Download presentation
Presentation is loading. Please wait.

1
Glucose Metabolism & Diabetes
How does diabetes disrupt the homeostatic levels of glucose in the blood?

2
Objectives Describe the major structures and functions of the liver and pancreas. Explain the intricacies of glucose, protein, and fat metabolism. Explain the roles of insulin and glucagon in maintaining homeostasis. Explain the processes of lipolysis, deamination glycogenolysis, and gluconeogenesis. Define the terms glycosuria, polyuria, polydipsia, and polyphagia and explain why diabetes causes these conditions. State the medical complications associated with diabetes and explain why these occur.

3
PART I LIVER & PANCREAS: STRUCTURE FUNCTION

4
THE LIVER: Structure Largest visceral organ in the body 1.5 kg (3.3 lb.), 4 lobes Sinusoids (blood vessels-similar to capillaries) between liver cells (hepatocytes) empty into the central vein
 between liver cells (hepatocytes) empty into the central vein.")
5
THE LIVER: Structure Functional unit of the liver: Liver lobule (50, ,000): cylindrical structure, several mm long 1-2 mm in diameter Central vein in center of lobule

6
THE LIVER: Structure Hepatocytes in a liver lobule form a series of irregular plates arranged like the spokes of a wheel Portal area between lobules: hepatic artery, interlobular portal vein, interlobular bile duct

7
Sinusoid with red blood cell and Kupffer cell
LIVER Blood flowing from the intestinal capillaries picks up many bacteria from the intestines. When bacterium comes into contact with a Kupffer cell (phagocytic cell: engulf pathogens, cell debris, and damaged blood cells) in less than 0.01 sec it passes inward through the cell membrane and gets lodged until it is digested. Less than 1% of incoming bacteria escapes to circulation. Sinusoid with red blood cell and Kupffer cell
 in less than 0.01 sec it passes inward through the cell membrane and gets lodged until it is. digested. Less than 1% of incoming bacteria. escapes to circulation. Sinusoid with red blood cell and Kupffer cell.")
8
HEPATIC PORTAL CIRCULATION
Blood from the spleen, pancreas, stomach & intestines enters the liver via the hepatic portal vein. Blood from the intestines is very high in glucose. Liver cells remove excess glucose, amino acids, toxins, bacteria. Blood leaves the liver by means of the hepatic vein, now with normal levels of glucose.

9
LIVER: Function Filtration and storage of blood.
Metabolism of carbohydrates, proteins, fats, and hormones. Storage of vitamins and minerals. Synthesis of plasma proteins. Synthesis and secretion of bile. PHAGOCYTE

10
Filtration of the blood

11
THE PANCREAS: Structure
The pancreas is approximately 20 cm (8 in) and weighs about 80g (3 oz) The pancreas has two major types of tissues: the acini (secrete digestive juices to duodenum) and the islets of Langerhans (secrete insulin and glucagon directly into blood) Human pancreas has 1 – 2 million islets of 0.3 mm in diameter, although the islets account for only about 1% of the pancreatic cell population
 and weighs about 80g (3 oz) The pancreas has two major types of tissues: the acini. (secrete digestive juices to duodenum) and the islets of. Langerhans (secrete insulin and glucagon directly into blood) Human pancreas has 1 – 2 million islets of 0.3 mm in diameter, although the islets account for only about 1% of the pancreatic cell population.")
12
THE PANCREAS: Structure
Ref: Islets of Langerhans contain 3 types of hormone-secreting cells Alpha cells (25%) Beta cells (60%) Delta cells (10%) F cells (PP cells) (5%) The islets are organized around small capillaries into which the cells secrete their hormones
 Beta cells (60%) Delta cells (10%) F cells (PP cells) (5%) The islets are organized around small capillaries into which the cells secrete their hormones.")
13
THE PANCREAS: Structure/Function
Alpha cells secrete glucagon elevates blood glucose concentrations Beta cells secrete insulin reduces blood glucose concentrations Delta cells secrete somatostatin- slows the rate of food absorption and digestive enzyme secretion F cells/PP cells secrete pancreatic polypeptide Close interrelation among various cell types allow regulation of secretion of some hormones by other hormones: insulin inhibits glucagon secretion, somatostatin inhibits insulin and glucagon secretion

14
PART II HOW DO THE LIVER & PANCREAS ALLOW US TO UTILIZE THE NUTRIENTS WE CONSUME?

15
Glucose: the preferred nutrient
Carbohydrates are the preferred source of energy for the body. Final products of carbohydrate digestion in the digestive tract are monosaccharides (glucose [80%], fructose and galactose) Much of fructose and all galactose are converted to glucose in the liver and released back into the blood. Glucose is a large molecule that must be broken down into a form of energy usable by the cell (ATP). health.howstuffworks.com/diabetes1.htm
 Much of fructose and all galactose are converted to glucose in the liver and released back into the blood. Glucose is a large molecule that must be broken down into a form of energy usable by the cell (ATP). health.howstuffworks.com/diabetes1.htm.")
16
A P P P Structure of ATP: Adenosine Triphosphate High-energy bonds
Phosphate groups adenosine

