Download presentation
Presentation is loading. Please wait.

1
Cancer- Associated Thrombosis CAT
Academic Day - Medical Oncology Jan 28, 2011

2
Armand Trousseau 1865: Association of Cancer and Thrombosis

3
“…struck by the frequency with which cancerous patients are affected with painful edema of the…extremities…other cases, in which the absence of appreciable tumour made me hesitate as to the nature of a disease of the stomach, my doubts were removed … I know the disease to be cancerous when phlegmasia alba dolens appeared in the … limb. There appears to be cachexiae…a particular condition of the blood which predisposes to spontaneous coagulation” Armand Trousseau, New Sydenham Society 1865

4
“J’ai perdu” “I am lost” the nature of my illness”
“The phlebitis that has just appeared tonight leaves me no doubt as to the nature of my illness” Trousseau 1867

5
Cancer and Venous Thromboembolism A two way street
Cancer causes Thrombosis CANCER THROMBOSIS Thrombosis affects the Biology of Cancer

6
Cancer and VTE - Introduction
Major complication in 4-20% of pts 6x risk Leading cause of death Risk increases with Cancer Therapy VTE Prophylaxis and Treatment - Complex Risk of recurrence & bleeding on treatment VTE in Cancer pts Reduction in Survival

7
VTE in Cancer Impact and Implications
May indicate occult Cancer May complicate known Cancer May complicate hospitalization, surgery or systemic Rx for Cancer

8
VTE in Cancer Impact and Implications
Second leading cause of death Interrupts/delays needed Ca treatment Anticoagulant therapy increases bleeding risk Reduces survival x likelihood of death Increases readmission x4 25% for VTE issues Economic burden: Hospitalization 11 days $20,000 (U.S. figures )
")
9
Cancer and VTE Topics for Discussion Pathogenesis of Thrombosis
Epidemiology - Tumour type/stage, ChemoRx Prognosis of Cancer and VTE Prophylaxis: Surgery/Medical/Central Catheters Thalidomide and Myeloma Treatment of VTE – Failure of LMWHs

10
Cancer and VTE Additional Topics New anticoagulants ?? For Cancer
Cancer Survival and Anticoagulants ? Treatment of Portal/Splenic Vein Thrombosis Treatment of Central Venous Catheter clots Treatment of Tumour Thrombi eg Renal Cell Ca Malignancy Workup in Idiopathic VTE

11
Cancer and VTE Pathogenesis

12
Rudolf Virchow

13
VIRCHOW’S TRIAD STASIS ENDOTHELIAL INJURY DVT HYPERCOAGULABILITY

14
Virchow’s Triad & Cancer
Venous stasis Prolonged bedrest Venous compression by tumor or nodes Venous invasion by tumor Endothelial Injury Direct invasion/adhesion by tumor Surgery Chemotherapy Radiation Venous catheters

15
Virchow’s Triad & Cancer
Activation of coagulation Tumour Cell Activities Procoagulant Fibrinolytic Inflammatory Cytokines Direct cell interactions - Endothelial - Monocytes/Macrophages - Platelets

16
Cancer and Thrombosis ↑TF ↑TF ↑PAI ↑TF ↑TF ↓ TM Platelet Plt TC
F X TF- FVIIa Prothrombin FVIIa uPAR Fibrinogen TF uPA FXa CP Thrombin TUMOUR CELL VEGF Fibrin Adhesion Mitogen Mitogen TNF IL-1 Monocyte Platelet ↑TF IL- 8 Plt ↑TF ↑PAI Adhesion TC ↑TF ↑TF ↓ TM Endothelial cell Rickles, F. Thrombosis Research 2001

17
Cancer and Thrombosis - Procoagulant
F X TF- FVIIa Prothrombin FVIIa uPAR Fibrinogen TF uPA FXa CP Thrombin TUMOUR CELL VEGF Fibrin Adhesion Mitogen Mitogen TNF IL-1 Monocyte Platelet ↑TF IL- 8 Plt ↑TF ↑PAI Adhesion TC ↑TF ↑TF ↓ TM Endothelial cell Rickles, F. Thrombosis Research 2001

18
Procoagulant Activity
Tissue Factor Transmembrane glycoprotein forms complex with VIIa Prime activator of Coagulation Cancer cells express TF constitutively Major role in VEGF/angiogenesis Cancer Procoagulant Cysteine proteinase Activates factor X directly Mostly in malignant tissue (Acute Promyelocytic Leukemia)
")
19
Cancer and Thrombosis - Fibrinolysis
F X TF- FVIIa Prothrombin FVIIa uPAR Fibrinogen TF uPA FXa CP Thrombin TUMOUR CELL VEGF Fibrin Adhesion Mitogen Mitogen TNF IL-1 Monocyte Platelet ↑TF IL- 8 Plt ↑TF ↑PAI Adhesion TC ↑TF ↑TF ↓ TM Endothelial cell Rickles, F. Thrombosis Research 2001

20
Fibrinolytic Properties
Most tumor cells can express proteins necessary for fibrinolysis: u-PA, t-PA and PAI-1, PAI-2 May also express receptors to activate fibrinolysis Likely cause of bleeding problems in leukemia Plasminogen activators/inhibitors may play role in tumor invasion, proliferation, and metastasis

21
Cancer and Thrombosis - Cytokines
F X TF- FVIIa Prothrombin FVIIa uPAR Fibrinogen TF uPA FXa CP Thrombin TUMOUR CELL VEGF Fibrin Adhesion Mitogen Mitogen TNF IL-1 Monocyte Platelet ↑TF IL- 8 Plt ↑TF ↑PAI Adhesion TC ↑TF ↑TF ↓ TM Endothelial cell Rickles, F. Thrombosis Research 2001

22
Tumours release inflammatory cytokines:
Cytokine Release Tumours release inflammatory cytokines: TNF, IL-1 acts on vascular endothelial cells Tissue Factor and PAI Thrombomodulin ( Protein C activation) VEGF (Vascular endothelial growth factor) Tissue Factor by endothel. cells and monocytes adhesion molecules expression by endothel. cells - attracts platelets, WBCs, tumour cells
 VEGF (Vascular endothelial growth factor) Tissue Factor by endothel. cells and monocytes. adhesion molecules expression by endothel. cells. - attracts platelets, WBCs, tumour cells.")
23
Cancer and Thrombosis – Cell interactions
F X TF- FVIIa Prothrombin FVIIa uPAR Fibrinogen TF uPA FXa CP Thrombin TUMOUR CELL VEGF Fibrin Adhesion Mitogen Mitogen TNF IL-1 Monocyte Platelet ↑TF IL- 8 Plt ↑TF ↑PAI Adhesion TC ↑TF ↑TF ↓ TM Endothelial cell Rickles, F. Thrombosis Research 2001

