Download presentation
Presentation is loading. Please wait.

1
Department of pharmacology
Antipsychotic Drugs Department of pharmacology

2
Classification Antipsychotic Drugs Antimanic drugs Antidepressants
anxiolytics

3
Antipsychotic Drugs

4
Contents Overview Introduction of Schizophrenia
Classification of antipsychotic drugs Chlorpromazine

5
Overview Antischizophrenic,neuroleptic drugs
These agents are prescribed for treating schizophrenia or management of psychotic symptoms

6
Overview What is schizophrenia ?
There appears to be a genetic component to schizophrenia. There is also evidence for changes in brain structure.

7
Schizophrenia schizophrenia Clinical Manifestations
Characteristics-- perturbations affecting: language perception thinking volition Behavior social activity size of ventricles

8
Unaffected twin Schizophrenic twin MRIs of monozygotic twins show marked enlargement of the lateral ventricle in the twin with schizophreniz

9
Schizophrenia Typically begins in late adolescence Insidious onset.
Syndrome overview: Typically begins in late adolescence Insidious onset. Poor outcome. Social withdrawal /perceptual distortions lead to chronic delusions /hallucinations.

10
Schizophrenia Positive Symptoms: Conceptual disorganization Delusions
Hallucinations

11
Schizophrenia Negative Symptoms: Anhedonia
Decreased emotional expression Impaired concentration Diminished socialization

12
The Nature of Schizophrenia
Incidence is about 70% of hospital patients mental health hospital, with a strong, but not invariable, hereditary component.

13
The Nature of Schizophrenia
Dopamine overactivity hypothesis (especially in left hemisphere). There is some evidence for involvement of 5-HT, and possibly other mediators, such as glutamate.
. There is some evidence for involvement of 5-HT, and possibly other mediators, such as glutamate.")
14
【pathogenesis of schizophrenia】
Relevance of pathogenesis of schizophrenia to dopaminergic nerve in CNS:

15
Pathogenesis of schizophrenia 1
Pathogenesis of schizophrenia 1.DA increases in the brain of the patient. 2.DR increases in the brain of the patient. 3.Functions of dopaminergic neurons increase.

16
4.Promotion of DA release induces episode of schizophrenia.
【pathogenesis of schizophrenia】 4.Promotion of DA release induces episode of schizophrenia. 5.Blocking DR inhibit episode of schizophrenia.

18
Four pathway of dopaminergic neurotransmission
1.limbic system- mesencephalic pathway emotion 2.cortico- mesencephalic pathway thinking and motion

19
Four pathway of dopaminergic neurotransmission
3.nigrostriatum pathway motion 4.hypothalamo-hypophysis pathway endocrine

20
Mechanism of action Antagonism of dopaminergic receptors (D2) in CNS. 1.to block dopamine receptors in limbic system-mesencephalic pathway to improve emotion

21
1 and 2 are therapeutic effects of drugs
Mechanism of action 2.to block dopamine receptor in cortico- mesencephalic pathway to restore thinking and motion 1 and 2 are therapeutic effects of drugs

22
Mechanism of action 3.to block dopamine receptor in nigrostriatum pathway to cause extrapyramidal symptoms the adverse effects of drugs

23
Mechanism of action 4.to bock dopamine receptor in hypothalamo-hypophysis pathway to cause endocrine dysfunction the adverse effects of drugs

24
Classification of antipsychotic drugs
Phenenothiazines (Chlorpromazine) Thioxanthenes (Tardan) Butyrophenones (Haloperidol) Atypicals (Clozapine)
 Thioxanthenes. (Tardan) Butyrophenones. (Haloperidol) Atypicals. (Clozapine)")
25
Available Medications
Typical medications Low potency agents - Chlorpromazine (sedation) High potency agents - Haloperidol (motor problems – extrapyramidal effects) “Atypical” agents Clozapine - great Olanzapine - good Risperidone – good Aripiprazole – partial agonist
 High potency agents - Haloperidol (motor problems – extrapyramidal effects) Atypical agents. Clozapine - great. Olanzapine - good. Risperidone – good. Aripiprazole – partial agonist.")
26
Typical Antipsychotics
Good ability to treat hallucinations and delusions in most people within approximately 2 months

