Download presentation
Presentation is loading. Please wait.

1
Can we use multigene-tests to guide the adjuvant treatment of early breast cancer? R5 陳三奇 VS 趙大中 J Natl Compr Canc Netw 2013;11:174-182 J

2
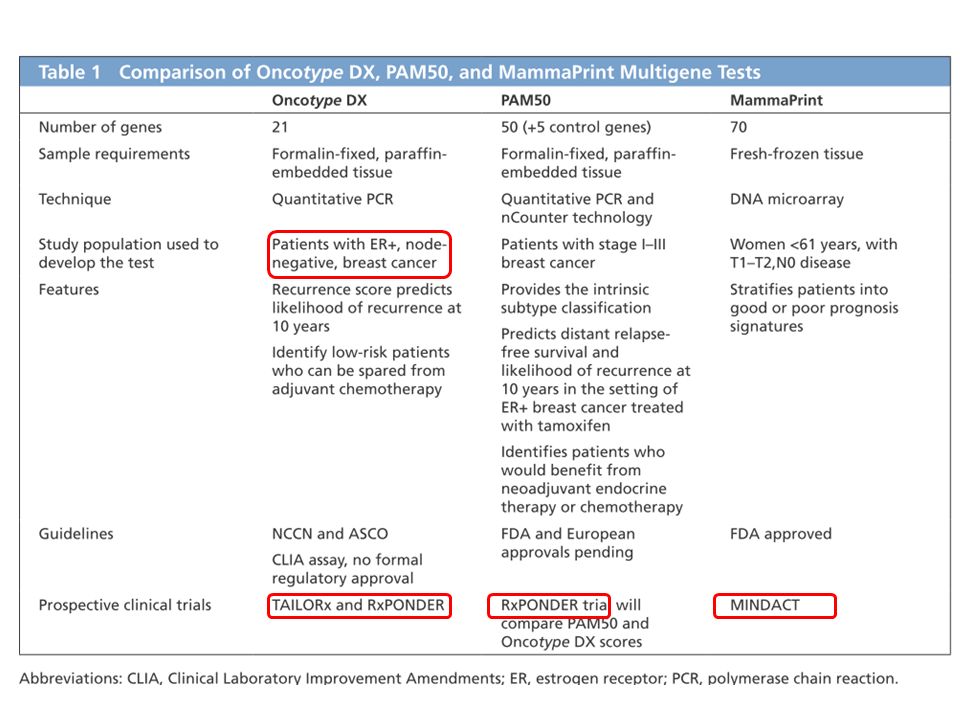
Breast cancer – A heterogeneous disease – Outcome predict by clinical and pathologic features. – Genomic tests since 2002 Oncotype DX, PAM50, and MammaPrint. Others: Rotterdam 76-gene signature, 3-gene SCMGENE panel – The role of these multigene tests ?

3
NSABP B-14 、 B-20 trial 10 years follow up Early breast cancer with ER(+) and LN (-) NSABP B-14 trial (National Surgical Adjuvant Breast and Bowel Project clinical trial B-14. ) – Randomly assigned to placebo (n=1453) or tamoxifen (n=1439) – Recurrent free survival :hazard ratio 0·58 (95% CI 0·50–0·67, p<0·0001) – Overall survival: HR 0·80, (95% CI 0·71–0·91, p=0·0008) NSABP B-20 trial – Randomly assigned to tamoxifen (n=788) or cyclophosphamide, methotrexate, fluorouracil, and tamoxifen (CMFT, n=789) – Rcurrence-free survival 0·52 ( 0·39–0·68,p<0·0001) – Overall survival 0·78, (0·60–1·01, p=0·063) Fisher et al. Lancet 2004; 364: 858–68
 – Randomly assigned to placebo (n=1453) or tamoxifen (n=1439) – Recurrent free survival :hazard ratio 0·58 (95% CI 0·50–0·67, p<0·0001) – Overall survival: HR 0·80, (95% CI 0·71–0·91, p=0·0008) NSABP B-20 trial – Randomly assigned to tamoxifen (n=788) or cyclophosphamide, methotrexate, fluorouracil, and tamoxifen (CMFT, n=789) – Rcurrence-free survival 0·52 ( 0·39–0·68,p<0·0001) – Overall survival 0·78, (0·60–1·01, p=0·063) Fisher et al. Lancet 2004; 364: 858–68.")
4
NSABP B-14NSABP B-20 Fisher et al. Lancet 2004; 364: 858–68

