Download presentation
Presentation is loading. Please wait.

1
OCCUPATIONAL HEALTH UPDATE 2014: EXTENDED CARE FACILITIES, SPICE
David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics & Epidemiology Associate Chief Medical Officer Medical Director, Occupational Health & Hospital Epidemiology University of North Carolina at Chapel Hill

2
GOALS OF CURRENT LECTURE
Understand activities of an occupational health service (OHS) in a healthcare facility Be able to list vaccines recommended for healthcare personnel (HCP) Be able to list infectious diseases relevant to HCP for which post-exposure prophylaxis is available Be able to manage exposure to blood or a contaminated fluid
 in a healthcare facility. Be able to list vaccines recommended for healthcare personnel (HCP) Be able to list infectious diseases relevant to HCP for which post-exposure prophylaxis is available. Be able to manage exposure to blood or a contaminated fluid.")
3
PREVENTING HCP INFECTIONS & INJURIES
It is the responsibility of the facility, to the extent possible, to provide a safe working environment. This includes minimizing the risk of infectious disease exposures and injuries. An organized program should be in place to identify and evaluate both infectious disease exposures and injuries, and to provide care of the exposed or injured employee.

4
PREVENTING HCP INFECTIONS & INJURIES
A casual attitude towards employee health entails a high cost Increased patient morbidity Increased staff morbidity Significant financial cost and legal risk Prevention is superior to treatment The tools used to reduce the risk of acquiring infection can be used to reduce the risk of injuries

5
OSHA NIOSH CDC FDA Health Department External Stakeholders Occupational Health Service Internal Stakeholders Legal/Administration Safety Medical Staff Worker’s compensation Infection Control

6
OCCUPATIONAL HEALTH ACTIVITIES
Pre-employment screening Immunization review Employment physical (selected; DOT, FAA, police) Drugs/alcohol screening Latex allergy screen (history; if positive, blood test) Screen for active TB (symptoms; if positive CxR, sputums?) Screen for latent TB (TST or IFGR blood test) Fit test clearance (questionnaire, medical exam?); N95 fit testing Hearing evaluation/audiogram (if indicated by noise exposure) Counseling: pregnant women, immunocompromised
 Drugs/alcohol screening. Latex allergy screen (history; if positive, blood test) Screen for active TB (symptoms; if positive CxR, sputums ) Screen for latent TB (TST or IFGR blood test) Fit test clearance (questionnaire, medical exam ); N95 fit testing. Hearing evaluation/audiogram (if indicated by noise exposure) Counseling: pregnant women, immunocompromised.")
7
OCCUPATIONAL HEALTH ACTIVITIES
Annual screening Immunization review Screen for active TB (symptoms; if positive CxR, sputums?) Screen for latent TB (TST or IGRA blood test) Evaluation of injured employees First aid Long-term care Communication with Worker’s Compensation Return to work evaluation (non-occupational diseases and/or injuries)
 Screen for latent TB (TST or IGRA blood test) Evaluation of injured employees. First aid. Long-term care. Communication with Worker’s Compensation. Return to work evaluation (non-occupational diseases and/or injuries)")
8
OCCUPATIONAL HEALTH ACTIVITIES
Evaluation of employees with a potentially communicable disease Need for exposure evaluation Need for work restriction Therapy if indicated Infectious disease exposures Determination of exposure & risk of disease transmission Evaluate for post-exposure prophylaxis Consider need for work restrictions Communicate with infection control if patients exposed

9
OCCUPATIONAL HEALTH ACTIVITIES
Work site evaluation For cause drug/alcohol testing Education Fire, chemical, radiation safety Infection control (communicable diseases, TB, bloodborne pathogens) Ergonomics Smoking cessation
 Ergonomics. Smoking cessation.")
10
OSHA: BLOODBORNE PATHOGEN RULE
Employers must establish an Exposure Control Plan (reviewed yearly) Employers must utilize a hierarchy of methods to prevent exposure to blood or potentially contaminated body fluids Engineering controls (e.g., needleless devices) Work practice controls (e.g., single handed recapping) Mandates use of universal precautions (all body fluids assumed contaminated except sweat) Requires offering hepatitis B vaccine to persons with the potential for exposure Persons may refuse by signing a declination form PEP must be immediately available as per CDC guidelines Yearly training required Federal Register December 6, 1991;56:64003–64182
 Employers must utilize a hierarchy of methods to prevent exposure to blood or potentially contaminated body fluids. Engineering controls (e.g., needleless devices) Work practice controls (e.g., single handed recapping) Mandates use of universal precautions (all body fluids assumed contaminated except sweat) Requires offering hepatitis B vaccine to persons with the potential for exposure. Persons may refuse by signing a declination form. PEP must be immediately available as per CDC guidelines. Yearly training required. Federal Register December 6, 1991;56:64003–")
11
TUBERCULOUS: OSHA & CDC GUIDANCE
Rule proposed by OSHA 997; withdrawn 2003 [compliance required with 29 CFR – Respiratory Protection; 29 CFR – General Duty Clause Section 5(a)(1)] CDC recommendations Prompt detection of infectious patients Airborne precautions (private room, >12 air exchanges per hour, direct out exhausted air) Treatment of people with suspected or confirmed TB disease Hierarchy of control measures Administrative measures: TB risk assessment of the setting, TB control plan, timely lab testing, training and educating HCP, screen exposed HCP Environmental control: Airborne isolation, proper hoods in labs Use of respiratory protective equipment (per OSHA - N95 respirator, medical clearance, yearly fit testing) CDC: OHSA: OHSA: 11
(1)] CDC recommendations. Prompt detection of infectious patients. Airborne precautions (private room, >12 air exchanges per hour, direct out exhausted air) Treatment of people with suspected or confirmed TB disease. Hierarchy of control measures. Administrative measures: TB risk assessment of the setting, TB control plan, timely lab testing, training and educating HCP, screen exposed HCP. Environmental control: Airborne isolation, proper hoods in labs. Use of respiratory protective equipment (per OSHA - N95 respirator, medical clearance, yearly fit testing) CDC: OHSA: p_table=FEDERAL_REGISTER&p_id= OHSA:")
12
AMERICANS FOR DISABILITY ACT (ADA)
Outlaws discrimination based on a “disability” Allows employers to exclude persons who pose a “direct threat” Disability is defined as a physical or mental impairment that substantially limits one or more major life activities Does not apply to a transitory impairment (duration <6 months) Impairment can be episodic or in remission Employee must request an accommodation Excludes persons who are engaging in use of illegal drugs or alcohol (covers persons post drug rehabilitation) – permits use of drug testing Requires employers to make “reasonable accommodations” Defined by person’s private physician Accommodations should place undue hardship on employer Allows employer to require a medical exam after hiring a job applicant (but employer cannot require an exam before making a job offer)
 Impairment can be episodic or in remission. Employee must request an accommodation. Excludes persons who are engaging in use of illegal drugs or alcohol (covers persons post drug rehabilitation) – permits use of drug testing. Requires employers to make reasonable accommodations Defined by person’s private physician. Accommodations should place undue hardship on employer. Allows employer to require a medical exam after hiring a job applicant (but employer cannot require an exam before making a job offer)")
13
FAMILY MEDICAL LEAVE ACT (FMLA)
Requires employers to grant eligible employees up to a total of 12 weeks of unpaid leave during any 12-month period for one of the following Birth and care of a child, or adoption Care for an immediate family member (spouse, child, parent) with a serious health problem Medical leave when employee is unable to work because of serious health problem Family member on active duty with military with a serious injury or illness Employers may require employee to take an accrued paid vacation or medical leave concurrently with FMLA Employees responsibility to request FMLA Employee’s medical provider must provide a certification form
 with a serious health problem. Medical leave when employee is unable to work because of serious health problem. Family member on active duty with military with a serious injury or illness. Employers may require employee to take an accrued paid vacation or medical leave concurrently with FMLA. Employees responsibility to request FMLA. Employee’s medical provider must provide a certification form.")
14
COMMON OCCUPATIONAL HAZARDS
Infections Viral respiratory diseases Aerosol transmitted diseases: Tuberculosis, pertussis Bloodborne pathogens: Percutaneous, mucus membrane Contact transmitted diseases: Syphilis, MRSA Fecal oral: Norovirus, rotavirus

