Download presentation
Presentation is loading. Please wait.

1
Selected by Waleed Awwad, MD, FRCSC
OITE Review Selected by Waleed Awwad, MD, FRCSC

2
1997

3
Year:1997 Question # 7 Figure 2 shows the lateral radiograph of the left hindfoot and ankle of a patient who fell 10 feet and landed on his left foot. The most predictable advantage of open reduction and internal fixation compared with closed management without reduction is a. an earlier return to function. b. decreased subtalar range arthrosis. c. increased ankle dorsiflexion. d. increased subtalar range of motion. e. restoration of height and width of the heel.

5
Correct Answer: e Explanation: Remember, when the calcaneus fractures it loses height, widens, shortens, and falls into varus. None of the first four answers are very "predictable" and that`s what they ask for. In butress plating, you can restore much of the height and width

6
Year:1997 Question # 10 What is the most appropriate biomechanical fixation method/device for a reverse oblique intertrochanteric fracture? a. Ender pins b. Sliding hip screw c. 95-degree fixed angle device d. Cerclage wire with interfragmentary fixation e. Medial displacement osteotomy with sliding hip screw

7
Correct Answer: c Too proximal for Enders. The fracture line would be parallel to a DHS screw; so that would be bad AO fundamentals. Cerlage wiring and interfrags is a pretty weak construct. Medial displacementosteotomies (Fig attached) are done mainly for intertrochs where the Gr. Troch is fractured off or where there is no posteromedial bone (calcar) continuity. There is, however, a "notching" that can be done to make a reverse intertroch more stable. (Fig attached)
 are done mainly for intertrochs where the Gr. Troch is fractured off or where there is no posteromedial bone (calcar) continuity. There is, however, a notching that can be done to make a reverse intertroch more stable. (Fig attached)")
8
Year:1997 Question Figure 5a shows the radiograph of a 22-year-old man 3 years after undergoing reduction and fixation for a fracture of the radius and ulna with two plates secured with 4.5 mm screws. A postoperative radiograph after the plate removal is shown in Figure 5b. Which of the following factors increases the risk of re-fracture? a. Young age b. Incomplete healing c. Use of a large plate d. Bony overgrowth around the plate e. Insufficient amount of time between fracture and plate removal

10
Correct Answer: c Young age would decrease the risk (not #1). There`s no evidence of incomplete healing (npt #2). They used 4.5 mm screws where a 3.5 mm would have been adequate. Bony overgrowth is evident and could potentially be a stress riser, but not nearly as much as those empty 4.5 mm screw holes (not #4). 3 years is plenty of time before plate removal can be done (not #5).
. There`s no evidence of incomplete healing (npt #2). They used 4.5 mm screws where a 3.5 mm would have been adequate. Bony overgrowth is evident and could potentially be a stress riser, but not nearly as much as those empty 4.5 mm screw holes (not #4). 3 years is plenty of time before plate removal can be done (not #5).")
11
Year:1997 Question # 28 Figures 7a and 7b show the wound and radiograph of a 44-year-old man who underwent plating for a closed fracture of his tibia 7 months ago. The wound has been draining for 4 months, and cultures are positive for Staphylococcus aureus. In addition to antibiotics, metal removed, and debridement, treatment should include a. electrical stimulation and casting. b. soft-tissue coverage and re-plating with a bone graft. c. bone grafting, soft-tissue coverage, and application of a cast. d. external fixation, staged soft-tissue coverage, and bone grafting. e. intramedullary rodding, staged soft-tissue coverage, and bone grafting.

13
Correct Answer: d Osteomyelitis, or inflammation of the bone, can result from hematogenous seeding, from direct inoculation (ie, following open fractures or following open reduction and internal fixation of fractures), or from the contiguous spread of bacteria from infected structures. Early diagnosis and effective surgical and antibiotic management can control the infection; suppression of its activity may last a lifetime. Basic treatment should include thorough debridement, irrigation, wound management (external fixation, staged soft-tissue coverage), and bone grafting.
, or from the contiguous spread of bacteria from infected structures. Early diagnosis and effective surgical and antibiotic management can control the infection; suppression of its activity may last a lifetime. Basic treatment should include thorough debridement, irrigation, wound management (external fixation, staged soft-tissue coverage), and bone grafting.")
14
Year:1997 Question # 32 Figures 10a and 10b show radiographs of a 27 year-old woman who sustained an injury to her left, nondominant forearm as a result of a motor vehicle accident. Under anesthesia, it is noted that the distal radioulnar joint is unstable but reducible in supination. Treatment should include a. closed reduction, followed by splint immobilization with the limb in supination. b. closed reduction and external fixation of the radius, followed by splint immobilization with the limb in supination. c. open reduction and external fixation of the radius, with fixation of the radioulnar joint. d. open reduction and internal plate fixation of the radius, with fixation of the distal radioulnar joint. e. open reduction and internal plate fixation of the radius, with immobilization of the distal radioulnar joint in supination.

16
Correct Answer: e The Galeazzi eponym, originally defined as fracture of the distal third of the radial shaft with an associated dislocation of the distal radioulnar joint (DRUJ), has been applied when referring to a fracture anywhere along the radial shaft as well as to fractures to both radius and ulna that occur in conjunction with a DRUJ injury. Monteggia and Galeazzi lesions require anatomic reduction of the diaphyseal fracture component in order to restore the normal axial interrelationship of the forearm bones and allow reduction of the dislocation. Fracture fixation is accompanied best by plating. Residual instability of a reduced DRUJ after anatomic plating of the radius can usually be addressed by immobilizing the limb in supination for 6 weeks postoperatively. Temporary pin fixation of the DRUJ is rarely required. Cast immobilization after surgical treatment of closed, unstable single bone forearm injuries has not been shown to have any detrimental effect on functional outcome.
, has been applied when referring to a fracture anywhere along the radial shaft as well as to fractures to both radius and ulna that occur in conjunction with a DRUJ injury. Monteggia and Galeazzi lesions require anatomic reduction of the diaphyseal fracture component in order to restore the normal axial interrelationship of the forearm bones and allow reduction of the dislocation. Fracture fixation is accompanied best by plating. Residual instability of a reduced DRUJ after anatomic plating of the radius can usually be addressed by immobilizing the limb in supination for 6 weeks postoperatively. Temporary pin fixation of the DRUJ is rarely required. Cast immobilization after surgical treatment of closed, unstable single bone forearm injuries has not been shown to have any detrimental effect on functional outcome.")
17
Year:1997 Question # 37 The incidence of vascular injury after an anterior knee dislocation is a. less than 5%. b. 10% to 25%. c. 30% to 50%. d. 60% to 80% e. greater than 95%.

18
Correct Answer: c Knee dislocation are classified relative to the position of the tibia, and there are five types. Anterior knee dislocation occur most frequently (40%), followed by posterior (33%), lateral (18%), and other (5%). The incidence of vascular injury after an anterior or posterior knee dislocation has been reported to be 20% - 35%. (Most studies quote 30%). Neurologic injuries most frequently involve the common peroneal nerve nerve because of its tethered proximity to the fibular head. Lateral and posterolateral dislocations are the most frequent causes of common peroneal nerve injury. Overall, incidence of neurologic injuries varies between 16% and 40%. Less than 50% of patients will have partial or complete recovery from a peroneal nerve.
, followed by posterior (33%), lateral (18%), and other (5%). The incidence of vascular injury after an anterior or posterior knee dislocation has been reported to be 20% - 35%. (Most studies quote 30%). Neurologic injuries most frequently involve the common peroneal nerve nerve because of its tethered proximity to the fibular head. Lateral and posterolateral dislocations are the most frequent causes of common peroneal nerve injury. Overall, incidence of neurologic injuries varies between 16% and 40%. Less than 50% of patients will have partial or complete recovery from a peroneal nerve.")
19
Year:1997 Question # 40 A 45-year-old man sustains an injury to his pelvic ring as a result of a motor vehicle accident. Radiographs are shown in Figures 11a through 11c, and a CT scan is shown in Figure 11d. Examination reveals that he is hemodynamically stable and has no associated injuries. Management should include a. anterior sacroiliac plate fixation. b. anterior fixation of the pubic symphysis. c. posterior fixation of the left sacroiliac joint. d. early mobilization and weight bearing without internal fixation. e. combined anterior fixation to the pubic symphysis and posterior fixation of the left sacroiliac joint.

21
Correct Answer: b Disruptions of the symphysis pubis are variable. The symphyseal ligaments, the pubic meniscus, and the arcuate ligament may be disrupted. For isolated disruptions of the symphysis pubis, most authors advocate closed, nonsurgical management, especially when the symphysis diastasis is less than 2.5 cm. In cases where the diastasis exceeds this limit, stabilization should be pursued.

22
Year:1997 Question # 41 Radiographs of a 24-year-old man who sustained an open tibial frature 11 months ago are shown in Figures 12a and 12b. Examination shows an anteromedial draining wound over the midtibia. Which of the following methods will most accurately identify the pathologic microorganisms? a. Swab culture of the sinus tract b. Operative sampling of the sinus tract c. Operative sampling of the posterolateral sequestrum d. Operative sampling of deep specimens from multiple foci e. Needle aspiration of the distal tibial metaphyseal abscess

24
Correct Answer: d In a recent study, pathogens that were identified on cultures of material obtained by swabbing of the superficial aspect of a wound and needle biopsy were compared with those that were isolated from material that was obtained at debridement. The cultures of material that was obtained by superficial swabbing of the wound and needle biopsy were inadequate for prediction of the presence of aerobic organisms. Moreover, the failure to isolate anaerobies from the material obtained by needle biopsy did not rule out the presence of anerobic organisms, nor does it rule out the possibility that osteomyelitis may be reactivated after intramedullary nailing with reaming. Therfore, tissue for culture of aerobic and anerobic organisms must be obtained during operative debridement in order to identify all pathogenic organisms. Other studies have shown that cultures must be taken from multiple sites in chronic osteomyelitis of long bones in order to properly treat all varieties of bacteria present.

25
Year:1997 Question A 37-year-old man who sustained a type IIIB open fracture of the middle third of the tibia after a severe crush injury has significant contusions and some necrosis of the posterior muscles. Treatment consists of debridement and external fixation. Which of the following muscle flaps should be used for soft-tissue coverage of the exposed anteromedial tibia? a. Soleus b. Fasciocutaneous c. Medial gastrocnemius d. Lateral gastrocnemius e. Free vascularized muscle

26
Correct Answer: e Grade IIIB indicates initial soft-tissue loss and extensive areas of denuded bone that make later flap coverage necessary. All grade IIIB and many grade IIIC wounds require flap coverage. For the proximal third of the leg, such coverage is best achieved with a gastrocnemius flap; a soleus flap will cover soft-tissue defects extending towards the mid-aspect of the tibia, but a free flap is required for more distal defects. If the solius or gastrocnemius muscles have been damaged, they are unsuitable for local coverage and a free flap must be substituted.

27
Year:1997 Question # 44 A previously active 36-year-old woman who fractured her right ankle 10 years ago and was treated with 6 weeks of cast immobilization now has had pain and swelling for the past year and is no longer able to play tennis or jog. Examination shows swelling and a 10-degree loss of dorsiflexion when compared with the normal, contralateral ankle. Radiographs show shortening of the fibula, widening of the ankle mortise, lateral tilt of the talus, and slight narrowing of the tibiotalar joint space. Treatment should include a. ankle fusion. b. osteotomy of the fibula. c. deltoid ligament reconstruction. d. a custom-made plastic shoe insert. e. nonsteroidal anti-inflammatory drug therapy

28
Correct Answer: b Patients who had reconstructive surgery for a malunion of a displaced fracture of the fibula were evaluated. In these patients who had pain, swelling of the ankle, and stiffness at an average of six years after the injury, the malunions were classified radiographically as either occult or overt. An occult malunion was one in which the talus remained in its normal position, but the lateral malleolus showed residual displacement, characterized byexternal rotation and shortening. In an overt malunion, there were similar changes in the lateral malleolus to correct the external rotation and shortening, to reduce the lateral subluxation or the anterior aspect of the tibiofibular joint, and to restore the stability of the talus.

29
Year:1997 Question # 61 A 38-year-old woman who sustained multiple blunt injuries, including a unilateral lateral compression injury to the pelvic ring as a result of a motor vehicle accident, is awake, alert, and normotensive; however, she has a decreased pulse pressure, a pulse of 110/min and a urine output of 20 mL/hr. She responds to an initial fluid bolus; however, after the fluids are slowed, perfusion begins to deteriorate. An increase in fluids and blood administration is instituted. To evaluate the abdomen as a potential bleeding source, management should include a. obtaining a CT scan of the abdomen. b. obtaining lateral decubitus radiographs of the abdomen. c. obtaining a crosstable lateral radiograph of the abdomen. d. performing an exploratory laporatomy. e. performing a supraumbilical diagnostic peritoneal lavage.

30
Correct Answer: e This question is for the initial evaluation of hemodynamic instability in a multitrauma patient with pelvic fractures. This question specifically asks for the test to evaluate the abdomen as a source of bleeding. While a CT scan can help us identify the pelvic fracture, a DPL is the quickest way to identify intra-abdominal bleeding, and the trauma surgeons can tell pretty quickly whether a patient needs to go to OR based on the outflow color from the DPL.