24
Tumor Cell Interactions with Host Cells
Endothelial Cells Indirect: via cytokines (TNF, IL-1, VEGF) Direct: Tumour cells have membrane adhesion molecules These integrins and selectins bind to tumour adhesion molecules receptors on endothelium cells Initiates local clotting activation & thrombosis Attracts and activates platelets and WBC’s Tumor-tumor and tumor-vascular cell adhesion leads to cell migration, cell invasion, angiogenesis
 Direct: Tumour cells have membrane adhesion molecules. These integrins and selectins bind to tumour adhesion molecules receptors on endothelium cells. Initiates local clotting activation & thrombosis. Attracts and activates platelets and WBC’s. Tumor-tumor and tumor-vascular cell adhesion leads to cell migration, cell invasion, angiogenesis.")
25
Tumor Cell Interactions with Blood Cells
Platelets Direct Adhesion of platelets to tumor cells and to vascular endothelial cells Activation by tumor cells in vitro & in vivo Release of proaggregation factors (ADP, cathepsin)
")
26
Tumor Cell Interactions with Blood Cells
Monocyte-Macrophage Tumors may induce expression of Tissue Factor on mononuclear phagocytes directly or via inflammatory mediators May be mechanism of localized fibrin deposition within tumor tissue

27
Cancer and VTE Epidemiology

28
Cancer and VTE – Epidemiology
4-20% of Cancer patients will have VTE during the course of their disease 15% Symptomatic, 50% asymptomatic, 50% autopsy Cancer has 4-7x risk of VTE Active Cancer accounts for 20% of New VTEs VTE is second most common cause of death

29
Cancer and VTE – Epidemiology
Annual Incidence - Small Cohort (Hospital)studies 6-8% - Epidemiological studies (data bases) - Recent Population studies ~ 1% Time course of VTE Odds Ratio Highest Incidence first 3 months 54X 3 -12 months 14X 1 - 3 years 4X
studies 6-8% - Epidemiological studies (data bases) Recent Population studies ~ 1% Time course of VTE Odds Ratio. Highest Incidence first 3 months 54X months 14X years 4X.")
30
Cancer and Risks of VTE Cancer - related Factors Treatment - related Factors Patient - related Factors Biomarkers

31
Cancer and Risks of VTE Cancer-related Factors
Tumour type: pancreas, stomach, gynecologic, renal, lung, primary brain, lymphoma, myeloma Advanced stage Initial period after diagnosis (3-6 months) Histology – adeno Ca >> squamous Ca 2-3x
 Histology – adeno Ca >> squamous Ca 2-3x.")
32
Cancer and Risks of VTE Treatment-related Factors Major Surgery RR 2x
Hospitalization RR 2.3x Cancer Therapy Chemotherapy RR x Hormonal therapy RR 1.6x Anti-angiogenesis drugs RR x Erythropoiesis Stimulating agents RR 1.7x Transfusions RR 1.6x Central vein catheters ??? 14%~4% recent data

33
Cancer and Risks of VTE Patient -related Factors Older age Female Sex
Race Black > Caucasian > Asian Comorbidities: Infection, Renal, Pulmonary, Arterial Thrombosis, Anemia, Obesity RR ~ Prothrombotic Mutations – FVL, Prothrombin Gene Prior VTE RR 6x Performance status- Immobility RR 2-4x

34
Cancer and Risks of VTE Candidate Biomarkers Risk Models
Pre-chemo platelets > 350,000 Pre-chemo WBC > 11,000 Hb < 100 gm/l Elevated Tissue Factor – Hi grade expression in Tumour cells, ↑Systemic TF levels ↑ D-dimer ↑ Soluble P-selectin (12%) RR 2.6 ↑ C-reactive protein
 RR 2.6. ↑ C-reactive protein.")
36
Cancer and Risks of VTE Cancer-related Factors
Tumour type: pancreas, stomach, gynecologic, renal, lung, primary brain, lymphoma, myeloma Advanced stage Initial period after diagnosis (3-6 months) Histology – adeno Ca>> squamous Ca 2-3x
 Histology – adeno Ca>> squamous Ca 2-3x.")
37
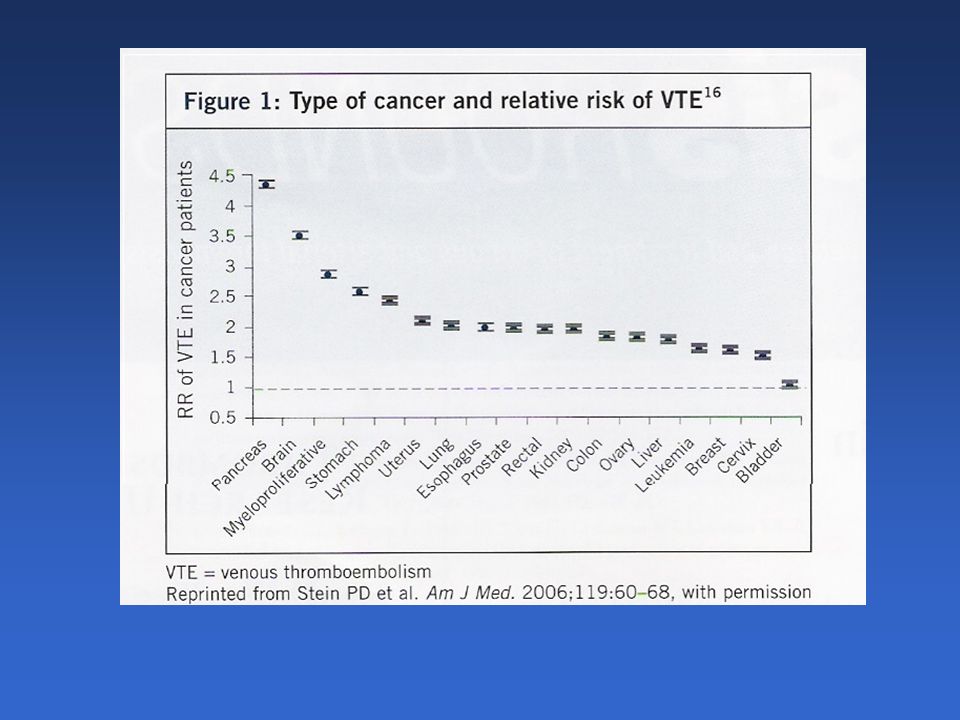
Cancer and VTE Cancers most strongly associated with VTE:
Bone 75 per 1,000/yr Ovary 65 Brain 64 Pancreas 45 Cancers most common in patients with VTE: Breast 26% of 1426 VTE’s Colorectal 13% Prostate 12% 168 Lung 11% 152 Based on population registry data, we now have fairly good data that the cancers that are most strongly associated with VTE are those of the brain, pancreas, and ovary. But because of the low prevalence of these malignancies, the cancers most commonly observed in patients with VTE are the most common cancers, including breast, colorectal and lung. Blom J. J Thromb Haemost 2006; 4:

38
Frequency, Risk Factors and Trends for VTE in Cancer Pts in Hospital
Sites with Highest Risk VTE % Odds Ratio p Pancreas % <.0001 Kidney % Ovary % Lung % Stomach % Brain % Myeloma % Non Hodg Lymphoma % Hodg Lymphoma % Khorana et al Cancer 2007;110:

40
Cancer and VTE - Metastatic Disease
Metastatic Disease increases VTE risk 4-13X Incidence of VTE / 100 pt-yr Pancreas Stomach Bladder Renal Lung Chew et al. Arch Int Med. 2006;166:

41
Cancer and VTE Cancer Therapy

42
Cancer Therapy VTE odds ratio.
Surgery in Cancer pts x Hospitalization x Cancer therapy Chemotherapy x Hormonal therapy x Anti-angiogenesis agents 1.3x Support Rx- Erythropoiesis agents 1.7x Transfusions - RBCs/Platelets 1.6x Central Venous Catheters 28% 4% ??? Radiation ???