5
CMFT Placebo Tamo Fisher et al. Lancet 2004; 364: 858–68

6
Conclusions of NSABP B-14 and B-20 trial 10 years follow up: – 1. Tamoxifen has much benefit in ER(+) and LN (-) patients. – 2. Older women tend to have higher tumor oestrogen-receptor concentrations and are more likely to benefit from tamoxifen than from chemotherapy; in younger women, the converse is true CMFT Tamo Placebo Fisher et al. Lancet 2004; 364: 858–68
 and LN (-) patients. – 2. Older women tend to have higher tumor oestrogen-receptor concentrations and are more likely to benefit from tamoxifen than from chemotherapy; in younger women, the converse is true CMFT Tamo Placebo Fisher et al. Lancet 2004; 364: 858–68.")
7
Oncotype DX Oncotype DX score: – Quantitative reverse transcriptase polymerase chain reaction (RT-PCR) – measures 21 genes in formalin-fixed paraffin- embedded breast tumors.
 – measures 21 genes in formalin-fixed paraffin- embedded breast tumors.")
8
Oncotype DX to Predict Recurrence of Tamoxifen-Treated, Node-Negative Breast Cancer Retrospective analysis of 668 tumor blocks in NSABP –B14 trial – ER (+), LN (-), Tamoxifen- treated Paik et al. N Engl J Med 2004;351:2817-26 Low v.s. high-risk groups (6.8% vs. 30.5; P<.001)
.")
9
Conclusion of Oncotype DX for NSABP B-14 trial: – The RS quantified the likelihood of distant recurrence in tamoxifen-treated patients with ER(+), LN(-) breast cancer. Paik et al. N Engl J Med 2004;351:2817-26

10
Oncotype DX to Predict Death of Node-Negative Breast Cancer A case-control study – N= 4969 – Node-negative, EBC from 1985 to 1994, not treated with adjuvant chemotherapy. – 220 patients died from breast cancer. Treated with tamoxifen, the death rate was – Low risk: 2.8 % – Intermediate risk: 10.7% – High risk :15% (P=.003). Not treated with Tamoxifen for ER(+) patients, the death rate was – Low risk: 6.2%. – Intermediate risk: 17.8% – High risk :19.9% Conclusion: – The RS strongly associated with risk of breast cancer death among ER- positive, tamoxifen-treated and untreated patients. Habel et al. Breast Cancer Research 2006, 8:25
. Not treated with Tamoxifen for ER(+) patients, the death rate was – Low risk: 6.2%. – Intermediate risk: 17.8% – High risk :19.9% Conclusion: – The RS strongly associated with risk of breast cancer death among ER- positive, tamoxifen-treated and untreated patients. Habel et al. Breast Cancer Research 2006, 8:25.")
11
The 21-gene recurrence score (RS) assay – quantifies the likelihood of distant recurrence in women with ER (+), LN (-), treated with adjuvant Tamoxifen. – Strongly related to cancer death in ER (+), LN (-), treated with or without Tamoxifen. Suggest that – combining Recurrence Score, tumor grade, and tumor size provides better risk classification than any one of these factors alone. However, the relationship between the RS and chemotherapy benefit is not known.
, LN (-), treated with or without Tamoxifen. Suggest that – combining Recurrence Score, tumor grade, and tumor size provides better risk classification than any one of these factors alone. However, the relationship between the RS and chemotherapy benefit is not known..")
12
Oncotype DX to Predict Recurrence of Tamo or CMF-treated,LN(-), ER (+) Breast Cancer Retrospective analysis of the RS in – NSABP B-20 – LN (-), ER (+), – Treated with tamoxifen or Tamoxifen plus chemotherapy (CMF-T) Paik et al. J Clin Oncol 2006,24:3726-3734. Low risk Int. risk High risk

13
Conclusions: – High risk patients experienced a significant benefit from chemotherapy, whereas low risk patients had no benefit. Paik et al. J Clin Oncol 2006,24:3726-3734.