31
Year:1997 Question # 64 An 18-year-old woman has a closed femoral shaft fracture and facial trauma. Cervical spine radiographs are normal. Because of moderate facial edema, internal fixation of the femur is delayed. Two days later, the patient is noted to have mental confusion and dyspnea. The lungs are clear to auscultation with normal breath sounds. Vital signs are pulse, 100/min; respiration, 35/min; blood pressure, 140/95 mm Hg. Arterial blood gases are pO2, 70; pCO2, 45. The pH was The most likely diagnosis is a. occult head injury. b. pulmonary embolism. c. spontaneous pneumothorax. d. fat embolism. e. upper airway obstruction

32
Correct Answer: d This scenario is pointing to fat embolism from the beginning. This is a young patient with a long bone fracture, two days out. The abg suggests acute hyppoxemia, without a compensated metabolic situation. While the confusion can be associated with a head injury, the abg is not. Confusion from hypoxemia is probably causal, and dyspnea too, is associated with fat embolism. The three most worrisome problems are listed, being PE, pneumothorax, and acute upper airway obstruction. The breath sounds woulkd all be affected in these however.

33
Year:1997 Question # 74 A 25-year-old woman who has multiple injuries, including closed femoral and tibial shaft fractures, is initially awake and alert, but during resusitation she becomes somnolent. A chest radiograph shows three rib fractures on the right side, and an AP view of the pelvis shows a 3-cm pubic diastasis. She has a systolic blood pressure of 220 mm Hg and a pulse rate of 38/min. Treatment should include a. pelvic angiography. b. diagnostic peritoneal lavage. c. emergency CT scan of the head and a neurosurgical consultation. d. administration of 2 L of crystalloid and blood type and crossmatching. e. insertion of a chest tube in the midclavicular line of the second intercostal space.

34
Correct Answer: c Although hypotension could be the cause of her somnolence, her SBP is quite high indicating that this is not likely, also she is not tachycardic which is a hallmark of hypovolemic shock. Cardiac Tamponade or tension ptx is another thought but this is not mentioned on the CXR. The only other source for somnolence to consider is neurogenic. Choices 1,2,4 all pertain to diagnosis of a hypovolemic origin. Choice 3 is best as it directly deals with a neurogenic origin as is likely in this case scenario.

35
Year:1997 Question # 88 Initial radiographs of a 56-year-old man who sustained a closed fractue of the distal tibia in a motor vehicle accident are shown in Figures 24a and 24b. Figure 24c shows a clinical photograph of the injured foot and ankle in the operating room 8 days later. The chances of surgical wound complications are most likely to be minimized by a. avoiding plate fixation of the distal tibia. b. keeping the incisions spread by more than 7 cm. c. using low-profile malleable plates. d. using a "pilon" fracture incision and a femoral distractor. e. using a topical antibiotic cream and delaying surgery for 3 to 5 more days

37
Correct Answer: a Several studies over the last several years have concluded that limited internal fixation (usually lateral) combined with external fixation reduce the risk of soft tissuue insult in pilon fxs. Choice 2, keeping the incisions 7 cm apart is correct but it is even better to not make 2 incisions at all. Choice 3, using low profile plates is also a good idea, but again, no plate is even better. Choice 4, using a pilon fracture incision and a femoral distractor indicates the intent for ORIF, which would be best avoided. Choice 5, using a topical antibiotic cream and delaying surgery for 3 to 5 more days is only partially true. Abx cream is not recommende nor helpful. Most authors do recommend delaying any open surgery until days after the trauma to allow the soft tissue swelling to subside. **JAAOS 1994 Nov./Dec **References:Keywords: Question 16 of 145
 combined with external fixation reduce the risk of soft tissuue insult in pilon fxs. Choice 2, keeping the incisions 7 cm apart is correct but it is even better to not make 2 incisions at all. Choice 3, using low profile plates is also a good idea, but again, no plate is even better. Choice 4, using a pilon fracture incision and a femoral distractor indicates the intent for ORIF, which would be best avoided. Choice 5, using a topical antibiotic cream and delaying surgery for 3 to 5 more days is only partially true. Abx cream is not recommende nor helpful. Most authors do recommend delaying any open surgery until days after the trauma to allow the soft tissue swelling to subside. **JAAOS 1994 Nov./Dec **References:Keywords: Question 16 of 145.")
38
Year:1997 Question # 120 An 18-year-old active duty soldier sustains a 6-cm segmental loss to the tibial diaphysis from an antipersonnel mine. Treatment consists of a fine wire circular external fixator with bone transport, and the immediate postopertive course is uneventful. The patient is given instructions in advancing the frame during a convalescent leave. A radiograph taken 5 weeks postoperatively shows a gain of 4.5 cm and a radiolucent linear area transversely through the middle of the regenerate bone. This finding is most likely the result of a. a fracture. b. a pin tract infection. c. advancing the frame too fast. d. advancing the frame to slowly. e. infection within the regenerate

39
Correct Answer: c The Ilizarov method of distraction osteosynthesis typically calls for lengthening/distracting at a rate of 1mm/day. At 7 weeks out, the radiographs show 4.5cm of distraction. This is 1cm longer than it should be distracted and accounts for the radiolucency in the regenerate bone. There is no history which is consistent with refracture or infection.

40
Year:1997 Question A patient undergoes anatomic reduction and stable fixation of a spiral distal fibula fracture that is 4.5 cm above the joint. With which of the following concomitant injuries is the patient most likely to benefit from placement of a syndesmosis screw? a. Deltoid ligament rupture b. Wagstaffes avulsion fracture c. Rupture of the anterior inferior tibiofibular ligament d. Oblique medial malleolus fracture that has been reduced and stabilized e. Transverse medial malleolus fracture that has been reduced and stabilized

41
Correct Answer: a In 1991, J Soleri, et al performed a biomechanical cadaveric study to investigate the need for syndesmotic screws in a Weber C ankle fracture. Their results supported earlier studies which showed that the medial complex (medial malleolus and deltoid ligament) is the primary stabilizer of the talus in the ankle mortise. As a result, they recommended the placement of a syndesmotic screw in Weber C ankle fractures with deltoid ligament insufficiency.
 is the primary stabilizer of the talus in the ankle mortise. As a result, they recommended the placement of a syndesmotic screw in Weber C ankle fractures with deltoid ligament insufficiency.")
42
Year:1997 Question A 25-year-old man sustains multiple injuries, including a pelvic ring disruption, in a motor vehicle accident. He is hemodynamically stable. Attempts to pass a urinary catheter are unsuccessful. What diagnostic test should be obtained next? a. CT scan b. Cystogram c. Urinalysis d. Excretory urogram e. Retrograde urethrogram

43
Correct Answer: e In pelvic trauma, inability to pass a urinary catheter may be a sign of urethral trauma. A retrograde urethrogram is sthe diagnositic study of choice.

44
Year:1997 Question A 35-year-old man sustains a closed Galeazzi fracture-dislocation and a fracture of the ulnar styloid process as a result of a high-speed motor vehicle accident. The radius fracture is anatomically fixed with a plate; however, the ulnar head remains dislocated. What structure is most likely responsible for preventing reduction? a. Radioulnar capsule b. Pronator Quadratus c. Flexor carpi ulnaris d. Extensor carpi ulnaris e. Triangular fibrocartilage complex

45
Correct Answer: d Difficulty with reduction of the ulnar head may be caused by interposition of the ECU. Due to its firm attachment to the triangular fibrocartilage complex by its fibro-osseous sheath, it is usually the structure that prevents reduction

46
Year:1997 Question Examination of a construction worker who received an accidental electric shock while on the job reveals that he is awake, alert, and holding his arm tightly against the chest and holding his forearm tightly to the front of the trunk. External rotation and abduction are severely limited and painful. Which of the following injuries best accounts for these findings? a. Luxatio erecta b. Anterior dislocation of the glenhumeral joint c. Superior dislocation of the glenhumeral joint d. Posterior dislocation of the glenhumeral joint e. Greater tuberosity fracture of the proximal humerus

47
Correct Answer: d Common causes of failure to externally rotate shoulder are DJD, adhesive capsulitis, and posterior dislocation. Seizures are the most common cause of posterior dislocations.

48
Year:1997 Question A 30-year-old soccor player has pain and swelling 4 hours after being kicked in the anterior compartment of the leg. Which of the following physical findings best indicates increased compartment pressure? a. Anterior compartment tenderness b. Pain with active ankle dorsiflexion c. Pain with passive flexion of the toes d. Pain with passive extension of the toes e. Decreased sensation on the dorsum of the foot

49
Correct Answer: c Severe pain, out of proportion to the injury, with passive stretching of a muscle is indicative of increased compartment pressures. Toe flexion would stretch the EHL and EDC muscles which reside in the anterior compartment. This compartment as well as the deep post. compartment are the most commonly involved. Generally speaking, compartment syndrome usually occurs in less than 24 hours. Ischemic injury starts when the pressures reach mmHg below DBP. Paralysis and sensory changes can occur within one hour of the ischemia. Within the first 4 hours of ischemia only noepraxic injury occurs, but after 8 hours there is axonotmesis which is irreversible. Also, the area of highest pressure is not always palpable but is generally at the level of the fracture.

50
Year:1997 Question A 31-year-old woman has had instability of the right ankle for the past 10 years. Stress radiographs show asymmetrical anterior drawer translation, excess lateral opening, and a unilateral os subfibulare on the affected side. In this patient, the os subfibulare represents a. a supernumary bone. b. an unfused accessory ossification center. c. a nonunion of an avulsion fracture of the talus. d. a nonunion of an avulsion fracture of the fibula. e. a nonunion of an avulsion fracture of the calcis.

51
Correct Answer: d This patient has signs c/w a torn anterior talofibular ligament (the most commonly ruptured ligament in the human body). It is thought that an os subfibulare represents an avulsion fracture of the anterior talofibular ligament and is not a normal variant. Anatomic studies have shown that there is no secondary ossification center at this site and when examined at the time of surgery it was noted that these all represented an avulsion fracture. An os subtibiale was noted in 20% of normal x-rays and found to be bilateral 50% of the time.
. It is thought that an os subfibulare represents an avulsion fracture of the anterior talofibular ligament and is not a normal variant. Anatomic studies have shown that there is no secondary ossification center at this site and when examined at the time of surgery it was noted that these all represented an avulsion fracture. An os subtibiale was noted in 20% of normal x-rays and found to be bilateral 50% of the time.")
52
Year:1997 Question A 20-year-old man who sustains closed femoral and tibial shaft fractures has mild distension of the abdomen, a systolic blood pressure of 75 mm Hg, and a pulse rate of 135/min. His neurovascular examination is normal. Lateral cervical spine, chest, and AP pelvis radiographs are normal. After administration of 2 L of crystalloid, he has a systolic blood pressure of 95 mm Hg and a pulse rate of 120/min. Management should now include a. diagnostic peritoneal lavage. b. immediate femoral nailing and splinting of the tibia. c. immediate stabilization of both the femur and the tibia. d. splinting the tibia and placing the femur in skeletal traction. e. simultaneous retrograde femoral nailing and an exploratory laparotomy

53
Correct Answer: a Shock can be classified as hypovolemic, cardogenic, neurogenic, and septic. Class I % blood volume loss up to 15%.....HR < SBP NI Pulse pressure NI Class II......% blood volume loss 15-30% HR > SBP NI Pulse pressure decreased Class III.....% blood volume loss 30-40% HR > SBP < Pulse pressure decreased Class IV.....% blood volume loss >40% HR > SBP < Pulse pressure decreased In a study of 100 patients with femur fractures (62 w/isolated fx and 38 w/additional fxs) no patient had greater than class II shock. In a patient with a closed femur fx and hypotension further work up is required to determine the cause of the hypotension (ie DPL). Treatment of the fracture immediately is indicated to decrease the risk of ARDS, and fat emboli syndrome
 no patient had greater than class II shock. In a patient with a closed femur fx and hypotension further work up is required to determine the cause of the hypotension (ie DPL). Treatment of the fracture immediately is indicated to decrease the risk of ARDS, and fat emboli syndrome.")
54
Year:1997 Question # 244 A 29-year-old man who has an isolated knee injury following a motor vehicle accident is neurovascularly intact, Plain radiographs are shown in Figures 68a and 68b, and two cuts of an axial CT scan are shown in Figures 68a and 68d. Reduction and fixation would be best accomplished by a. percutaneous reduction and hybrid external fixation. b. arthroscopically assisted reduction and percutaneous screw fixation from anterolateral to posterolateral. c. open reduction and plating through an anterolateral approach with meniscal elevation. d. open reduction with screw fixation through a midline anterior approach with tibial tubercle elevation. e. open reduction and plating through an approach between the medial head of the gastrocnemius and the semitenedinosus.

56
Correct Answer: e Lateral plateau fractured 70-80% and medial plateau only 10-20%. This is due to medial plateau being stronger, and when fractured is usually a more violent injury w/more soft tissue injuries (meniscal tear 50%, ligamentatous injury 30%, peroneal neuropraxia, popliteal vessel injury, and compartment syndrome. Schatzker Classification: Type I: Split fx of lateral plateau. Type II: Split depression fx of lateral plateau. Type III: Depression fx of lateral plateau. Type IV: Fracture of medial plateau. Type V: Bicondylar fx. Type VI: Plateau fx w/separation of metaphysis from diaphysis. RX of Types I - IV: lateral L plates, Types V, and VI: ring or hybrid fixator. Rx of Type IV fx cannot be performed by anterior approach and must be exposed directly from posteromedial or posterolateral incisions.

57
Year:1997 Question # 253 A 35-year-old man sustained a comminuted type II open fracture of the humeral shaft associated with a complete radial nerve palsy as a result of a motor vehicle accident. Along with administration of antibiotics and debridement, treatment should include a. skeletal traction, an electromyogram, and nerve conduction studies. b. immediate nerve exploration and application of a hanging arm cast. c. surgical fracture fixation and immediate nerve exploration. d. surgical fracture fixation and nerve exploration if no recovery is apparant after 4 months. e. functional humeral bracing and nerve exploration in four months if no recovery is apparant after 4 months.