43
Cancer and VTE Thrombosis and Chemotherapy

44
VTE and Chemotherapy Chemotherapy - independent risk for VTE
Pts on Chemotherapy VTE % /yr VTE during Chemo Early Mortality RR 2X Cancer pts Cancer pts + Chemo VTE risk x x Recurrent VTE x x

45
Rate of VTE in Breast Cancer
Stage % VTE * Treatment I none tamoxifen tamoxifen + CTX II tamoxifen CTX tamoxifen + CTX III/IV CTX *Asymptomatic VTE

46
Prothrombotic Effects of Chemotherapy
Damage to vascular endothelium Platelet Activation/Aggregation Increased Procoagulants Decreased Anticoagulants (AT III, PC, PS) Tumour and Endothel. cell Apotosis increase TF Tumour cell Cytokine Release increases TF Monocyte/Macrophage Expression of TF Decrease Fibrinolysis Haddad T. Thromb Res :555-68
 Tumour and Endothel. cell Apotosis increase TF. Tumour cell Cytokine Release increases TF. Monocyte/Macrophage Expression of TF. Decrease Fibrinolysis. Haddad T. Thromb Res :")
47
VTE and Chemotherapy Chemotherapy and VTE 10-20% / yr
Cisplatin % L-asparaginase % Fluoruracil % Thalidomide + Decadron / ChemoRx % Anti-angiogenesis drugs (Avastin) marginal - 30%? Supportive Rx: EPO, G-CSF, Steroids %?
 marginal - 30% Supportive Rx: EPO, G-CSF, Steroids %")
48
Risk Model - ChemoRx associated VTE Khorana
Patient Characteristic Odds Ratio Cancer site Very high risk - stomach, pancreas 4.3 High Risk - lung, lymphoma, gyn, blad. testic Low Risk - breast, colorectal, Head & Neck 1.0 Pre-chemo Platelets >350x109/l Hgb <100 g/l or ESAs use Prechemo WBC > 11x109/l BMI >35 kg/m Khorana A. Blood 2008; 111:4902

49
Risk Model - ChemoRx associated VTE
Patient Characteristic Risk Score Cancer site Very high risk - stomach, pancreas 2 High Risk - lung, lymphoma, gyn, blad. Testic. 1 Pre-chemo Platelets >350x109/l Hgb <100 g/l or ESAs Prechemo WBC > 11x109/l BMI >35kg/m Khorana A. Blood 2008; 111:4902

50
Risk Model - ChemoRx associated VTE
Results during 4 cycles of ChemoRx Risk group % of pts Risk of VTE Risk Score Low 27% % Intermediate 60% % ≥ 3 High 13% % Median time – ChemoRx to VTE months Khorana A. Blood 2008; 111:4902

51
Risk Model – Progression/Mortality
Results after 4 months of ChemoRx (3%- 38 d) Risk group VTE Progression Death HR* % HR* % HR* Group 1 Low Group 2 Intermed Group 3 High * HR- Hazard Ratio p < .0001 Model predicts early VTE, Progression and Mortality Kuderer Blood 2008;112 ASH abstract 172
 Risk group VTE Progression Death. HR* % HR* % HR* Group 1 Low Group 2 Intermed Group 3 High * HR- Hazard Ratio p < Model predicts early VTE, Progression and Mortality. Kuderer Blood 2008;112 ASH abstract 172.")
52
Khorana Model Ay Model Risk Assessment Models
Thrombosis in Cancer Risk Assessment Models Khorana Model Ambulatory patients followed for febrile neutropenia and other complications on new chemo regimen VTE not a predefined outcome Ay Model Ambulatory patients with new diagnosis of cancer or progression of cancer followed in the Vienna CATS VTE is primary outcome and objectively verified Khorana model + D-dimer + sP-selectin Khorana et al. Blood Ay et al Blood 2010. ASH Education Session 2010

53
VTE Risk Model - CATS study Vienna CATS (Cancer and Thrombosis study)
Prospective, Observational Cohort study in Cancer pts Newly diagnosed or Progression after previous remission Brain, Breast, Lung, GI, Renal, Prostate, Myeloma, Lymphoma No ChemoRx > 3months, No surgery or RadioRx >2 weeks 2 year observation: VTE, death Risk of Symptomatic Objectively confirmed VTE Ay C et al. Blood 2010;116:5377

54
VTE Risk Model -CATS Patient Characteristic Risk Score Cancer site
Very high risk - stomach, pancreas 2 High Risk - lung, lymphoma, gyn, blad. Testic. 1 Pre-chemo Platelets > 350x109/l 1 Hgb < 100 g/l or ESAs 1 Prechemo WBC > 11x109/l 1 BMI > 35kg/m Soluble P- selectin ≥ ng/ml 1 D-Dimer ≥ 1.44 ug/ml 1 Ay C et al Blood 2010; 116:5377

55
Khorana VTE Risk Model - CATS
Results after 6 months Risk Score % of 819 pts Risk of VTE HR % 1.5% % % 2.7 2 27% 9.6% 5.5 ≥ % % 9.5 Score ≥ 3 PPV 22.1% NPV 94.9% Ay C et al Blood 2010; 116:5377

56
Khorana Model Validation
Thrombosis in Cancer Khorana Model Validation Prospective follow up of 819 patients Median observation time/follow-up: 656 days 6-mo cumulative VTE rates: Patients Events n % Score ≥3 93 17.7% Score 2 221 9.6% Score 1 229 3.8% Score 0 276 1.5% Log-rank test P<0.001) Ay et al Blood 2010. ASH Education Session 2010 56 56
 Ay et al Blood ASH Education Session")
57
Expanded VTE Risk Model - CATS
Results after 6 months Risk Score % of 819 pts Risk of VTE HR % % % % % % % % % % ≥ % % Score ≥ 5 PPV 42.9% NPV 94.4% Ay C et al Blood 2010; 116:5377

58
Ay Model for Outpatients
Thrombosis in Cancer Ay Model for Outpatients Addition of D-dimer and soluble P-selectin to Khorana model: 6-mo cumulative VTE rates: Patients, n Events, % Score ≥5 30 35% Score 4 51 20.3% Score 3 130 10.3% Score 2 218 3.5% Score 1 190 4.4% Score 0 200 1.0% Ay et al Blood 2010. ASH Education Session 2010 58 58