15
COMMON OCCUPATIONAL HAZARDS
Injuries Work-related (e.g., falls, strain, sprain) Ergonomic (e.g., strain, sprain, repetitive motion) Dermatitis (related to latex gloves, antiseptics) Hearing loss (noise related) Indoor air quality
 Ergonomic (e.g., strain, sprain, repetitive motion) Dermatitis (related to latex gloves, antiseptics) Hearing loss (noise related) Indoor air quality.")
16
OTHER OCCUPATIONAL HAZARDS
Chemicals: Anti-neoplastics, disinfectants & sterilants, anesthetic gases, organic solvents, mercury, asbestos Radiation: Ionizing radiation, radioisotopes Lasers Fire and electrical Violence Psychosocial stress Bioterrorist agents (microbial, chemical, nuclear)
")
19
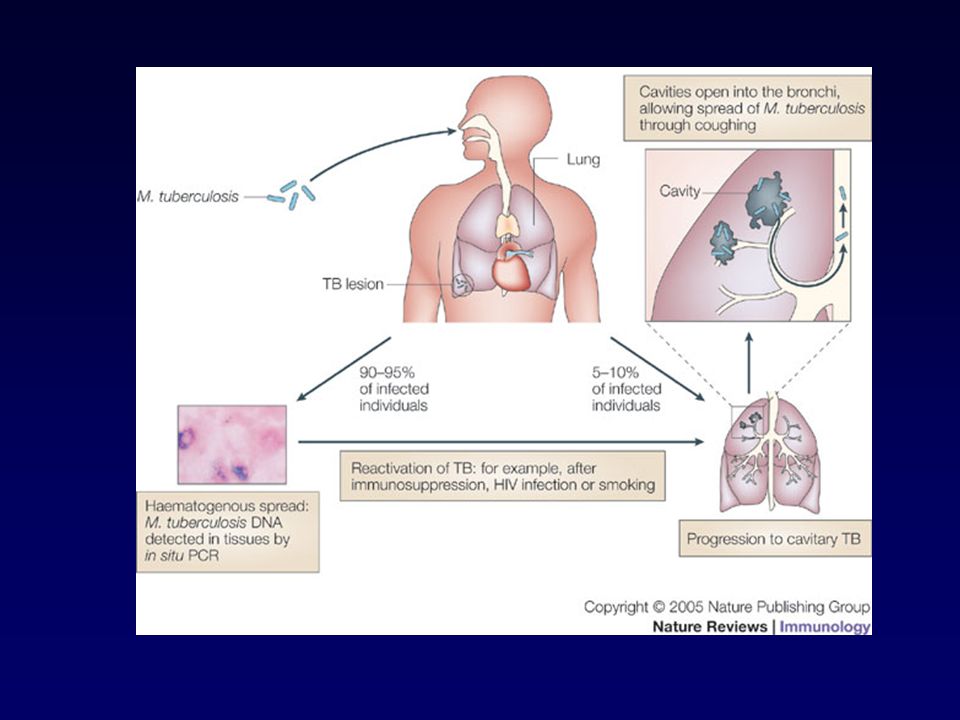
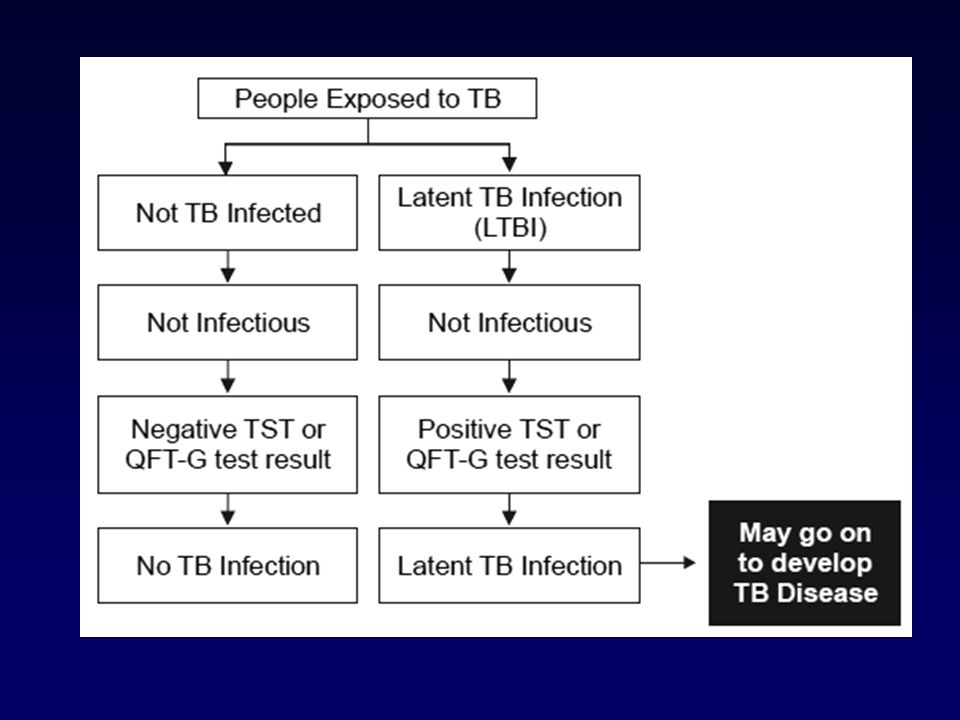
Person with LTBI (Infected) Person with TB Disease (Infectious)
LTBI vs. TB Disease Person with LTBI (Infected) Person with TB Disease (Infectious) Has a small amount of TB bacteria in his/her body that are alive, but inactive Has a large amount of active TB bacteria in his/her body Cannot spread TB bacteria to others May spread TB bacteria to others Does not feel sick, but may become sick if the bacteria become active in his/her body May feel sick and may have symptoms such as a cough, fever, and/or weight loss Usually has a TB skin test or TB blood test reaction indicating TB infection Radiograph is typically normal Radiograph may be abnormal Sputum smears and cultures are negative Sputum smears and cultures may be positive Should consider treatment for LTBI to prevent TB disease Needs treatment for TB disease Does not require respiratory isolation May require respiratory isolation Not a TB case A TB case
 Person with TB Disease (Infectious) Has a small amount of TB bacteria in his/her body that are alive, but inactive. Has a large amount of active TB bacteria in his/her body. Cannot spread TB bacteria to others. May spread TB bacteria to others. Does not feel sick, but may become sick if the bacteria become active in his/her body. May feel sick and may have symptoms such as a cough, fever, and/or weight loss. Usually has a TB skin test or TB blood test reaction indicating TB infection. Radiograph is typically normal. Radiograph may be abnormal. Sputum smears and cultures are negative. Sputum smears and cultures may be positive. Should consider treatment for LTBI to prevent TB disease. Needs treatment for TB disease. Does not require respiratory isolation. May require respiratory isolation. Not a TB case. A TB case.")
20
TESTING FOR LATENT TUBERCULOUS INFECTION
Test methods Mantoux tuberculin skin test (TST) IGRA IGRA can be used in place of TST These tests do NOT exclude LTBI or TB disease Decisions about medical management should include other data and not just rely on TST/IGRA results Cannot switch back and forth between TST and IGRA 2-Step testing: Recommended for person who have not had TST within previous 12 months (required for staff and patients of LTCF) NC TB manual =
 IGRA. IGRA can be used in place of TST. These tests do NOT exclude LTBI or TB disease. Decisions about medical management should include other data and not just rely on TST/IGRA results. Cannot switch back and forth between TST and IGRA. 2-Step testing: Recommended for person who have not had TST within previous 12 months (required for staff and patients of LTCF) NC TB manual =")
21
CANDIDATES FOR TST TST of individuals and groups should be undertaken only if the diagnostic evaluation and a course of preventive therapy can be completed Routine testing of low-risk individuals is NOT recommended The following adults are legally required to receive a TST: Patients and staff in long term care facilities upon admission and employment, using the 2-step skin test method Household and other close contacts of active cases of pulmonary and laryngeal TB Persons reasonably suspected of having TB disease Persons with HIV infection or AIDS NC TB Policy Manual, New Edition, 23 January 2012

22
TST VS IGRA TST advantages TST disadvantages IGRA advantages
Standard for years Inexpensive TST disadvantages Requires 2 (or 4 visits) Requires proper placement Requires reading May be positive due to prior BCG PPD in short supply IGRA advantages Not dependent on experienced users Single visit Not affected by prior BCG IGRA disadvantages Expensive Wobble
 Requires proper placement. Requires reading. May be positive due to prior BCG. PPD in short supply. IGRA advantages. Not dependent on experienced users. Single visit. Not affected by prior BCG. IGRA disadvantages. Expensive. Wobble.")
23
ADMINISTERING THE TST Inject 0.1 mL of PPD (5-TU) intradermally into forearm between skin layers Produce wheal (raise area) of 6-10 mm in diameter Requires 2-8 weeks after exposure to turn positive (CDC, wait 10 weeks) 2-step testing: Place and read PPD, and if negative repeat in 2-4 weeks to check for booster phenomenon Two-step method not needed if a person has ever had a tw-step skin test OR if the person has had a single skin test within the last 12 months (i.e., If PPD in past year that counts as first step in 2-step testing) Follow standard precautions for infection control
 2-step testing: Place and read PPD, and if negative repeat in 2-4 weeks to check for booster phenomenon. Two-step method not needed if a person has ever had a tw-step skin test OR if the person has had a single skin test within the last 12 months (i.e., If PPD in past year that counts as first step in 2-step testing) Follow standard precautions for infection control.")
24
READING THE PPD Read 48-72 hours after injection
Palpate (feel) injection site to find raised area Measure diameter of induration across forearm; only measure induration, not erythema Record size of induration in mm
 injection site to find raised area. Measure diameter of induration across forearm; only measure induration, not erythema. Record size of induration in mm.")
25
INTERPRETING THE TST REACTION
>5 mm is classified as positive: HIV-infected persons Recent contacts of infectious TB Persosn with fibrotic changes on CxR consistent with prior TB Patients with organ transplants and other immunocompromised persons >10 mm is classified as positive: Recent arrivals from high-prevalence countries (< 5-years) Inject drug users Residents and personnel (HCP) of high-risk congregate settings Persons with conditions that increase the risk for progression to active TB Children <4 years of age >15 mm is classified as positive: Persons with no known risk factors for TB
 Inject drug users. Residents and personnel (HCP) of high-risk congregate settings. Persons with conditions that increase the risk for progression to active TB. Children <4 years of age. >15 mm is classified as positive: Persons with no known risk factors for TB.")
26
PROBLEMS WITH TST False-Positive False-Negative NTM BCG vaccination
Problems with TST administration False-Negative Anergy Viral, bacterial, fungal infection Very youg; advanced age Live-virus vaccination Overwhelming TB Renal failure/disease Lymphoid disease Low protein states Immunosuppressive drugs Problems with TST administration