58
Correct Answer: c 10-18% incidence. 90% neuropraxia w/95% of these recovering spontaneously within 3-4 months. If no return evident clinically EMG/NCS studies are indicated w/possible delayed exploration. Injury to nerve that occurs during initial fracture management may indicate laceration by bone fragments and should be explored immediately. Other indications for primary exploration are open fx, penetrating injuries, and spiral fx of mid distal 1/3 (Holstein-Lewis Fx).
.")
59
Year:1997 Question # 270 Radiographs of a fracture after a rotational injury are shown in Figure 78. A mortise view shows no widening of the ankle mortise. There is no swelling or tenderness over the medial ankle. Which of the following treatment options will most rapidly and effectively restore ankle function? a. Removable fracture brace, and early mobilization b. Closed reduction and nonweightbearing cast immobilization c. Open reduction and plate fixation of the lateral malleolus d. Open reduction of the lateral malleolus and repair of the torn anterior tibiofibular ligament e. Open reduction of the lateral malleolus, repair of the torn anterior tibiofibular ligament, and repair of the deltoid ligament

61
Year:1997 Question # 272 Figures 79a and 79b show a fracture of the tibia in a 53-year-old woman who fell down stairs. Management consists of closed reduction, casting, and bracing. Which of the following factors is most likely to compromise the outcome? a. Early weightbearing b. Age of the patient c. The intact fibula d. The initial angulation e. Location of the fracture

63
1998

64
Year:1998 Question # 5 A 17-year-old boy who sustained a closed clavicle fracture after he was ejected from an all-terrain vehicle was treated with a figure-of-8 brace 1 year ago. He now reports continuous pain at the site of the fracture and is unable to actively raise his arm above his head. A radiograph is shown in Figure 1. Management should now consist of a. an onlay bone graft. b. electrical stimulation. c. resection of the distal clavicle. d. plate fixation and a bone graft. e. smooth wire fixation and a bone graft.

66
Correct Answer: d The xray here reveals a midshaft non-united clavicle fx. The boy is one year out and intervention of some sort is indicated at this time. The recommended choice at this time is plate fixation with bone graft. Bone graft alone or Kwires will not yield a stable fixation allowing compression and healing.

67
Year:1998 Question # 8 What is the treatment of choice for an adult who has an isolated fracture of the ulna at the junction of the distal and middle thirds, with 5 degrees apex dorsal angulation and a 25% displacement? a. Intramedullary rodding b. Functional bracing c. Closed reduction and a long arm cast d. Closed reduction and application of an external fixator e. Open reduction and internal fixation with a dorsal plate

68
Correct Answer: b Isolated fractures of the mid/distal ulna (nightstick variety) do not always require ORIF as do their radial counterparts. Studies have shown that functional bracing is as effective as ORIF if there is <10degrees angulation and <50% displacement. A long arm cast is not necessary as this only leads to elbow stiffness. These pts should be followed radiographically for progressive displacement which would necessitate ORIF. It is important also to look for associated injuries about the elbow and wrist.
 do not always require ORIF as do their radial counterparts. Studies have shown that functional bracing is as effective as ORIF if there is <10degrees angulation and <50% displacement. A long arm cast is not necessary as this only leads to elbow stiffness. These pts should be followed radiographically for progressive displacement which would necessitate ORIF. It is important also to look for associated injuries about the elbow and wrist.")
69
Year:1998 Question # 26 Which of the following provides the most stable fixation for comminuted fractures of the posterior acetabular wall? a. Cable b. Buttress plate c. Methylmethacrylate d. Multiple lag screws e. Multiple Kirschner wires

70
Correct Answer: b Fractures of posterior wall occur more freq than any other type of acetabular fracture. Nearly 33 % of isolated post. Wall fxs are comminuted. Failure of fixation is devastating complication best prevented by rigid fixation. Often comminuted fractures involve fragments close to post rim such that attempts to fix these with screws or pins would violate the articular surface. Study referenced tested screws alone vs plate/screws (buttress) under wt-bearing conditions and found plate much stronger.
 under wt-bearing conditions and found plate much stronger.")
71
Year:1998 Question # 28 What posterior pelvic ring injury is most commonly associated with neurologic compromise? a. Sacral fracture lateral to the foramina b. Sacral fracture medial to the foramina c. Sacroiliac fracture-dislocation d. Sacroiliac dislocation e. Iliac wing fracture

72
Correct Answer: b Classification of Sacral fractures: Based on direction, location and level of sacral fractures Each type has characteristic clinical presentationsClassification of Sacral Fractures: Zone 1: region of ala Occasionally associated with partial damage to L5 nerve root MOI-lateral compression Zone 2: region of sacral foramina Frequently assoc. with sciatica Zone 3: region of central canal Frequently assoc. with saddle anesthesia and loss of sphincter function High incidence (25%) seen in falls (Jumper`s fx) Routine pelvic x-rays are useless Require: Ferguson views, tomograms or CT scans
 seen in falls (Jumper`s fx) Routine pelvic x-rays are useless Require: Ferguson views, tomograms or CT scans.")
73
Year:1998 Question # 29 A patient has a noncomminuted displaced fracture of the radial head with a distal radioulnar dissociation. What is the most appropriate treatment for the radial head? a. Allograft replacement b. Radioulnar synostosis c. Excision of the radial head d. Open reduction and internal fixation e. Silicone radial head replacement

74
Correct Answer: d Radial head fractures account for 33% elbow fractures MOI-axial load on pronated forearm Mason classification: Type I: non-displaced or minimally displaced ( articular surface < 2mm) Type II: displaced > 2 mm Type III: comminuted, not reconstructable Type IV: fracture plus elbow dislocation Essex-Lopresti: fracture of radial head with DRUJ dissociation. disruption of interosseous membrane Problem with silicone implants-much less stiff than intact interosseous membrane allowing for radial shortening over time. Problem with excision---same, radial shortening with loss of wrist motion In bad Type III fxs, may require excision of head with implant, then if proximal migration of radius occurs pt will require radioulnar synostosis in future but not acutely.
 Type II: displaced > 2 mm Type III: comminuted, not reconstructable Type IV: fracture plus elbow dislocation Essex-Lopresti: fracture of radial head with DRUJ dissociation. disruption of interosseous membrane Problem with silicone implants-much less stiff than intact interosseous membrane allowing for radial shortening over time. Problem with excision---same, radial shortening with loss of wrist motion In bad Type III fxs, may require excision of head with implant, then if proximal migration of radius occurs pt will require radioulnar synostosis in future but not acutely.")
75
Year:1998 Question # 31 Examination of a 45-year-old construction worker who was crushed by falling dirt and buried to midchest level reveals hemodynamic instability; however, radiographs of the chest are normal, and results of a diagnostic peritoneal lavage are negative. Despite the administration of a fluid bolus and packed red blood cells, hemodynamic instability persist. A radiograph of the pelvis is shown on Figure 4. The next step in the management should be a. application of a pelvic external fixator. b. a pelvic sling. c. angiography of the pelvis. d. open reduction and internal fixation. e. open packing of the pelvic hematoma.

77
Correct Answer: a Pelvic ring injuries treatment requirements are related to degree of osseous-ligamentous injury, displacement and treatment requirements are related to degree of osseous-ligamentous injury, displacement and presence of associated pelvic/abd/thoracic/ or head injuries 20% have associated hemodynamic instability 15% mortality rate Algorhythm:

78
Year:1998 Question # 53 Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation? a. Injury to the subclavian artery b. Injury to the brachial plexus c. Segmented fracture d. 100% displacement e. Associated displaced surgical neck fracture of the humerus

79
Correct Answer: a Indications for open reduction/internal fixation of acute clavicle fractures include: Open fracture Skin tenting that fails to respond to closed reduction "Floating shoulder" - Ipsilateral clavicle and unstable scapula fracture Neurovascular injury that is progressive or fails to respond to closed reduction: Brachial plexus injuries do not necessitate ORIF as they are most likely due to stretching of the plexus and unlikely to improve with exploration. If subclavian artery or vein injury is suspected, an anteriogram should be performed. Exploration is mandatory in the event of a torn large vessel. Some type II distal clavicle fractures

80
Year:1998 Question # 56 The Injury Severity Score (ISS), using point scores from five different body systems, is a method that aids in predicting the chances of mortality in a patient with multiple injuries by a. adding the scores in all five body systems. b. adding the squares of the scores in the three most severely injured systems. c. doubling the cumulative scores for head and chest systems. d. combining the scores from the most and least injured systems. e. correcting the score in the most severely injured system for age.
, using point scores from five different body systems, is a method that aids in predicting the chances of mortality in a patient with multiple injuries by. a. adding the scores in all five body systems. b. adding the squares of the scores in the three most severely injured systems. c. doubling the cumulative scores for head and chest systems. d. combining the scores from the most and least injured systems. e. correcting the score in the most severely injured system for age.")
81
Correct Answer: b The Injury Severity Score (ISS) was developed in 1974 to help predict morbidity and mortality of the multiply injured patient and also for purposes of evaluating and directing emergency and subsequent care. Injury scores until that time had failed to take into account the importance of concomitant injuries to different major body systems and their affect on mortality. Poor correlation existed between injury score and mortality. The Injury Severity score was developed as a modification of the Abbreviated Injury Score (AIS) which assesses the severity of injury to each of five different systems (head or neck, face, chest, abdominal or pelvic contents, extremities or pelvic girdle and general). Scores for each system ranged from 0-5. Researchers found that if, instead of taking the cumulative score (as in AIS) the squares of the scores in the three most severely injured systems were added, mortality and morbidity were closely predicted. Highest score possible 75.
 was developed in 1974 to help predict morbidity and mortality of the multiply injured patient and also for purposes of evaluating and directing emergency and subsequent care. Injury scores until that time had failed to take into account the importance of concomitant injuries to different major body systems and their affect on mortality. Poor correlation existed between injury score and mortality. The Injury Severity score was developed as a modification of the Abbreviated Injury Score (AIS) which assesses the severity of injury to each of five different systems (head or neck, face, chest, abdominal or pelvic contents, extremities or pelvic girdle and general). Scores for each system ranged from 0-5. Researchers found that if, instead of taking the cumulative score (as in AIS) the squares of the scores in the three most severely injured systems were added, mortality and morbidity were closely predicted. Highest score possible 75.")
82
Year:1998 Question # 74 A patient sustained a joint depression-type fracture of the calcaneus that healed despite lack of treatment. The loss of dorsiflexion the patient is now experiencing is most likely the result of a. widening and shortening of the heal. b. weakness of the gastrocnemius-soleus complex. c. anterior impingement from a horizontal talus. d. unrecognized compartment syndrome of the foot. e. degenerative arthritis of the tibiotalar joint.

83
Correct Answer: c In a joint depression fracture, the calcaneus is driven upward against the talus by the impact. A fracture line is created that begins in the sinus tarsi near the lateral wall and propagates obliquely across the posterior facet to the medial wall. This fracture line is known as the primary fracture line. Because the posterior facet is no longer under the talus, the talus settles into a position parallel to the ground. Even though the foot is in a neutral position, any attempt to dorsiflex the foot will cause the talar neck to impinge on the anterior aspect of the tibia.

84
Year:1998 Question # 78 Which of the following injuries is most commonly associated with a fracture of the scapular body? a. Vascular injury b. Tear of the rotator cuff c. Injury to the brachial plexus d. Fracture of an upper thoracic rib e. Fracture of the proximal humerus

85
Correct Answer: d 96% of patients had associated injuries, with upper thoracic rib fractures being most common. Most scapular fractures occur as a result of direct impact over the scapular region. Other associated injuries: hemopneumothorax 29%, pulmonary contusion 8%, head injury 34%, ipsilateral clavicle fracture 25%, cervical spine injury 12%. Surgical indications: - scapular neck fractures with more than 40 degrees of angulation in either the transverse or coronal plane, or with 1 cm or more of displacement - greater than 3 to 5 mm step-off of glenoid joint surface - scapular spine fractures at the base of the acromion and those with more than 5 mm displacement may be at risk for the development of a nonunion

86
Year:1998 Question # 80 Figure 16 shows the AP radiograph of a 32-year-old man with a fracture cephalad to the fovea of the femoral heat. A CT scan shows a single head fragment. After closed reduction of the hip, there is 5 mm of residual articular incongruity. Management should now include a. hybrid total hip arthroplasty. b. noncemented hemiarthroplasty of the hip. c. closed reduction and percutaneous pin fixation. d. open reduction through an anterior approach to the hip. e. excision of the head fragment.

88
Correct Answer: d Pipkin classification of femoral head fractures: - Type I: occurs below the fovea - Type II: occurs above the fovea, consequently the blood supply through the foveal artery may be intact - Type III: associated with femoral neck fracture - Type IV: associated with an acetabular fracture - With fractures involving the fovea or involving the superior weightbearing dome, anatomic reduction is mandatory. If this is not achieved through a closed reduction and confirmed by CT, open reduction is carried out through a Smith-Petersen anterior approach to the hip. Stabilization of the fracture through interfragmental screw compression techniques is required.

89
Year:1998 Question # 81 Figure 17a shows the postoperative AP hip radiograph of a 35-year-old woman who sustained an isolated fracture of the femoral neck while skiing 7 months ago. Treatment consisted of open reduction and screw fixation. She now reports continuous pain in the groin and an inability to bear weight. AP and lateral radiographs shown in Figures 17b and 17c reveal no evidence of healing of the fracture. Management at this time should consist of a. a quadratus femoris pedicle bone graft. b. a proximal femoral allograft. c. intertrochanteric osteotomy. d. total hip arthroplasty. e. hip hemiarthroplasty

90
Correct Answer: c An abduction osteotomy at the intertrochanteric level, converts shearing forces into compressive forces. The compression promotes healing of the fracture

91
Year:1998 Question # 84 Which of the following surgical approaches to the hip is associated with the highes incidence of heterotopic ossification? a. Ilioinguinal b. Extended iliofemoral c. Combined ilioinguinal and Kocher-Langenbeck (posterior) d. Kocher-Langenbeck (posterior) e. Kocher-Langenbeck (posterior) with trochanteric osteotomy
 d. Kocher-Langenbeck (posterior) e. Kocher-Langenbeck (posterior) with trochanteric osteotomy.")
92
Correct Answer: b Heterotopic ossification after an acetabular fracture has been shown to be related to the surgical exposure, male sex, associated head injury, and the fracture type. The incidence of Brooker III and IV heterotopic ossification in the Kocher-Langenbeck exposure was 10.5%; for the ilioinguinal exposure, 2%; extended iliofemoral, 35%; combined Kocher-Langenbeck/ilioinguinal exposures, 27%.