14
Oncotype DX to Predict DFS and OS of postmenopausal, ER(+), LN(+) treated with CT SWOG-8814, INT-0100 – Postmenopausal women, ER (+), LN (+) – Randomized into 3 group for adjuvant therapy : Tamoxifen CAF-T (cyclophosphamide, doxorubicin, and fluorouracil x 6 cycles, Tamoxifen for 5 years) CAFT Results: – CAF-T or CAFT was superior to Tamoxifen for DFS, and marginally for OS. – Adjusted HRs favoured CAF-T over CAFT. KS el tl.Lancet. 2009 Dec 19;374(9707):2055-63
:")
15
Retrospective analysis the recurrence score on DFS by treatment group (tamoxifen vs CAF-T) N= 367 specimens, tamoxifen, n=148; CAF-T, n=219. Albain et al. Lancet Oncol 2010; 11: 55–65 Tamoxifen alone Oncotype DX to Predict DFS and OS of postmenopausal, ER(+), LN(+) treated with CT
, LN(+) treated with CT.")
16
Low risk group Int. risk groupHigh risk group All patients Disease free survival Albain et al. Lancet Oncol 2010; 11: 55–65

17
Low risk group Int. risk group High risk group Overall survival Albain et al. Lancet Oncol 2010; 11: 55–65 Conclusion: – High RS, LN (+), ER(+) benefit from addition of CAF to Tamoxifen in free survival (HR, 0.59; log rank P=.033) with the addition of CAF – Low RS did not benefit from adjuvant chemotherapy, despite positive node.
, ER(+) benefit from addition of CAF to Tamoxifen in free survival (HR, 0.59; log rank P=.033) with the addition of CAF – Low RS did not benefit from adjuvant chemotherapy, despite positive node..")
18
The use of Oncotype DX may identify – LN(-), ER (+) EBC with high risk of recurrence. – LN(+), ER (+) EBC with low risk of recurrence may not have benefit from chemotherapy. NCCN guideline
, ER (+) EBC with low risk of recurrence may not have benefit from chemotherapy. NCCN guideline.")
19
TAILORx trial: – 11,000 patients with ER+, HER2–, node-negative breast cancer. – RS: Arm A: 25 – Trial enrollment completed in 2010 and trial results are not yet available. RxPONDER trial (SWOG S1007) January 2011 – ER+, HER2– breast cancer with 1 to 3 positive nodes (N1) – Enroll 4000 women with an RS of 25 or less, 2000 patients per arm planned – The primary effect of chemotherapy on LN(+) breast cancer who have an RS of 25 or less. – Secondary objectives comparison of Oncotype DX and PAM50 risk of relapse (ROR) scores
 January 2011 – ER+, HER2– breast cancer with 1 to 3 positive nodes (N1) – Enroll 4000 women with an RS of 25 or less, 2000 patients per arm planned – The primary effect of chemotherapy on LN(+) breast cancer who have an RS of 25 or less. – Secondary objectives comparison of Oncotype DX and PAM50 risk of relapse (ROR) scores.")
20
Prospective Clinical Trials of Oncotype DX:TAILORx and RxPONDER

21
PAM50 ROR score

22
Use RT-qPCT to categorizes tumors into the 4 intrinsic subtypes – luminal A – luminal B – HER2-enriched – basal-like ROR score to estimate the probability of relapse at 5 years. Parker el al. J Clin Oncol 27:1160-1167

23
Tamoxifen-treated, early- stage, ER+ breast cancer, DSS= disease specific survival Samuel Leung et al. Clin cancer research 2010;16:5222

24
NCIC MA12 trial – Predict the benefit of tamoxifen in premenopausal women in the, whereas ER status alone had limited value. Dongsheng Tu et al.Clin Cancer Res 2012;18:4465-4472. IHC status PAM50

25
TransATAC analysis – Good agreement between PAM50 ROR and Oncotype DX – PAM50 ROR score provided more prognostic information about 10-year distant recurrence than Oncotype DX – More patients assigned to the low-risk category by PAM50. half of the patients in the intermediate-risk Oncotype DX group were classified into the low-risk PAM50 luminal A category. RxPONDER trial Dowsett et al 2011 Cancer research

