Download presentation
Presentation is loading. Please wait.

1
Alcohol policy: research and practice Professor Colin Drummond Institute of Psychiatry King’s College London MSc Addiction January 2011

2
Topics What are the drivers? What are the policy options? What is happening in England? What about Europe? Conclusions

3
What are the drivers?

10
“Rising consumption over the last 25 years have been accompanied by an increase in availability” 68% increase in licensed hotels and restaurants 100% increase in off licences 145% increase in on licence applications Increased capacity of on licenses: “Super pubs” are now 20 times bigger than typical pubs

11
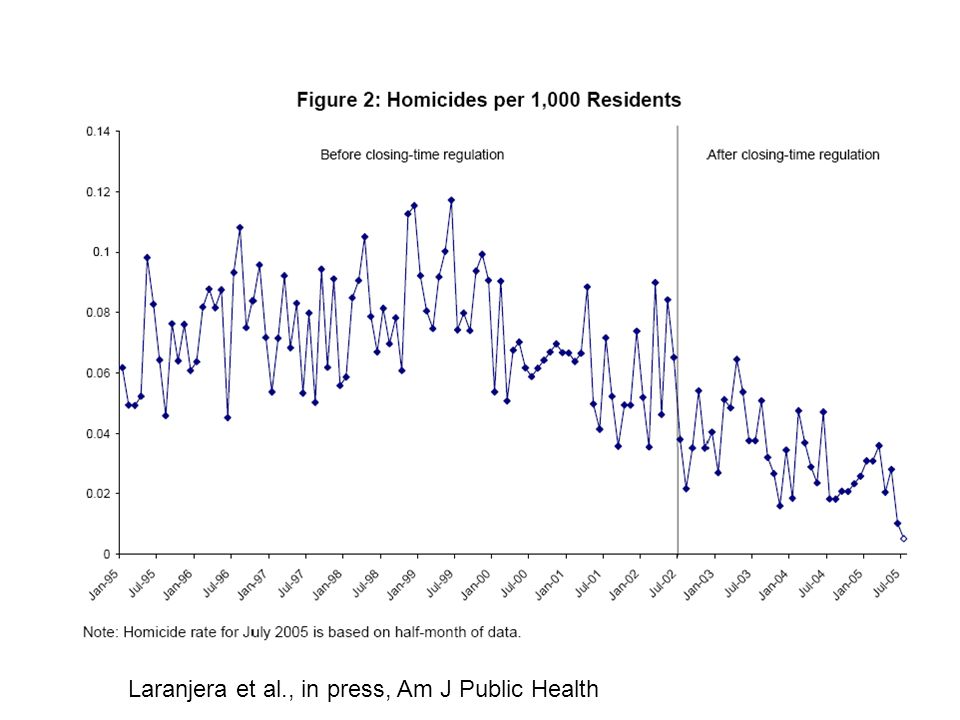
The Licensing Act 2003 explained: Flexible opening hours for premises, with the potential for up to 24 hour opening, seven days a week. This will help to minimise public disorder resulting from fixed closing times.

12
Laranjera et al., in press, Am J Public Health

14
Policy options

15
What the experts said….. Bruun et al., 1975 Royal College of Psychiatrists, 1986 British Medical Association, 1989 Faculty of Public Health Medicine, 1991 Edwards et al., 1994 Royal College of Physicians and the British Pediatric Association, 1995 Babor et al., 2003 Academy of Medical Sciences, 2004 WHO expert committee, 2007 NICE, 2010

16
DISCLAIMER: NO EFFECTIVE STRATEGIES HAVE BEEN USED IN THE MAKING OF THIS DOCUMENT

17
AHRSE, 2004 The two main supply-side levers that are commonly cited as influencing harm are price and availability: –price is controlled by Government through levels of taxation; it is also governed by the laws of supply and demand – for example, price promotions; and –availability is controlled through restrictions on suppliers (planning and licensing law) and individuals. There is a clear association between price, availability and consumption. But there is less sound evidence for the impact of introducing specific policies in a particular social and political context: –our analysis showed that the drivers of consumption are much more complex than merely price and availability; –evidence suggested that using price as a key lever risked major unintended side effects; –the majority of those who drink do so sensibly the majority of the time. –Policies need to be publicly acceptable if they are to succeed; and measures to control price and availability are already built into the system.