27
PRE-EXPOSURE PROPHYLAXIS

28
VACCINE PREVENTABLE DISEASES
Anthrax (PEP) Cervical, vulvar, vaginal cancer (HPV) Diphtheria (outbreak) Genital warts (HPV) Hepatitis A (PEP, outbreak) Hepatitis B (PEP) Hepatitis D H. influenza type b Human papillomavirus Influenza A and B Japanese encephalitis Liver cancer (hepatitis B) Lyme disease Measles (PEP, outbreak) Meningococcal (outbreak) Monkeypox Mumps (outbreak) Pertussis (outbreak) Pneumococcal disease Poliomyelitis (outbreak) Rabies (PEP) Rectal cancer (HPV) Rotavirus Rubella (outbreak) Smallpox (PEP, outbreak) Tetanus (PEP) Tuberculosis Typhoid fever Varicella (PEP) Yellow fever Zoster (Shingles) PEP = post-exposure prophylaxis
 Cervical, vulvar, vaginal cancer (HPV) Diphtheria (outbreak) Genital warts (HPV) Hepatitis A (PEP, outbreak) Hepatitis B (PEP) Hepatitis D. H. influenza type b. Human papillomavirus. Influenza A and B. Japanese encephalitis. Liver cancer (hepatitis B) Lyme disease. Measles (PEP, outbreak) Meningococcal (outbreak) Monkeypox. Mumps (outbreak) Pertussis (outbreak) Pneumococcal disease. Poliomyelitis (outbreak) Rabies (PEP) Rectal cancer (HPV) Rotavirus. Rubella (outbreak) Smallpox (PEP, outbreak) Tetanus (PEP) Tuberculosis. Typhoid fever. Varicella (PEP) Yellow fever. Zoster (Shingles) PEP = post-exposure prophylaxis.")
29
ADULT IMMUNIZATION SCHEDULE, US, 2014

30
ADULT IMMUNIZATION SCHEDULE, US, 2014

31
KEY REFERENCES

32
SUMMARY OF CURRENT FDA APPROVED INFLUENZA VACCINES
Older vaccines Standard IM inactivate influenza vaccine (TIV) {>6 mo} Inhaled live-attenuated influenza vaccine (LAIV) {2-49} Newer vaccines Licensure of high titer influenza vaccine for persons 65 years and older (improved immunogenicity and efficacy) {>65 years} Licensure of intradermal influenza vaccine {18-64 years} Licensure of cell culture-based influenza vaccine*^ {>18 years} Licensure of 2 quadrivalent influenza (2 A, 2 B strains) vaccines* {>3}+ Licensure of recombinant influenza (HA only) vaccine*^ {18-49} * No ACIP statement available, ^ not produced in eggs, +inactivated vaccine
 {>6 mo} Inhaled live-attenuated influenza vaccine (LAIV) {2-49} Newer vaccines. Licensure of high titer influenza vaccine for persons 65 years and older (improved immunogenicity and efficacy) {>65 years} Licensure of intradermal influenza vaccine {18-64 years} Licensure of cell culture-based influenza vaccine*^ {>18 years} Licensure of 2 quadrivalent influenza (2 A, 2 B strains) vaccines* {>3}+ Licensure of recombinant influenza (HA only) vaccine*^ {18-49} * No ACIP statement available, ^ not produced in eggs, +inactivated vaccine.")
33
SUMMARY OF CURRENT ACIP RECOMMENDATIONS
Influenza 1 annual dose for all persons >6 months of age Required to be offered to residents and HCP in ECFs in NC Immunize as soon as vaccine becomes available for the current season 33

34
SUMMARY OF CURRENT FDA APPROVED PNEUMOCOCCAL VACCINES
Polysaccharide vaccine (PPSV23) Contains 23 different pneumococcal strains FDA approved for all person >50 years of age FDA approved for high risk persons years of age Conjugate vaccine (PCV13) Contains 13 different pneumococcal strains Conjugation with diphtheria toxin may improve immunogenicity
 Contains 23 different pneumococcal strains. FDA approved for all person >50 years of age. FDA approved for high risk persons years of age. Conjugate vaccine (PCV13) Contains 13 different pneumococcal strains. Conjugation with diphtheria toxin may improve immunogenicity.")
35
SUMMARY OF CURRENT ACIP RECOMMENDATIONS
Pneumococcal (polysaccharide, PPSV23) Age >65: All persons Age >19: Medical or other risk indications Required to be offered to residents in ECFs in NC Revaccination may be recommended (first dose <65 years AND now >65 years AND >5 years have passed) Pneumococcal (conjugate, PCV13) No recommendation for revaccination Immunocompromised persons (see chart, next slide) Vaccine naïve: PCV13 following at least 8 weeks later by PPSV23 Previous receipt of PPSV23: PCV13 >1year after last PPSV23 35
 Age >65: All persons. Age >19: Medical or other risk indications. Required to be offered to residents in ECFs in NC. Revaccination may be recommended (first dose <65 years AND now >65 years AND >5 years have passed) Pneumococcal (conjugate, PCV13) No recommendation for revaccination. Immunocompromised persons (see chart, next slide) Vaccine naïve: PCV13 following at least 8 weeks later by PPSV23. Previous receipt of PPSV23: PCV13 >1year after last PPSV")
36
CDC. MMWR 2012;61:816

37
SUMMARY OF CURRENT ACIP RECOMMENDATIONS
Zoster One dose for persons >60 years of age regardless of whether they had a prior episode of zoster FDA approved for persons >50 years of age - ACIP statement to be delayed (pending resolution of vaccine shortage) Live attenuated vaccine; avoid in immunocompromised persons Meningococcal Recommended for adults had high risk of disease 2-dose primary series administered 2-months apart for persons 2-54 with persistent complement deficiency, functional or anatomic asplenia, or HIV infection (adolescents) MCV4, persons <55 years; MPSV4 persons >56 years
 Live attenuated vaccine; avoid in immunocompromised persons. Meningococcal. Recommended for adults had high risk of disease. 2-dose primary series administered 2-months apart for persons 2-54 with persistent complement deficiency, functional or anatomic asplenia, or HIV infection (adolescents) MCV4, persons <55 years; MPSV4 persons >56 years.")
38
SUMMARY OF CURRENT ACIP RECOMMENDATIONS
Tetanus-diphtheria-acellular pertussis (/Tdap) Substitute 1 dose Tdap for all adults when Td booster due May be use to provide tetanus PEP Provide to all adults with exposure to young children (no delay after Td) Recommended for pregnant women (preferably 2nd or 3rd trimester)
 Substitute 1 dose Tdap for all adults when Td booster due. May be use to provide tetanus PEP. Provide to all adults with exposure to young children (no delay after Td) Recommended for pregnant women (preferably 2nd or 3rd trimester)")
39
SUMMARY OF CURRENT ACIP RECOMMENDATIONS
Hepatitis B Occupation: HCP Medical: clotting disorder, hemodialysis, ESRD Behavioral: Multiple sexual partners, injecting drug users, hx STD Other: Household/sexual contact with chronic HBV, travel, inmate >6 mo, clients/staff of institution for developmentally disable Diabetes (new) Hepatitis B vaccination should be administered to unvaccinated adults with diabetes who are aged 19 through 59 years (A, 2) Hepatitis B vaccination may be administered at the discretion of the treating clinician to unvaccinated adults with diabetes who age aged >60 years (B, 2)
 Hepatitis B vaccination should be administered to unvaccinated adults with diabetes who are aged 19 through 59 years (A, 2) Hepatitis B vaccination may be administered at the discretion of the treating clinician to unvaccinated adults with diabetes who age aged >60 years (B, 2)")
40
SUMMARY OF CURRENT ACIP RECOMMENDATIONS
Mumps, measles, rubella (MMR) Mumps Born before 1957: Considered immune (except during outbreak) Born during or after 1957: 1 or more doses Immunity = Appropriate immunizations or positive serology Measles Born before 1957: Consider immune (except during outbreak) Born after 1957: 1 or more doses Rubella 1 dose of MMR to susceptible women of childbearing potential Immunity: Positive serology or documented vaccine 40
 Mumps. Born before 1957: Considered immune (except during outbreak) Born during or after 1957: 1 or more doses. Immunity = Appropriate immunizations or positive serology. Measles. Born before 1957: Consider immune (except during outbreak) Born after 1957: 1 or more doses. Rubella. 1 dose of MMR to susceptible women of childbearing potential. Immunity: Positive serology or documented vaccine. 40.")
41
SUMMARY OF CURRENT ACIP RECOMMENDATIONS
Varicella: 2 doses Special consideration should be given to those who have close contact with persons at high risk for severe disease (e.g., immunocompromised persons), are at high risk for exposure or transmission (e.g., teachers of young children, college students, military recruits, international travelers) Immunity: Birth before 1980 (not HCP or pregnant women), history of varicella or zoster by a HCP, positive serology, or laboratory evidence of infection HPV: 3 doses (0, 2, 6) All women and men <26 years of age (only quadrivalent vaccine from Merck approved for men) 41
, are at high risk for exposure or transmission (e.g., teachers of young children, college students, military recruits, international travelers) Immunity: Birth before 1980 (not HCP or pregnant women), history of varicella or zoster by a HCP, positive serology, or laboratory evidence of infection. HPV: 3 doses (0, 2, 6) All women and men <26 years of age (only quadrivalent vaccine from Merck approved for men) 41.")
42
RECOMMENDED VACCINES FOR HCP: CDC, ACIP, HICPAC
Hepatitis B (OHSA required) Influenza* Measles (MMR preferred)* Mumps (MMR preferred)* Rubella (MMR preferred)* Varicella (V)* Tetanus (Tdap)* Diphtheria (Tdap)* Pertussis (Tdap)* * Required at UNC 42
 Influenza* Measles (MMR preferred)* Mumps (MMR preferred)* Rubella (MMR preferred)* Varicella (V)* Tetanus (Tdap)* Diphtheria (Tdap)* Pertussis (Tdap)* * Required at UNC. 42.")
43
IMMUNIZATION OF HCP WITH CERTAIN CONDITIONS, ACIP, 2011