93
Year:1998 Question # 108 Which of the following radiographic views best shows the size and displacement of a posterior wall fracture of the acetabulum? a. Inlet view of the pelvis b. Outlet view of the pelvis c. AP view of the hip d. Iliac oblique view (external oblique) of the hip e. Obturator oblique view (internal oblique) of the hip
 of the hip. e. Obturator oblique view (internal oblique) of the hip.")
94
Correct Answer: e Obturator Oblique (internal oblique) inlet view best shows A/P displacement of the pelvis (not acetabulum) outlet view shows superior displacement posteriorly and both superior or inferior displacement anteriorly (PELVIS) AP of hip-shows : 1. Pelvic brimCanterior border of anterior column 2. Ileoischial line- border of posterior column 3. Roof of acetabulum 4. Medial wall of acetabulum 5. Posterior border of acetabulum Iliac oblique (external oblique)-45 degree external rotation with beam centered on hip. Shows posterior column, anterior border of acetabulum and iliac wing Obturator oblique (internal oblique)-elevate affected hip up 45 degrees. Shows obturator foramen, anterior column, posterior lip
 inlet view best shows A/P displacement of the pelvis (not acetabulum) outlet view shows superior displacement posteriorly and both superior or inferior displacement anteriorly (PELVIS) AP of hip-shows : 1. Pelvic brimCanterior border of anterior column 2. Ileoischial line- border of posterior column 3. Roof of acetabulum 4. Medial wall of acetabulum 5. Posterior border of acetabulum Iliac oblique (external oblique)-45 degree external rotation with beam centered on hip. Shows posterior column, anterior border of acetabulum and iliac wing Obturator oblique (internal oblique)-elevate affected hip up 45 degrees. Shows obturator foramen, anterior column, posterior lip.")
95
Year:1998 Question # 113 Figure 25a shows the initial postoperative AP radiograph, and FIgures 25b and 25c show the current AP and lateral radiographs of a 46-year-old woman who underwent open reduction and internal fixation of a distal fibula fracture and placement of a syndesmosis screw 15 months ago. She has full function, but the ankle swells with activity. Th radiographs reveal that a. fixation of the syndesmosis has failed. b. widening of the ankle mortise has led to failure of fixation. c. infection around the syndesmosis screw has led to osteomyelitis. d. the syndesmosis screw is broken. e. motion between the tibia and fibula has caused loosening of the syndesmosis screw

97
Correct Answer: e 1. fixation failure is incorrect because the mortise is not wide 2. mortise is not widened 3. osteomyelitis would not have the uniform sclerotic margin 4. the screw isn=t broken 5. only three cortices are crossed and this allows motion at the syndesmosis which causes the lucency References:

98
Year:1998 Question # 127 A healed fracture of the tibia that demonstrates 25 degrees apex posterior angulation and 28 degrees varus angulation on AP and lateral radiographs is most accurately described as a a. complex deformity with angulation in two planes. b. single deformity less than 20 degrees, apex posterolateral. c. single deformity greater than 30 degrees, apex posterolateral. d. single deformity less than 20 degrees, apex posterolmedial e. single deformity greater than 30 degrees, apex posteromedial

99
Correct Answer: c Single deformity greater than 30deg, apex posterolateral. To accurately describe post-traumatic long bone deformities (fractures, malunions or nonunions) with regards to angulation and/or translation it is important to realize that the actual deformity is rarely in a pure apex anterior, posterior, valgus of varus direction. Instead the true plane of the apex is tangential to the points of reference given by the radiographs. This plane, described as the apex of the deformity, can be precisely calculated using trigonometric formulae or crudely assessed by extrapolating from two films at 90deg to each other (AP & lat). For example, a tibial angulation that appears apex posterior on the lateral view and in varus on the AP is actually a single deformity with a posterolaterally directed apex. Similarly, an apex that is anterior and valgus is not two separate deformities but rather a single deformity with an apex that is directed anteromedially. The true angle of this deformity is always greater than that seen on either the AP or lateral views; there are mathematical tables available for determining this, or you can estimate. Finally, angulation and translation should be regarded and described separately since they are often in different planes.
 with regards to angulation and/or translation it is important to realize that the actual deformity is rarely in a pure apex anterior, posterior, valgus of varus direction. Instead the true plane of the apex is tangential to the points of reference given by the radiographs. This plane, described as the apex of the deformity, can be precisely calculated using trigonometric formulae or crudely assessed by extrapolating from two films at 90deg to each other (AP & lat). For example, a tibial angulation that appears apex posterior on the lateral view and in varus on the AP is actually a single deformity with a posterolaterally directed apex. Similarly, an apex that is anterior and valgus is not two separate deformities but rather a single deformity with an apex that is directed anteromedially. The true angle of this deformity is always greater than that seen on either the AP or lateral views; there are mathematical tables available for determining this, or you can estimate. Finally, angulation and translation should be regarded and described separately since they are often in different planes.")
100
Year:1998 Question # 134 Which of the following methods of treatment of a displaced Lisfranc fracture-dislocation will most reliably lead to good functional results? a. Weightbearing short leg cast b. Nonweightbearing short leg cast c. Removable splint and early motion d. Open reduction and internal fixation e. Elastic compression bandage with full weightbearing

101
Correct Answer: d lisfranc injuries occur at the midfoot with damage to the articulation between the metatarsals and cuneiforms. The Lisfanc ligament courses obliquely between the second metatarsal and medial cuneiform. As many as 95% of patients with Lisfanc joint dislocations have been shown to have associated metatarsal fractures. Fractures of the midtarsal bones (cuneiforms, cuboid and navicular) have been seen in up to 39% of these patients. Diagnosis requires adequate radiographs (AP, lateral and oblique films) with close attention to anatomic relationships. The medial border of the second metatarsal should line up with the medial border of the middle cuneiform on the AP film while the medial border of the fourth metatarsal should be aligned with the medial border of the cuboid on the oblique film. Nondisplaced fractures without ligament instability (stress radiographs) can be treated in non-weightbearing cast for six weeks. In displaced or unstable injuries, open anatomic reduction and fixation is indicated. With severe comminution, the tarsometatarsal joints within the medial column can be fused acutely.
 have been seen in up to 39% of these patients. Diagnosis requires adequate radiographs (AP, lateral and oblique films) with close attention to anatomic relationships. The medial border of the second metatarsal should line up with the medial border of the middle cuneiform on the AP film while the medial border of the fourth metatarsal should be aligned with the medial border of the cuboid on the oblique film. Nondisplaced fractures without ligament instability (stress radiographs) can be treated in non-weightbearing cast for six weeks. In displaced or unstable injuries, open anatomic reduction and fixation is indicated. With severe comminution, the tarsometatarsal joints within the medial column can be fused acutely.")
102
Year:1998 Question # 144 A patient is in respiratory distress as a result of a high-speed motor vehicle accident. After emergency intubationm the arterial blood is poorly oxygenated, and examination shows left-sided trachael deviation, absence of breath sounds on the right sidem and tympany on percussion over the right side of the chest. Management should include a. positive-pressure ventilation. b. an immediate radiograph of the chest. c. adjustment of the position of the endotrachael tube. d. insertion of a large-bore needle into the pericardial space. e. insertion of a large-bore needle in the right second intercostal space, midclavicular line

103
Correct Answer: e These are classic signs of a tension pneumothorax. A tension PTX results when there is damage to the lung parenchyma allowing inspired air to escape into the pleural space. This leads to an increase in intrapleural pressure and a shift in the mediastinum to the contralateral side, resulting in narrowing or occlusion of the vena cava at the diaphragm. Immediate thoracic decompression is mandatory to prevent death. This is performed by placing a large-bore needle into the second intercostal space in the midlavicular line . This should be followed immediately by tube thoracostomy

104
Year:1998 Question # 145 The axial stability of a 4-pin uniplanar external fixator used to treat a patient who has a transverse midthird fracture of the tibia with a 5-mm fracture gap can be most greatly increased by a. allowing the ends of the fracture to touch. b. adding a second connecting bar. c. adding one pin to each fracture fragment. d. increasing the pin diameter from4 mm to 6 mm. e. decreasing the connecting bar-to-bone distance from 6 cm to 4 cm.

105
Correct Answer: a Bone contact allows load sharing between bone and fixator for compressive, torsional, and certain bending loads. Without bone contact, the external fixator must support full load, and this can have a significant effect on fracture healing. With transverse fx`s, application of compression across the fracture site can greatly increase the stiffness of the frame-bone system.

106
Year:1998 Question # 157 Figure 35 shows the postoperative radiograph of a femur fracture proximal to a total knee prosthesis that was treated by open reduction and plate fixation 9 months ago. What is the most likely reason the previously well-seated screw has backed out of the central portion of the plates? Infection Nonunion Improper screw length Osteonecrosis of the distal fragment Use of a cortical screw instead of a cancellous screw

108
Correct Answer: b Failure of fx healing is the most common clinical complication of fx`s. The factors that influence fx healing differ from case to case. Morphologic studies of ununited fx`s have described 2 different types of nonunions: (1) those with unmineralized fibrous and fibrocartilaginous tissue bridging the fx gap, and (2) those with a cleft or gap between the ends of the fx`d bone, which are usually covered with similar fibrous tissue or fibrocartilage. The former situation, which is clinically the more common one, is called a nonunion; the latter is called pseudarthrosis. An analysis of 95 human tissue specimens of nonunions and pseudarthroses demonstrated that in extraarticular fx`s, all cases of delayed healing are first nonunions. Subsequently, microscopic clefts may appear within the tissues that compose the nonunion, and, in time and only in certain cases, a dominant cleft may propagate to form a practically complete separation of the fx ends, ie., pseudarthrosis. *See attached article
 those with unmineralized fibrous and fibrocartilaginous tissue bridging the fx gap, and (2) those with a cleft or gap between the ends of the fx`d bone, which are usually covered with similar fibrous tissue or fibrocartilage. The former situation, which is clinically the more common one, is called a nonunion; the latter is called pseudarthrosis. An analysis of 95 human tissue specimens of nonunions and pseudarthroses demonstrated that in extraarticular fx`s, all cases of delayed healing are first nonunions. Subsequently, microscopic clefts may appear within the tissues that compose the nonunion, and, in time and only in certain cases, a dominant cleft may propagate to form a practically complete separation of the fx ends, ie., pseudarthrosis. *See attached article.")
109
Year:1998 Question # 192 To prevent injury to the posterior interosseous nerve during the approach for reduction and fixation of a fracture of the radial head, anterior retraction should be performed with the forearm maximally pronated and the elbow extended. b. maximally pronated and the elbow flexed. c. maximally supinated and the elbow flexed. d. maximally supinated and the elbow extended. e. in neutral rotation, with the elbow extended.

110
Correct Answer: b The posterior interosseous nerve is vulnerable to injury during the posterolateral approach to the radial head as it winds around the neck of the radius within the substance of the supinator muscle. Maximal pronation and flexion at the elbow moves the nerve medially out of the operative field so that the supinator and the underlying joint capsule can be incised without danger.

111
Year:1998 Question # 213 In patients older than age 50 years who experience shoulder dislocation or proximal humerus fracture, the incidence of associated neurologic abnormality documented by electromyogram is as high as 10% b. 20% c. 50% d. 70% e. 90%

112
Correct Answer: C Several complications can occur with glenohumeral dislocations and humeral neck fractures including rotator cuff tear, vascular injuries, osteonecrosis, and nerve injuries. When diagnosed by EMG the incidence of axillary and other types of nerve lesions is 20-30% for all age groups. Blom and Dahlback found that patients over 50 are considerably more affected. In this age range the incidence of nerve injury documented by EMG may be as high as 50% (23 of 53 patients).
.")
113
Year:1998Question # 241 A 37-year-old laborer sustained a fracture of the posterior acetabular wall. Two years following operative management, the patient reports severely limited hip motion, and back pain. Radiographs reveal extensive mature heterotopic ossification with preservation of the hip joint space. Management should now consist of resection arthroplasty and local radiation. b. in situ fusion of the hip. c. excision of heterotopic bone, total hip arthroplasty, and oral indomethacin. d. excision of heterotopic bone, and local radiation. e. excision of heterotopic bone, hemiarthroplasty, and oral indomethacin.