17
A P P P A P P P + C6H12O6 CATABOLISM: Molecule Breakdown
Glucose is broken down into many molecules of ATP (higher # if O2 present) A P P P When bond is broken, energy is released to do cellular work A P P P + Adenosine Diphosphate
 A. P. P. P. When bond is broken, energy is released to do cellular work. A. P. P. P. + Adenosine. Diphosphate.")
18
Glucose Metabolism The process of glucose metabolism involves 1) glycolysis, ) the citric acid cycle (Krebs cycle) ) electron transport. 1-cytoplasm; 2, 3-mitochondria Complete reaction: C6H12O6 + 6O2 >> 6CO2 + 6H2O Net gain = 36 ATP
 glycolysis, 2) the citric acid cycle (Krebs cycle) 3) electron transport. 1-cytoplasm; 2, 3-mitochondria. Complete reaction: C6H12O6 + 6O2 >> 6CO2 + 6H2O. Net gain = 36 ATP.")
19
Only 40% of the energy released through catabolism of glucose is captured in ATP.
The remaining 60% escapes as heat that warms the interior of the cells and the surrounding tissues. If cells have inadequate amounts of glucose to catabolize, the immediately shift to the catabolism of fats for energy. In starvation, proteins are used for energy after carbohydrate and fats are depleted.

20
Fat & Protein Metabolism
Triglycerides >> Fatty acids & Glycerol (lipids) Proteins >> amino acids Lipids and amino acids are broken down into molecules that can enter the citric acid cycle LIPOLYSIS: catabolism of lipids DEAMINATION: catabolism of amino acids Fatty acids or glycerol or amino acids >>intermediate compounds >>Citric Acid Cycle >> ETS >> ATP
 Proteins >> amino acids. Lipids and amino acids are broken down into molecules that can enter the citric acid cycle. LIPOLYSIS: catabolism of lipids. DEAMINATION: catabolism of amino acids. Fatty acids or glycerol or amino acids. >>intermediate compounds. >>Citric Acid Cycle >> ETS >> ATP.")
21
Alternative Catabolic Pathways
Triglycerides Glycogen Proteins Fatty Acids Glycerol Glucose Amino Acids Pyruvic acid cytoplasm Acetyl-CoA mitochondrion Citric Acid Cycle Electron Transport ATP Production

22
REGULATION OF NUTRIENTS
Insulin regulates the uptake of nutrients into the cells, the storage of nutrients not being used, and the conversion of one nutrient type to another.

23
Metabolic Efficiency: Glucose
Cells rely on insulin for efficient absorption of glucose from the blood (except brain cells) Insulin also enhances ATP production Without insulin not enough glucose is supplied to tissues for energy metabolism
 Insulin also enhances ATP production. Without insulin not enough glucose is supplied to tissues for energy metabolism.")
24
A SIMPLIFIED VIEW OF THE
MECHANISM OF INSULIN SIMPLY PUT, insulin can be thought of as the funnel that allows glucose to pass through the receptors into cells. S= SUGAR (glucose)
")
25
Insulin & its chemistry
Insulin is a small protein (MW of human insulin 5808) composed of two amino acid chains connected by two disulfide linkages. Secreted by beta cells, insulin circulates in blood in unbound form. It has a plasma half-life of about 6 min and is cleared from circulation in 10 – 15 min Insulin not combined with receptors in target cells are degraded by insulinase -mostly in liver and also in kidneys and muscles Connecting peptide (white) joins the two chains
 composed of two amino acid chains connected by two disulfide linkages. Secreted by beta cells, insulin circulates in blood in unbound form. It has a plasma half-life of about 6 min and is cleared from circulation in 10 – 15 min. Insulin not combined with receptors. in target cells are degraded by. insulinase -mostly in liver and. also in kidneys and muscles. Connecting peptide (white) joins the two chains.")
26
INSULIN MOLECULE Protein of 21 amino acid A chain and
30 amino acid B chain, Disulfide linkages 21 A Chain B Chain 30

27
Mechanism of Action of Insulin*
The insulin receptor is a combination of 4 subunits held together by disulfide linkages: two α-subunits lying outside the cell membrane and two β- subunits protruding into the cell cytoplasm.

28
Mechanism of Insulin When insulin binds to the α-subunit in target tissues, the β- subunits in turn become activated.

29
Mechanism of Action of Insulin*
Activation of the β-subunits triggers a series of reactions that draw the glucose transporter to the cell membrane. Cells (liver, muscle, adipose, but not brain) are now able to increase their uptake of glucose. (w/in seconds after insulin binds with its membrane) The cell membrane also becomes more permeable to many amino acids.
 are now able to increase their uptake of glucose. (w/in seconds after insulin binds with its membrane) The cell membrane also becomes more permeable to many amino acids.")
30
Mechanism of Action of Insulin*

31
Mechanism of Action of Insulin
Ref:

32
Insulin: Glucose Storage
Only enough ATP for immediate cellular requirements is made at any one time Glucose that is NOT needed for ATP is ANABOLIZED into glycogen and stored for later use in the liver and in muscles. GLYCOGENESIS: synthesis of glycogen from glucose molecules Insulin stimulates glycogenesis (glycogen anabolism) inhibits glycogenolysis (glycogen catabolism)
 inhibits glycogenolysis (glycogen catabolism)")
33
Why is glucose stored as glycogen?
Glucose is in liquid form. As the number of glucose molecules increases, the pressure inside the cell increases. Converting glucose to glycogen (in solid form) relieves pressure inside the cell.
 relieves pressure inside the cell.")
34
Glucose Conversion to Fat
Excess glucose is preferentially stored as glycogen BUT When cells are saturated with glycogen (liver cells store 5 to 8% of their weight as glycogen, muscle cells 1 to 3%) additional glucose is converted to fat in the liver and stored as fat in adipose cells.
 additional glucose is converted to fat in the liver and stored as fat in adipose cells.")
35
Insulin: Glucose>>Fat Storage
Insulin promotes the conversion of all excess glucose in liver that cannot be stored as glycogen into fatty acids Fatty acids are packaged as triglycerides in low density lipoproteins transported by blood to adipose tissue Insulin activates lipoprotein lipase in the capillary walls of adipose tissue, which splits triglycerides into fatty acids. This enables them to be absorbed into adipose cells where they are converted again to triglycerides and stored.