59
Cancer and VTE Prognosis

60
VTE, Cancer and Survival
1.00 DVT/PE and Malignant Disease 94 % 0.80 0.60 Probability of Death Malignant Disease 42% 0.40 DVT/PE Only 29% 0.20 We also now have evidence that VTE in cancer patients are associated with a particularly bad prognosis. In a study based on information on 9 million hospital discharges that was collected in the US Medicare database from 1998 to 1990, you can see that patients with cancer and thrombosis are almost 3 times more likely to die than patients with either disease alone. So having cancer certainly shortens survival, but having VTE on top of that dramatically increase the risk of dying over the next 6 months. Based on Medicare ICD-9 hospital discharge diagnoses during Nonmalignant Disease 20% 0.00 Number of Days Levitan - Medicine 1999;78:285

61
VTE, Cancer and Survival
100 1- yr survival Cancer at time of VTE 12% Cancer without VTE % 80 60 Survival, % of patients 40 p< .001 20 Similar findings has been reported by other population-based studies. In this study by from Denmark, you can see the the 1-y survival for patients who presented with cancer and VTE at the same time is only 1/3 of that in patients with cancers alone. Years after Diagnosis Sorensen - NEJM 2000;343:1846

63
Cancer and VTE Prophylaxis of VTE

64
Cancer and VTE- Prophylaxis
Prophylaxis in Surgery for Cancer Prophylaxis in Medical Pts with Cancer Prophylaxis for Central Venous Catheters

65
Cancer Associated Thrombosis CAT Prophylaxis and Treatment
ASCO ACCP 2008

66
Prophylaxis and Treatment in Patients with Cancer
Am. Soc of Clin. Oncology Guidelines Recommendations for VenousThromboembolism Prophylaxis and Treatment in Patients with Cancer G Lyman, A Khorana, A Falanga et al Journal of Clinical Oncology Dec. 1, 2007, 25(34):
:")
67
ACCP GUIDELINES Chest 133; 6 June 2008 supplement

68
ACCP Guidelines Levels of evidence/recommendations
Grade Risk/benefit Methodologic Strength Implications 1 A Clear RCTs Ø limitations Strong recommendations 1 B Clear RCTs + limitations Strong recommendations 1 C Clear Ø RCTs - extrapolations Strong recommendations 1 C Clear Observational studies Intermediate strength 2 A Unclear RCTs Ø limitations Intermediate strength 2 B Unclear RCTs + limitations Weak recommendations 2 C Unclear Ø RCTs - extrapolations Weak recommendations 2 C Unclear Observational studies Very weak

69
Cancer and VTE- Prophylaxis
Surgical Oncology

70
VTE and Surgical Oncology
Patients undergoing cancer surgery: Major risk group – no prophylaxis % VTE On prophylaxis - at least 2x the risk of DVT On prophylaxis - more than 3x the risk of fatal PE Cancer-independent predictor of prophylaxis failure Prolonged VTE risk % VTE Day 21+ post-op Cause of death in 46% in first 30 days post-op

71
2,373 patients in 31 Italian hospitals
Project: A Clinical Outcome-Based Prospective Study of VTE in Cancer Surgery 2,373 patients in 31 Italian hospitals 30-day Symptomatic VTE - 2.1% In-hospital prophylaxis: 82% Post-discharge prophylaxis: 31% Agnelli G - Ann Surg :89-95 DVT= PE= Death=0.8

72
@ristos: VTE Timing VTE Event - 40% > 21 days after surgery
No. events Agnelli G - Ann Surg :89-95

73
@ristos: 30-day Mortality
General: 2.9% Urological: 0.6% Gynecological: 0.2% Overall at 30 days: 1.7% VTE–related: 46% No. events Agnelli G - Ann Surg :89-95

74
@ristos: Risk Factors for VTE in Cancer Surgery
Variable Effect OR %CI Age 60 years Previous VTE Yes Anesthesia 2 hours Stage Advanced Bed rest post-op 4 days Agnelli G - Ann Surg :89-95

75
ENOXACAN II - Duration of Prophylaxis after Cancer Surgery
curative, open surgery for abdo or pelvic cancer double-blind RCT in 37 centers, 8 countries placebo enoxaparin 40 mg QD R enoxaparin 40 mg QD surgery Day 6-10 Day 25-31 bilat venography Bergqvist - NEJM 2002;346:975

76
Duration of Prophylaxis after Major Abdominal Surgery
unblinded, multicenter RCT (interim report) unspecified proportion had cancer (N=117) Prophylaxis stopped Dalteparin 5000 U od + GCS R Dalteparin 5000 U od surgery Day 7 Day 28 bilat venography Rasmussen - Cancer Treat Rep 2002; 28:141
 unspecified proportion had cancer (N=117) Prophylaxis stopped. Dalteparin 5000 U od + GCS. R. Dalteparin 5000 U od. surgery. Day 7. Day 28. bilat venography. Rasmussen - Cancer Treat Rep 2002; 28:141.")
77
Prolonged thromboprophylaxis after cancer operations
ENOXACAN II enoxaparin FAME dalteparin p=0.02 p=0.03 8/165 21/107 20/167 8/91 Rasmussen - ASH (2003) Bergqvist - NEJM 2002;346:975
 Bergqvist - NEJM 2002;346:975.")
78
Cancer Surgery Patients
Prophylaxis LDUH and LMWH efficacious in cancer surgery For anticoagulant prophylaxis, greater protection at higher doses UF Heparin tid vs bid dalteparin 5,000 U vs 2,500 U od Extending prophylaxis for 3 weeks after discharge 60% risk reduction in DVTs (venographic)
")
79
ASCO 2008 Guidelines – VTE in Cancer
Prophylaxis: Cancer Surgery - Prophylactic doses - UFH / LMWH / Fondaparinux early post-op x 7-10 days - Mechanical methods if bleeding risk - LMWH x 4 weeks for Major abdo-pelvic surgery, residual cancer, DVT risk (previous VTE, obese, prolonged immobility) Lyman G et al. J Clin Oncol 2007; 25(34):
 Lyman G et al. J Clin Oncol 2007; 25(34):")
80
ACCP 2008 Guidelines - VTE in Cancer
Prophylaxis: Cancer Surgery Cancer Patients undergoing major surgery Prophylaxis – LMWH, LDUH tid, Fondaparinux x 7-10 days or discharge Grade 1A Hi Risk Cancer Surgery Prophylaxis - up to 28 days post-op Grade 2A

81
Intermission – Spring Break

82
Cancer and VTE- Prophylaxis
Medical Oncology Ambulatory Patients

83
VTE and Chemotherapy Chemotherapy - independent risk for VTE
Pts on Chemotherapy VTE % /yr Cancer pts Cancer pts + Chemo VTE risk 4x x Recurrent VTE 2x x

84
Prevention of Thromboembolism in Cancer Medical Oncology Pts
Levine Stage IV Breast – RRR 85% Hass TOPIC Breast/Lung -NS Perry PRODIGE – Gliomas - NS Agnelli PROTECHT Metastatic Ca- RRR 47% Reiss CONKO Pancreas – RRR 65% Maraveyas 2009 FRAGEM Pancreas – RRR 62%

