Download presentation
Presentation is loading. Please wait.

1
Cooperation – Who benefits the most?- Camilla Blomqvist PhD thesis in social work Qualitative and quantitative study Finished by 2009

2
Aim How co-operate child psychiatry, social services and school when all organizations are involved with the child? How does the process look like to be a co- operating case? Is the child perspective similar or different in the different organizations?

3
Method Observations in consultations Observations and interviews in cases Survey

5
Distribution of survey answers

6
Who answered the survey? 1 in 5 were men Most men were from School services and Child Psychiatry It was more common that women had worked at least 6 years than men (38% vs 25%). The average for job experience was a little more than 8 years. The majority of personnel with more than 15 years of experience worked in Child Psychiatry and at school.
. The average for job experience was a little more than 8 years. The majority of personnel with more than 15 years of experience worked in Child Psychiatry and at school..")
7
Who is cooperating? Joint cooperation: Child Psychiatry/School/Social services -41% participate 1-4 times/month (frequent cooperation), -40% less than once quarterly. -The remainder every other or every third month. Half of those who frequently cooperate have at least 10 cooperative cases per year. (many cases few meetings or few cases many meetings) Child Psychiatry cooperates more often than school and social services:
, -40% less than once quarterly. -The remainder every other or every third month. Half of those who frequently cooperate have at least 10 cooperative cases per year. (many cases few meetings or few cases many meetings) Child Psychiatry cooperates more often than school and social services:.")
8
Who cooperates? Frequent cooperation is most common among personnel with 6-15 years of job experience.

9
How does cooperation take place? Telephone and mail is more common than meetings. Meetings often include the parents. This is more common for Child Psychiatry. Meetings that include the parents and children are most common for Social services.

10
Thoughts on cooperation Every other person from Child Psychiatry/Social services feels that he/she has good or very good cooperation with school services. A little more than 1 in 3 from Child Psychiatry/School services feel that he/she has good or very good cooperation with social services. 1 in 4 from Social/School services feels that he/she has good or very good cooperation with Child Psychiatry services.

11
Differences in cooperation – all Perception/Experience of cooperation with Social services and Child Psychiatry changes positively once one has experience of it. The perception of cooperation with School services is not dependant upon experience. Differences are amplified: those who cooperate within School and Social services (70%) are more familiar with the UN’s Children’s rights than those within Child Psychiatry are (24%).
 are more familiar with the UN’s Children’s rights than those within Child Psychiatry are (24%)..")
12
What influences the development of cooperation between organizations

13
The best for the child All organizations are familiar with the UN’s Children’s rights act. Social and school services are more familiar than Child Psychiatry. Assessments regarding what is best for a child is done for each individual case – Social services more than the others Organizations reach consensus together regarding what is best for a child. Social services most often decides what is best for a child when their is disagreement. 1 in 6 do not discuss what is best for a child in their organizations. This is equally common in all organizations.

14
Consultations at Child Psychiatry Participated in 42 treatment/diagnosis consultations. Listened to 269 patient histories

15
Partial results from consultations The majority of cases were brought up by the parents. Cooperation was initiated by referral or invitation. In 4 of 10 cases cooperation was started. The idea with cooperation was benefits for Child Psychiatry or for Child Psychiatry and the family.

16
Focus shifts between children, parents, and which contributions Child Psychiatry can make. The case officer’s preconceptions characterize the child’s history and influences efforts. Ambiguous between assessment/treatment.

17
Eight cases From treatment consultation/treatment at Child Psychiatry All the children had problems in school as well as previous contact with Child Psychiatry and social services. 7 out of 8 children had had long-term contact. 7 out of 8 were boys. Children between 10 and 17 years old. 2 of the children lived with their original families. Many resources have been given to the families.