36
Insulin: Protein Metabolism
Insulin (like growth hormone) stimulates transport of amino acids into cells. Insulin increases the translation of messenger RNA, thus forming new proteins.
 stimulates transport of amino acids into cells. Insulin increases the translation of messenger RNA, thus forming new proteins.")
37
Insulin: Protein & Fat Metabolism
Insulin and growth hormone interact synergistically to promote growth Insulin stimulates the absorption of fatty acids and glycerol by adipocytes, where they are stored as triglycerides.

38
Summary: Metabolic Effects of Insulin
Increases rate of glucose transport into target cell Increases rate of glucose utilization and ATP formation Increases conversion of glucose to glycogen (liver, skeletal muscle) Increases amino acid absorption and protein synthesis Increases triglyceride synthesis (adipose tissue) *DECREASES HIGH BLOOD GLUCOSE LEVELS*
 Increases amino acid absorption and protein synthesis. Increases triglyceride synthesis (adipose tissue) *DECREASES HIGH BLOOD GLUCOSE LEVELS*")
39
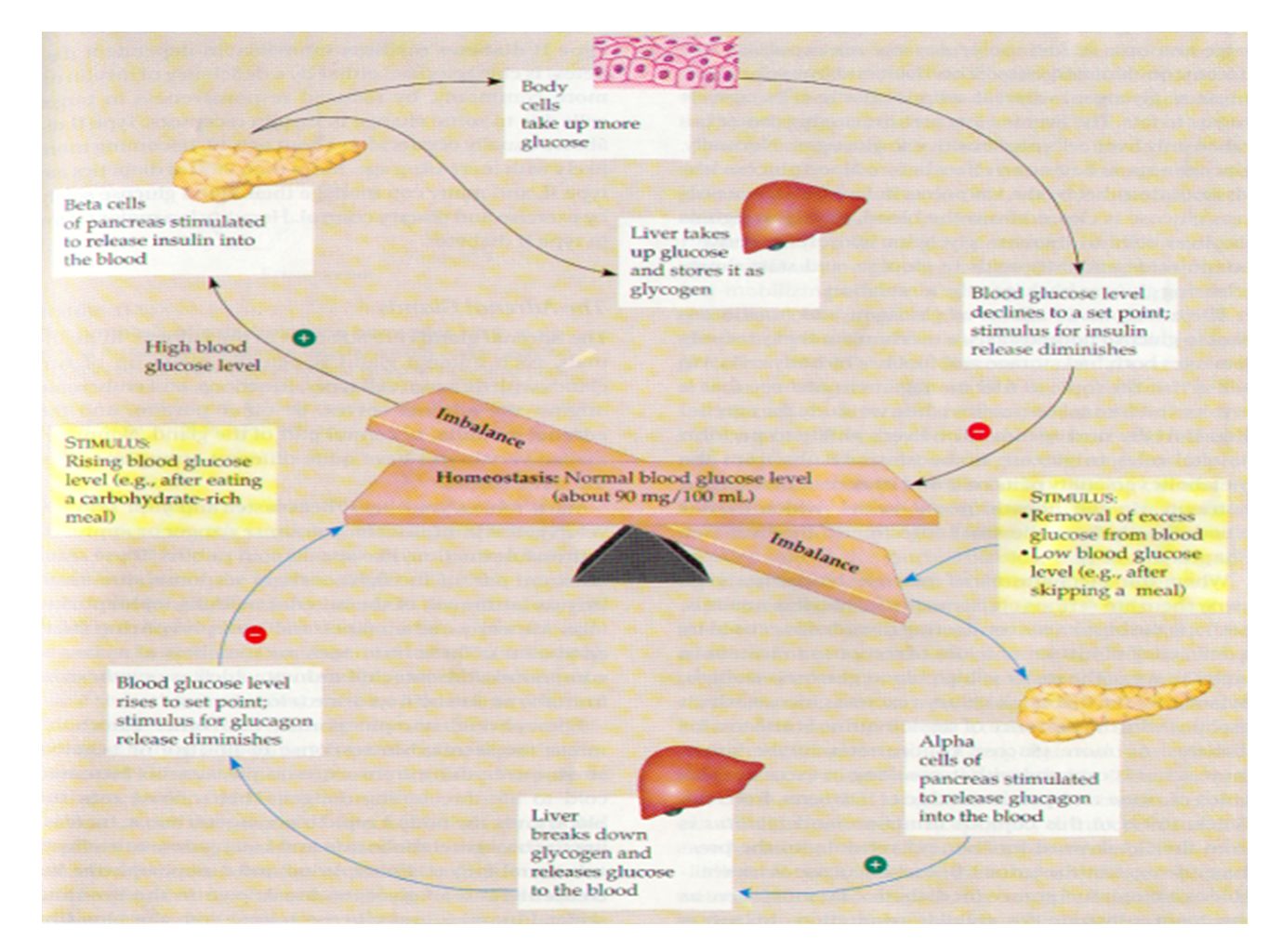
THE REGULATION OF BLOOD GLUCOSE
Beta Cells in Islets of Langerhans Receptors ↑Blood Glucose Stimulus