114
Correct Answer: d The use of various prophylactic measures to decrease the incidence of ectopic bone formation has been reported in the literature. One suggested approach is to minimize surgical osteotomies and the amount of subperiosteal stripping and pericapsular trauma during operation. Many surgeons seek to maximize the use of the ilioinguinal and Kocher-Langenbeck approaches. these approaches, however, remain inadequate for certain T shaped and both column fractures, as well as old fractures that require the extended iliofemoral approach for reduction. Another approach to prophylactic therapy is low dose radiation immediately after hip surgery; several authors have reported success in reducing the incidence and severity of HO. Prophylactic use of diphosphonate to reduce the amount of ectopic bone formation after total hip arthroplasty has been shown to be ineffective. Diphosphonate compounds prevent mineralization of the osteoid matrix, but not the production of the matrix. Moreover, diphosphonate must be administered systemically, and mineralization of the osteoid can proceed once it is discontinued. Anti-inflammatory drugs such as indomethacin, ibuprofen, and fluriprofen have been shown to be potentially effective in reducing ectopic bone formation and appear to present fewer risks compared to other forms of prophylactic therapy. However, well designed, prospective, controlled studies are needed go evaluate the long term effects of these drugs. It is important to note that there are four factors found to highly correlate with Grade 1 ectopic bone formation were identified and may be considered predictive of Grade 1 HO. They are: 1) the extended iliofemoral approach; 2) multiple (two or more) perifracture operative findings; 3) T type fractures; and 4) the presence of associated injuries to the chest and abdomen. The incidence of HO in patients with these risk factors can be greater than 30% with greater than 8% developing restriction of hip motion.
 the extended iliofemoral approach; 2) multiple (two or more) perifracture operative findings; 3) T type fractures; and 4) the presence of associated injuries to the chest and abdomen. The incidence of HO in patients with these risk factors can be greater than 30% with greater than 8% developing restriction of hip motion.")
115
Year:1998 Question # 255 Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head? Lateral Y b. Scapular AP c. Neutral rotation AP d. Internal rotation AP e. External rotation AP

116
Correct Answer: d A Hill-Sachs lesion is found in greater than 80% of the patients with recurrent anterior dislocations. The lesion is found at the posterolateral margin of the humeral articular surface. The lesion will have articular cartilage lateral to it and a raw, cancellous surface. The normal sulcus will be smooth with vascular channels. The Hill-Sachs lesion is best viewed with the arm in marked internal rotation with an AP radiograph of the shoulder. This places the lesion in the most visible view by rotating the lesion out laterally from behind the humeral head. A scapular AP view places the scapula flat on the plate of the cassette. This view shows the glenohumeral joint space well, and will also show fractures of the humerous and glenoid lip.

117
Year:1998 Question # 258 Following closed reduction for the injury shown in Figures 69a and 69b, treatment should consist of repair or reconstruction of the medial collateral ligament. b. repair or reconstruction of the medial and lateral collateral ligaments. c. immobilization for 5 days or less. d. immobilization for 14 days. e. immobilization for 25 days.

118
Correct Answer: c Elbow dislocation is commonly due to a fall on the outstretched hand and is the second most common dislocation to shoulder dislocation. Articular injuries occur in 25-50% of these injuries. Clinically with stress tests and in surgical exploration, it has been shown that the medial collateral ligament is damaged in ALL fracture-dislocations. Residual calcification has been show to occur in the substance of the medial coll. Ligament in 85% of patients, and in the lat coll lig in 75% of cases. Desired treatment is reduction and early range of motion. If there is instability, an arc of motion in the stable ranges should be initiated should begin within 5 days and should continue for 1 week. Gradual resumption of flexion and extension should continue for 3-4 weeks. A fracture-dislocation should be treated with immediate fracture elbow reduction, and repair of the fracture according to its own characteristic. Prolonged immobilization should be avoided at all costs. Residual flexion contractures should be treated with a hyperextension splint at night with physical rehabilitation. Surgical repair/intervention in simple dislocations (ie no fracture) has been shown to have worse results than nonoperative intervention with less flexion contracture being observed in the nonoperative groups. 10% compared to 15%. Therefore, in the nonathlete, early reduction and early ROM is the preferred mode of therapy.
 has been shown to have worse results than nonoperative intervention with less flexion contracture being observed in the nonoperative groups. 10% compared to 15%. Therefore, in the nonathlete, early reduction and early ROM is the preferred mode of therapy.")
119
Year:1998 Question # 273 The radiographs shown in Figures 71a through 71c, and the CT scan shown in Figure 71d reveal an acetabular fracture that should be classified as t-type. b. both column. c. transverse. d. anterior column. e. anterior column posterior hemitransverse.

121
Correct Answer: b Acetabular fractures are classified in the following manner: Type A Partial Articular One Column · A1-posterior wall · A2-posterior column · A3-Anterior wall and/or anterior column Type B Partial Articular Transverse Oriented Fracture · B1-Tranverse + posterior wall · B2-T-types · B3-Anterior with posterior hemitransverse Type C Complete Articular, Both Column Fracture Both columns are fractured, and all articular segments including the roof are detached from the remaining segment of ilium. This is the "FLOATING ACETABULUM", which is s form of T-fracture with the horizontal limb proximal to the acetabulum. · C1-both column with ant column fracture extending to iliac crest (high variety) · C2-both column with ant. column fracture extending to the anterior border of the ilium (low variety) · C3-both column, ant fracture enters the SI joint Image 71c shows an obturator oblique view which clearly shows an anterior column fracture and that the ilium is separated from the acetabulum. Figure 71b is and iliac oblique which shows the posterior column fracture and a significant protrusio, the classic spur sign is also seen in this figure.
 · C2-both column with ant. column fracture extending to the anterior border of the ilium (low variety) · C3-both column, ant fracture enters the SI joint Image 71c shows an obturator oblique view which clearly shows an anterior column fracture and that the ilium is separated from the acetabulum. Figure 71b is and iliac oblique which shows the posterior column fracture and a significant protrusio, the classic spur sign is also seen in this figure.")
122
Year:1998 Question # 274 What is the most common nerve injury following a Monteggia fracture-dislocation of the forearm in adults? Posterior interosseous b. Anterior interosseous c. Radial d. Median e. Ulnar

123
Correct Answer: a Monteggia Fracture consists of an ulna fracture associated with dislocation of the radial head. It occurs <5% of all forearm fractures. Bado classified Monteggia fractures: Type 1- Anterior dislocation of the radial head with anteriorly angulated fracture of the ulna Type II- Posterior dislocation of the radial head with posterior angulated fracture of the ulna Type III-Lateral or anterolateral dislocation of the radial head with a fracture of the ulnar metaphysis Type IV-Anterior dislocation of the radial head with a fracture of the radius and ulna The most common nerve injury involved in Moteggia`s fractures involve the deep branch of the radial nerve or the posterior interosseous nerve. The usual course is is spontaneous recovery, and exploration is not warranted unless full function does not return within 6-8 weeks. However, a good neurologic exam is warranted prior to reduction attempts. Several cases of post. interosseous entrapment have been documented where the nerve is actually wrapped around the radial head and impedes reduction. The answer given, posterior interosseous, is a branch of the radial nerve, and is the most common neurologic structure damaged in a Monteggia fracture. The anterior interosseous can be damaged but is not very common. The radial, median and ulnar nerves proper are rarely involved.

124
Year:1998 Question # 275 Which of the following conditions is associated with the highest mortality rate in patients with a pelvic fracture? Shock from hypovolemia Associated rupture of the bladder Arterial bleeding on pelvic angiogram Presence of a hematoma in the perineum and scrotum Fractures of both the anterior and posterior pelvic ring

125
Correct Answer: a Pelvic fracture patients outcome has been shown to be directly linked to degree of hemodynamic instability. Mortality rates were 3.4% in stable patients versus 42% in unstable patients. It should also be noted that the patients who were hemodynamically unstable were older, had more severe pelvic trauma, greater multisystem trauma, and, as expected, much higher mortality. Therefore, the primary goal in initial management of trauma victims (not just with pelvic fractures) is hemodynamic stability
 is hemodynamic stability.")
126
2001

127
Year:2001 Question # 1 A 49-year-old man has a persistent Trendelenburg gait after undergoing open reduction and internal fixation of a posterior wall acetabular fracture 6 months ago. The radiographs reveal a normal joint space with no heterotopic ossification and no signs of osteonecrosis. Weakenss in what muscle group is the most likely cause of his limp? Gluteus maximus Gluteus medius Tensor fascia lata Iliopsoas Vastus lateralis

128
Correct Answer: b References:Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, Lippincott Williams & Wilkins, 1984, pp
: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, Lippincott Williams & Wilkins, 1984, pp")
129
Year:2001 Question # 8 After plating of a both-bone forearm fracture in an adult, which of the following actions is most important to achieve maximal forearm rotation? Early motion Surgery within 7 days Restoration fo the radial bow Compression fixation of both bones Repair of the interosseous ligament

130
Correct Answer: c References:Schemitsch EH, Richards RR: The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. JBJS Am 1992;74:

131
Year:2001 Question # 27 Which of the following is considered a typical feature of a T-type acetabular fracture? Disruption of the iliac wing Disruption of the obturator ring A spur sign Secondary congruence Predominantly anterior column displacement

132
Correct Answer: b References:Letournel E, Judet R: T-shaped fractures, in Fractures of the Acetabulum. Springer-Verlag, 1981, pp Saterbak AM, Marsh JL, Brandser E, Turbett T: Acetabular fractures classification of Letournel and Judet: A systematic approach. Iowa Orthop J 1995;15:

133
Year:2001 Question # 31 A 30-year-old man sustained multiple injuries in a motor vehicle accident, including bilateral femoral shaft fractures a pelvic ring fracture, and a floating right elbow. Following stabilization of the life-threatening injuries, treatment of the right humerus should consist of closed reduction and application of a cast closed reduction and placement of a reamed humeral nail closed reduction and percutaneous pinning open reduction and internal fixation application of an external fixation device

134
Correct Answer: d References:Johnson KD: Management of fractures of the femur,tibia, and upper extremity in the multiply injured patient. Instr Course Lect 1990;39: Dabezies EJ, Banta CJ II, Murphy CP, d`Ambrosia RD: Plate fixation of the humeral shaft for acute fractures, with and without radial nerve injuries. J Orthop Trauam 1992;6:10-13.

135
Insufficient fluid resuscitation Unrecognized spinal trauma
Year:2001 Question # 36 A 23-year-old woman who was struck by a motor vehicle has a Glasgow Coma Scale score of 15 and a systolic blood pressure of 110mm Hg on arrival in the emergency department. Examination reveals a rotationally unstable pelvic ring injury and multiple long bone fractures. Initial management consists of IV administration of 3L of lactated Ringer`s solution over 2 hours. Reexamination now reveals that the patient is tachycardic and her systolic blood pressure has dropped to 60mmHg. What is the most likely cause of this event? Insufficient fluid resuscitation Unrecognized spinal trauma Unrecognized brain injury Myocardial infarction Failure to stabilize the pelvic ring injury

136
Correct Answer: a References:Browner BD, Jupter JB, Levine AM, Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp
: Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp")
137
Year:2001 Question # 50 A 19-year-old man sustained multiple puncture wounds to his side, neck, and posterior and anterior chest wall following explosion of a homemade pipe bomb 6 weeks ago. The patient now reports difficulty with overhead activity. Examination reveals loss of scapular stability with the scapula retracted and the inferior pole rotated medially. Winging is increased with attempts to elevate the arm. Electromyography confirms the diagnosis of what type of nerve palsy? Spinal accessory Suprascapular Long thoracic Axillary Musculocutaneous

138
Correct Answer: c References:Connor PM, Yamaguchi K, Manifold SG, Pollock RG, Flatow EL, Bigliani LU: Split pectoralis major transfer for serratus anterior palsy. Clin Orthop 1997;341:

139
Year:2001 Question # 64 What nerve is most commonly injured during an ilioinguinal approach to the acetabulum? Femoral ilioinguinal obturator L5 nerve root lateral femoral cutaneous

140
Correct Answer: e References:Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp
: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp")
141
Year:2001 Question # 74 Which of the following is considered a contraindication to the treatment of a humeral shaft fracture with functional bracing? Radial nerve palsy Transverse fracture Distal third fracture Low-velocity gunshot fracture Ipsilateral brachial plexus palsy

142
Correct Answer: e References:Brien WW, Gellman H, Becker V, Garland DE, Waters RL, Wiss DA: Managment of fractures of the humerus in patients who have an injury of the ipsilateral brachial plexus. JBJS Am 1990;72: Sarmiento A, Zagorski JA, Zych GA, Latta LL, Capps CA: Functional bracing for the treatment of fractures of the humeral diaphysis. JBJS Am 2000;82:

143
Year:2001 Question # 82 Which of the following factors will have the greatest affect on the stability of the hip after closed reduction of a posterior wall fracture-dislocation? Magnitude of the posterior capsular disruption Length of time until reduction occurs Size of the wall fragment Presence of femoral head depression Presence of loose bodies in the fovea of the hip joint

144
Correct Answer: c References:Beaty JH (ed): OKU 6, Rosemont, IL, AAOS, 1999, pp Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. JBJS Am 1996;78:
: OKU 6, Rosemont, IL, AAOS, 1999, pp Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. JBJS Am 1996;78:")
145
Year:2001 Question # 123 What type of major pelvic ring injury has the greatest average transfusion requirement? Lateral compression Vertical sheer Anteroposterior compression Fractures through the sacrum Fractures through the iliac wing

146
Correct Answer: c References:Turen CH, Dube MA, LeCroy MC: Approach to the polytraumatized patient with musculoskeletal injuries. J Am Acad Orthop Surg 1999;7: Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma 1989;29:

147
Year:2001 Question # 124 Where does the nutrient artery to the tibia most commonly enter the bone? Aneriorly above the pes anserinus Anteriorly 4 cm above the ankle Laterally above the fibular head Posteriorly below the posterior cruciate ligament insertion Posterior in the medial malleolus

148
Correct Answer: d References:Brinker MR, Cook SD, Dunlap JN, Christakis P, Elliot MN: Early changes in nutrient artery blood flow following tibial nailing with and without reaming: A preliminary study. J Orthop Trauma 1999;13:

149
Year:2001 Question # 129 Which of the following is considered the most important factor in fracture healing in adults? Age of the patient Gender of the patient Neurologic status of the extremity Blood supply Fracture pattern

150
Correct Answer: d References:Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, AAOS, 2000, pp
: Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, AAOS, 2000, pp")
151
Year:2001 Question # 142 When treating tibial plateau fractures, the most important reason that proximal tibial transfixation wires should be placed at least 14 mm from the articular surface is to obtain good fixation in subchondral bone allow radiographic visualization of the joint reduction minimize the risk that septic arthritis will develop increase the range of knee flexion compress the articular fragments

152
Correct Answer: c References:DeCoster TA, Crawford MK, Kraut MA: Safe extracapsular placement of proximal tibia transifxation pins. JOT 1999;13: Reid JS, Van Slyke MA, Moulton MJ, Mann TA: Safe placement of proximal tibial transifxation wires with resepct to intracapsular penetration. JOT 2001;15:10-17

153
Year:2001 Question # 150 What structures are located within the femoral canal as it passes beneath the inguinal ligament? Femoral artery, femoral vein, and femoral nerve Femoral artery and femoral vein Femoral artery, femoral vein, and lymphatics Femoral artery, femoral vein, femoral nerve, and lymphatics Internal iliac artery, internal iliac vein, and femoral nerve

154
Correct Answer: c References:Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp
: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp")
155
Year:2001 Question # 161 A 35-year-old laborer sustains an irreparable fracture of the radial head after falling 12 feet. Examination reveals tenderness at the elbow and wrist and pain with manipulation of the distal radioulnar joint. In addition to resection of the radial head, management should include hinged bracing of the elbow. immobilization in a long arm cast. prosthetic replacement of the radial head. repair of the distal radioulnar joint. application of a hinged external fixator.