18
Alcohol strategy options Babor et al. (2003) Alcohol: No ordinary commodity High impact –Taxation & pricing –Restricting availability –Limiting density of outlets –Lower BAC limits –Graduated driving licences Medium impact –Brief interventions –Treatment –Safer drinking environment –Heavier enforcement Low impact –Unit labelling –“Sensible” drinking campaigns –Public education –School based education –Voluntary advertising restrictions ALCOHOL HARM REDUCTION STRATEGY FOR ENGLAND (AHRSE) 2004
 Alcohol: No ordinary commodity High impact –Taxation & pricing –Restricting availability –Limiting density of outlets –Lower BAC limits –Graduated driving licences Medium impact –Brief interventions –Treatment –Safer drinking environment –Heavier enforcement Low impact –Unit labelling – Sensible drinking campaigns –Public education –School based education –Voluntary advertising restrictions ALCOHOL HARM REDUCTION STRATEGY FOR ENGLAND (AHRSE)")
19
Some major problems No money No targets No high impact strategies Licensing relaxation Voluntary codes for alcohol industry Less effective controls on alcohol consumption Increased criminalisation

20
University of Sheffield report on pricing and promotion (Nov 2008) Commissioned by DH High impact of tax increase Increases across the board have more impact High impact of minimum price Greater impact on heavy drinkers and under-age Impact on harm (40p min price->41,000 less hospital admissions; £500M health cost savings, also reduced crime, unemployment) Smaller impact of banning promotions
 Commissioned by DH High impact of tax increase Increases across the board have more impact High impact of minimum price Greater impact on heavy drinkers and under-age Impact on harm (40p min price->41,000 less hospital admissions; £500M health cost savings, also reduced crime, unemployment) Smaller impact of banning promotions")
21
Impact of minimum price per unit of alcohol on consumption minimum price (p) Change in consumption (%)
 Change in consumption (%)")
22
What the government said March 2009: Donaldson: minimum price of 50p per unit of alcohol to reduce consumption, idea of passive drinking March 2009: Brown: “But... it’s also right that we do not want the responsible sensible majority of moderate drinkers to have to pay more or suffer as a result of the excesses of a small minority” March 2009: Lansley: "There is clearly a need for action. But it is very important to recognise that to deal with this problem we need to deal with people's attitudes and not just the supply and price of alcohol. Higher taxes on high-alcohol drinks aimed at young people March 2009: Donaldson: “I take a different view as to whether heavy drinking is a minor and insignificant problem.” April 2009: Darling Budget: Retains plan for 2% above inflation increase in alcohol tax

23
The growing influence of industry, UK 2004, AHRSE proposes industry levy, threatens legislation 2004, Diageo hosts meeting with PM 2004, CEO of Portman Group joins AERC, and is member of Better Regulation Commission, Scottish Ministerial Advisory Committee on Alcohol Problems, Director, Advertising Standards Agency, Trustee, Drinkaware Trust. 2004, Advertising industry threats to sue Academy of Medical Sciences over Calling Time report

24
The growing influence of industry, UK Nov 2004, Portman group named as agency responsible for delivering public health messages on alcohol in England, in Choosing Health White Paper 2005, DCMS sides with alcohol industry (BBPA) on implementation of Licensing Act 2006, Drinkaware trust, new incarnation of Portman Group, £5M p.a. budget, supported by a national producers fund, “independent” steering group 2005-6, EU alcohol policy roundtable for DG Sanco. Hosted by European Policy Centre. UK companies active in attempting to rubbish public health research.

