Download presentation
Presentation is loading. Please wait.

1
Dr. Sham Sunder

2
Kidney damage for >= 3months, as defined by structural / functional abnormalities of kidney with or without decreased GFR, and manifest by either : Pathologic abnormalities Markers of kidney damage, including abnormalities in composition of blood / urine or abnormalities on imaging GFR =3 months, with / without kidney damage

3
By Radiology – USG / CT / MRI etc… By Histology – Renal Biopsy

4
Microalbuminuria Proteinuria Hematuria esp associated with proteinuria Casts ( with cellular elements )
")
5
Cockcroft-Gault formula C cr (ml/min) = (140-age) x weight *0.85 if female 72 x S cr MDRD Study equation GFR (ml/min/1.73 m 2 ) = 186 x (S cr ) -1.154 x (age) -.203 x (0.742 if female) x (1.210 if African American)
 = (140-age) x weight *0.85 if female 72 x S cr MDRD Study equation GFR (ml/min/1.73 m 2 ) = 186 x (S cr ) x (age) x (0.742 if female) x (1.210 if African American)")
6
STAGEDESCRIPTIONGFR ( ml/min/1.73m2 ) 1Kidney damage with normal / increased GFR >=90 2Kidney damage with mildly decreased GFR 60 – 89 3Moderately decreased GFR30 – 59 4Severely decreased GFR15 – 29 5Kidney failure< 15 / dialysis
 1Kidney damage with normal / increased GFR >=90 2Kidney damage with mildly decreased GFR 60 – 89 3Moderately decreased GFR30 – 59 4Severely decreased GFR15 – 29 5Kidney failure< 15 / dialysis")
7
STAGEACTION PLAN 1DIAGNOSIS AND TREATMENT SLOW PROGRESSION 2ESTIMATE PROGRESSION 3EVALUATE AND TREAT COMPLICATIONS 4PREPARE FOR RENAL REPLACEMENT THERAPY 5RENAL REPLACEMENT

8
Diagnosis Measures to slow progression Estimate Progression Evaluation and Treatment of Complications Preparation for Renal Replacement Therapy

9
History Physical Examination

10
CLINICAL FACTORSSOCIODEMOGRAPHIC FACTORS DIABETES MELLITUSOLDER AGE HYPERTENSIONEXPOSURE TO CERTAIN CHEMICALS / ENVIRONMENTAL CONDITIONS AUTOIMMUNE DISEASESLOW INCOME / EDUCATION SYSTEMIC INFECTIONS URINARY TRACT INFECTIONS URINARY STONES LOWER URINARY TRACT OBSTRUCTION NEOPLASIA FAMILY HISTORY OF CKD RECOVERY FROM AKI REDUCTION IN KIDNEY MASS DRUGS LOW BIRTH WEIGHT

11
Tests & DiagnosticsSignificance / Goal Blood Pressure< 130 / 80 mm Hg ; Use ACEI /ARB Serum CreatinineTo estimate GFR; Historical values assist in determining acuity and progression of disease Urinalysis with microscopyPresence of RBCs / RBC casts and or Proteinuria – further work up Serum Electrolytes ( Na+, K+ )Useful as crude surrogate of renal disease Help to guide antihypertensives Help to identify patients in need of medical nutrition education Calcium, Phosphorus, PTH, ALP, 25-OH VITAMIN D Assists in treatment of metabolic bone disease Complete Blood Count Peripheral Blood Smear Evaluate for anemia TSAT, S.FerritinUseful in evaluation of iron stores
Useful as crude surrogate of renal disease Help to guide antihypertensives Help to identify patients in need of medical nutrition education Calcium, Phosphorus, PTH, ALP, 25-OH VITAMIN D Assists in treatment of metabolic bone disease Complete Blood Count Peripheral Blood Smear Evaluate for anemia TSAT, S.FerritinUseful in evaluation of iron stores")
12
Tests & DiagnosticsSignificance / Goals Renal Ultrasound with or without Arterial Doppler Characterize Kidney number and size Echogenicity of kidneys Rule out presence of obstruction Rule out renovascular disease Cholesterol panelEspecially useful for patients with nephrotic range proteinuria Random urine protein Random urine creatinine Ratio approximate values obtained by 24 hour collection Hepatitis SerologyNegative Hep B testing mandates vaccination Serum Protein Electrophoresis Urine Protein Electrophoresis In adults with renal disease to rule out Myeloma Antinuclear antibodyWarranted for adults with proteinuria / evidence for SLE HIVWarranted in selected population Renal BiopsyIndicated in pts with hematuria and / proteinuria and lack of evidence of systemic disease

14
Protein Restriction Reducing Intraglomerular Hypertension Reducing Proteinuria Control of Blood Glucose Control of Blood Pressure

15
Reduces symptoms associated with uremia Slows the rate of decline in renal function at earlier stages of renal diseases K/DOQI clinical practice guidelines recommend daily protein intake between 0.60 – 0.75 g / Kg per day 50 % of protein intake should be of high biological value As patient approaches CKD Stage V, spontaneous protein intake decreases & patient enter a state of Protein – Energy Malnutrition. Recommended protein intake is 0.9 g / Kg per day