156
Correct Answer: c References:Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp Hotchkiss RN, An KN, Sowa DT, Basta S, Weiland AJ: An anatomic and mechanical study of the interosseous membrane of the forearm: Pathomechanics of proximal migration of the radius. J Hand Surg Am 1989;14:
: Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp Hotchkiss RN, An KN, Sowa DT, Basta S, Weiland AJ: An anatomic and mechanical study of the interosseous membrane of the forearm: Pathomechanics of proximal migration of the radius. J Hand Surg Am 1989;14:")
157
Year:2001 Question # 173 What portion of the calcaneus typically maintains a normal relationship to the talus in displaced intra-articular calcaneus fractures? Sustentaculum tali Tuberosity Anterolateral Posterior facet Lateral wall

158
Correct Answer: a References:Olexa TA, Ebraheim NA, Haman SP: The sustentaculum tali: Anatomic, radiographic, and surgical considerations. Foot and Ankle Int 2000;21: Sanders R: Intra-articular fractures of the calcaneus: Present state of the art. J Orthop Trauma 1992;6:

159
Year:2001 Question # 179 What is the most likely cause of mortality within the first 48 hours in patients who sustain a pelvic fracture from a lateral compression mechanism? Aortic rupture b. Pelvic arterial injury c. Pelvic venous injury d. Hollow viscous injury e. Head injury

160
Correct Answer: e References:Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resusitative requirements, and outcome. J Trauma 1989;29:

161
Year:2001 Question # 190 Concurrent injuries to which of the following structures results in an increased osteogenic response to fracture? Head Liver Chest Major artery Bladder

162
Correct Answer: a References:Kushwaha VP, Garland DG: Extremity fractures in the patient with a traumatic brain injury. J Am Acad Orthp Surg 1998;6: Spencer RF: The effect of head injury on fracture healing: A quantitative assessment. J Bone Joint Surg Br 1987;69:

163
Year:2001 Question # 199 When compared to plate fixation, antegrade intramedullary nailing of humeral shaft fractures results in better elbow function. a higher rate of union. a higher rate of complications. a higher rate of infection. longer surgical time.

164
Correct Answer: c References:Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999; 13: McCormack RG, Brien D, Buckley RE, McKee MD, Powell J, Schemitsch EH: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail:A prospective randomized trial. J Bone Joint Surg Br 2000;82:

165
Year:2001 Question # 202 An ankle fracture heals with an anatomically aligned mortise and 2 mm of displacement of the distal fibula fracture. What affect will these findings have on the tibiotalar joint? Decreased contact loading Increased contact loading Increased external rotation Increased medial-lateral translation Normal loading, rotation, and translation

166
Correct Answer: e References:Brown TD, Hurlbut PT, Hale JE, et al: Effects of imposed hindfoot constraint on ankle contact mechanics for displaced lateral malleolar fractures. J Orthop Trauma 1994;8: Michelson JD: Fractures about the ankle. J Bone Joint Surg Am 1995;77:

167
Year:2001 Question # 211 Which of the following factors has been shown to be an independent risk factor for infection after open reduction and internal fixation of the calcaneus through an extensile lateral incision? Age of greater than 50 years History of smoking A comminuted posterior facet Extension of the fracture into the sustentaculum Use of phenytoin

168
Correct Answer: b References:Folk JW, Starr AJ: Early wound complications of operative treatment of calcaneus fractures: Analysis of 190 fractures. J Orthop Trauma 1999;13:

169
Year:2001 Question # 215 In the treatment of femoral shaft fractures, the lowest union rate has been reported after which of the following types of nailing? Reamed antegrade locked Reamed antegrade unlocked Reamed retrograde locked Unreamed antegrade locked Unreamed retrograde locked

170
Correct Answer: e References:Moeb BR, Watson JT, Cramer KE, Karges DE, Teefey JS: Unreamed retrograde intramedullary nailing of fractures of the femoral shaft. J Orthop Trauma 1998;12: Moeb BR, Watson JT: Retrograde intramedullary nailing, without reaming, of fractures of the femoral shaft in multiply injured patients. J Bone Joint Surg Am 1995;77:

171
Year:2001 Question # 218 A 35-year-old man sustained an isolated closed displaced bicondylar tibial plateau fracture after being struck by a car. Reduction and internal fixation of both condyles can be most safely achieved using which of the following surgical approaches? Isolated anterior midline Isolated lateral parapatellar Isolated posteromedial Combined anterolateral and posteromedial Combined anterior midline and posterior transpopiteal

172
Correct Answer: d References:Georgiadis GM: Combined anterior and posterior approaches for complex tibial plateau fixations. J Bone Joint Surg Am 1989;71:

173
Year:2001 Question # 225 Which of the following is considered the most important factor in preventing failure of fixation of displaced femoral neck fractures? Use of a compression screw and side plate Use of cannulated screws Accuracy of reduction Reduction on a traction table Release of a capsular hematoma

174
Correct Answer: c References:Chua D, Jaglal SB, Schatzker J: Predictors of early failure of fixation in the treatment of displaced subcapital hip fractures. J Orthop Trauma 1998;12: Swiontkowski MF: Intracapsular fractures of the hip. J Bone Joint Surg Am 1994;76:

175
Year:2001 Question # 228 What type of knee dislocation is most likely to be irreducible by closed means? Posterior Anterior Lateral Posterolateral Posteromedial

176
Correct Answer: d References:Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp Quinlan AG, Sharrard WJW: Posterolateral dislocation of the knee with capsular interposition. J Bone Joint Surg Br 1958;40:
: Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp Quinlan AG, Sharrard WJW: Posterolateral dislocation of the knee with capsular interposition. J Bone Joint Surg Br 1958;40:")
177
Year:2001 Question # 233 In trauma patients older than 60 years, mortality most closely correlates with the injury severity score (ISS). the extremity abbreviated injury score (AIS). the need for orthopaedic surgery. the timing of orthopaedic surgery. a history of type I diabetes mellitus.
. the extremity abbreviated injury score (AIS). the need for orthopaedic surgery. the timing of orthopaedic surgery. a history of type I diabetes mellitus.")
178
Correct Answer: a Tornetta G, Mostafavi H, Riina J, et al: Morbidity and morality in elderly trauma patients. J Trauma 1999;46:

179
Year:2001 Question # 237 What is the most common complication at a minimum of 1 year after treatment with a reamed antegrade nail for a femoral shaft fracture? Nonunion Malunion Trendelenburg gait Hip discomfort Osteonecrosis of the femoral head

180
Correct Answer: d References:Bain GI, Zacest AC, Paterson DC, Middleton J, Pohl AP: Abduction strength following intramedullary nailing of the femur. J Orthop Trauma 1997;11:93-97.

181
Year:2001 Question # 249 A varus malreduction of a comminuated talar neck fracture will result in varus hindfoot and decreased subtalar motion. increased contact loading of the posterior facet. subtalar instability. anterior ankle impingement. talonavicular subluxation.

182
Correct Answer: a References:Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78: Sangeozan BJ, WagnerUA, HArrington RM, Tencer AF: Contact characteristics of the subtalar joint: The effects of talar neck misalignment. J Orthop Res 1992;10:

183
Year:2001 Question # 255 The poor results following surgical treatment of posterior wall acetabular fractures are most commonly associated with sciatic nerve injury. articular comminution. heterotopic ossification. deep venous thrombosis. osteonecrosis of the femoral head.

184
Correct Answer: b References:Browner BD, Jupiter JB, Levine AM, Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders 1998, pp Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 1996;78: Saterbak AM, Marsh JL, Nepola JV, Brandser EA, Turbett T: Clinical failure after posterior wall acetabular fractures: The influence of initial fracture patterns. J Orthop Trauma 2000;14:
: Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders 1998, pp Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 1996;78: Saterbak AM, Marsh JL, Nepola JV, Brandser EA, Turbett T: Clinical failure after posterior wall acetabular fractures: The influence of initial fracture patterns. J Orthop Trauma 2000;14:")
185
Year:2001 Question # 257 When comparing women who sustained a pelvic ring fracture with women who have multiple injuries without a pelvic ring fracture, those with a pelvic ring fracture have been found to have a higher subsequent rate of miscarriage. infertility. depression. failure to achieve physiologic sexual arousal. urinary difficulties.

186
Correct Answer: e References:Copeland CE, Bosse MJ, McCarthy ML, et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.

187
Year:2001 Question # 270 During intramedullary tibial nailing, compartment pressures in the leg are most elevated by the use of reaming. continuous traction. a medial starting point. a lateral starting point. a solid nail.

188
Correct Answer: b References:Shakespeare DT, Henderson NJ: Compartmental pressure changes during calcaneal traction in tibial fractures. J Bone Joint Surg Br 1982;64: McQueen MM, Christie J, Court-Brown CM: Compartment pressures after intramedullary nailing of the tibia. J Bone Joint Surg Br 1990;72:

189
2002

190
Year:2002 Question # 8 When performing open reduction and internal fixation of a displaced fracture of the scapular neck, which of the following peripheral nerves is at the greatest risk of injury? Axillary Musculocutaneous Upper Subscapular Radial Dorsal scapular

191
Correct Answer: a Anatomically the axillary nerve wraps underneath the glenoid, through the quadrangular space (a frequent test question!!!) and then laterally to innervate the deltoid. The posterior approach to the shoulder (which is usually how you fix the scapula) goes b/t the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve). Excessive traction on the teres minor can cause damage to the axillary nerve. The quadrangular space is made up of the teres minor (superior), the Long head of the triceps (medial), the humerus (lateral) and the teres major (inferior) and the axillary nerve and the posterior humeral circumflex artery run in this space.
 and then laterally to innervate the deltoid. The posterior approach to the shoulder (which is usually how you fix the scapula) goes b/t the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve). Excessive traction on the teres minor can cause damage to the axillary nerve. The quadrangular space is made up of the teres minor (superior), the Long head of the triceps (medial), the humerus (lateral) and the teres major (inferior) and the axillary nerve and the posterior humeral circumflex artery run in this space.")
192
Year:2002 Question # 45 A patient with an isolated femur fracture has an injury severity score (ISS) of 9. A patient with bilateral femur fractures and no other injuries has an ISS of 9 16 18 25 81
 of 9. A patient with bilateral femur fractures and no other injuries has an ISS of")
193
Correct Answer: 1 This question is interesting because it attempts to see if you have a rudamentary knowledge of the ISS system. They don`t expect you to know the actual numbers - just the concepts. The ISS incorporates anatomic indices w/ severity indices.The ISS uses injury severity developed in the abbreviated injury scale (AIS)(AIS-90). The ISS uses the highest AIS-90 score from the three most severely injured anatomic areas for any given patient. These AIS-90 values (1 to 5) are each squared, and then summed for a total ISS score. For example, a patient with a flail chest has an AIS-90 thorax of 4, a closed femur fracture AIS-90 skeletal system of 3, a ruptured spleen AIS-90 abdomen of 4; the ISS score for this patient would be 41. The ISS considers only the highest AIS-90 score from any single anatomic site. This decreases the ability of this score to predict injury severity in patients with multiple injuries within the same anatomic area. Nonetheless, the ISS has become an important predictor of injury severity and mortality and is one of the national standards for injury severity assessment. An ISS of 16 or more has been shown to be associated with a mortality of 10%
(AIS-90). The ISS uses the highest AIS-90 score from the three most severely injured anatomic areas for any given patient. These AIS-90 values (1 to 5) are each squared, and then summed for a total ISS score. For example, a patient with a flail chest has an AIS-90 thorax of 4, a closed femur fracture AIS-90 skeletal system of 3, a ruptured spleen AIS-90 abdomen of 4; the ISS score for this patient would be 41. The ISS considers only the highest AIS-90 score from any single anatomic site. This decreases the ability of this score to predict injury severity in patients with multiple injuries within the same anatomic area. Nonetheless, the ISS has become an important predictor of injury severity and mortality and is one of the national standards for injury severity assessment. An ISS of 16 or more has been shown to be associated with a mortality of 10%")
194
Year:2002 Question # 59 Which of the following factors has the greatest influence on achieving a good outcome following surgical treatment of tibial plateau fractures? obtaining anatomic reduction of the articular surface restoring mechanical alignment and stability using minimally invasive stabilization techniques initiating early knee range of motion intiating early weight bearing