85
Prevention of Thromboembolism in Cancer
Stage IV breast cancer patients receiving CTX Double-blind RCT x 6 months Very low-dose warfarin: 1 mg x 6 wks INR Placebo Warfarin No Thromboembolism % % p = 0.03 Major bleeding % % NS All bleeding % % NS Levine - Lancet (1994)
")
86
Cumulative Thromboembolism in Patients Treated with Warfarin
Risk Reduction – 85% warfarin 20 placebo 15 Patients with thrombosis (%) 10 P=0.031 5 Author query: do you want to include the table which is present in the original figure, and lists the number of patients at risk who were received either warfarin or placebo during the months of randomization. Do you wish to mention the type of patients on this slide? i.e. patients receiving chemotherapy for metastatic breast cancer. delete 3 6 9 12 15 Time from randomization (months) Levine - Lancet 1994;343:886
 10. P= Author query: do you want to include the table which is present in the original figure, and lists the number of patients at risk who were received either warfarin or placebo during the months of randomization. Do you wish to mention the type of patients on this slide i.e. patients receiving chemotherapy for metastatic breast cancer. delete Time from randomization (months) Levine - Lancet 1994;343:886.")
87
Prevention of Thromboembolism in Cancer TOPIC studies
Advanced Cancer on ChemoRx LMWH vs. placebo x 6 months Dopplers q 4 weeks TOPIC 1- Breast Ca Placebo LMWH p VTE % 4% Bleeding % % TOPIC 2 - Lung Ca Overall VTE % % Stage IV VTE 10.1% % Bleeding % % Haas et al J Throm Haemos 2005; 3 (suppl) OR 059
 OR 059.")
88
Prevention of Thromboembolism in Cancer PRODIGE- ASC0 2007
Malignant Glioma LMWH vs. placebo x 6 months RCT double blind Target 512 pts Only 186 randomized *** Efficacy outcome: 6 month VTE-free survival Safety outcome : Bleeding Perry J. et al J Clin Onc :suppl abstract 2011

89
Prevention of Thromboembolism in Cancer PRODIGE - ASC0 2007
Outcomes LMWH Placebo 99 pts pts VTE % (9 ) 17% (12) HR .7 p=.3 Major Bleed % (5) % (1) HR 4.0 p= .2 All major bleeds - intracranial Perry J. et al J Clin Onc :suppl abstract 2011
 17% (12) HR .7 p=.3. Major Bleed 5.1% (5) 1.2% (1) HR 4.0 p= .2. All major bleeds - intracranial. Perry J. et al J Clin Onc :suppl abstract")
90
Prevention of Thromboembolism in Cancer PROTECHT study – ASH 2008
Metastatic or locally advanced Ca on ChemoRx RCT double-blind clinical outcome LMWH vs placebo 2:1 randomization while on ChemoRx maximum 4 months 1,150 pts LMWH 769: Placebo 381 Primary Efficacy Endpoint: Composite of Venous/Arterial Thromboembolic events Safety: Major Bleeding Agnelli Blood; 112:abstract 6

91
Prevention of Thromboembolism in Cancer PROTECHT study – ASH 2008
Cancer type % Lung Colon Breast Ovary Stomach Rectum Pancreas Head/Neck Other

92
Prevention of Thromboembolism in Cancer PROTECHT study - Results
LMWH Placebo Study Patients pts pts Treatment duration days days TE events % (16) % (15) p=.033 - Lung Ca % % - GI % 2.7% DVT % 2.1% PE % 0.8% Major Bleed % p=.177 Minor Bleed % 7.9% Relative Risk Reduction % NNT 53.8
 3.9% (15) p= Lung Ca 4% 8.8% - GI 1.5% 2.7% DVT 1.0% 2.1% PE 0.4% 0.8% Major Bleed 0.7% 0 p=.177. Minor Bleed 7.4% 7.9% Relative Risk Reduction % NNT")
93
Prevention of Thromboembolism in Cancer
CONKO 004 study – ASCO 2009 Open Prospective Randomized 312 Advanced Pancreatic Cancer ChemoRx vs ChemoRx + Enox 1mg/kg od x 3 months Outcomes: Symptomatic VTE /Bleeding Reiss et al JCO 2009; 27 LBA 4506

94
Prevention of Thromboembolism in Cancer
CONKO 004 – ASCO 2009 Outcome Observed Enox 1 mg/kg RRR 152 pts 160 pts VTE % % % Major Bleed % % No difference in Time to Progression or Overall Survival Reiss et al JCO 2009; 27 LBA 4506

95
Prevention of Thromboembolism in Cancer
FRAGEM study Prospective Multi-centre 123 Advanced Pancreatic Cancer Gemcitabine vs Gemcitabine + Fragmin (CLOT protocol) for 3 months Outcome: Study period VTE, Overall VTE, Death (VTE) Maraveyas A. Eur J of Cancer Suppl 2009;7:362
 for 3 months. Outcome: Study period VTE, Overall VTE, Death (VTE) Maraveyas A. Eur J of Cancer Suppl 2009;7:362.")
96
Prevention of Thromboembolism in Cancer
FRAGEM study Outcome Gem Gem+Fragmin RR 64 pts pts Overall VTE 31% % p= .02 Study Period VTE 25% % p=.002 Death (VTE) 9% % p=.028 Maraveyas A. Eur J of Cancer Suppl 2009;7:362
 9% 0% .08 p=.028. Maraveyas A. Eur J of Cancer Suppl 2009;7:362.")
97
Prevention of Thromboembolism in Cancer
Conflicting results of Prophylaxis studies Negative effect of prophylactic dose LMWH in some Lung, Breast, Glioma studies Positive effect of prophylactic dose LMWH in certain tumour eg lung, GI (PROTECHT) Positive effect in “Therapeutic dose” LMWH in Advanced Pancreatic Ca Optimal dose, duration, specific tumour type/stage needs further definition
 Positive effect in Therapeutic dose LMWH in Advanced Pancreatic Ca. Optimal dose, duration, specific tumour type/stage. needs further definition.")
98
Cancer and VTE- Prophylaxis Thalidomide and Lenalidomide
Medical Oncology Thalidomide and Lenalidomide

99
Thrombotic Complications with VEGF Inhibitors
Both Arterial (~5%) & Venous (~12%) Thrombosis and Bleeding associated with anti-VEGF drugs 16-23% thrombotic events with Bevacizumab – Avastin VTE RR= Nalluri - Meta- analysis 15 RCTs- 8,000 pts VEGF important for neoangiogenesis and maintenance of normal endothelial cell function and regeneration Anti-VEGF drugs Endothelial cell apotosis exposure of basement membrane – thrombosis decrease platelet inhibitors PGI-2 /NO3 - thrombosis loss of endothelial vessel lining integrity - bleeding
 & Venous (~12%) Thrombosis and Bleeding associated with anti-VEGF drugs % thrombotic events with Bevacizumab – Avastin. VTE RR= 1.38 Nalluri - Meta- analysis 15 RCTs- 8,000 pts. VEGF important for neoangiogenesis and maintenance of normal endothelial cell function and regeneration. Anti-VEGF drugs Endothelial cell apotosis. exposure of basement membrane – thrombosis. decrease platelet inhibitors PGI-2 /NO3 - thrombosis. loss of endothelial vessel lining integrity - bleeding.")
100
Thalidomide and VTE Thalidomide and analogs (Lenalidomide)
VTE risk with Thalidomide in Myeloma Rx <5% Thalidomide + Decadron % VTE + Anthracyclines 12-28% VTE Uncontrolled studies: efficacy “Mini dose” Warfarin, Full Dose Warfarin, LMWH, ASA