27
Typical Antipsychotics
Limited effect on negative symptoms Flat affect Avolition Anhedonia Attentional impairment (Cognition)
")
28
Chlorpromazine

29
Pharmacologic effects 1
Pharmacologic effects 1.effects on CNS (1) antipsychotic effect (2) sedation and synergism with other CNS depressives (3) antiemetic effects (4) effects on temperature-regulating mechanisms 2.altering endocrine 3.peripheral effects
 antipsychotic effect (2) sedation and synergism with other CNS depressives (3) antiemetic effects (4) effects on temperature-regulating mechanisms 2.altering endocrine 3.peripheral effects")
30
1.effects on CNS antipsychotic effects tranquilization: to make animals docile and friendly, rapidly to control manic states of psychotic patients and make them quiet (calming effect) and peaceful; to make patients feel indifferent, then induce sleep in few days.
 and peaceful; to make patients feel indifferent, then induce sleep. in few days.")
31
1.effects on CNS antipsychotic effects
(2) intellect restoration, emotional quieting, reducing psychomotor excitement of the patient in few weeks. (3) to eliminate hallucination and illusion of the patient in few months.
 intellect restoration, emotional quieting, reducing psychomotor excitement of the patient. in few weeks. (3) to eliminate hallucination and illusion of the patient. in few months.")
32
(4) For normal person to induce sedation
 For normal person to induce sedation")
33
Action mechanism Blocking dopamine D2 receptor in limbic system- mesencephalic and cortico-mesencephalic pathways.

34
Dopamin receptor: two type, five subtype
- DA1 (D1-like receptor): D1,D5 - DA2 (D2-like receptor): D2,D3, D4
: D1,D5. - DA2 (D2-like receptor): D2,D3, D4.")
35
D2 receptor activation motor activity aggravates schizophrenia
D2 receptor blockade alleviation of schizophrenia

36
2) sedation and synergism with other CNS depressives analgesics, sedative-hypnotics, anesthetics.
 sedation and synergism with other CNS depressives analgesics, sedative-hypnotics, anesthetics.")
37
Pharmalogical effects
3)Antiemetic effect. -This is a results of blocking DA2 receptor. -In low doses, blocking DA2 receptor in chemoreceptor trigger zone(CTZ). -In high doses, chlorpromazine may directly depress the medulla vomiting center.
Antiemetic effect. -This is a results of blocking DA2 receptor. -In low doses, blocking DA2 receptor in chemoreceptor trigger zone(CTZ). -In high doses, chlorpromazine may directly depress the medulla vomiting center.")
38
Pharmalogical effects
4)effect on temperature-regulating mechanism to inhibit temperature-regulating center in hypothalamus to induce poikilothermia (hypothermia, hyperthermia).
effect on temperature-regulating mechanism. to inhibit temperature-regulating center in hypothalamus to induce poikilothermia (hypothermia, hyperthermia).")
39
4)effect on temperature-regulating mechanism
in a cold climate it decrease temperature in body in a hot climate they can cause hyperthermia

40
Pharmalogical effects
(2) Autonomic nervous system effects a) Hypotensive effects receptor blockade, postural hypotension b) Anticholinergic effects---- Blocking M-receptor dry mouth, constipation, blurred vision, urinary retention, etc.
 Autonomic nervous system effects. a) Hypotensive effects. receptor blockade, postural hypotension. b) Anticholinergic effects---- Blocking M-receptor. dry mouth, constipation, blurred vision, urinary retention, etc.")
41
Pharmalogical effects
Endocrine system effect Increasing the lactogenic hormone. Increased levels of prolactin may lead to galactorrhea . Phenothiazines decrease FSH and ACTH. Decreasing release and secretion of pituitary growth hormone.