40
THE REGULATION OF BLOOD GLUCOSE
Increased Insulin secretion and synthesis Intracellular communication Beta Cells in Islets of Langerhans Receptors ↑Blood Glucose Stimulus

41
THE REGULATION OF BLOOD GLUCOSE
Increased Insulin secretion and synthesis Insulin carried in blood Intracellular communication Muscle and fat cells throughout body Liver cells Beta Cells in Islets of Langerhans Receptors ↑Glucose uptake ↓Glucose synthesis Glycogen synthesis Response ↑Blood Glucose Stimulus ↓Blood Glucose ↓Blood Glucose

42
THE REGULATION OF BLOOD GLUCOSE
Increased Insulin secretion and synthesis Efferent Pathway Insulin carried in blood Intracellular communication Muscle and fat cells throughout body Liver cells Effectors Beta Cells in Islets of Langerhans Receptors ↑Glucose uptake ↓Glucose synthesis Glycogen synthesis Response ↑Blood Glucose Stimulus ↓Blood Glucose Negative Feedback ↓Blood Glucose

43
…and LOW blood glucose…
After the meal is over and blood glucose level begins to fall to a low level: The pancreas decreases insulin secretion Glycogen synthesis in liver is stopped Glucose uptake by liver from blood is prevented If blood glucose levels continue to fall, - GLUCAGON will increase the RELEASE of glucose from the cells

44
…and for more glucose… GLUCAGON also causes:
GLYCOGENOLYSIS: Breakdown of glycogen into glucose GLUCONEOGENESIS: Increase of synthesis of glucose from amino acids and the glycerol portion of fat

45
FOR ADDITIONAL NUTRIENTS…
GLUCAGON causes: LIPOLYSIS: Activation of adipose cell lipase making fatty acids available for use as energy source GLUCAGON is a large polypeptide composed of a chain of 29 amino acids and has a molecular weight of Secreted by alpha cells.

47
Somatostatin A polypeptide with 14 amino acids with a 3 min half-life in blood. Same chemical substance as growth hormone inhibitory hormone. Secreted by delta cells. All factors related to ingestion of food stimulate somatostatin secretion Somatostatin has many inhibitory effects: Depresses secretion of insulin and glucagon Decreases motility of stomach, duodenum and gallbladder Decreases secretion and absorption in GI tract It extends the period of time for assimilation of food

48
Pancreatic Polypeptide
Secreted by F cells Inhibits gallbladder contractions Regulates the production of some pancreatic enzymes May help control the rate of nutrient absorption by the digestive tract

49
Part III Diabetes: What’s the problem?

50
Review: Endocrine Effects of Insulin
Stimulates Inhibits Liver Skeletal Muscle Adipose tissue glycogenesis glycogenolysis triglyceride synthesis ketogenesis gluconeogenesis glucose uptake protein synthesis protein degradation glycogenesis glycogenolysis triglyceride storage lipolysis Promotes anabolic processes Inhibits catabolic processes

52
Importance of Insulin Without insulin, glucose transport into the cells will be insufficient. Lacking glucose, cells will have to rely on protein and fat catabolism for fuel. Also, when there is not enough insulin, excess glucose cannot be stored in the liver and muscle tissue. Instead, glucose accumulates in the blood-- above normal levels.

53
The high concentration of glucose in the blood (resulting from the lack of insulin) is called hyperglycemia, or high blood sugar.
 is called hyperglycemia, or high blood sugar.")
54
Blood Glucose Fasting blood glucose concentration (person who has not eaten in the past 3- 4 hours) Normal person: mg / 100 ml Diabetic patient: mg / 100 ml After a meal: Normal person: mg / 100 ml Diabetic patient: < 200 mg / 100 ml

55
EXCESS OF BLOOD GLUCOSE…
Exerts high osmotic pressure in extracellular fluid, causing cellular dehydration Excess of glucose begins to be lost from the body in the urine: GLYCOSURIA

56
GLYCOSURIA >>>
Excessive glucose in the kidney filtrate acts as an osmotic diuretic, inhibiting water reabsorption resulting in POLYURIA: huge urine output >>> decreased blood volume and dehydration. Dehydration stimulates hypothalamic thirst centers, causing POLYDIPSIA: excessive thirst.

57
OTHER SIDE EFFECTS of POLYURIA
The dehydration resulting from polyuria also leads to dry skin. During a period of dehydration, blurred vision can be caused by fluctuations in the amount of glucose and water in the lenses of the eyes.

58
POLYPHAGIA POLYURIA, POLYDYPSIA, & POLYPHAGIA= THE 3 CARDINAL SIGNS OF DIABETES POLYPHAGIA: excessive hunger and food consumption, a sign that the person is “starving in the land of plenty.” That is, although plenty of glucose is available, it cannot be used, and the cells begin to starve. Without fuel, cells cannot produce energy >> fatigue and weight loss.

59
Insulin deficiency >> metabolic use of FAT
A deficiency of insulin will accelerate the breakdown of the body’s fat reserves for fuel. Free fatty acids become the main energy substrate for all tissues except the brain. Increased lipolysis results in the production of organic acids called ketones (KETOGENESIS) in the liver.
 in the liver.")
60
KETOGENESIS>>KETOSIS
The increased ketones in the blood lower the pH of blood, resulting in a form of acidosis called KETOSIS, or ketoacidosis. Ketones are excreted in the urine: KETONURIA.