16
Increased intraglomerular filtration pressure & glomerular hypertrophy - a response to loss of nephron number It promotes ongoing decline of kidney function even if the inciting process has been treated. ACEI & ARBs Inhibit angiotensin induced vasoconstriction of efferent arteriole Reduces intraglomerular filtration pressure and proteinuria

17
If monotherapy is not effective, combined therapy with both ACEI & ARB can be tried 2 nd line drugs : Calcium Channel Blockers Diltiazem, Verapamil Especially - Diabetic Nephropathy & Glomerular diseases

18
Leading cause of Chronic Kidney Disease Control of Blood Glucose : excellent glycemic control reduces the risk of kidney disease & its progression in both Type 1 & 2 Diabetes Mellitus Recommendations : FBS : 90 – 130 mg/dl HbA1C < 7% Control of Blood Pressure & Proteinuria : ACEI & ARBs

19
Hypertension : sodium and water retention renin angiotensin system activation Control of BP : to slow progression of CKD to prevent extrarenal complications ( cardiovascular disease / stroke ) Goal : BP < 130 / 80 mm Hg BP 1g/day )
 Goal : BP < 130 / 80 mm Hg BP 1g/day )")
20
Salt Restriction Diuretics Loop Diuretics : Furosemide 40 mg BD Bumetanide 1mg BD Thiazides : less efficacious gfr < 30 – 40 ml/min Both ameliorate hyperkalemia seen with ACEI / ARB ACEI / ARB Check S.Creat & S.K+ within 1 -2 weeks Upto 30 % increase in creatinine is acceptable Beta blockers / CCB / Alpha blockers / Vasodilators

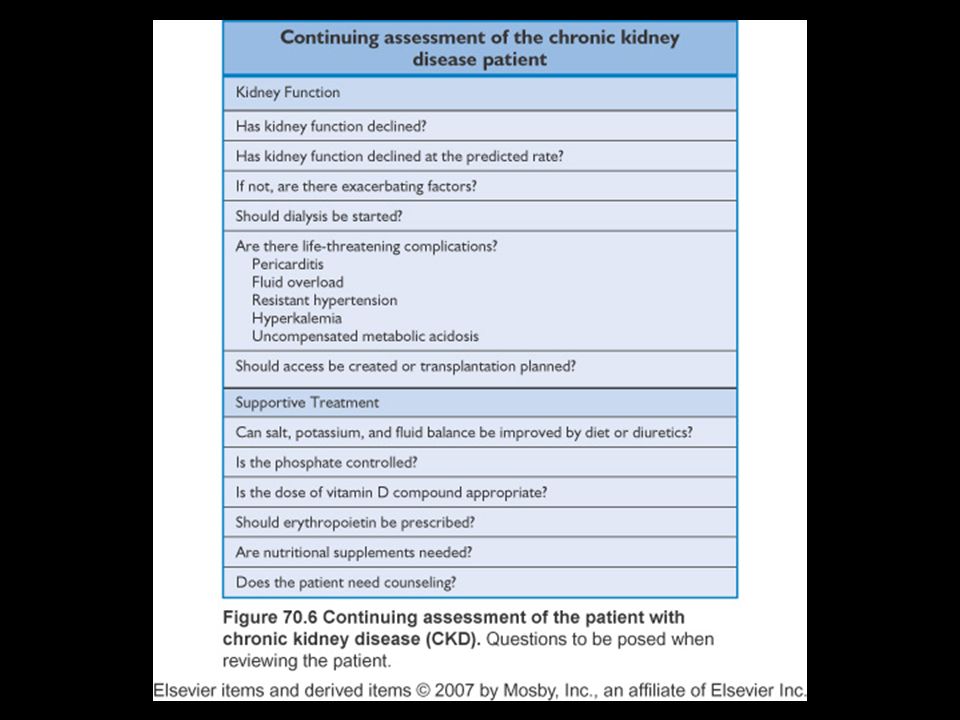
24
Anemia Bone Disorders Dyslipidemia Cardiovascular disease

25
Defined as Hemoglobin < 13.5 g/dl in males < 12 g/dl in females Normocytic normochromic anemia – as early as in Stage III CKD or universally by Stage IV CKD Primary cause : insufficient production of Erythropoetin Additional factors : iron deficiency folate / vit B12 deficiency chronic inflammation hyperparathyroidism / bm fibrosis

26
Target Hb : 11 g/dl Target Iron status : TSAT : lower limit > = 20 S.Ferritin : ng/ml lower limit : 200 – HD CKD 100 – Non HD CKD > 500 not routinely recommended Check Hb monthly while on ESAs Iron studies monthly when started on ESA On stable ESA Therapy : Iron studies can be done 3 monthly