44
SPECIAL USE VACCINES IN HCP
Anthrax: Post-exposure BCG: Pre-exposure (high risk) Hepatitis A: Post-exposure, outbreak, research, travel Japanese encephalitis: Research, travel Meningococcal: Outbreak, laboratory (spinning CSF), travel Polio: Research, travel Rabies: Post-exposure, research, travel Typhoid: Research, travel Vaccinia: Pre-exposure?, post-exposure, research Yellow fever: Research, travel 44
 Hepatitis A: Post-exposure, outbreak, research, travel. Japanese encephalitis: Research, travel. Meningococcal: Outbreak, laboratory (spinning CSF), travel. Polio: Research, travel. Rabies: Post-exposure, research, travel. Typhoid: Research, travel. Vaccinia: Pre-exposure , post-exposure, research. Yellow fever: Research, travel. 44.")
45
HEPATITIS B VACCINE Indications Administration
Universal; HCP with potential blood exposure (OSHA required OR signed refusal) Administration IM dose into deltoid; 1-1.5” needle, gauge Schedule: 0, 1, 6 mo (May interchange current vaccines) Prior to administration do not routinely perform serologic screening for HB unless cost effective After 3rd dose, test for immunity (>10 mIU/mL){OSHA required}; if inadequate provide 3 more doses and test again for immunity; if inadequate test consider as “nonresponder” If non-immune after 6 (or 3) doses, test for HBsAg
 Administration. IM dose into deltoid; needle, gauge. Schedule: 0, 1, 6 mo (May interchange current vaccines) Prior to administration do not routinely perform serologic screening for HB unless cost effective. After 3rd dose, test for immunity (>10 mIU/mL){OSHA required}; if inadequate provide 3 more doses and test again for immunity; if inadequate test consider as nonresponder If non-immune after 6 (or 3) doses, test for HBsAg.")
46
Estimated Incidence of HBV infections among HCP and General Population, United States, 1985-1999
Healthcare Personnel General U.S. Population This graph shows a 90% decline in the incidence of HBV infections in healthcare personnel from the year 1985 to In the early to mid 1980’s, the incidence of HBV infection in healthcare personnel was much higher than in the general population. However, following the 1987 publication of universal precaution guidelines and the 1991 Occupational Safety and Health Administration requirement that employers provide HBV vaccination to healthcare personnel, the incidence in healthcare personnel has dropped below that in the general population.

47
HBV AMONG GENERAL PUBLIC AND HCP
1970s: HCP had a prevalence of HBV infection ~10x greater than that of general population 1983: ~17,000 HBV infections among HCP Currently: ~263 acute HBV infections Due to HBV vaccine and Improvements in infection control practices

48
CDC MMWR 2013;62 (RR-10)
")
49
ASSURING HCP COVERAGE Healthcare facility employees - requirement for employment Medical staff - include in credentialing process Students - require for attending class Volunteers - require Contract workers - require in contract Emergency responders

50
PROOF OF IMMUNITY FOR HCP
Vaccine Birth before 1957 MD Dx + Serology Self Report Documented Vaccination Mumps 1 Yes3 No Measles 1 Rubella 1,2 Varicella Yes 4 Hepatitis B >10 MIU/mL4 Pertussis Influenza 1Consider immunization of HCP born before 1957, recommend during an outbreak; 2All HCP of childbearing potential should be immunized; 3requires lab confirmation; 4Obtain 1-6 months post last vaccine dose Weber DJ, Schaffner W. ICHE 2011;32:912-4 50

51
PROVIDING VACCINES Patient name and identification number Vaccine
Dose, Site, Route of Administration Date given Manufacturer Lot number Name, title & address of person providing vaccine Date next dose due Informed consent

52
PROVIDING VACCINES: SEROLOGIC TESTING
Pre-immunization testing for immunity Do not obtain serological screening for immunity unless cost-effective, desired by employee (may require employee to bear cost), or vaccine contraindicated (e.g., MMRV, hepatitis B) Post-immunization testing for immunity Indicated for hepatitis B, rabies (high risk exposure) Consider persons with an with an “indeterminate” antibody level susceptible
, or vaccine contraindicated (e.g., MMRV, hepatitis B) Post-immunization testing for immunity. Indicated for hepatitis B, rabies (high risk exposure) Consider persons with an with an indeterminate antibody level susceptible.")
53
DATA RECORDED ON EXPOSURES
Employee Data Name, unit number, job description Date, incident form completed Employer, supervisor Source Data Name, unit number, location, infection(s) Exposure Data Location, date, type & circumstances of exposure
 Exposure Data. Location, date, type & circumstances of exposure.")
54
EXPOSURE EVALUATION Determine if source case has infection and is infectious Determine transmission possible (i.e., appropriate exposure without protection) Determine if employee is susceptible (may require labs) Determine if prophylaxis available & indicated Consider alternative prophylaxis (if available) if employee has contraindications to prophylaxis of first choice Arrange follow-up
 Determine if employee is susceptible (may require labs) Determine if prophylaxis available & indicated. Consider alternative prophylaxis (if available) if employee has contraindications to prophylaxis of first choice. Arrange follow-up.")
55
EMPLOYEE COUNSELING Information to be provided to HCP who are exposed to an infectious agent Recommended follow-up Risk (if known) of transmitting the infection to patients, other personnel, or other contacts Methods of preventing the transmission of infection to other persons
 of transmitting the infection to patients, other personnel, or other contacts. Methods of preventing the transmission of infection to other persons.")
56
EMPLOYEE COUNSELING Information to be provided to HCP who are offered prophylaxis Alternative means of prophylaxis Risk (if known) of infection if treatment not accepted Degree of protection provided by therapy Potential side effects of therapy
 of infection if treatment not accepted. Degree of protection provided by therapy. Potential side effects of therapy.")
57
INCIDENCE OF BLOODBORNE EXPOSURES, 1997-2011

58
POST-EXPOSURE PROPHYLAXIS
Anthrax Avian influenza (H5N1) Diphtheria Hepatitis A Hepatitis B HIV Human bite wound Influenza A Influenza B Measles Meningococcal infection Monkey bite Monkeypox Pertussis (whooping cough) Rabies Smallpox Syphilis Tuberculosis (TB) Varicella (chickenpox) Zoster (shingles)
 Diphtheria. Hepatitis A. Hepatitis B. HIV. Human bite wound. Influenza A. Influenza B. Measles. Meningococcal infection. Monkey bite. Monkeypox. Pertussis (whooping cough) Rabies. Smallpox. Syphilis. Tuberculosis (TB) Varicella (chickenpox) Zoster (shingles)")
59
NO POST-EXPOSURE PROPHYLAXIS
Hepatitis C Mumps Parvovirus B19 Rubella Severe acute respiratory distress syndrome (SARS)
")
60
Risk of Bloodborne Virus Transmission after Occupational Percutaneous Exposure
Source HBV HBeAg + HBeAg - HCV HIV Risk % % 1.8% 0.3% The risk of HBV transmission after a percutaneous exposure to HBV-infected blood, without postexposure treatment, varies, depending on the e-antigen status of the source. If the source is e-antigen positive, the risk of transmission will be up to 30%, whereas if the source is e-antigen negative, the risk is from 1-6%. The average risk of HCV transmission after a percutaneous exposure to HCV-infected blood is 1.8%, with a range of 0-7%. The average risk of HIV infection after a percutaneous exposure to HIV-infected blood is 0.3%, or 1 in 300 exposures (with a 95% confidence interval of 0.2%-0.5%). The average risk is based on aggregate data, and may not apply to specific exposure events.
. The average risk is based on aggregate data, and may not apply to specific exposure events.")
61
DEFINITION OF EXPOSURE
Percutaneous exposure to contaminated body fluid Mucous membrane exposure to contaminated body fluid Non-intact skin expose to contaminated body fluid Contaminated fluids: blood, CSF, vaginal secretions, semen, synovial, pleural, peritoneal, pericardial, amniotic