61
Complications of KETOSIS:
Serious electrolyte losses also occur as the body rids itself of excess ketones. Ketones are negatively charged and carry positive ions out with them. Sodium and potassium are also lost from the body; because of the electrolyte imbalance, the person get abdominal pains and may vomit, and the stress reaction spirals even higher. Can result in coma, death

62
Effects of insulin deficiency on metabolic use of fat
Excess fat metabolism leads to an increase in plasma cholesterol >>> increased plaque formation on the walls of blood vessels. Leads to atherosclerosis & other cardiovascular problems: cerebrovascular insufficiency, ischemic heart disease, peripheral vascular disease, and gangrene.

63
Effects of insulin deficiency on metabolic use of fat
Degenerative changes in cardiac circulation can lead to early heart attacks. Heart attacks are 3-5 times more likely in diabetic individuals than in nondiabetic individuals. The most common cause of death with diabetes mellitus is myocardial infarction.

64
Other complications of diabetes:
A reduction in blood flow to the feet can lead to tissue death, ulceration, infection, and loss of toes or a major portion of one or both feet. Damage to renal blood vessels can cause severe kidney problems. (Nephropathy) Damage to blood vessels of the retina can also cause blindness. (Retinopathy)
 Damage to blood vessels. of the retina can also cause. blindness. (Retinopathy)")
65
Non-Proliferative Retinopathy
Blood vessels in the retina leak and hemorrhage. Patient may notice a decrease in vision if the swelling and hemorrhage affect the macula. Macula edema is the most common cause of visual loss in diabetic retinopathy.

66
Non-Proliferative Diabetic Retinopathy
Fundus photo of normal macula Hemorrhages in non-proliferative diabetic retinopathy

67
Proliferative Retinopathy
New blood vessels grow in the eye. These new blood vessels tend to bleed and leak causing vision loss. These new blood vessels may also pull on the retina causing retinal detachment.

68
Proliferative Diabetic Retinopathy
New blood vessel growth around optic nerve in proliferative diabetic retinopathy Hemorrhage from new blood vessel growth in proliferative diabetic retinopathy

69
Side Effects of Excess Sugar
Loss of vision due to cataracts: Excessive blood sugar chemically attaches to lens proteins, causing cloudiness. Skin infections sometimes occur because excess sugar in the blood suppresses the natural defense mechanism like the action of white blood cells. And sugar is an excellent food for bacteria for food to grow in. BACTERIA CELLS

70
Periodontitis High blood glucose also helps bacteria in the mouth to grow, making tooth and gum problems worse. Gingivitis: bacteria grow in the shallow pocket where the tooth and gum meets; gum begins to pull away from the tooth. Progresses to: Periodontitis: infection causes actual bone loss, teeth begin to pull away from the jaw itself

71
Latter Stages of Periodontitis

72
Damage to the Nerves Numbness and tingling in feet and night leg cramps may result from nerve damage due to prolonged high glucose levels that cause changes in the nerves and “neuron starvation” from lack of cellular glucose. Nerve damage can also lead to a loss of the ability to feel pain in the feet, leading to undue pressure>>calluses>> ulceration. (Neuropathy)
")
73
Diabetic Neuropathy Neuropathy can result in two sets of what appear to be contradictory problems. Most patients who have neuropathy have one these problems but some can be affected by both: 1) symptoms of pain, burning, pins and needles or numbness which lead to discomfort 2) loss of ability to feel pain and other sensation which leads to neuropathic ulceration
 symptoms of pain, burning, pins and needles or numbness which lead to discomfort. 2) loss of ability to feel pain and other sensation which leads to neuropathic ulceration.")
74
Diabetic Neuropathy Patients with neuropathy lose their sensation of pain. As a result, they exert a lot of pressure at one spot under the foot when they walk, building up a callus at that site without causing discomfort. The pressure becomes so high that eventually it causes breakdown of tissues and ulceration.