27
Ferrous sulphate 325 mg bid – tid IV Iron Dextran IV Iron Sucrose IV Sodium Ferric Gluconate Complex Folic acid and Vitamin B 12 supplements Erythropoetin Stimulating Agents : Epoetin alfa Epoetin beta Darbepoetin alfa Epoetin alfa / beta : 50 -100 IU / Kg SC per week Darbepoetin alfa : 40 mcg SC every 2 weeks

28
Osteitis Fibrosa Cystica Osteomalacia Adynamic bone disease Mixed osteodystrophy Secondary Hyperparathyroidism Vitamin D deficiency Acidosis Aluminium accumulation Osteoporosis in elderly Osteopenia caused by steroids

29
Renal bone disease – significantly increase mortality in CKD patients Hyperphosphatemia – one of the most important risk factors associated with cardiovascular disease in CKD patients

30
K/DOQI recommends : CKD Stage III & IV : S.Phosphorus : 2.7 - 4.6 mg / dl CKD Stage V : S.Phosphorus : 3.5 - 5.5 mg / dl CKD STAGEGFR RANGEINTACT PTH ( pg/ml ) 330 – 5935 – 70 415 – 2970 – 110 5< 15 / Dialysis150 – 300
 330 – 5935 – – 2970 – 110 5< 15 / Dialysis150 – 300")
31
CKD STAGEGFR RANGEPTH LEVELSS.Calcium & S.Phosphorus 330 -59Every 12 months 415-29Every 3 months 5< 15 / dialysisEvery 3 monthsEvery month

32
Reduce dietary phosphate intake Phosphate binders : calcium carbonate calcium acetate aluminium hydroxide magnesium carbonate ( rarely used ) sevelamer hydrochloride lanthanum carbonate The use of calcium salts is limited by development of hypercalcemia Calcium acetate poses a less problem as less calcium is absorbed
 sevelamer hydrochloride lanthanum carbonate The use of calcium salts is limited by development of hypercalcemia Calcium acetate poses a less problem as less calcium is absorbed")
33
Calcimimetics – Cinacalcit : Agent that increase calcium sensitivity of the calcium sensing receptor expressed by parathyroid gland Down regulating the parathyroid hormone secretion Reduce hyperplasia of parathyroid gland Calcitriol 0.25 mcg OD Paricalcitol 1 mcg daily or 2mcg 3 times a week

34
Vitamin D deficiency : < 5 ng/ml – Ergocalciferol 50000 IU orally weekly for 12 weeks and then monthly thereafter 5 – 15 ng/ml – Ergocalciferol 50000 IU orally weekly for 4 weeks and then monthly thereafter 16 – 30 ng/ml – Monthly Ergocalciferol Acidosis : K/DOQI – total Co2 >=22 mEq/L Sodium bicarbonate 650 – 1300 mg bid – tid

35
A major risk factor for cardiovascular morbidity & mortality Prevalence of hyperlipidemia increases as renal functions diminish All patients with CKD must be evaluated for Dyslipidemia Fasting lipid profile – annually

36
Stage V CKD patients with dyslipidemia should always be evaluated for secondary causes : Nephrotic syndrome Hypothyroidism Diabetes mellitus Excessive alcohol consumption Liver disease Drugs : oral contraceptives, haart etc… Goal : LDL – Cholesterol < 100 mg / dl

37
LDL : 100 – 129 mg/dl : Lifestyle changes Not responded : Low dose statin LDL >= 130 mg/dl : Lifestyle changes + Statins TG >= 200 mg/dl : Lifestyle changes + Statins

39
Control BP : ACEI / ARB Treat dyslipidemia : Lifestyle changes + Statins Good Glycemic control Treat anemia Correct hyperphosphatemia Treat hyperparathyroidism Correct hyperkalemia

40
Hepatitis B vaccination : 3 doses (0,1,2 months ) higher dose ( 40 mcg / ml ) Pneumococcal vaccination : single dose one time revaccination 5 yrs after initial vaccination Influenza vaccination : recommended annually for adults > 50 yrs age
 higher dose ( 40 mcg / ml ) Pneumococcal vaccination : single dose one time revaccination 5 yrs after initial vaccination Influenza vaccination : recommended annually for adults > 50 yrs age")
41
Patients of CKD Stage IV approaching Stage V should be referred for Vascular access if hemodialysis is preferred Peritoneal dialysis catheter placement if peritoneal dialysis is preferred AVF is most preferred access for HD patients Ideally created 6 months prior to start of HD Non dominant upper extremity And that arm is to be preserved – no iv lines AVG : 3-6 weeks prior to start of HD PD Catheter : 2 weeks prior to start of HD

44
GFR not below 15 ml/min.1.73m2 but in presence of Intractable volume overload Hyperkalemia Hyperphosphatemia Hypercalcemia / Hypocalcemia Metabolic acidosis Anemia Uremic encephalopathy Uremic pericarditis Severe hypertension, acute pulmonary edema

Similar presentations







activate vitamin D (renal 1-alpha hydroxylase) produces erythropoietin.>")








>")