62
NEEDLESTICK INJURIES: MANAGEMENT
Test source for hepatitis B (HBsAg), hepatitis C, HIV (consider rapid test) Provide hepatitis B prophylaxis, if indicated Provide follow-up for hepatitis C, if indicated If source HIV+ or at “high risk” for HIV, exposure confirmed, offer employee HIV prophylaxis per CDC protocol Maintain confidentiality: Separate records, labs & pharmacy requisitions sent with code number
, hepatitis C, HIV (consider rapid test) Provide hepatitis B prophylaxis, if indicated. Provide follow-up for hepatitis C, if indicated. If source HIV+ or at high risk for HIV, exposure confirmed, offer employee HIV prophylaxis per CDC protocol. Maintain confidentiality: Separate records, labs & pharmacy requisitions sent with code number.")
63
NEEDLESTICK INJURIES: MANAGEMENT
OSHA requirements Employer shall make immediately available a confidential medical evaluation and follow-up Identification and documentation of source case; test source case for HBV, HCV and HIV after consent (if required) Offer to test employee for HBV and HIV (if employee refuses HIV testing hold blood for 90 days) Offer post-exposure prophylaxis, as medically indicated, per CDC recommendations; offer counseling Provide employee with results of evaluation with 15 days
 Offer to test employee for HBV and HIV (if employee refuses HIV testing hold blood for 90 days) Offer post-exposure prophylaxis, as medically indicated, per CDC recommendations; offer counseling. Provide employee with results of evaluation with 15 days.")
64
NEEDLESTICK INJURIES: MANAGEMENT
State regulations When the source case is known, the attending physician or occupational health provider responsible for the exposed person shall notify the healthcare provider of the source case that an exposure has occurred. This healthcare provider shall arrange HIV testing of the source person (unless known to be HIV+) and notify the OHS provider of the test results. In the event consent is refused the local health director may order testing
 and notify the OHS provider of the test results. In the event consent is refused the local health director may order testing.")
65
PEP FOR HBV EXPOSURES