25
Improving health and treatment services Improve staff training on early identification Pilot early identification and treatment National Needs Assessment MOCAM, evidence review Better help for vulnerable groups (e.g. homeless, drug addicts, mentally ill, young people)
.")
26
Treatment: a spectrum of need Harmful Hazardous Dependence Increasing consumption Brief interventions Specialist interventions Residential interventions Assisted withdrawal

27
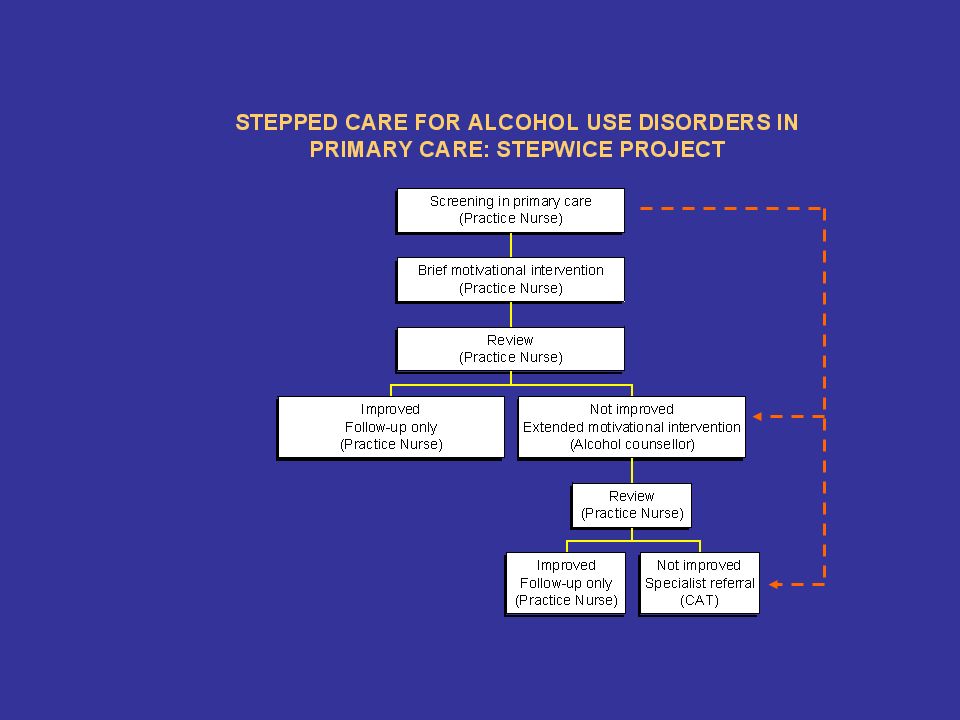
The potential of ‘stepped care’ Caters for a range of needs Intensive interventions delivered only to those who do not respond to brief interventions Practical clinical algorithm (care pathway) Already accepted in a range of conditions New method of shared care with specialists supporting GPs
 Already accepted in a range of conditions New method of shared care with specialists supporting GPs")
30
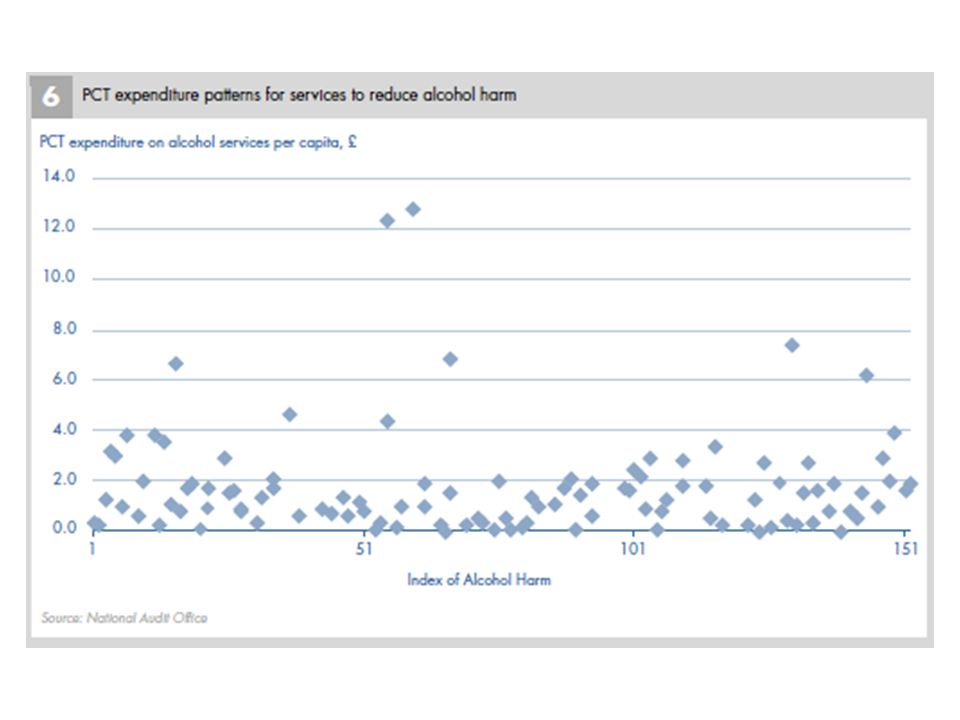
Gap between need and access (PSUR) by region
 by region")
31
Alcohol Screening and Brief Intervention Research Programme national brief intervention research consortium A&E St. Mary’s 'Scientia Vincit Timorem'