75
A TYPICAL NEUROPATHIC ULCER IS…
1) PAINLESS 2) SURROUNDED BY CALLUS 3) ASSOCIATED WITH GOOD FOOT PULSES (BECAUSE THE CIRCULATION IS NORMAL) 4) AT THE BOTTOM OF THE FOOT & TIPS OF TOES
 PAINLESS. 2) SURROUNDED BY. CALLUS. 3) ASSOCIATED WITH GOOD FOOT PULSES. (BECAUSE THE CIRCULATION IS NORMAL) 4) AT THE BOTTOM. OF THE FOOT. & TIPS OF TOES.")
76
EFFECTS OF DECREASED INSULIN
Hyposecretion of Insulin Undiscovered mechanisms Malfunction of hormone signal in target cells Decreased insulin effects Increased blood glucose level (hyperglycemia) Decreased glucose available for cellular respiration Kidney’s ability to conserve glucose is exceeded Increased glucose in interstitial fluid Water follows glucose into urine by osmosis Increased urine glucose level (glycosuria) Provides nutrients for microorganisms Net water loss from body Increased volume of urine (polyuria) Increased susceptibility to infection Thirst (polydipsia) EFFECTS OF DECREASED INSULIN = signs & symptoms
 Decreased glucose. available. for cellular respiration. Kidney’s ability to. conserve. glucose is exceeded. Increased glucose in. interstitial fluid. Water follows glucose. into. urine by osmosis. Increased urine glucose. level (glycosuria) Provides nutrients for. microorganisms. Net water loss from. body. Increased volume of. urine (polyuria) Increased. susceptibility. to infection. Thirst. (polydipsia) EFFECTS OF DECREASED INSULIN. = signs & symptoms.")
77
Decreased insulin effects Neurons “starve” Production of Coma
Hyposecretion of Insulin Undiscovered mechanisms Malfunction of hormone signal in target cells Decreased insulin effects Increased blood glucose level (hyperglycemia) Decreased glucose available for cellular respiration Neurons “starve” Shift from using carbohydrates to using fats Nerve diseases Production of ketone bodies Coma Increased blood lipid levels (hyperlipidemia) Weight Loss EFFECTS OF DECREASED INSULIN Acidosis Gallstones Cardiovascular Disorders = signs & symptoms Eye (retina) damage Ulcers & Gangrene Kidney damage Heart Disease Blindness
 Decreased glucose. available. for cellular respiration. Neurons. starve Shift from using. carbohydrates to. using fats. Nerve diseases. Production of. ketone bodies. Coma. Increased blood. lipid levels. (hyperlipidemia) Weight. Loss. EFFECTS OF. DECREASED. INSULIN. Acidosis. Gallstones. Cardiovascular. Disorders. = signs & symptoms. Eye (retina) damage. Ulcers & Gangrene. Kidney. damage. Heart. Disease. Blindness.")
78
INSULIN DEFICIENCY Polyphagia Hyperglycemia Increased lipolysis
Glycosuria EFFECTS OF DECREASED INSULIN Increased free fatty acids (FFA) Polyuria Increased FFA oxidation (liver) Polydipsia Volume depletion DIABETIC COMA Ketoacidosis
 Polyuria. Increased FFA. oxidation (liver) Polydipsia. Volume. depletion. DIABETIC. COMA. Ketoacidosis.")
79
Glucose and insulin secretion
BLOOD GLUCOSE PLASMA INSULIN CONCENTRATION 5 10 15 20 TIME (MIN)
")
80
GLUCOSE TOLERANCE Glucose tolerance is the body’s ability to manage its blood sugar level within normal range. The Cori cycle is a strategy used by the body to accomplish this. The blood sugar of normal individuals can sometimes drop to the hypoglycemic level. This can even be caused by ingesting too much sugar, trig- gering the release of extra insulin.

81
TOO MUCH OF A GOOD THING…
Diabetics use insulin injections to treat high blood glucose levels. It is essential that blood glucose levels always be maintained above a critical level. Brain cells use only glucose for energy. When blood glucose levels fall too low (20 to 50 mg/ml), symptoms of hypoglycemic shock develop – nervous irritability leading to fainting, seizures and coma
, symptoms of hypoglycemic shock develop – nervous irritability leading to fainting, seizures and coma.")
82
Part Iv Diabetes: Type I Vs. Type II

83
History of Diabetes Mellitus
TIME EVENT 1500 BC Ebers Papyrus first describes diabetes 400 BC Susruta records diabetes symptoms and classifies types of diabetes. Charaka refines this work in 6AD. 10 AD Celsus develops a clinical description of diabetes 20 AD Aretaeus coins the term diabetes. 1869 Langerhans describes clusters of cells (islets) in the pancreas. 1889 von Mering and Minkowski observe that diabetes develops when an animal's pancreas is removed. 1921 Banting and Best obtain and purify islets of Langerhans from an animal pancreas, inject the material (insulin) into a diabetic animal, and find a fall in blood sugar level.
 in the pancreas von Mering and Minkowski observe that diabetes develops when an animal s pancreas is removed Banting and Best obtain and purify islets of Langerhans from an animal pancreas, inject the material (insulin) into a diabetic animal, and find a fall in blood sugar level.")
84
The disease’s name was derived from two terms:
Diabetes– Greek for siphon or fountain for the characteristic frequent urination Mellitus– Latin for sweet as honey. In 1679, a physician tasted the urine of a person with diabetes and described as sweet like honey.