66
The upper curve on the line graph represents the estimated number of stage 3 (AIDS) classifications among adults and adolescents diagnosed with HIV infection in the United States and dependent areas, by year of diagnosis from 1985 through 2010; the lower curve represents the estimated number of deaths of adults and adolescents with HIV infection ever classified with stage 3 (AIDS), by year of death from 1985 through The peak in stage 3 (AIDS) in 1993 can be associated with the expansion of the HIV surveillance case definition implemented in January The overall declines in stage 3 (AIDS) and deaths of persons with stage 3 (AIDS) are due in part to the success of highly active antiretroviral therapies, introduced in 1996. In recent years, stage 3 (AIDS) classifications and deaths of persons with stage 3 (AIDS) have remained stable. All displayed data are estimates. Estimated numbers resulted from statistical adjustment that accounted for reporting delays, but not for incomplete reporting. Deaths of persons with stage 3 (AIDS) may be due to any cause (may not be HIV-related). Deaths of persons with stage 3 (AIDS) are classified as adult or adolescent based on age at death. 66
 classifications and deaths of persons with stage 3 (AIDS) have remained stable. All displayed data are estimates. Estimated numbers resulted from statistical adjustment that accounted for reporting delays, but not for incomplete reporting. Deaths of persons with stage 3 (AIDS) may be due to any cause (may not be HIV-related). Deaths of persons with stage 3 (AIDS) are classified as adult or adolescent based on age at death. 66.")
67
In the United States and dependent areas, the estimated rate of adults and adolescents living with diagnosed HIV infection ever classified as stage 3 (AIDS) was per 100,000 population at the end of The rate for adults and adolescents living with stage 3 (AIDS) ranged from an estimated 2.4 per 100,000 population in American Samoa to an estimated 1,685.2 per 100,000 in the District of Columbia. The District of Columbia (i.e., Washington, DC) is a city; please use caution when comparing the rate of persons living with stage 3 (AIDS) in DC with the rates in states. All displayed data are estimates. Estimated numbers resulted from statistical adjustment that accounted for reporting delays, but not for incomplete reporting. Persons living with stage 3 (AIDS) are classified as adult or adolescent based on age at end of 2010.
 are classified as adult or adolescent based on age at end of")
68
HIV INFECTION AS A RESULT OF OCCUPATIONAL EXPOSURE IN HCP
HIV infections in HCP as a result of exposures (12/2001) Documented conversions = 57 26 have developed AIDS Types of exposures Percutaneous exposure 48, mucocutaneous 5, both 2, unknown route of exposure 2 Source of exposure HIV-infected blood 49, concentrated virus in lab 3, visibly bloody fluid 1, unspecified fluid 4
 Documented conversions = have developed AIDS. Types of exposures. Percutaneous exposure 48, mucocutaneous 5, both 2, unknown route of exposure 2. Source of exposure. HIV-infected blood 49, concentrated virus in lab 3, visibly bloody fluid 1, unspecified fluid 4.")
69
US PHS HIV POSTEXPOSURE GUIDELINES: NEW RECOMMENDATIONS
PEP is recommended when occupational exposures to HIV occur HIV status of exposure source patient should be determined, if possible, to guide need for HIV PEP PEP medication regimens should be started as soon as possible after exposure to HIV, and should be continued for a 4-week duration New recommendation: PEP medication regimen should contain 3 (or more) antiretroviral drugs for all occupational exposures to HIV Close follow-up for exposed person should be provided; follow-up should begin within 72 ours of an HIV exposure Expert consultation recommended for any occupational exposure to HIV New recommendation – if newer 4th generation combination HIV p24 Ag HIV test is used for follow-up of exposed HCP, HIV testing may be concluded 4 months after exposure; in a newer test is not available, follow for 6 months Kuhnar DT, et al. ICHE 2013;34:
 antiretroviral drugs for all occupational exposures to HIV. Close follow-up for exposed person should be provided; follow-up should begin within 72 ours of an HIV exposure. Expert consultation recommended for any occupational exposure to HIV. New recommendation – if newer 4th generation combination HIV p24 Ag HIV test is used for follow-up of exposed HCP, HIV testing may be concluded 4 months after exposure; in a newer test is not available, follow for 6 months. Kuhnar DT, et al. ICHE 2013;34:")
70
US PHS HIV POSTEXPOSURE GUIDELINES: GUIDELINE EMPHASIS
Primary prevention of occupational exposures Prompt management of occupational exposures Selection of PEP regimens that have the fewest side-effects and are best tolerated by prophylaxis recipients Anticipating and preemptively treating side effects commonly associated with taking anti-retroviral drugs Attention to potential interactions involving both drugs that could be included in HIV PEP regimens, as well as other medications that PEP recipients could be taking Consultation with experts on PEP management strategies HIV testing of source patients (without delay in PEP initiation) using methods that product rapid results Counseling and follow-up of exposed HCP
 using methods that product rapid results. Counseling and follow-up of exposed HCP.")
71
US PHS HIV POSTEXPOSURE GUIDELINES: DEFINITIONS
HCP = all paid and unpaid persons working in healthcare settings who have the potential for exposure to infectious materials, contaminated medical supplies and equipment, or contaminated environmental surfaces (e.g., ED, dental, lab, autopsy personal; MDs, RNs, technicians, pharmacists, students, trainees, etc.) Exposure that place HCP at risk = Percutaneous injury, contact of mucous membranes or nonintact skin with blood, tissue, or other potentially infected material (OPIM) Potentially infectious material = blood, visibly bloody body fluids, semen, vaginal secretions. Also CSF, synovial fluid, pleural fluid, peritoneal fluid, amniotic fluid, pericardial fluid. No known risk (unless visibly bloody) = feces, nasal secretions, saliva, sputum, sweat, tears, urine, and vomitus Human bites result in 2-way exposure
 Exposure that place HCP at risk = Percutaneous injury, contact of mucous membranes or nonintact skin with blood, tissue, or other potentially infected material (OPIM) Potentially infectious material = blood, visibly bloody body fluids, semen, vaginal secretions. Also CSF, synovial fluid, pleural fluid, peritoneal fluid, amniotic fluid, pericardial fluid. No known risk (unless visibly bloody) = feces, nasal secretions, saliva, sputum, sweat, tears, urine, and vomitus. Human bites result in 2-way exposure.")
72
US PHS HIV POSTEXPOSURE GUIDELINES: RISK OF HIV
Type of exposure Percutaneous ~0.3% Mucous membrane = ~0.09% For percutanous exposure, factors increasing risk of HIV acquisition A device visibly contaminated with patient’s blood A procedure that involved a need being placed directly in a vein or artery Deep injury Blood from a person with late stage disease Hollow bore (as opposed to solid bore) needle Despite lower risk, PEP should still be offered even if the source patient has an undetectable viral load
 needle. Despite lower risk, PEP should still be offered even if the source patient has an undetectable viral load.")
73
US PHS HIV POSTEXPOSURE GUIDELINES: PEP I
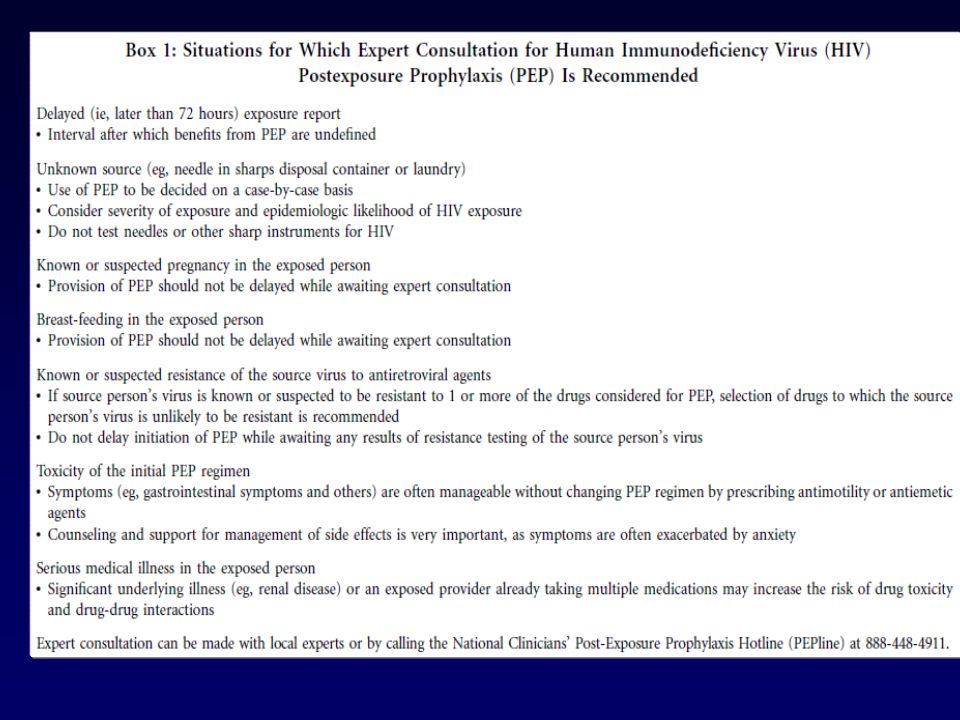
Obtain expert consultation if source patient is known to harbor drug-resistant HIV (but do NOT delay initial therapy to obtain consultation) If exposed person is pregnant, obtain expert consultation (but in general safe anti-retroviral therapy is available) Breast feeding is NOT a contra-indication to PEP but lactating HCP should be counseled regarding the high risk of HIV transmission through breast milk (stopping breast feeding is the best method to completely protect the fetus) Each healthcare facility should develop a plan to assess exposures and provide timely PEP
 If exposed person is pregnant, obtain expert consultation (but in general safe anti-retroviral therapy is available) Breast feeding is NOT a contra-indication to PEP but lactating HCP should be counseled regarding the high risk of HIV transmission through breast milk (stopping breast feeding is the best method to completely protect the fetus) Each healthcare facility should develop a plan to assess exposures and provide timely PEP.")
74
US PHS HIV POSTEXPOSURE GUIDELINES: PEP II
PEP is NOT recommended if source if HIV negative Re-evaluate exposed HCP within 72 hours post-exposure Ideally use a rapid (results in ~ 30 minutes) to test source patient Ideally use a 4th generation HIV test (combined antibody/antigen test) Use of a 4th generation tests allows identification of most infections during the “window period” Do not be concerned about the “window period” (i.e., source antibody negative but virus positive) If source patient not immediately available for testing, begin PEP (discontinue if source patient is HIV negative)
 to test source patient. Ideally use a 4th generation HIV test (combined antibody/antigen test) Use of a 4th generation tests allows identification of most infections during the window period Do not be concerned about the window period (i.e., source antibody negative but virus positive) If source patient not immediately available for testing, begin PEP (discontinue if source patient is HIV negative)")
75
US PHS HIV POSTEXPOSURE GUIDELINES: PEP III
Initial PEP within hours of exposure PEP is likely to be less effective when started more than 72 hours post-exposure (but the interval after which no benefit is gained from PEP in humans is unknown) Provide PEP for 4 weeks Provide 3-drug HIV PEP regimen 3 drugs superior in reducing viral burden in HIV infected persons Decreases concerns about possible drug resistance in source patient New regimens have improved safety and tolerability New regimens have fewer side effects (likely therefore improved adherence)
 Provide PEP for 4 weeks. Provide 3-drug HIV PEP regimen. 3 drugs superior in reducing viral burden in HIV infected persons. Decreases concerns about possible drug resistance in source patient. New regimens have improved safety and tolerability. New regimens have fewer side effects (likely therefore improved adherence)")
77
US PHS HIV POSTEXPOSURE GUIDELINES: PEP IV
Preferred PEP Embricitabine (FTC) plus tenofovir (TDF) – dispensed as Truvada PLUS Raltegravir (RAL) Regimen is tolerable, potent, conveniently administered, minimal drug interactions Likely safe in pregnancy (limited data)
 plus tenofovir (TDF) – dispensed as Truvada PLUS. Raltegravir (RAL) Regimen is tolerable, potent, conveniently administered, minimal drug interactions. Likely safe in pregnancy (limited data)")
81
US PHS HIV POSTEXPOSURE GUIDELINES: PEP V
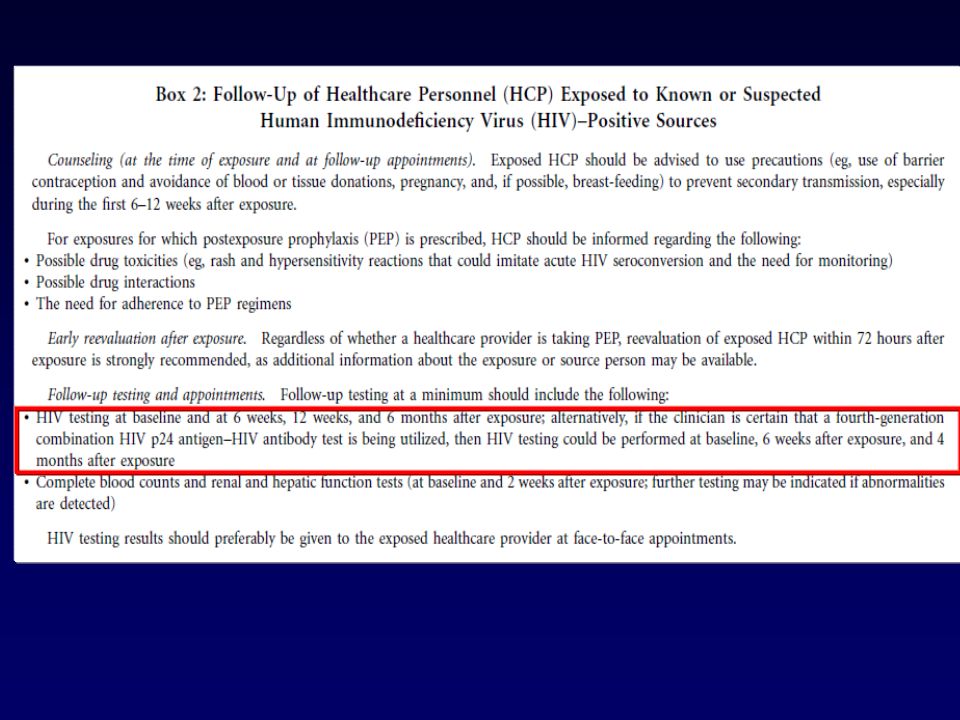
Toxicity monitoring Symptoms, focused physical exam CBC with differential, ALT, AST, Amylase, BUN, Creat, glucose (if on PI) Monitor at baseline and 2 weeks (and if any acute symptoms develop) Follow-up HIV testing At 6 weeks and 4 months (if using 4th generation HIV test) At 6 weeks, 12 weeks, 6 months (if using 3rd generation HIV test) If HCP exposed to source with HIV and HCV, follow for 1 year