32
June 2007

33
Safe, Sensible, Social –No specific funding commitment –Local needs assessment –Redefinition of target groups: young binge drinkers & older adults drinking over 50/35 units –New PSA targets: alcohol-related hospital admissions –National Audit Office study –Roll out of units campaign, social marketing, brief interventions –NTA role: NATMS

34
Safe, Sensible, Social & young people Young people<18 and 18-24 binge drinkers Sharpened criminal justice for drunken behaviour Toughened enforcement of underage sales Trusted guidance for parents and young people Public information campaign to promote sensible drinking Public consultation on alcohol pricing and promotion Local alcohol strategies and partnerships: universal education, targeted support, specialist drug and alcohol treatment (£62M Young People’s Substance Misuse Grant)
")
38
PSA 25 To reduce the rate of alcohol related hospital admissions by 2011 Alcohol related admissions rising by 73,000 pa Aim to reduce the rate from 25% to 11% pa NHS contribution to this of 6% Through the Alcohol Improvement Programme

39
Early Implementor PCTs NHS Planned delivery on RA-RHAs Implementation Support Priority access learning Evidence Trailblazers (SIPS), ANARP Effectiveness review, HES data,etc Trailblazers (SIPS), ANARP Effectiveness review, HES data,etc PCTs (Unplanned) delivery on targets through implementation of elements of the high impact actions learning Alcohol Interventions Improvement Centre Enabling change Priority support to early implementor PCTs. Tools: Learning sets, collaboratives, etc Learning Centre Collects, co-ordinates and disseminates learning and good practice. Tools: SIPS toolkits, HuBCAPP, e-learning resource NST(DH) Supports 18 struggling PCTs P.A. Strategic reports & follow-up visits Review Support Regional co- ordinators (DH/SHA) Responsibility to ensure delivery of targets learning National Alcohol Improvement Programme DH Policy Team Role: Work with outside bodies to facilitate frontline delivery. Develop policy, Develop Guidance, Commission, co-ordinate and contract manage support projects, channel expertise, DH branded learning NWPHO Provide local data on need and key evidence Start delivering RA-RHAs Receive priority support from AIIC Implement high impact actions Support Influence £600k £2.7m £250k £750k £4m £1.2m £60k Total £9.66m for 2009/10 £100k
 Supports 18 struggling PCTs P.A. Strategic reports & follow-up visits Review Support Regional co- ordinators (DH/SHA) Responsibility to ensure delivery of targets learning National Alcohol Improvement Programme DH Policy Team Role: Work with outside bodies to facilitate frontline delivery. Develop policy, Develop Guidance, Commission, co-ordinate and contract manage support projects, channel expertise, DH branded learning NWPHO Provide local data on need and key evidence Start delivering RA-RHAs Receive priority support from AIIC Implement high impact actions Support Influence £600k £2.7m £250k £750k £4m £1.2m £60k Total £9.66m for 2009/10 £100k.")
40
“High Impact Changes” 1.Work in partnership 2.Develop activities to control alcohol misuse 3.Influence change through advocacy 4.Improve the effectiveness and capacity of specialist treatment 100 extra people treated can save 28 admissions 5.Appoint an Alcohol Health Worker Can save 15 admissions per month = 180 per year 6.IBA - Provide more help to encourage people to drink less IBA in A&E can save 40 admissions per year 7.Amplify national social marketing priorities