101
Thalidomide and VTE Mechanisms of Thalidomide associated VTE
Alters Endothelial cell PAR-1 expression after Doxorubicin injury leads to Thrombin binding and Platelet activation Serum Thrombomodulin drops in first month of Rx Acquired APC resistance High levels of vWf and FVIII

102
Thalidomide and Risks of VTE
Thalidomide Newly dx Relapsed/refractory alone % % + Hi dose Dex % % + Melphalan/Pred % % + Doxorubicin % %* + Cyclophosphamide % % + Multiagent Chemo % % Higher VTE Risk: Newly diagnosed RR 2.5 Doxorubicin regimen RR 4.3 Int Myeloma Working group. Leukemia 2008;22:414

103
Thalidomide and Risks of VTE
Lenalidomide Newly dx Relapsed/refractory Alone % + Dexamethasone 8-75% % RR 3.5 + Cyclophophamide % + Bortezomib % Thalidomide + ChemoRx in other Cancers Prostate: Thal + docetaxel % Renal Cell: Thal + Gemcitibine + 5-Fu % Melanoma /Brain mets: Thal + Temozolamide % Int Myeloma Working group. Leukemia 2008;22:414

104
Thalidomide and Risks of VTE
Risk Factors Obesity BMI > 30kg/m2 Previous VTE, Central Venous Catheter Co-morbid conditions: Cardiac, Renal, DM, Sepsis, Immobility Erythropoietin Newly diagnosed Myeloma, Hyperviscoisty Hi dose Dexamethasone Doxorubicin Multiagent ChemoRx

105
Thalidomide and VTE Prophylaxis “Suggestions”
Thalidomide alone No prophylaxis/ASA ?? 0 or 1 risk factor Thalidomide 2+ risk factors Prophylactic LMWH ***newly diagosed Warfarin INR 2-3 Thalidomide + Hi dose Dex Prophylactic LMWH + Doxorubicin Warfarin INR 2-3 + Multiagents *** No methodologically sound studies Int Myeloma Working group. Leukemia 2008;22:414

106
ASCO 2008 Guidelines – VTE in Cancer
Prophylaxis: Medical Oncology Pts - No routine prophylaxis for ambulating pts - ??? LMWH or Warfarin ~ INR 1.5+ Myeloma pts on Thalidomide + ChemoRx / Decadron (based on extrapolations from Ortho surgery and Breast Ca studies) Lyman G et al. J Clin Oncol 2007; 25(34):
 Lyman G et al. J Clin Oncol 2007; 25(34):")
107
ACCP 2008 Guidelines - VTE in Cancer Prophylaxis
Medical Oncology pts Ambulatory pts on Chemo/hormonal Rx No routine primary prophylaxis Grade 1C

108
Cancer and VTE- Prophylaxis Cancer Patients in Hospital
Medical Oncology Cancer Patients in Hospital

109
VTE Prophylaxis - Cancer Pts in Hospital
Study Pts Ca Pts Placebo Rx RR p VTE% VTE% MEDENOX % <.001 PREVENT % ARTEMIS % Lyman G et al. J Clin Oncol 2007; 25(34):
:")
110
ASCO 2008 Guidelines – VTE in Cancer
Prophylaxis: Hospitalized Pts: - Prophylactic doses - UFH / LMWH / Fondaparinux if no bleeding concerns Lyman G et al. J Clin Oncol 2007; 25(34):
:")
111
ACCP 2008 Guidelines - VTE in Cancer
Medical Oncology pts Bedridden with acute medical illness: Prophylactic doses – UFH / LMWH / Fondaparinux Grade 1A

112
Central Venous Catheters & VTE
Cancer and VTE Central Venous Catheters & VTE

113
Incidence of CVC-Related DVT
Not well established Methodologically weak studies & inconsistencies among the studies: - differences in study design and study population - lack of standardized technique of CVC insertion - inconsistent definition of VTE events (CVC occlusion vs fibrin sleeve) - different levels of clinical surveillance - variable accuracy of diagnostic tests
 - different levels of clinical surveillance. - variable accuracy of diagnostic tests.")
114
Incidence of CVC-Related DVT
Rate of thrombosis requiring PICC removal – 3.4% 1.1/1,000 catheter days - no prophylaxis (n=351) Walshe – J Clin Onc 2002; 20:3276 Symptomatic thrombosis - 4% /1,000 device days PICCs, Porta- caths, Hickman catheters – 444 pts A. Lee - J Clin Onc 2006; 24:1404 Clinically Important CVC-related DVT %
 Walshe – J Clin Onc 2002; 20:3276. Symptomatic thrombosis - 4% 0.3 /1,000 device days PICCs, Porta- caths, Hickman. catheters – 444 pts. A. Lee - J Clin Onc 2006; 24:1404. Clinically Important CVC-related DVT 2 - 4%")
115
Central Venous Catheter - DVT Risk Factors
Risk Factor O.R. More than 1 attempt 5.5 Previous CVC insertion 3.8 Left side CVC 3.5 Tip Position SVC vs RA 2.7 Arm vs Chest ports 8.1 Khorana J Clin Onc 2009; 27:4839

116
Preventing Central Venous Catheter Thrombosis in Cancer (RCTs)
Warfarin 1 mg/day DVT sympt DVT Study Endpoint No. control warf control warf Bern, venogram D % * 10 % % 10 % Couban, sympt. DVT NR NR % % Heaton, sympt. thromb NR NR % 18 %

117
Preventing Central Venous Catheter Thrombosis in Cancer (RCTs)
LMWH DVT Study Endpoint No. control LMWH P Monreal, venogram Day % * 6 % Reichardt, clinical % %

118
CVC-related Thrombosis in Cancer Pts
Rate of clinically-important symptomatic DVT appears to have decreased ~ 4% Rate of thrombosis requiring PICC removal – 3.4% Primary prophylaxis with Minidose warfarin or LMWH appear to NOT be effective nor necessary in general

119
ACCP 2008 Guidelines - VTE in Cancer
Prophylaxis: Medical Oncology pts Bedridden with acute medical illness Prophylaxis - LDUH, LMWH, Fondaparinux Gr 1A Ambulatory receiving Chemo/hormonal therapy No routine prophylaxis Gr 1C Central Venous Catheters No prophylaxis with LMWH or Warfarin Gr 1B