 Monitor at baseline and 2 weeks (and if any acute symptoms develop) Follow-up HIV testing. At 6 weeks and 4 months (if using 4th generation HIV test) At 6 weeks, 12 weeks, 6 months (if using 3rd generation HIV test) If HCP exposed to source with HIV and HCV, follow for 1 year.")
82
INFLUENZA: EPIDEMIOLOGY
Pathogens: A (most severe; pandemics), B (less severe; epidemics) and C (mild) Geographic distribution: Global Reservoir: Humans, swine, birds Incubation: 1-5 days (average ~2 days) Transmission: Droplet (airborne?), direct and indirect contact Communicability 1-2 days before onset of symptoms to 7 days post-onset (adults) or 10 days (children) Attack rate: Up to 60% in closed setting No carrier state but inapparent or mild illness may occur
, B (less severe; epidemics) and C (mild) Geographic distribution: Global. Reservoir: Humans, swine, birds. Incubation: 1-5 days (average ~2 days) Transmission: Droplet (airborne ), direct and indirect contact. Communicability. 1-2 days before onset of symptoms to 7 days post-onset (adults) or 10 days (children) Attack rate: Up to 60% in closed setting. No carrier state but inapparent or mild illness may occur.")
83
Influenza Disease Burden to U.S. Society in an Average Year
Deaths 25, ,000 Hospitalizations 114, ,500 Physician visits ~ 25 million Influenza Disease Burden to U.S. Society in an Average Year A recent study by Thompson et al concluded that the number of influenza-related deaths has increased significantly in the past 2 decades [Thompson 2003]. The number of pneumonia and influenza deaths rose by 83% from the through influenza seasons. For the through seasons, the greatest average numbers of deaths were associated with influenza A (H3N2) viruses, followed by influenza B, and influenza A (H1N1). Influenza viruses were associated with annual averages of 8,097 underlying pneumonia and influenza deaths, 36,155 underlying respiratory and circulatory deaths, and 51,203 all-cause deaths. The authors attributed the increase in influenza-related deaths during the past 2 decades at least partially to the aging of the population. They noted that people aged 85 years of age and older are 32 times more likely to die from an influenza-associated underlying pneumonia and influenza death than people between 65 and 69 years old. Because it is a highly contagious, acute respiratory disease, influenza is responsible for an average of 50 to 60 million infections annually, resulting in 25 million health care visits [Couch 2000]. An estimated 114,000 to 142,000 excess hospitalizations occur each year secondary to influenza [ACIP 2004], although others suggest it may be over 0.25 million [Couch 2000]. The annual direct medical costs of influenza are estimated at between $1 and $3 billion [Patriarca 1999]. Economic losses are likely higher: $3 to $5 billion [Patriarca 1999]. Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA. 2003;289: Couch RB. Influenza: prospects for control. Ann Intern Med. 2000;133: Advisory Committee on Immunization Practices. Prevention and control of influenza. MMWR. 2004;53(RR06):1-40. Patriarca PA. New options for prevention and control of influenza. JAMA. 1999;282:75-77. Infections and illnesses million Thompson WW et al. JAMA. 2003;289: Couch RB. Ann Intern Med. 2000;133: Patriarca PA. JAMA. 1999;282:75-7. ACIP. MMWR. 2004;53(RR06):1-40.
 viruses, followed by influenza B, and influenza A (H1N1). Influenza viruses were associated with annual averages of 8,097 underlying pneumonia and influenza deaths, 36,155 underlying respiratory and circulatory deaths, and 51,203 all-cause deaths. The authors attributed the increase in influenza-related deaths during the past 2 decades at least partially to the aging of the population. They noted that people aged 85 years of age and older are 32 times more likely to die from an influenza-associated underlying pneumonia and influenza death than people between 65 and 69 years old. Because it is a highly contagious, acute respiratory disease, influenza is responsible for an average of 50 to 60 million infections annually, resulting in 25 million health care visits [Couch 2000]. An estimated 114,000 to 142,000 excess hospitalizations occur each year secondary to influenza [ACIP 2004], although others suggest it may be over 0.25 million [Couch 2000]. The annual direct medical costs of influenza are estimated at between $1 and $3 billion [Patriarca 1999]. Economic losses are likely higher: $3 to $5 billion [Patriarca 1999]. Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and. respiratory syncytial virus in the United States. JAMA. 2003;289: Couch RB. Influenza: prospects for control. Ann Intern Med. 2000;133: Advisory. Committee on Immunization Practices. Prevention and control of influenza. MMWR. 2004;53(RR06):1-40. Patriarca PA. New options for prevention and control of influenza. JAMA. 1999;282: Infections and illnesses million. Thompson WW et al. JAMA. 2003;289: Couch RB. Ann Intern Med. 2000;133: Patriarca PA. JAMA. 1999;282:75-7. ACIP. MMWR. 2004;53(RR06):1-40.")
84
Clinical Manifestations by Age Group
Influenza Sign/Symptom Children Adults Elderly Cough (nonproductive) ++ ++++ +++ Fever + Myalgia Headache Malaise Sore throat Rhinitis/nasal congestion Abdominal pain/diarrhea – Nausea/vomiting Clinical Manifestations by Age Group In general, influenza may include these symptoms [ High fever Headache Tiredness/weakness (can be extreme) Nonproductive cough Sore throat Runny nose Body or muscle aches Diarrhea and vomiting also can occur, but are more common in children Common physical signs of influenza infection include the appearance of being ill, skin that is hot and moist to the touch, flushed face, hyperemic mucus membranes, and clear nasal discharge [Cox 1999]. This slide identifies the symptoms that occur most or least frequently in persons of varying age with influenza and, therefore, that have the more or less value in diagnosing influenza infection in specific age groups. Monto et al reported that, in patients aged 12 years and older, the best multivariate predictors of influenza during confirmed community influenza outbreaks are cough and fever, with a significant positive predictive value of 79% (P<.001) [Monto 2000]. In children, gastrointestinal symptoms such as nausea, vomiting, abdominal pain, and diarrhea are frequently observed [Cox 1999]. Febrile convulsions are the initial sign of influenza infection in many children [Cox 1999]. Adults and adolescents may have abrupt onset of fever and chills with headache, sore throat, myalgia, malaise, anorexia, and a dry cough [Cox 1999]. Elderly patients may not develop a low-grade fever, thereby its absence does not rule out the flu. However, shortness of breath is a common presenting symptoms in elderly persons [Cox 1999]. Monto AS, Gravenstein S, Elliott M, et al. Clinical signs and symptoms predicting influenza infection Arch Intern Med. 2000;160: Cox NJ, Subbarao K. Influenza. Lancet. 1999;354: ++++ Most frequent sign/symptom; + Least frequent; – Infrequent Monto AS et al. Arch Intern Med. 2000;160: Cox NJ et al. Lancet. 1999;354:
 Fever. + Myalgia. Headache. Malaise. Sore throat. Rhinitis/nasal congestion. Abdominal pain/diarrhea. – Nausea/vomiting. Clinical Manifestations by Age Group. In general, influenza may include these symptoms [ High fever. Headache. Tiredness/weakness (can be extreme) Nonproductive cough. Sore throat. Runny nose. Body or muscle aches. Diarrhea and vomiting also can occur, but are more common in children. Common physical signs of influenza infection include the appearance of being ill, skin that is hot and moist to the touch, flushed face, hyperemic mucus membranes, and clear nasal discharge [Cox 1999]. This slide identifies the symptoms that occur most or least frequently in persons of varying age with influenza and, therefore, that have the more or less value in diagnosing influenza infection in specific age groups. Monto et al reported that, in patients aged 12 years and older, the best multivariate predictors of influenza during confirmed community influenza outbreaks are cough and fever, with a significant positive predictive value of 79% (P<.001) [Monto 2000]. In children, gastrointestinal symptoms such as nausea, vomiting, abdominal pain, and diarrhea are frequently observed [Cox 1999]. Febrile convulsions are the initial sign of influenza infection in many children [Cox 1999]. Adults and adolescents may have abrupt onset of fever and chills with headache, sore throat, myalgia, malaise, anorexia, and a dry cough [Cox 1999]. Elderly patients may not develop a low-grade fever, thereby its absence does not rule out the flu. However, shortness of breath is a common presenting symptoms in elderly persons [Cox 1999]. Monto AS, Gravenstein S, Elliott M, et al. Clinical signs and symptoms predicting influenza infection Arch Intern. Med. 2000;160: Cox NJ, Subbarao K. Influenza. Lancet. 1999;354: Most frequent sign/symptom; + Least frequent; – Infrequent. Monto AS et al. Arch Intern Med. 2000;160: Cox NJ et al. Lancet. 1999;354:")
85
Influenza Manifestations & Complications
Children Adults Frequent Sinusitis, bronchitis, bronchiolitis, pneumonia, croup, acute otitis media Primary viral pneumonia, secondary bacterial pneumonia, sinusitis, bronchitis Rare Encephalopathy, myositis, rhabdomyolysis, myocarditis, pericarditis, Reye syndrome, sepsis-like syndrome Myositis, rhabdomyolysis, myocarditis, pericarditis Exacerbations of underlying disease Cardiovascular, diabetes, asthma, cystic fibrosis Cardiovascular, diabetes, asthma, COPD Influenza Manifestations & Complications Loughlin J, Napalkov P, Wegmueller Y et al. A study of influenza and influenza-related complications among children in a large US health insurance plan database. Pharmacoeconomics 2003;21: Treanor JJ. Influenza virus. In: mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas and Bennetts Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, PA: Churchill Livingstone; 2000: ACIP. MMWR 2004;53(RR06):1-40. Loughlin J et al. Pharmocoeconomics. 2003;21: Treanor JJ. Influenza virus. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, PA: Churchill Livingstone; 2000: ACIP. MMWR 2004;53 (RR06):1-40.
:1-40. Loughlin J et al. Pharmocoeconomics. 2003;21: Treanor JJ. Influenza virus. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, PA: Churchill Livingstone; 2000: ACIP. MMWR 2004;53 (RR06):1-40.")
86
CDC. MMWR 2008;57(RR-18):1-59
:1-59")
87
Type of Nuclear Material
Viral Nomenclature Type of Nuclear Material Hemagglutinin Neuraminidase A / Sydney / 184 / 93 (H3N2) Virus type Geographic origin Strain number Year of isolation Virus subtype 1. CDC. Atkinson W, et al. Chapter 13: Influenza. In: Epidemiology and Prevention of Vaccine-Preventable Diseases, 4th ed. Department of Health and Human Services, Public Health Service, 1998, 220
 Virus type. Geographic origin. Strain number. Year of isolation. Virus subtype. 1. CDC. Atkinson W, et al. Chapter 13: Influenza. In: Epidemiology and Prevention of Vaccine-Preventable Diseases, 4th ed. Department of Health and Human Services, Public Health Service, 1998, 220.")
88
Pandemic influenza …………… 1918 1977 H1N1 “Spanish” H1N1 “Russian” 1947
2009 H1N1 pdm09 1957 H2N2 “Asian” flu 1968 H3N2 “Hong Kong” flu 1940 Influenza B