42
Prolactin FSH ACTH growth hormone.

43
Therapeutic uses 1. Psychotic disorders, all kind of schizophrenia.

44
Therapeutic uses 2. Nausea and vomiting.(except carsickness).
ineffective for vomiting induced by stimulating vestibules of ears (motion sickness). effective for nausea and vomiting,
. effective for nausea and vomiting,")
45
Therapeutic uses 3.Artificial hibernation*
Artificial hibernation therapy can be used in serious patients with toxic infection, toxication and trauma etc. CPZ + pethidine + promethazine Artificial hibernation therapy

46
physical reduction of body temperature ↓ body temperature↓+ central depression(sleep) irritability to pathologic reaction↓; basal metabolism↓→ O2 consumption↓; vasodilation→to improve microcirculation to protect the important organs from damage to gain enough time for effective etiological treatment by other drugs.
 irritability to pathologic reaction↓; basal metabolism↓→ O2 consumption↓; vasodilation→to improve microcirculation to protect the important organs from damage to gain enough time for effective etiological treatment by other drugs.")
47
Therapeutic uses 4. antipruritics: promethazine (H1 blocking). 5
Therapeutic uses 4.antipruritics: promethazine (H1 blocking). 5. intractable hiccup: chlorpromazine.
. 5. intractable hiccup: chlorpromazine.")
48
Adverse effects 1.general adverse effects central depression,
M-receptor blockage

49
Adverse effects 2.Extrapyramidal effects:Duo to DA receptor block:
a) Parkinsonism b) Akathisia c) Acute dystonia treated by central muscarinic antagonists Duo to supersensitive to DA: Tardive dyskinesia
 Parkinsonism. b) Akathisia. c) Acute dystonia. treated by central muscarinic antagonists. Duo to supersensitive to DA: Tardive dyskinesia.")
50
Adverse effects 2.extrapyramidal effects acute dystonic reaction (facial grimacing and torticollis) tardive dyskinesia (sucking the lips and other involuntary facial movements).
.")
51
patient display sucking of the lips and other involuntary facial movement. (The dyskinesia may persist for after discontinuation of the therapy).
..")
52
Adverse effects 33.cardiovascular effects: orthostatic hypotension (First choice NA or AD?), syncope and reflex tachycardia.
, syncope and reflex tachycardia.")
53
Adverse effects 4.Inducing psychosis by drug 5.acute toxication
po. large dose: 1~2 g / time, clinical symptoms: narcoma ,Bp shock, cardiac damage, arrhythmia……

54
Adverse effects 6.allergic reaction
skin reactions, leukopenia, obstructive jaundice

55
Adverse effects 7 Endocrine disorder: Hyperprolactinemia--causes:
For women: Amenorrhea(abnormal suppression or absence of menstrual flow), galactorrhea , infertility For men: impotence infertility,diminished libido For children: decreasing growth.
, galactorrhea , infertility. For men: impotence infertility,diminished libido. For children: decreasing growth.")
56
Drug interaction: 1)Increasing CNS inhibition with ethanol, sedative-hypnotics, morphine. 2)Inhibiting the of L-Dopa (agonist of the doparmin-receptor). 3)Increase the dose with phentoin and carbamazepine.
Inhibiting the of L-Dopa (agonist of the doparmin-receptor). 3)Increase the dose with phentoin and carbamazepine.")
57
Antipsychotic drugs Contraindications epilepsy coma
elderly with CVS disorders severe hepatic and renal dysfunction

58
Atypical antipsychotic drugs
Clozapine and Risperidone selectively inhibit D4 and 5-HT2-receptors. Risperidone selectively inhibit D2 and 5-HT2-receptors.

