector, on-line support

34
National Confidential Inquiry into Suicide and Homicide by People with Mental Illness Website: http://www.manchester.ac.uk/nci Follow us on Twitter https://twitter.com/NCISH_UK Like us on Facebook https://www.facebook.com/pages/Centre-for-Mental-Health-and-Risk

Similar presentations
 © National Confidential Inquiry.>")











 © National Confidential Inquiry.>")
 WALES (2002-2012) © National Confidential.>")