120
Cancer and VTE Treatment of VTE

121
Challenges of Treatment of Cancer-associated VTE
Risk of Recurrence of VTE Risk of Bleeding on Anticoagulants Negative impact on Quality of Life Mortality

122
Recurrent VTE and Bleeding
Symptomatic DVT - Prospective Follow-up 1 yr No Cancer Cancer Hazard Ratio p No Rec VTE % % Major Bleed 4.9% % Prandoni - Blood (2002)
")
123
Oral Anticoagulant Therapy
Recurrent VTE on Oral Anticoagulant Therapy 30 Hazard ratio 3.2 Cancer (21%) 20 Cumulative Proportion (%) Recurrent Thromboembolism 10 No Cancer (7%) 181 661 1 160 631 2 3 129 602 4 5 6 92 161 7 8 9 73 120 10 11 12 64 115 Time (months) Cancer No Cancer Prandoni - Blood 2002;100:3484
 20. Cumulative Proportion (%) Recurrent Thromboembolism. 10. No Cancer (7%) Time (months) Cancer. No Cancer. Prandoni - Blood 2002;100:3484.")
124
Anticoagulant Therapy of VTE Cumulative Proportion (%) Major Bleeding
Major Bleeding During Anticoagulant Therapy of VTE 30 Hazard ratio 2.2 20 Cancer (12%) Cumulative Proportion (%) Major Bleeding 10 No Cancer (5%) 181 661 1 170 636 2 3 141 615 4 5 6 102 170 7 8 9 81 127 10 11 12 68 124 Time (months) Cancer No Cancer Prandoni - Blood 2002;100:3484
 Cumulative Proportion (%) Major Bleeding. 10. No Cancer (5%) Time (months) Cancer. No Cancer. Prandoni - Blood 2002;100:3484.")
125
Long-term Anticoagulation - Cancer Pts
Warfarin is problematic: failure rates - recurrent thrombosis 3x - bleeding 2x difficult to maintain therapeutic range Repeated INRs / poor venous access Repeated interruptions for procedures and thrombocytopenia

126
Traditional anticoagulation for venous thromboembolism
in cancer patients is neither effective nor safe.

127
Advantages of LMWH over OAC
routine laboratory monitoring not needed weight-adjusted dosing few drug interactions Can easily accommodate invasive procedures and thrombocytopenia effective in patients with warfarin failure So given the limitations of warfarin, clinicians started using LMWH for long-term treatment when it became available for outpatient treatment. Compared to warfarin therapy, LMWHs do not require routine laboratory monitoring, is given based on body weight, is much more flexible in accommodating invasive procedures and thrombocytopenia. And lastly, anecdotal experience told us that LMWHs are effective in treating patients who developed recurrent thrombosis while on warfarin therapy.

128
Randomized trial of long-term LMWH vs. oral anticoagulants
CLOT in Cancer Trial Randomized trial of long-term LMWH vs. oral anticoagulants in Cancer patients with Acute VTE Lee et al - NEJM 2003;349:146

129
Clot in Cancer: Study Design
Initial Long-term treatment treatment dalteparin oral anticoagulant 200 U/kg QD INR 2-3 Active cancer with DVT/PE R dalteparin dalteparin 200 U/kg QD U/kg QD x 1 mo then 150 U/kg QD x 5 mos Lee - NEJM 2003;349:146

130
CLOT in Cancer Study: Events
LMWH N=336 OAC P-value* Recurrent VTE 9% 17% 0.002 Major bleed 6% 4% 0.27 While on study treatment, a total of 31 patients experienced a major bleeding event, 19 were in the LMWH group and 12 were in the OAC group. Overall, there was more bleeding in the OAC group, with 62 patients having any bleeding compared to 46 in the LMWH group. However, the differences in major and any bleeding between the 2 treatment groups were not statistically significant. Reasons related to major bleeds: LMWH OAC Platelet < Elevated INR 4 (1.4, 1.4, 1.5, 1.7) 6 (4.5, 4.6, 5.9, 6.9, 6.9, 12.0) Other reasons 15 6 PD 2 to bleed 9/19 6/12 Lee - NEJM 2003;349:146
 6 (4.5, 4.6, 5.9, 6.9, 6.9, 12.0) Other reasons PD 2 to bleed 9/19 6/12. Lee - NEJM 2003;349:146.")
131
Clot in Cancer: Recurrent VTE
5 10 15 20 25 Days Post Randomization 30 60 90 120 150 180 210 Probability of Recurrent VTE, % risk reduction = 52% P-value = 0.002 dalteparin OAC This graph shows the Kaplan Meier estimates of the probability of recurrent thrombosis over time. As you can see, over the 6-month study period, the risk reduction in recurrent VTE was 52% in favour of dalteparin. This difference was highly statistically significant with a p-value of Up to 6 months, the probability of recurrent thrombosis was reduced from 17.4% in the OAC group to 8.8% in the LMWH group. Hazard ratio 0.48 (0.30 – 0.77). Combined endpoint of VTE+MB, HR is 0.61, 39% risk reduction. Lee - NEJM 2003;349:146
. Combined endpoint of VTE+MB, HR is 0.61, 39% risk reduction. Lee - NEJM 2003;349:146.")
132
Treatment of VTE in Oncology
Randomized trials (LMWH vs warfarin) CANTHANOX (enoxaparin) – Meyer 2002 CLOT (dalteparin) – A Lee et al 2003 Subgroup of LITE (tinzaparin) – Hull et al 2006 ONCENOX (enoxaparin) – Deitcher 2006 Cohort study (LMWH) Monreal - et al (dalteparin) To-date, 3 RCTs have studied the efficacy and safety of long-term treatment with LMWH specifically in patients with cancer. The first 2 studies have been published and the two latter studies are small or subgroup results that have been presented in abstract form only. I am going to review the results from the two published studies.
 CANTHANOX (enoxaparin) – Meyer CLOT (dalteparin) – A Lee et al Subgroup of LITE (tinzaparin) – Hull et al ONCENOX (enoxaparin) – Deitcher Cohort study (LMWH) Monreal - et al (dalteparin) To-date, 3 RCTs have studied the efficacy and safety of long-term treatment with LMWH specifically in patients with cancer. The first 2 studies have been published and the two latter studies are small or subgroup results that have been presented in abstract form only. I am going to review the results from the two published studies.")
133
LMWH for VTE in Cancer Patients
Canthenox stopped - poor accrual Warfarin LMWH Study pts pts pts Recurrent VTE 4% % NS Major Bleed % % p=.09 1. Enoxaparin x 3 months Meyer – Arch Intern Med 2002;162:1729

134
LMWH for VTE in Cancer Patients
Warfarin LMWH RR p CLOT Recurrent VTE % % 52% <.002 Major bleed % % LITE Recurrent VTE % % % Major Bleed % % 2. Dalteparin x 6 months 3. Tinzaparin x 3 months Lee – NEJM 2003;349:146 Hull – Am J Med 2006;1062