59
Atypical antipsychotic drugs
Sulpiride selectively inhibit D2-receptors in the mesolimbic and mesocortical areas of the brain. Sulpiride ,Clozapine and risperidone have low risk of extra-pyramidal adverse reaction.

60
Atypical antipsychotic drugs
Sulpiride Selectively inhibit D2-receptors in the mesolimbic and mesocortical areas of the brain. Producing low extra-pyramidal adverse reaction.

61
Summary for chlorpromazine

62
1. blocking 3 types of receptors
DR MR αR 2. effect on 3 systems CNS endocrine system Autonomic nervous system 3. 3 main clinical uses psychotic disorders nausea and vomiting, artificial hibernation 4. 3 main adverse reactions central depression extrapyramidal effects cardiovascular effects

63
Antimanic drug Lithium carbonate

64
Pharmacodynamics Possible mechanisms of action:
-effects on electrolyte/ion transport neurotransmitter -neurotransmitter release modulation influence on second messengers. Lithium salts how to affect second messengers?(learning by yourself)
")
65
Antidepressants Overview Classification TCA Antidepressants

66
Overview Depression is an alteration of mood characterized by sadness, worry, and anxiety. The patient may suffer from losses of weight, libido, and enthusiasm.

67
Depression Clinical depression is a syndrome that may include:
Sustained mood disturbances Impaired memory and concentration Disturbed sleep Reduced energy level Reduced libido Impaired sleep.

68
Depression Patient complaints suggestive of depression may include:
Pain (headaches, body aches) A mood of apathy, anxiety, or irritability Sexual complaints low energy, excessive tiredness reduced capacity for enjoyment.
 A mood of apathy, anxiety, or irritability. Sexual complaints. low energy, excessive tiredness. reduced capacity for enjoyment.")
69
Classification of Antidepressant Drugs
Five of antidepressant Tricyclic antidepressants (TCA) Monoamine oxidase inhibitors (MAO) NA reuptake inhibitors Serotonin-specific reuptake inhibitors (SSRIs) Serotonin and NA-specific reuptake inhibitors
 Monoamine oxidase inhibitors (MAO) NA reuptake inhibitors. Serotonin-specific reuptake inhibitors (SSRIs) Serotonin and NA-specific reuptake inhibitors.")
70
Most antidepressants are believed to improve by increasing NT
Catecholamine 5-HT stores

71
Tricyclic antidepressant TCAs
Imipramine

72
Pharmalogic effects CNS
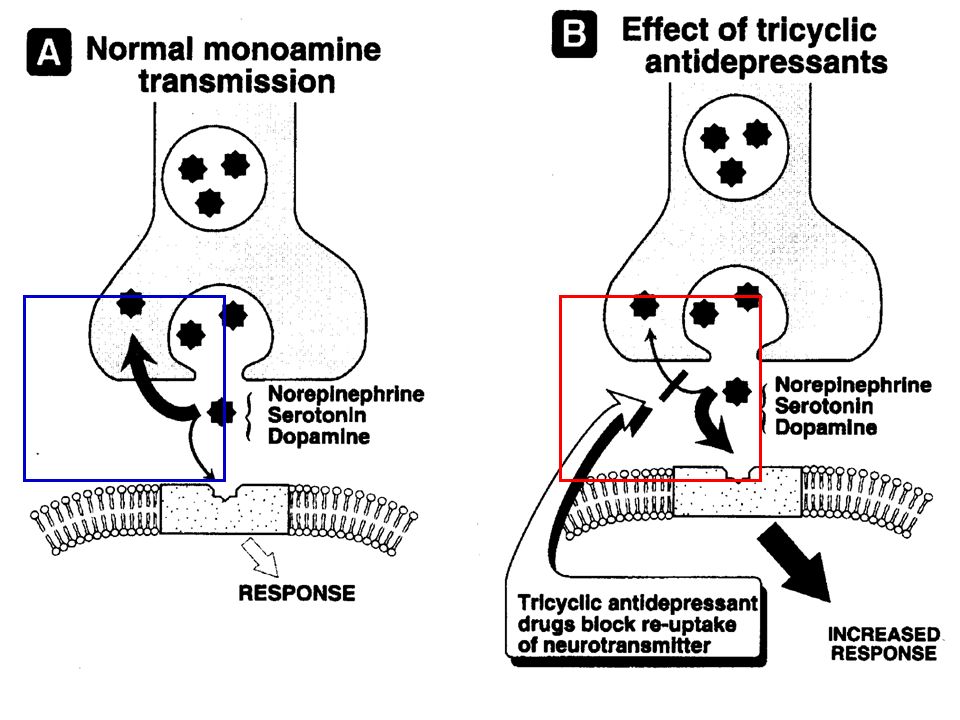
-In the depressed patients , an elevation of mood occur 2-3 weeks after administration begins, the latency period can be as long as 4 weeks. -The imipramine blocks the re-uptake of serotonin and NA