85
Type II or Non-Insulin Dependent Diabetes Mellitus (NIDDM)
TYPES OF DIABETES Type I or Insulin-Dependent Diabetes Mellitus (IDDM) The pancreas makes no insulin. It is a result of progressive and irreversible destruction of the islets by the patient's immune system. Treatment: Blood Glucose Measurements Daily Insulin Injections Exercise & Diet Type II or Non-Insulin Dependent Diabetes Mellitus (NIDDM) The pancreas produces some insulin, but often, not sufficient to lower the blood glucose level to normal. Blood Glucose Measurements Oral Medication Insulin Injections
 The pancreas makes no insulin. It is a result of progressive and irreversible destruction of the islets by the patient s immune system. Treatment: Blood Glucose. Measurements. Daily Insulin Injections. Exercise & Diet. Type II or Non-Insulin Dependent Diabetes Mellitus (NIDDM) The pancreas produces some insulin, but often, not sufficient to lower the blood glucose level to normal. Blood Glucose Measurements. Oral Medication. Insulin Injections.")
86
Classification of Diabetes Mellitus
Type 1 (previously called Type I; Insulin-dependent diabetes mellitus, IDDM, juvenile diabetes) Pathophysiology Immune-mediated destruction of ß cells Idiopathic Absolute insulin deficiency- insulin therapy required Accounts for 5 to 10 percent of cases Diabetes Control and Complications Trial (DCCT) showed that control of glycemia slows the onset and progression of eye, kidney, and nerve complications
 Pathophysiology. Immune-mediated destruction of ß cells. Idiopathic. Absolute insulin deficiency- insulin therapy required. Accounts for 5 to 10 percent of cases. Diabetes Control and Complications Trial (DCCT) showed that control of glycemia slows the onset and progression of eye, kidney, and nerve complications.")
87
Pathophysiology of IDDM
Juvenile (14 years of age) Age (years) Stages in the Development of Diabetes Mellitus Genetic predisposition Overt Immunologic abnormalities Normal insulin release Progressive loss of insulin Glucose normal Overt diabetes C-peptide present No β-cell mass
 Age (years) Stages in the Development of Diabetes Mellitus. Genetic predisposition. Overt Immunologic. abnormalities. Normal insulin. release. Progressive. loss of insulin. Glucose. normal. Overt. diabetes. C-peptide. present. No. β-cell. mass.")
88
Classification of Diabetes Mellitus
Type 2 (Type II; Non-insulin-dependent diabetes mellitus, NIDDM) Ranges from predominantly insulin resistance with relative insulin deficiency to a predominantly secretory defect with insulin resistance Insulin therapy required in 20-30% patients; oral hypoglycemic drugs used in most cases; diet and exercise sufficient in mild cases Accounts for 90 to 95 percent of the 18 million cases in the United States.
 Ranges from predominantly insulin resistance with relative insulin deficiency to a predominantly secretory defect with insulin resistance. Insulin therapy required in 20-30% patients; oral hypoglycemic drugs used in most cases; diet and exercise sufficient in mild cases. Accounts for 90 to 95 percent of the 18 million cases in the United States.")
89
Type I vs. Type II Diabetes
Type I (IDDM) Type II (NIDDM) Age at onset Usually under 40 Usually over 40 Body weight Thin Usually overweight Symptoms Appear suddenly Appear slowly Insulin produced None Too little, or it is ineffective Insulin required Must take insulin May require insulin Other names Juvenile onset diabetes Adult onset diabetes
 Type II (NIDDM) Age at onset. Usually under 40. Usually over 40. Body weight. Thin. Usually overweight. Symptoms. Appear suddenly. Appear slowly. Insulin produced. None. Too little, or it is ineffective. Insulin required. Must take insulin. May require insulin. Other names. Juvenile onset diabetes. Adult onset diabetes.")
90
CAUSES OF DIABETES Two factors especially important in the development of diabetes: 1) Heredity: About a 5% risk of developing Type II diabetes if mother, father, or sibling has diabetes. Higher risk (up to 50%) if overweight. 2) Obesity: 80% of people w/ Type II diabetes are overweight when diagnosed and symptoms disappear in many of the obese patients when they lose weight.
 Heredity: About a 5% risk of developing Type II diabetes if mother, father, or sibling has diabetes. Higher risk (up to 50%) if overweight. 2) Obesity: 80% of people w/ Type II diabetes are overweight when diagnosed and symptoms disappear in many of the obese patients when they lose weight.")
91
Other causes/triggers of diabetes:
Age: As people age, their bodies may have fewer insulin- producing beta cells. Faulty immune system: Scientists now believe that there is not one cause of diabetes, but multiple factors that may trigger the immune system to destroy beta cells. Viruses: Certain viruses may destroy beta cells in susceptible people.

92
Other causes/triggers of diabetes:
Physical trauma: An accident or injury may destroy the pancreas, where insulin is normally produced. Stress: Hormones released during periods of stress may block the effect of insulin. Pregnancy: Hormones produced during pregnancy may block the effect of insulin. Drugs: Drugs prescribed for another condition may unmask diabetes.

93
Maintaining Control Protect heart, nerves, blood vessels, eyes, and kidneys by controlling blood glucose level. Maintain schedule for checking blood glucose level and taking insulin. Maintain well-balanced meal plan, exercise program, and healthy weight.

94
How does exercise help? Most of the time muscle tissue
depends on fatty acids for energy Under two conditions muscles use large amounts of glucose: During moderate or heavy exercise (muscle fibers become permeable to glucose even in the absence of insulin– important in Type I) During the few hours after a meal (while pancreas is secreting more insulin– important in Type II). Most of the glucose is stored as muscle glycogen.
 During the few hours after a meal (while pancreas is secreting more insulin– important in Type II). Most of the glucose is stored as muscle glycogen.")
95
The Diabetic Meal Plan Under this plan, 60 to 70 percent of your total daily calories should come from grains, beans, and starchy vegetables, with the rest being meat, cheese, fish and other proteins. Fats, oils, and sweets should be used sparingly. The Diabetes Food Pyramid suggests the following daily servings of food for people with diabetes:

96
DIABETES FOOD PYRAMID

97
The Diabetes Food Pyramid differs from the standard Food Guide Pyramid in the way that it groups different foods together. Because blood glucose is of primary concern to people with diabetes, the Diabetes Food Pyramid focuses on the way in which certain foods affect blood glucose levels. For example, in the standard pyramid, beans and legumes are grouped with meats, due to their protein content. In the diabetes pyramid, however, beans are grouped with starches, because they affect blood glucose in the same way that starchy foods do.

98
And ONE LASE TIME, why are…
Maintaining a well-balanced meal plan, exercise program, and healthy weight AND Maintaining a schedule for checking blood glucose levels taking insulin SO IMPORTANT??????