89
INFLUENZA: PREVENTION
Respiratory hygiene Hand hygiene Droplet precautions for ill patients Furlough for ill HCP Influenza vaccine for HCP and patients May use antiviral for pre-exposure (only if vaccine contra-indicated), PEP (immunocompromised, pregnant), and treatment
, PEP (immunocompromised, pregnant), and treatment.")
90
STANDARD VERSUS HIGH DOSE INFLUENZA VACCINE, ADULTS >75 YEARS
Falsey AR, et al. JID 2009;200:172-80

91
EFFICACY OF HIGH DOSE INFLUENZA VACCINE: INFLUENZA A
PD ILI = protocol-defined influenza-like illness; presented Oct. ACIP meeting

92
EFFICACY OF HIGH DOSE INFLUENZA VACCINE: INFLUENZA B

93
INFLUENZA IN HEALTHCARE FACILITIES
More than 25 outbreaks described in literature in acute care hospitals Infected staff may initiate outbreak or aid in propagation HCW infection may lead to absenteeism and disruption of health care Attack rates in HCWs have ranged from 25% to 80% More than 15 outbreaks described in literature in extended care facilities Important morbidity and mortality among residents may result High rates of immunization (>60%) among staff may lead to decreased attack rate in residents
 among staff may lead to decreased attack rate in residents.")
94
SUMMARY OF CLUSTER RCTs ASSESSING THE IMPACE OF HCP IMMUNIZATION
Study Coverage Control Intervention Mortality Difference Potter J, 1997 4.9% 61% 17% 10% 7.0% Carman W, 2000 13.6% 50.9% 22.4% 8.8% Hayward A, 2006 5.9% 43.2% 15.3% 11.2% 4.1% Lemaitre M, 2009 31.8% 69.9% 6.0% 5.2% 0.8%* Multivariate analysis for death, vaccination OR 0.80 (p=0.008)
")
95
Indirect Benefits of Influenza Vaccination of Health Care Providers
Mortality of residents was significantly reduced (10% vs 17%) in nursing homes where the staff was vaccinated (SV) compared to facilities where they were not (S0) 20 Vaccine groups SV (n=490) SO (n=561) (P=0.0009) Total patient mortality (%) 10 Indirect Benefits of Influenza Vaccination of Health Care Workers In the season, the effects of vaccination of healthcare workers on morbidity and mortality of the patient population was studied in a randomized, controlled study in Glasgow. N = 1059 patients in 12 geriatric medical long-term care facilities; 653 (61%) of 1078 healthcare workers were vaccinated Vaccination of healthcare workers was associated with a reduction in total patient mortality from 17% to 10% (odds ratio 0.56; 95% CI 0.40, 0.80). ILI odds ratio was 0.57 (95% CI 0.34, 0.94). Vaccination of residents was not associated with significant effects on mortality; odds ratio 1.15 (95% CI 0.81, 1.64). Potter J, Stott DJ, Elder RAG et al. Influenza vaccination of health care workers in long-term-care Hospitals reduces the mortality of elderly patients. J Infect Dis 1997;175:1-6. 20 40 60 80 100 120 140 Time in days Potter J et al. J Inf Dis. 1997;175:1-6.
 in nursing homes where the staff was vaccinated (SV) compared to facilities where they were not (S0) 20. Vaccine groups. SV (n=490) SO (n=561) (P=0.0009) Total patient mortality (%) 10. Indirect Benefits of Influenza Vaccination of Health Care Workers. In the season, the effects of vaccination of healthcare workers on morbidity and mortality of the patient population was studied in a randomized, controlled study in Glasgow. N = 1059 patients in 12 geriatric medical long-term care facilities; 653 (61%) of 1078 healthcare workers were vaccinated. Vaccination of healthcare workers was associated with a reduction in total patient mortality from 17% to 10% (odds ratio 0.56; 95% CI 0.40, 0.80). ILI odds ratio was 0.57 (95% CI 0.34, 0.94). Vaccination of residents was not associated with significant effects on mortality; odds ratio 1.15 (95% CI 0.81, 1.64). Potter J, Stott DJ, Elder RAG et al. Influenza vaccination of health care workers in long-term-care. Hospitals reduces the mortality of elderly patients. J Infect Dis 1997;175: Time in days. Potter J et al. J Inf Dis. 1997;175:1-6.")
96
Indirect Benefits of Influenza Vaccination of Health Care Providers
20 long-term care facilities, stratified cluster randomization staff influenza vaccination or not Resident mortality odds ratio 0.58 (95% CI 0.40, 0.84) p=0.014 Resident mortality (%) Indirect Benefits of Influenza Vaccination of Health Care Workers 20 long-term care facilities in UK ( patients). Randomly offered vaccine or not. All deaths were recorded over 6 months in winter of 1996/97. Random sample of 50% of patients selected for virological surveillance combined with nasal and throat swabs every 2 weeks during the epidemic period. Swabs tested by tissue culture and PCR for influenza A and B. Influenza uptake in healthcare workers was 50.9% in hospitals in which they were routinely offered vaccine, compared with 4.9% in those in which they were not. Uncorrected rates of mortality are given in the slide. Mortality of residents (n =102/749) in ‘vaccine hospitals’ was 13.6% Mortality of residents (n=154/688) in ‘no vaccine hospitals’ was 22.4% At necropsy, PCR was positive in 0 of 17 patients from vaccine hospitals and 6 of 30 from no vaccine hospitals (p=0.055). Vaccination of healthcare workers was associated with a substantial decrease in mortality among LTCF residents. Virological surveillance showed no associated decrease in non-fatal influenza infection in patients. Carman WF, Elder AG, McAulay K et al. Effects of influenza vaccination of healthcare workers on mortality of elderly people in long-term care: a randomised controlled trial. Lancet 2000;355:93-7. n = 749 n = 688 No significant difference in % residents positive for influenza: ‘Vaccine hospitals’ 5.4%; ‘no vaccine hospitals’ 6.7% Carman WF et al. Lancet. 2000;355:93-7.
 p= Resident mortality (%) Indirect Benefits of Influenza Vaccination of Health Care Workers. 20 long-term care facilities in UK ( patients). Randomly offered vaccine or not. All deaths were recorded over 6 months in winter of 1996/97. Random sample of 50% of patients selected for virological surveillance combined with nasal and throat swabs every 2 weeks during the epidemic period. Swabs tested by tissue culture and PCR for influenza A and B. Influenza uptake in healthcare workers was 50.9% in hospitals in which they were routinely offered vaccine, compared with 4.9% in those in which they were not. Uncorrected rates of mortality are given in the slide. Mortality of residents (n =102/749) in ‘vaccine hospitals’ was 13.6% Mortality of residents (n=154/688) in ‘no vaccine hospitals’ was 22.4% At necropsy, PCR was positive in 0 of 17 patients from vaccine hospitals and 6 of 30 from no vaccine hospitals (p=0.055). Vaccination of healthcare workers was associated with a substantial decrease in mortality among LTCF residents. Virological surveillance showed no associated decrease in non-fatal influenza infection in patients. Carman WF, Elder AG, McAulay K et al. Effects of influenza vaccination of healthcare workers. on mortality of elderly people in long-term care: a randomised controlled trial. Lancet. 2000;355:93-7. n = 749. n = 688. No significant difference in % residents positive for influenza: ‘Vaccine hospitals’ 5.4%; ‘no vaccine hospitals’ 6.7% Carman WF et al. Lancet. 2000;355:93-7.")
97
REDUCTION IN OUTCOMES IN HCP RECEIVING INFLUENZA VACCINE
infection Sick days due to respiratory illness Days lost from work Patient mortality Patient mortality 28% 41% 41% 39% 88% Saxen 1999 Carmen 2000 Potter 1997 Wilde 1999 Wilde 1999* Attack rate unvaccinated = 13.4% Talbot TT, Weber DJ, et al. ICHE 2005;26:

98
BARRIERS AND SOLUTIONS TO HCW INFLUENZA VACCINE CONCERNS
Access to vaccine, inconvenience Off-hours clinics Use of mobile vaccination carts Vaccination at staff and department meetings Cost Provision of vaccine free of charge Concerns for adverse events Targeted education, including specific information to dispel vaccine myths

99
BARRIERS AND SOLUTIONS TO HCW INFLUENZA VACCINE CONCERNS
Fear of needles Use of LAIV for eligible HCP Other Strong and visible leadership Visible vaccination of key leaders Surveillance of HCP-associated influenza Accurate tracking of individual and unit-based compliance Active declination for HCP who do not wish to be or cannot be vaccinated

100
THANK YOU!

Similar presentations





















![Health Care Personnel Influenza Vaccination [ORGANIZATION NAME] [ORGANIZATION LOGO]](/19/5878711/big_thumb.jpg "Health Care Personnel Influenza Vaccination [ORGANIZATION NAME] [ORGANIZATION LOGO]>")