73
Pharmalogic effects Autonomic nervous system Blocking M-receptor

74
Pharmalogic effects Cardovascular effect:
Hypotensin (blocking α receptor) Tachycardia
 Tachycardia.")
75
Mechanism of TCA: Blocking re-uptake of neurotransmitter (NA) (5-HT)
 (5-HT)")
77
Clinic use 1) depression 2)enuresis 3) anxiety and
phobic-anxiety syndromes 4)Obsessive-compulsive neurosis companied by depression
Obsessive-compulsive. neurosis companied by. depression.")
78
Untoward effects 1)anticholinergic effect 2)cardiac arrhythmas
3)manic excitement can occur in patient with bipolar manic-deprssive illness
manic excitement can occur in patient with bipolar manic-deprssive illness.")
79
Untoward effects 4)The combination of a MAO inhibtor with tricyclic antipressants should not be avoided ,since hyperpyrexia, convulsions and coma can result
The combination of a MAO inhibtor with tricyclic antipressants should not be avoided ,since hyperpyrexia, convulsions and coma can result.")
80
Selective Serotonin reuptake inhibitors (SSRI)
A.Fluoxetine B.Paroxetine

81
Summary for antidepressant Drugs

82
Antidepressant Drugs 1. Pharmacological effects (1) Central effects
Inhibiting reuptake of monoamine transmitters Improving patient’s mood after 2 weeks Sedative effects in normal subjects

83
Antidepressant Drugs 1. Pharmacological effects (2) Autonomic effects
Muscarinic blocking effects (3) Cardiovascular effects a-blocker, Hypotension, tachycardia, arrhythmia
 Cardiovascular effects. a-blocker, Hypotension, tachycardia, arrhythmia.")
84
Antidepressant Drugs 2. Clinical uses (1) Treatment of depression
Endogenous, melancholic, etc. (2) Treatment of enuresis (3) Anxiety and panic disorder
 Treatment of enuresis. (3) Anxiety and panic disorder.")
85
Chlorpromazine caused blurred vision, tachycardia, and dry mouth, constipation is due to the blocking: A dopamine (DA) receptor B a adrenaline receptors C ß adrenaline receptors D M receptor E N receptor
 receptor. B a adrenaline receptors. C ß adrenaline receptors. D M receptor. E N receptor.")
86
The role of chlorpromazine in normal person is:
A restlessness B be in high spirits C nervous insomnia D sedation E above are not

87
1.How are agents in this chapter classified?
2.Describe the pharmacological effects of Chlorpromazine. 3 What are the major differences between the TCA and SSRIs?

88
4 Could adrenaline be used in the hypotension induced by chlorpromazine? Why?

Similar presentations



 Department of pharmacology.>")


 Drugs>")





 Chapter 17: Schizophrenia and the Affective Disorders.>")




 2- Schizophrenia.>")