41
NICE Guidance 2010-11 Alcohol use disorders –Preventing harmful drinking (PH24) –Diagnosis and clinical management of alcohol related physical complications (CG100) –Diagnosis, assessment and management of harmful drinking and alcohol dependence (CG) Related guidance –Psychiatric comorbidity (CG) –Complex pregnancies (CG)
 –Diagnosis and clinical management of alcohol related physical complications (CG100) –Diagnosis, assessment and management of harmful drinking and alcohol dependence (CG) Related guidance –Psychiatric comorbidity (CG) –Complex pregnancies (CG)")
42
Government’s Alcohol Strategy 2013 Minimum unit price Revision of licensing act Responsibility deal for industry Drinkaware Review drinking guidelines NHS health check Under 18 A&E pathway Payment by results

44
What about Europe?

51
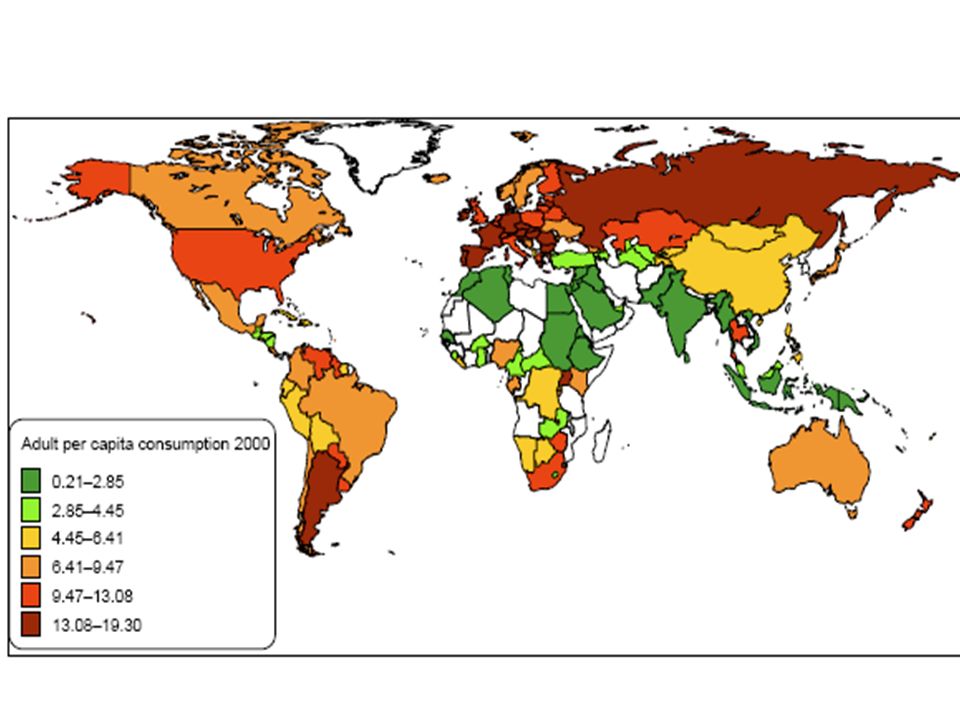
Policy score Less than 9½ 9½ to 10½ 10½ to 12½ More than 12½ Source: Anderson & Baumberg, 2006