195
Correct Answer: b Despite old studies claims that anatomic articular reduction is of the utmost importance to good outcome in tibial plateau fractures, newer better research focusing on functional outcomes suggest that as much as 5mm of articular step off may be acceptable and much more important is that there be no malalignment or residual instability of the tibia. It is not uncommon for recent studies on tibial plateau fractures to suggest that a step-off of £2 mm in the articular surface, even under the lateral meniscus, is necessary to achieve a good outcome. However, a number of studies have indicated that articular incongruity following a tibial plateau fracture, particularly a lateral plateau injury, is well tolerated and that the amount of articular congruity plays a small role in determining the outcome following management of these fractures. Effect of Factors Other than Articular Reduction Instability of the knee has been shown by many investigators to be strongly associated with a poor clinical outcome Malalignment of the proximal part of the tibia with the shaft also contributes to a poor outcome following a tibial plateau fracture. Rasmussen 36 found that osteoarthritis had developed in nineteen (13%) of 146 patients with proximal tibial valgus angulation of <10° at seven years of follow-up, whereas it had developed in six of eleven patients with valgus angulation of >10°. Varus angulation of any amount was poorly tolerated. Meniscal injury is frequently associated with a tibial plateau fracture, with a reported prevalence of 20% to 47% 47,48 . Either medial or lateral meniscectomy at the time of surgical treatment of a tibial plateau fracture is strongly associated with a high prevalence of osteoarthritis and a poor outcome 37,44
 of 146 patients with proximal tibial valgus angulation of <10° at seven years of follow-up, whereas it had developed in six of eleven patients with valgus angulation of >10°. Varus angulation of any amount was poorly tolerated. Meniscal injury is frequently associated with a tibial plateau fracture, with a reported prevalence of 20% to 47% 47,48 . Either medial or lateral meniscectomy at the time of surgical treatment of a tibial plateau fracture is strongly associated with a high prevalence of osteoarthritis and a poor outcome 37,44.")
196
Year:2002 Question # 67 A healthy cognitively intact 70 year old woman sustains an unstable intertrochanteric fracture that is stabilized with a well placed sliding hip screw. Allowing immediate unrestricted weight bearing will result in a decreased time to functional return an increased risk of postoperative hip dislocation an increased risk of sideplate breakage an increased risk of implant cutout an increased risk of wound healing problems

197
Correct Answer: a The answer is clear, the faster you get an elderly individiual ambulating the better. The question tells you that the fracture was stabilised with a WELL PLACED sliding screw. Early ambulation would provude a compressive force to the fracture speeding the healing process. All of this in addition to the multitude of medical benfits from early mobilisation (dec PE, dec MI etc..)References:Koval KJ, Aharonoff GB, Su ET, Zuckerman JD. Effect of acute inpatient rehab on outcome after fracture of the femoral neck or intertroch fractures. JBJS 1998;80:
References:Koval KJ, Aharonoff GB, Su ET, Zuckerman JD. Effect of acute inpatient rehab on outcome after fracture of the femoral neck or intertroch fractures. JBJS 1998;80:")
198
Year:2002 Question # 75 In an obtunded patient with a tibial fracture and suspected compartment syndrome, fasciotomy should be performed when intracompartment pressure are > 30mm Hg > 40mm Hg within 40mm Hg of systolic pressure within 30 mm Hg of diastolic pressure within 30 mm Hg of mean arterial blood pressure

199
Correct Answer: d Compartment syndrome is an elevation of interstitial pressure in closed fascial compartment that results in microvascular compromise. Necrosis of tissue may begin at interstitial pressure as low as 30 mm. Many surgeon use 30 mm Hg as the cut off for performing fasciotomy. compartment measurements within 20 mm Hg of diastolic pressure is an indication for fasciotomy (DBP - compartment pressure is a relative indicator of tissue perfusion). Measurements should be taken as close to the fracture site as possible to achieve the highest readings. Clinical signs/symptoms: pain out of proportion, pain with passive ROM, pallor, paresthesias, loss of pulses. References:McQueen MM:Compartment monitoring in tibial fractures JBJS 1998;78: Nassif JM: Effect of acute reamed vs unreamed IMN on compartment syndrome when traeating closed tibial shaft fractures. JOT 2000;14:
. Measurements should be taken as close to the fracture site as possible to achieve the highest readings. Clinical signs/symptoms: pain out of proportion, pain with passive ROM, pallor, paresthesias, loss of pulses. References:McQueen MM:Compartment monitoring in tibial fractures JBJS 1998;78: Nassif JM: Effect of acute reamed vs unreamed IMN on compartment syndrome when traeating closed tibial shaft fractures. JOT 2000;14:")
200
Year:2002 Question # 108 What is the best indication for intramedullary nailing of the humerus? Impending pathologic fracture from metastatic disease Open fracture Closed fracture with and associated femur fracture Closed fracture with radial nerve palsy Nonunion of a midshaft fracture

201
Correct Answer: 1 Indications for surgical management of humeral shaft fractures: open fracture, except low-energy handgun wound; associated vascular injury; floating elbow; segmental fracture; pathologic fracture; bilateral humeral fractures; humeral fracture in polytrauma patient; neurologic loss after lacerating injury; neurologic loss during closed fracture alignment; inability to maintain acceptable alignment; displaced intra-articular fracture extension. Indications for use of IM nails include segmental fractures in which plate placement would require considerable soft-tissue dissection, fractures in osteopenic bone, pathologic fractures, and humeral shaft fractures in polytrauma patients who may need to use the injured arm for mobilization and ambulation. A randomized prospective study comparing intramedullary nails versus plates demonstrated no statistically significan differences in healing outcomes assessed between humeral diaphyseal fractures treated with IM nails and those treated with plates. Antegrade IM nails were associated with a higher incidence of shoulder pain and stiffness. Plating was associated with a higher incidence of elbow pain and stiffness as well as slightly higher incidence of nonunion and infection.References:Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, AAOS, 2002, pp Chapman JR, Hanley MB, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. JOT 2000;14:162-6.
: Orthopaedic Knowledge Update 7. Rosemont, IL, AAOS, 2002, pp Chapman JR, Hanley MB, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. JOT 2000;14:")
202
Year:2002 Question # 123 Nonsurgical management is most appropriate for which of the following transverse patellar fractures? Nondisplaced fracture in an active 25 y/o laborer who can perform a straight leg raise Minimally displaced fracture in a 40 y/o patient who cannot perrform a straight leg raise Displaced fracture in an 80 y/o retired farmer Displaced fracture in a patient on renal dialysis Displaced fracture in a patient with diabetes mellitus

203
Correct Answer: A Nonsurgical treatment is indicated for all nondisplaced patellar fx and for minimally displaced fractured associated with an intact extensor mechanism. The latter group includes patients with 2-3 mm of fx displacement as well as patients with extra articular distal fractures and intact ability to perform a straight leg raise. Surgical treatment has become the accepted standard for the management of displaced patellar fractures, and fractures that have no extensor mechanism (straight leg raise).
.")
204
Year:2002 Question # 155 A 19-year-old man is combative, confused, and requires intubation after a motor vehicle accident. An AP radiograph of the pelvis reveals 3cm of symphyseal separation and bilateral anterior widening of the sacroiliac joints. Abdominal ultrasound reveals no obvious pathology. After administration of IV crystalloid, the patient is normotensive. What is the most appropriate next step in management? External fixation of the pelvis Open reduction and Internal fixation of the pubic symphysis CT of the head CT of the abdomen Exploratory laparotomy

205
Correct Answer: C This question goes back to basic ATLS. While the obvious answer to the open book pelvis (for definitive management) is external fixation or ORIF, the more pressing issue is the patients overall condition. After establishing the ABC`s (intubated, on a ventilator, and normotensive), the secondary survey ensues. The abdominal US serves in this regard to rule out any gross abdominal abnormalities (free fluid, etc) and is a tool becoming more often utilized acutely instead of CT. This is discussed in the referenced chapter from OKU 6. Since there is no obvious pathology and the patient is stable, answer d and e are not correct. Any mental status changes warrants ruling out of intracranial abnormalities in the acute setting. This is best done with a head CT.
 is external fixation or ORIF, the more pressing issue is the patients overall condition. After establishing the ABC`s (intubated, on a ventilator, and normotensive), the secondary survey ensues. The abdominal US serves in this regard to rule out any gross abdominal abnormalities (free fluid, etc) and is a tool becoming more often utilized acutely instead of CT. This is discussed in the referenced chapter from OKU 6. Since there is no obvious pathology and the patient is stable, answer d and e are not correct. Any mental status changes warrants ruling out of intracranial abnormalities in the acute setting. This is best done with a head CT.")
206
Year:2002 Question # 158 Following surgical treatment of an intertrochanteric femur fracture with a fixed angle dynamic hip screw, what factor has the greatest effect on the rate of implant cutout? Length of the side plate Length of the barrel Angle of the device Use of a compression screw Tip-apex distance

207
Correct Answer: E Cutout is related most strongly to the distance of the screw tip from the chondral surface. The length of the side plate and barrel have no bearing on this nor does the angle of the device. Compression screw has not been shown to affect failure of the implant. The 2nd reference is a paper that investigates 19 DHS screw cutouts. The tip-apex distance is the sum of the distance from the tip of the screw to the apex of the femoral head on an AP and a lateral (the 2 are added). In the article, the average distance for those that did not cut out was 24 mm compared to 38 mm in the cutout group. There was a strong relationship between and increasing tip-apex distance and rate of cutout. Thus, the ideal position of the screw tip is around 1 cm from the joint.References:OKU Trauma 2 Baumgaertner MR et al: The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. JBJS 1995;77:
. In the article, the average distance for those that did not cut out was 24 mm compared to 38 mm in the cutout group. There was a strong relationship between and increasing tip-apex distance and rate of cutout. Thus, the ideal position of the screw tip is around 1 cm from the joint.References:OKU Trauma 2 Baumgaertner MR et al: The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. JBJS 1995;77:")
208
Year:2002 Question # 169 A 40yo man who sustained multiple injuries in a MVC is in class III hemorrhagic shock. Which of the following findings would be most likely to be present in this patient ? normal mental status normal systolic blood pressure urine output of 15 ml/hr respiratory rate of 20 breaths/min pulse rate of less than 100 beats/min

209
Correct Answer: c SHOCK EBL(% bld vol) P SBP UOP(ml/hr) Class I- <750cc (15% BV) <100 nl >30 Class II cc (15-30%) >100 nl ClassIII cc(30-40%) >120 decr 5-15 Class IV- >2000cc (40%) >140 decr negligible Some KEY POINTS !! -Normotensive pelvic injury patients have a 3% mortality; patients with a SBP <90 have a 38% mortality rate. -Most pelvic bleeding is venous (90% cancellous bone & retroperitoneal lumbar venous plexus). -Most common pelvic arterial injury at time of angio is internal pudendal artery. -APC pelvic injuries are associated with signif greater transfusion requirements than LC injuries.References:Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): OKU: Trauma 2. Rosemont, IL, AAOS, p
 P SBP UOP(ml/hr) Class I- <750cc (15% BV) <100 nl >30 Class II cc (15-30%) >100 nl ClassIII cc(30-40%) >120 decr 5-15 Class IV- >2000cc (40%) >140 decr negligible Some KEY POINTS !! -Normotensive pelvic injury patients have a 3% mortality; patients with a SBP <90 have a 38% mortality rate. -Most pelvic bleeding is venous (90% cancellous bone & retroperitoneal lumbar venous plexus). -Most common pelvic arterial injury at time of angio is internal pudendal artery. -APC pelvic injuries are associated with signif greater transfusion requirements than LC injuries.References:Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): OKU: Trauma 2. Rosemont, IL, AAOS, p")
210
Year:2002 Question # 189 A 23 year old man sustains a nondisplaced clavicle fracture and an ipsilateral scapular neck fracture with 1 cm of displacement. Definitive treatment should consist of nonsurgical management open reduction and internal fixation of the clavicle open reduction and internal fixation of the scapula open reduction and internal fixation of the scapula and clavicle resection of the acromioclavicular joint

211
Correct Answer: 1 Up until recent studies showing that nonoperative tx for floating shoulder injuries with minimal displacement did well all of these injuries were treated with open reduction and internal fixation of the simple fracture (clavicle or scapula depending on pattern). The perceived risks until recently were abduction weakness, decreased range of motion, chronic pain, malunion, and nonunion with nonoperative treatment. These risks have been shown as less a concern than suspected with recent studies from Edwards showing comparable results to ORIF for floating shoulder injuries. The superior shoulder suspensatory complex is an osseous and soft-tissue ring supported by superior and inferior osseous struts. This ring is composed of the glenoid process, the coracoid process, the coracoclavicular ligament, the distal part of the clavicle, the acromioclavicular joint, and the acromial process. The superior strut is the middle part of the clavicle, and the inferior strut is the lateral part of the scapular body and the scapular spine.References:1. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, Il, American Academy of Orthopaedic Surgeons, 2002, pp Edwards SG: Nonoperative treatment of ipsilateral fractures of the scapula and clavicle. JBJS Am 2000; 82:
. The perceived risks until recently were abduction weakness, decreased range of motion, chronic pain, malunion, and nonunion with nonoperative treatment. These risks have been shown as less a concern than suspected with recent studies from Edwards showing comparable results to ORIF for floating shoulder injuries. The superior shoulder suspensatory complex is an osseous and soft-tissue ring supported by superior and inferior osseous struts. This ring is composed of the glenoid process, the coracoid process, the coracoclavicular ligament, the distal part of the clavicle, the acromioclavicular joint, and the acromial process. The superior strut is the middle part of the clavicle, and the inferior strut is the lateral part of the scapular body and the scapular spine.References:1. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, Il, American Academy of Orthopaedic Surgeons, 2002, pp Edwards SG: Nonoperative treatment of ipsilateral fractures of the scapula and clavicle. JBJS Am 2000; 82:")
212
Year:2002 Question # 199 A young healthy patient sustains a severe crush injury resulting in a comminuted midshaft tibia fracture and an 8 * 10 cm medial soft-tissue difect with exposed bone. There is no associated vascular injury. Which of the following procedures will most predictably result in successful coverage? Split thickness skin graft Fasciocutaneous flap Soleus Flap Gastrocnemius flap Free Tissue transfer