18
Partial results of cases Families were moved around between organizations Personnel change Ambiguity Little room for the child’s best Disagreement Exposure For both the family and personnel Time Long time to gather oneself

19
What was the final result of cooperation in the cases? Better cooperation between organizations Treatment process begins together Slow change – no change? Disagreement among organizations

20
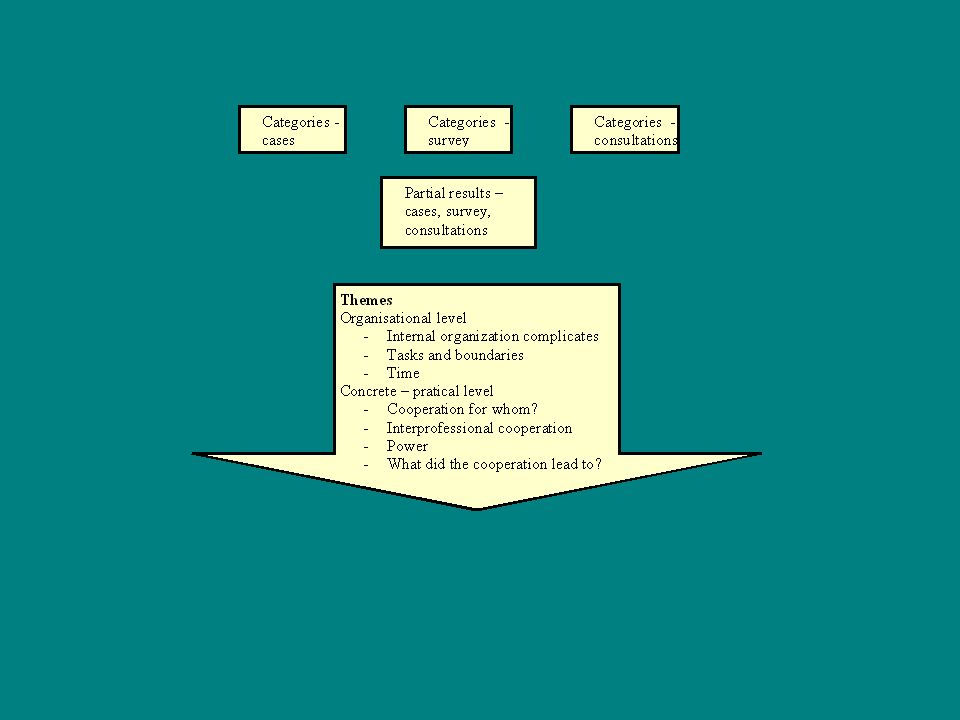
Conclusions – organizational level Internal organization complicates things Assignments and boundaries -Skepticism for the assessments of other organizations -Discussions about costs -Confidentiality -The efforts of the organizations and the children's needs Time -Problems in 1st grade are not solved in 9th grade -Seasonally controlled organization -Simultaneous work

21
Conclusions – concrete practical level For whom are we cooperating? -Personnel? -Child? -Parents? Inter-professional cooperation internally and externally -Different professions – different explanation theories? -Fun to work together. -Difficulties describing the causes of problems. -Teachers are important for children. -Lack of clarity in their work efforts. Power -Parents and children feel they are overrun -Personnel also feel they are overrun

22
The cooperation of organizations and the UN’s child rights act – how does it work? The child becomes an object. It takes time for the child’s story to be heard. The child’s exposure –In individual meetings –In the agreements of organizations –In difficulties obtaining help

23
Things to think about … … How would cooperation be affected with one authority instead of three? … How would the personnel’s efforts be affected if they talked with and not about the family? … Would there be a difference if the child’s story was heard earlier? … What would happen if cooperation started earlier? … Would it make a difference if the child’s needs controlled organizational efforts instead of the resources of the organization?

Similar presentations


. It was completed over a 5 week period in a.>")
 Proficient (2 points) Partially Proficient (1 point) Incomplete (0 points) POINTS Focus on the task and participation Consistently.>")



 rate yourself on your ability to complete all the assignments for class. Why? I rate my self a 5. I always get my.>")