26
MammaPrint and the MINDACT Prospective Clinical Trial

27
MammaPrint Using DNA microarrays, a 70-gene prognostic signature, MammaPrint, for node- negative breast cancer was developed in 2002. (2002 Nature) – low- or high-risk for distant metastases at 5 years. – MammaPrint outperformed standard clinical and histologic predictors of patient prognosis. – approved by the FDA in 2007 for node-negative patients.
 – low- or high-risk for distant metastases at 5 years. – MammaPrint outperformed standard clinical and histologic predictors of patient prognosis. – approved by the FDA in 2007 for node-negative patients..")
28
The MINDACT trial (Microarray In Node-negative and 1–3 Node-Positive Disease May Avoid Chemo Therapy) – Prospective randomized phase III clinical trial – MINDACT had a predefined pilot phase in which the data and treatment decisions of the first 800 patients were analyzed, and those results were published in 2011. (2011 Eur J Can)
.")
29
The MINDACT trial

30
http://www.lifemath.net/cancer/breastcancer/therapy/

31
Chemotherapy: – anthracycline-containing regimen – or docetaxel/capecitabine. Endocrine therapy: – a switching strategy of tamoxifen for 2 years, then letrozole for 5 years, versus – letrozole for 7 years

33
Question 1: Should we use gene-predictors to define the need of adjuvant treatment?

34
MammaPrint – prognosis in untreated node-negative patients. – 29% discordance in low and high risk groups between Adjuvant! and MammaPrint 32% low risk with Adjuvant! – => high risk with MammaPrint 68% high risk with Adjuvant! – => low risk with MammaPrint – The MINDACT will address this issue

35
Question 2: Should we use gene predictors to guide treatment choice, particularly to understand if an ER- positive tumor needs chemotherapy in addition to hormone therapy?

36
NCCN suggest – Chemotherapy in case of node positivity – Oncotype DX :negative nodes with T>1 cm St. Gallen suggest – favor chemotherapy if a tumor is >5 cm or if 4+ metastatic nodes. If a tumor is between 2 and 5 cm, or if only 1-3 nodes positive? – Oncotype DX High recurrent score: predict chemotherapy benefit Low recurrent score: no evidence of benefit. Gray zone in intermediate RS – RS: 11- 25, 45% of all subjects – Ongoing TAILORx trial

37
Question 3: Can we use genomic predictors to choose the type of chemotherapy?

38
A multigene signature predictive of the activity of paclitaxel and 5-fluorouracil, doxorubicin, and cyclophosphamide (FAC), in neoadjuvant setting – Complete pathological response : more powerful predictor of treatment outcome. – multigene signature positive predictive value is modest (52%) negative predictive value is high (92%) We can probably select what not to use, but not what to use Ayers M el al. J Clin Oncol 2004;22(12):2284
 negative predictive value is high (92%) We can probably select what not to use, but not what to use Ayers M el al. J Clin Oncol 2004;22(12):2284.")
39
Question 4: Are genomic predictors ready for routine clinical practice?

40
Combining one or more gene-expression classifiers into a single model together with traditional clinico-pathological parameters hat still retain important prognostic information.

41
Future Developments: Cancer Genome Sequencing A revolution in DNA sequencing technology began in 2005. 2009–2010,Washington University School of medicine. Sequenced the patient’s normal DNA, the primary tumor DNA, and the DNA of the metastasis – identified somatic DNA changes. – significant evolution in the cancer can occur during metastatic spread

42
Luminal subtype breast cancers, a statistically significant difference (P=.02) is seen in the number of point mutations – Point mutation – black: copy number – green: interchromosome translocation – blue: intra-chromosome
 is seen in the number of point mutations – Point mutation – black: copy number – green: interchromosome translocation – blue: intra-chromosome")
43
Similarly, comparison of the genomes of basal-like, HER2- enriched, luminal A, and luminal B breast cancers, as defined by PAM50, shows that the number of translocations is much higher in basal-like and HER2- enriched cases. (2012 nature)
.")
44
The neoadjuvant AI trial, ACOSOG Z1031, were sequenced – TP53 higher preoperative endocrine prognostic index scores higher pretreatment and posttreatment proliferation indexes. – GATA3 mutations in the transcription factor associated with response to AI therapy. – MAP3K1 low pre– and post–AI treatment Ki-67 level (the opposite of p53) correlated with good-prognosis breast cancer. Genome sequencing – may identify the molecular abnormalities – identified poor risk by multigene tests – provide potential new targets for therapy
 correlated with good-prognosis breast cancer. Genome sequencing – may identify the molecular abnormalities – identified poor risk by multigene tests – provide potential new targets for therapy.")
45
Thanks for your attention~

Similar presentations






 on the Efficacy.>")
 Baselga.>")



>")