52
AMPHORA EU research programme grant 4m Euros, 4 years 9 Workpackages, including –Price consumption and harm –Availability –Cultural determinants –Marketing and advertising –Brief interventions and treatment –Drinking environments –Illegal production

53
1.1. EU adults drink 27g alcohol (nearly three drinks) a day, more than twice the world's average. 2. About 138,000 EU citizens, aged 15-64 years, die prematurely from alcohol in any one year. 3. EU drinkers consume more than 600 times the exposure level set by the European Food Safety Authority for genotoxic carcinogens, of which ethanol is one. 4. Countries with stricter and more comprehensive alcohol policies generally have lower levels of alcohol consumption, and policies are tending to get stricter in recent years. 5. Alcohol policies impact on alcohol consumption, even when talking into account broader socio-demographic changes, such as increased urbanization which is associated with increased consumption and increased maternal age at all childbirths which is associated with decreases in consumption. 6. Online alcohol marketing and alcohol branded sports sponsorship increase the likelihood of 14 year olds to drink alcohol. 7. Brief interventions for risky drinking and pharmacological treatments for alcohol use disorders are effective. 8. The proportion of people who actually access treatment out of those who need it ranges from only 1 in 25 to 1 in 7. 9. Young people are often already drunk by the time they go out, fuelled by cheap alcohol from shops and supermarkets, with drinking venues exacerbating problems further. 10. 10. Monitoring alcohol policy and its impact needs much improvement.

54
European Alcohol Strategy WHO Global alcohol strategy 2010 WHO Implementation plan 2013 WHO European Alcohol Action Plan 2012 EU Alcohol Strategy?

55
Conclusions Effective strategies are available Implementation variable across Europe Influence of the alcohol industry Lack of political will Lack of public support?

56
References Bruun et al. (1975) Alcohol control policies in public health perspective. Finnish Foundation for Alcohol Studies. New Brunswick, New Jersey. Prime Ministers Strategy Unit (2003) Interim Analysis. Cabinet Office. Prime Ministers Strategy Unit (2004) Alcohol Harm Reduction Strategy for England. Cabinet Office, London Drummond et al. (2005) Alcohol Needs Assessment Research Project. Department of Health Anderson and Baumberg (2006) Alcohol in Europe. Institute of Alcohol Studies NTA (2006) Models of Care for Alcohol Misusers Raistrick et al (2007) Review of the effectiveness of treatment for alcohol problems. Department of Health National Audit Office (2008) Reducing alcohol harm. NAO
 Interim Analysis. Cabinet Office. Prime Ministers Strategy Unit (2004) Alcohol Harm Reduction Strategy for England. Cabinet Office, London Drummond et al. (2005) Alcohol Needs Assessment Research Project. Department of Health Anderson and Baumberg (2006) Alcohol in Europe. Institute of Alcohol Studies NTA (2006) Models of Care for Alcohol Misusers Raistrick et al (2007) Review of the effectiveness of treatment for alcohol problems. Department of Health National Audit Office (2008) Reducing alcohol harm. NAO.")
57
References contd Oforei-Adjei, Casswell, Drummond et al (2007) World Health Organisation Expert Committee on Alcohol Problems, Second Report. WHO, Geneva. Babor et al (2003) Alcohol, no ordinary commodity. OUP, Oxford Room et al., (2005) Alcohol and publi health. Lancet, 365, 519 Lancet series 2009: http://www.thelancet.com/series/alcohol-and-global- healthhttp://www.thelancet.com/series/alcohol-and-global- health http://amphoraproject.net/w2box/data/e-book/AM_E- BOOK_2nd%20edition%20- %20final%20Sept%202013_c.pdf
 Alcohol, no ordinary commodity. OUP, Oxford Room et al., (2005) Alcohol and publi health. Lancet, 365, 519 Lancet series 2009: healthhttp:// health BOOK_2nd%20edition%20- %20final%20Sept%202013_c.pdf.")
Similar presentations





 Public Health Alcohol: Its Impact & Address.>")








 practice because it affects: service delivery.>")