99
Heart Disease and Stroke
Heart disease is the leading cause of diabetes-related deaths. Adults with diabetes have heart disease death rates about two to four times higher than adults without diabetes. The risk for stroke is two to four times higher among people with diabetes. About 65 percent of deaths among people with diabetes are due to heart disease and stroke.

100
Blindness Diabetes is the leading cause of new cases of blindness among adults aged years. Diabetic retinopathy causes 12,000 to 24,000 new cases of blindness each year.

101
Kidney Disease Diabetes is the leading cause of end-stage renal disease, accounting for 44 percent of new cases. In 2001, 42,813 people with diabetes began treatment for end-stage renal disease. In 2001, a total of 142,963 people with end- stage renal disease due to diabetes were living on chronic dialysis or with a kidney transplant.

102
Nervous System Disease
About 60 percent to 70 percent of people with diabetes have mild to severe forms of nervous system damage. The results of such damage include impaired sensation or pain in the feet or hands, slowed digestion of food in the stomach, carpal tunnel syndrome, and other nerve problems. Severe forms of diabetic nerve disease are a major contributing cause of lower-extremity amputations.

103
Amputations More than 60 percent of non-
traumatic lower-limb amputations occur among people with diabetes. In , about 82,000 non-traumatic lower-limb amputations were performed annually among people with diabetes.

104
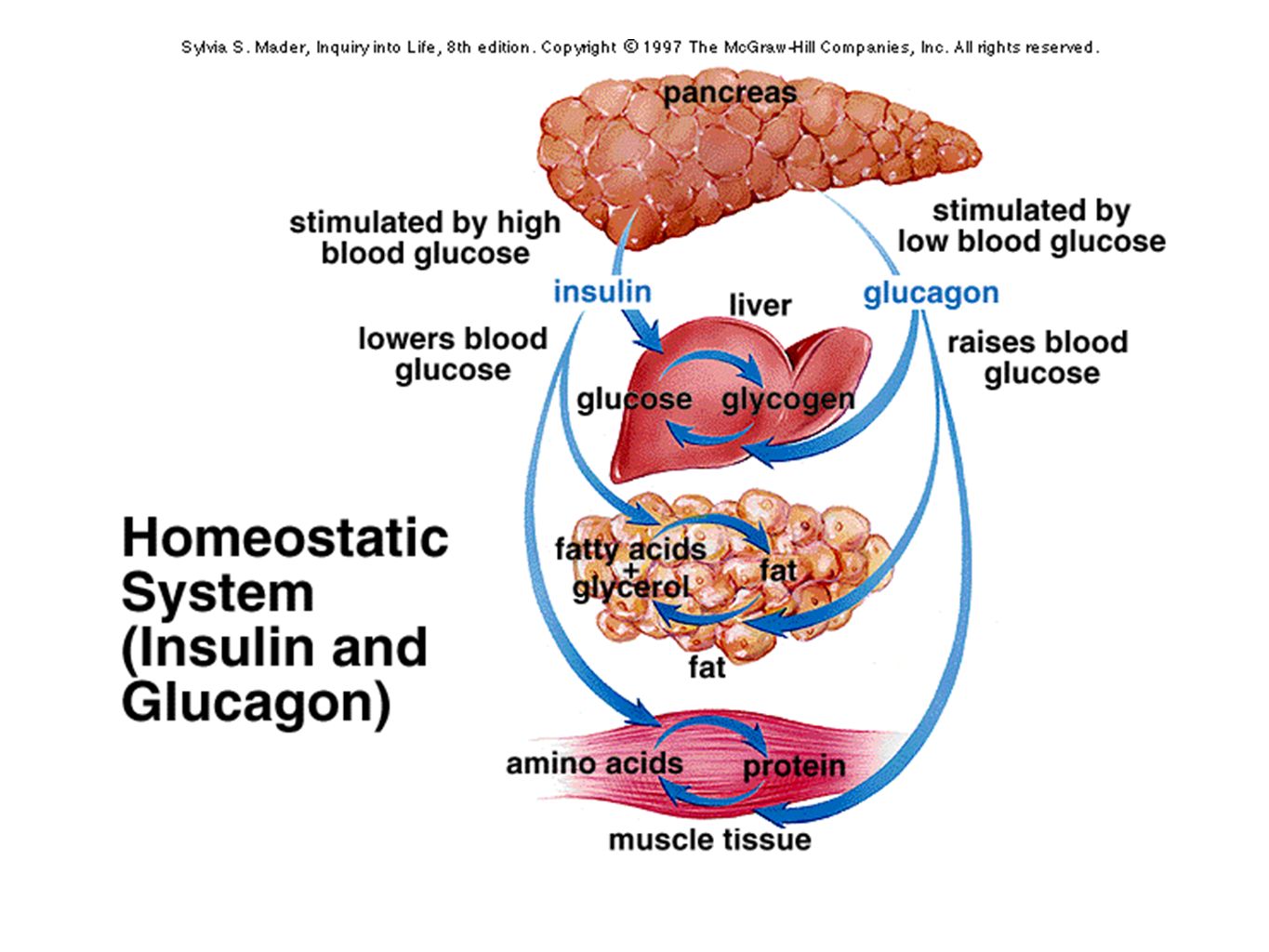
homeostatic mechanism
One final look at the homeostatic mechanism in question: In diabetes, where is the missing link? Can you remember all of the biochemical consequences??? The physical consequences??

Similar presentations








 muscle proteins liver glycogen fat lipids glucose.>")
 muscle proteins liver glycogen fat lipids glucose.>")






 state>")

>")