135
LMWH for VTE in Cancer Patients
Summary of Treatment Studies for CAT 1029 pts: CANTHENOX / CLOT / LITE Risk Reduction - VTE Risk Reduction - Major Bleeding Risk Reduction - Mortality Chest. 133; 6:June 2008 suppl 493S

136
Treatment of Cancer Associated Thrombosis
Cochrane Meta-analysis 2008 – Akl 11 RCTs Initial Rx of VTE: LMWH vs IV UFH Cancer pts with LMWH Mortality Reduction Relative Risk = .71 Cochrane Review Akl 6 RCTs Long term Rx of VTE in Cancer LMWH vs VKAs Bleeding RR = Survival RR = .96 Reduction VTE recurrence - LMWH RR = .47

137
Treatment of Recurrent VTE Failure of Anticoagulants
Cancer and VTE Treatment of Recurrent VTE Failure of Anticoagulants

138
Cancer and Recurrent VTE Failure of Anticoagulation
Cancer Pts 4-6 x risk of VTE 3x risk of recurrent VTE on VKAs 3-6x risk of major bleed on VKAs CLOT study 9-17% recurrence on LMWH/VKAs IVC filters 32% VTE recurrence rate

139
Cancer and Recurrent VTE
Dose escalation of LMWH study - Carrier and Lee Retrosp. Cohort: Ca pts recurrent VTE on LMWH or VKAs Management - Anticoagulant escalation: VKA Therapeutic LMWH x 4wks Maintenance LMWH (75%) Low dose LMWH Therapeutic LMWH for 4wks Maintenance LMWH Maintenance LMWH Therapeutic LMWH > 6-12 wks Therapeutic LMWH 20-25% increase wt-adj dose > 4 wks Carrier M , Lee A. J Thromb Haemost 2009; 7: 760-5
 Low dose LMWH Therapeutic LMWH for 4wks. Maintenance LMWH. Maintenance LMWH Therapeutic LMWH > 6-12 wks. Therapeutic LMWH 20-25% increase wt-adj dose > 4 wks. Carrier M , Lee A. J Thromb Haemost 2009; 7:")
140
Cancer and Recurrent VTE
Dose escalation of LMWH study - Carrier and Lee Baseline Results: 70 Cancer pts with Recurrent VTE Most common – lung, Met. Ca - 63% Initial VTE: 56% leg DVT, 17% arm DVT (5 of 12 CVC related) 20% PE 7% DVT+ PE Initial Anticoag. 67% LMWH: Th -32%, Mn - 51%, LD-17% 33% VKAs: 48% INR>2, 30% INR <2 ***No anti-FXa levels at time of recurrence Carrier M , Lee A. J Thromb Haemost 2009; 7: 760-5
 20% PE 7% DVT+ PE. Initial Anticoag. 67% LMWH: Th -32%, Mn - 51%, LD-17% 33% VKAs: 48% INR>2, 30% INR <2. ***No anti-FXa levels at time of recurrence. Carrier M , Lee A. J Thromb Haemost 2009; 7:")
141
Cancer and Recurrent VTE
Dose escalation of LMWH study - Carrier and Lee Study Results: 70 Recurrent VTE - 57% Leg DVT - 19% arm DVT (5/13 – CVC) - 21% PE - 3% IVC 67% of recurrent VTE at new site 29% in the first 4 weeks of Rx (median 3.5 months) Dose escalation: pts Therapeutic LMWH 15 pts 120% Therapeutic LMWH Carrier M , Lee A. J Thromb Haemost 2009; 7: 760-5
 - 21% PE. - 3% IVC. 67% of recurrent VTE at new site. 29% in the first 4 weeks of Rx (median 3.5 months) Dose escalation: 55 pts Therapeutic LMWH. 15 pts 120% Therapeutic LMWH. Carrier M , Lee A. J Thromb Haemost 2009; 7:")
142
Cancer and Recurrent VTE
Dose escalation of LMWH study - Carrier and Lee Results: Follow-up 3+ months 6 pts(8.6%) had second recurrence: 3 pts on therap LMWH 3 pts on 120% LMWH 5 of 6 had metastatic disease, 4 of 6 – Lung Ca All 6 treated by increasing LMWH dose by 20-25% no further symptomatic VTE during 3 month follow-up Carrier M , Lee A. J Thromb Haemost 2009; 7: 760-5
 had second recurrence: 3 pts on therap LMWH. 3 pts on 120% LMWH. 5 of 6 had metastatic disease, 4 of 6 – Lung Ca. All 6 treated by increasing LMWH dose by 20-25% no further symptomatic VTE during 3 month follow-up. Carrier M , Lee A. J Thromb Haemost 2009; 7:")
143
Cancer and Recurrent VTE
Dose escalation of LMWH study - Carrier and Lee Results: Follow-up 3+ months Recurrent VTE Event rate - 9.9%/yr Bleeding - 3 pts:1 ICH (brain Ca), 2 minor 4.8%/yr Median time to second recurrence: 1.9 months Median time - first recurrence to death: 11.4 months Median survival after second recurrence: 4.3 months
, 2 minor 4.8%/yr. Median time to second recurrence: 1.9 months. Median time - first recurrence to death: 11.4 months. Median survival after second recurrence: 4.3 months.")
144
Cancer and Recurrent VTE
Dose Escalation of LMWH Study - Carrier and Lee Summary: Cancer pts with recurrent VTE poor prognosis - Median survival 11.4 months 4.3 months if second recurrence Escalating LMWH dose effective in treating Ca pts with “resistance” to standard LMWH or VKAs

146
Central Catheter Thrombosis
Treatment

147
If Catheter not required (no Anticoag. Contraindications)
NCCN Practice Guidelines Catheter Associated Thrombosis: If Catheter not required (no Anticoag. Contraindications) Remove catheter when clinically appropriate Anticoagulate Recommended duration of therapy - at least 3 months Massive catheter related DVT consider thrombolysis
 Remove catheter when clinically appropriate. Anticoagulate. Recommended duration of therapy - at least 3 months. Massive catheter related DVT consider thrombolysis.")
148
NCCN Practice Guidelines
Catheter Associated Thrombosis: If Catheter still required (no Anticoag. contraindications) Anticoagulate as long as catheter in place Recommended duration of therapy - at least 3 months Consider catheter removal if symptoms persists Massive catheter related DVT consider thrombolysis
 Anticoagulate as long as catheter in place. Recommended duration of therapy - at least 3 months. Consider catheter removal if symptoms persists. Massive catheter related DVT consider thrombolysis.")
149
Cancer and VTE Selected references
Lyman, Khorana et al. JCO 2009; 29: (Oct 10, 2009) NCCN Practice Guidelines 2010 Lyman et al. JCO 2007; 25: Ay et al. Blood 2010; 116: Khorana et al. Blood 2008; 111:
 NCCN Practice Guidelines Lyman et al. JCO 2007; 25: Ay et al. Blood 2010; 116: Khorana et al. Blood 2008; 111:")
150
THANK YOU

Similar presentations




 Kingsbrook Jewish Medical Center Clinical Instructor of Pharmacy Practice.>")

