213
Correct Answer: 5 Gustillo/Anderson GIIIB or higher injuries of the tibia has been Rotational flaps for the proximal 1/3 of the tibia (Gastroc specifically), Rotational flap (Soleus specifically) or free flap for fractures of the middle third, and free flap for fractures of the distal third. Obviously these guidelines were not hard and fast, and other local wound characteristics needed to be considered (i.e vasc. supply, infection, size of defect, etc.) but these principles could and probably still can be generalized to treatment of these tibial wounds. Therefore most of us should have narrowed this question down to choice 3 and 5, because the other flaps do not provide the coverage needed (i.e. muscle over bone in choice 1 and 2), or their vascular pedicle and location makes it a poor choice for midshaft tibia soft tissue coverage (i.e choice 4). To come to the final answer of choice five the reference article below reports that in their study the treatment of an acute traumatic soft-tissue defect of the tibia, a free flap is significantly less likely to have a short-term wound complication than is treatment with a rotational flap. This is why the answer is choice 5. It does bring up the question of whether this is applicable to the proximal tibia because it is implied in there study, however I have found conflicting data regarding coverage of the proximal tibia and imagine that this would not be on the test. For the proximal tibia rotational flaps and free flaps are both viable options, although trends seem to be going towards free flaps. Remember: free flaps is always the choice for middle and distal third tibial coverage, and would be the likely choice for proximal as well, although controversial.
, Rotational flap (Soleus specifically) or free flap for fractures of the middle third, and free flap for fractures of the distal third. Obviously these guidelines were not hard and fast, and other local wound characteristics needed to be considered (i.e vasc. supply, infection, size of defect, etc.) but these principles could and probably still can be generalized to treatment of these tibial wounds. Therefore most of us should have narrowed this question down to choice 3 and 5, because the other flaps do not provide the coverage needed (i.e. muscle over bone in choice 1 and 2), or their vascular pedicle and location makes it a poor choice for midshaft tibia soft tissue coverage (i.e choice 4). To come to the final answer of choice five the reference article below reports that in their study the treatment of an acute traumatic soft-tissue defect of the tibia, a free flap is significantly less likely to have a short-term wound complication than is treatment with a rotational flap. This is why the answer is choice 5. It does bring up the question of whether this is applicable to the proximal tibia because it is implied in there study, however I have found conflicting data regarding coverage of the proximal tibia and imagine that this would not be on the test. For the proximal tibia rotational flaps and free flaps are both viable options, although trends seem to be going towards free flaps. Remember: free flaps is always the choice for middle and distal third tibial coverage, and would be the likely choice for proximal as well, although controversial.")
214
Year:2002 Question # 207 A 19-year-old man sustains an isolated, displaced transcervical femoral neck fracture in a motor vehicle accident. An urgent closed reduction attempt in the operating room results in ersidual varus angulation and 1 cm of displacement. Appropriate management should now consist of in situ fixation. bipolar hemiarthroplasty. total hip arthroplasty. open reduction and internal fixation. in situ fixation and bone grafting.

215
Correct Answer: 4 Fractures of the femoral neck in young patients are extremely rare. The results of treatment are poorer than octogenarians. In addition, the force required to fracture the femoral neck in young patients is much higher than in the old and represents and high-angle, shear-type frature that extends to the lesser tuberosity. As expected, the rates of non-union (0- 65%) and AVN (19- 90%) are higher. It is imperative to fix these ASAP, within 8-12 hours, depending on the author. If closed reduction fails to restore anatomic alignment, proceed to open reduction through an anterior approach. If closed recution is successful, the fracture is internally fixed with multiple cannulated screws or 6.5 mm A-O cancellous screws.
 and AVN (19- 90%) are higher. It is imperative to fix these ASAP, within 8-12 hours, depending on the author. If closed reduction fails to restore anatomic alignment, proceed to open reduction through an anterior approach. If closed recution is successful, the fracture is internally fixed with multiple cannulated screws or 6.5 mm A-O cancellous screws.")
216
Year:2002 Question # 217 A 32-year-old man has a displaced radial head fracture with an associated posterolateral elbow dislocation. Examination reveals pain and swelling throughout the elbow, forearm, and wrist. In addition to closed redution of the elbow dislocation, management should include a long arm cast. a hinged elbow brace. an external fixator with articulated hinge. radial head resection. open reduction and internal fixation of the radial head

217
Correct Answer: e Pain throughout his forearm and wrist represents an injury to the interosseous membrane (IOM) and DRUJ, a variant of the Essex-Lopresti lesion. (The original Essex- Lopresti lesion was described as a radial head fracture and DRUJ disruption without an associated elbow dislocation.) You need to restore the lateral buttress proximally to retain axial stability of the forearm, either with ORIF of the radial head or else metal or allograft head implant. If you do not restore the buttress, proximal migration of the radius can occur. Temporary pin fixation of the DRUJ in neutral position may be added to neutralize the tendency toward proximal migration. None of the other choices restore the proximal buttress of the radius.
 and DRUJ, a variant of the Essex-Lopresti lesion. (The original Essex- Lopresti lesion was described as a radial head fracture and DRUJ disruption without an associated elbow dislocation.) You need to restore the lateral buttress proximally to retain axial stability of the forearm, either with ORIF of the radial head or else metal or allograft head implant. If you do not restore the buttress, proximal migration of the radius can occur. Temporary pin fixation of the DRUJ in neutral position may be added to neutralize the tendency toward proximal migration. None of the other choices restore the proximal buttress of the radius.")
218
Year:2002 Question # 220 A 24-year-old man sustains a displaced trancervical femoral neck fracture and is treated with multiple cannulated screws. Five months after the injury, the patient reports continued hip pain and is unable to bear weight. Sequential radiographs and a CT scan reveal 10 deg. of varus angualtion. Management should now consist of continued obsevation with weight bearing. valgus intertrochanteric osteotomy. bipolar hemiarthroplasty. electrical stimulation. cancellous autologous bone grafting to the femoral neck

219
Correct Answer: b References:Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71: Kellam JF, Fischer TJ, Tonetta P III, Bosse MHJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp
: Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp")
220
Year:2002 Question # 262 What type of displaced unstable posterior pelvic ring injury will benefit most from open reduction and internal fixation? Transforaminal sacral fracture Sacral alar fracture Iliac fracture Sacroiliac fracture-dislocation Sacroiliac dislocation

221
Correct Answer: 5 Pure sacroiliac lesions are associated with poor outcomes, especially of exact reduction is not achieved. Fractures of the iliac wing, sacroiliac fracture-dislocation, or mixed fractures with SI propagation have the best prognoses, but the outcomes do not correlate to the quality of reduction. References:Starr AJ: Long-term functional prognosis of posterior injuries in high-energy pelvic disruption. J Orthop Trauma 1998;12: Koval KJ (ed): OKU 7. Rosemont, IL, AAOS, 2002, pp
: OKU 7. Rosemont, IL, AAOS, 2002, pp")
Similar presentations
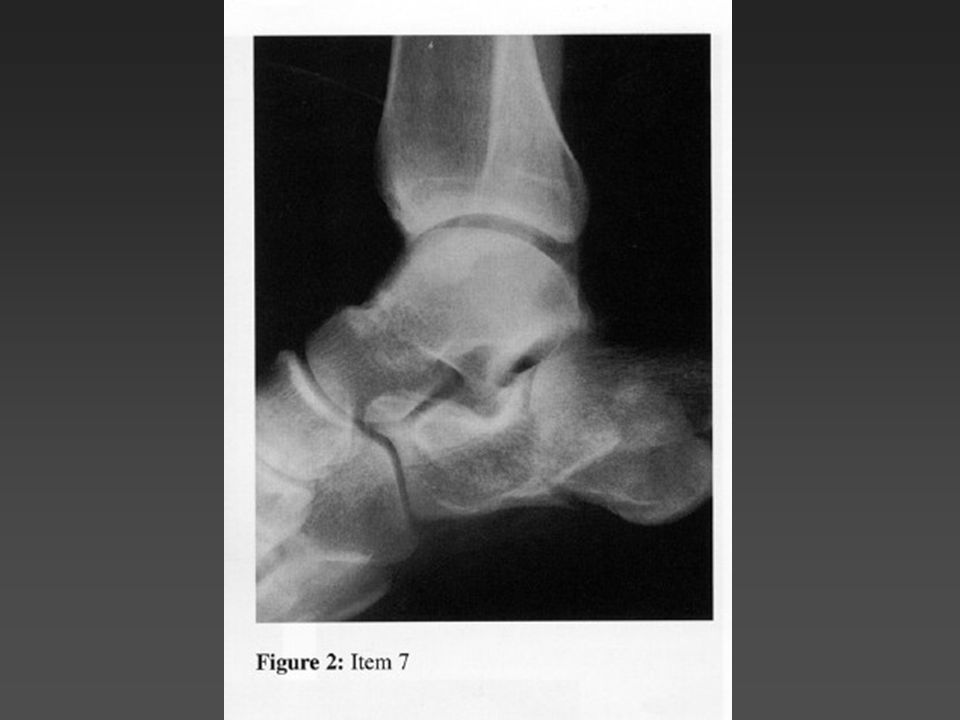






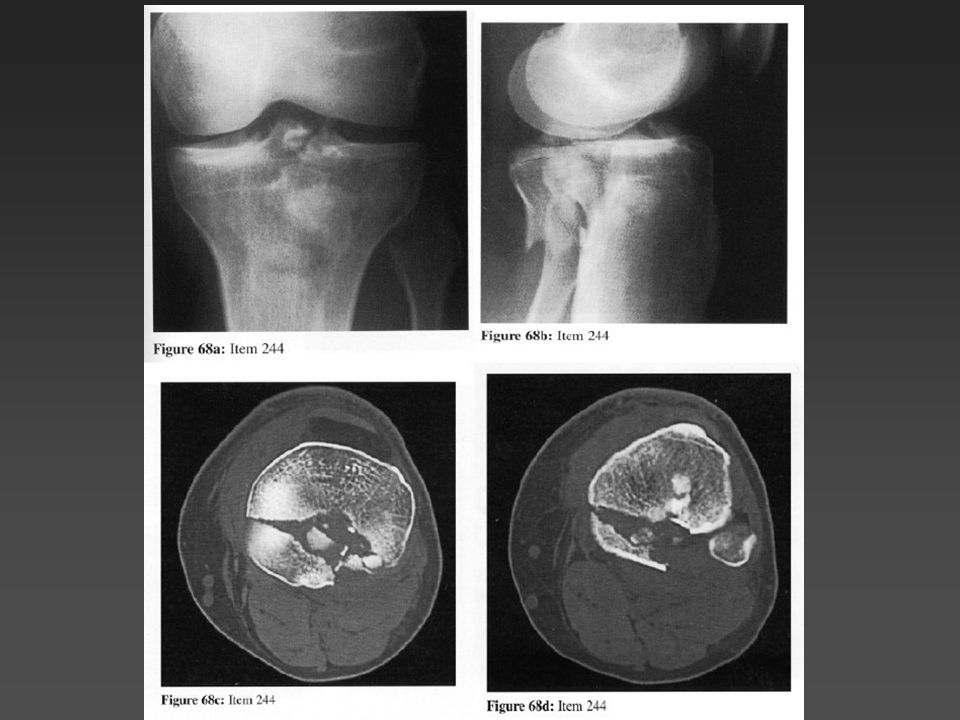

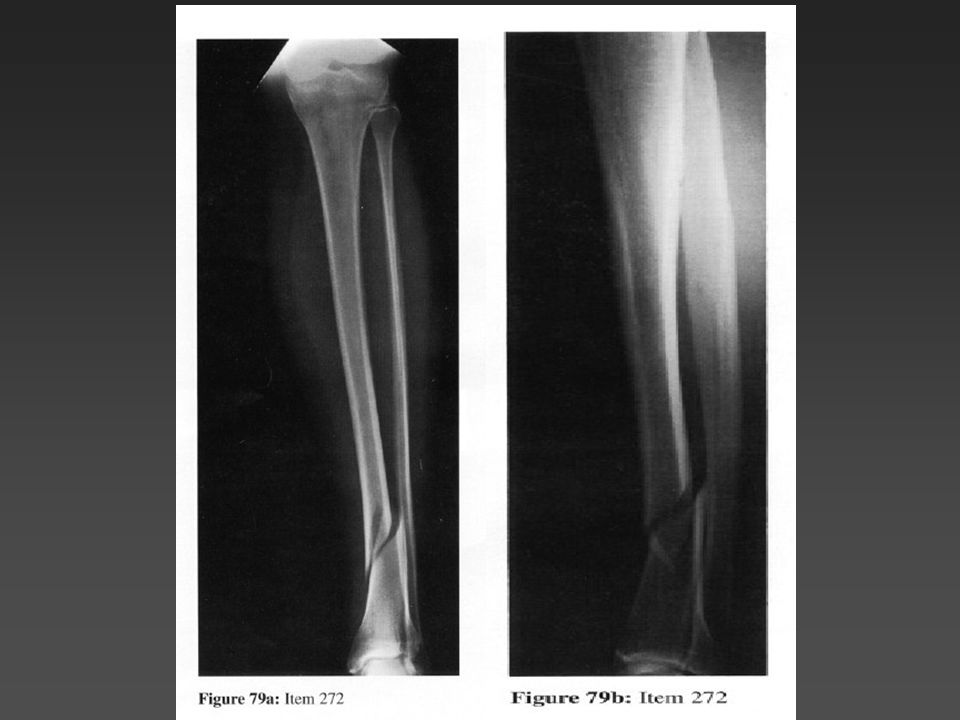
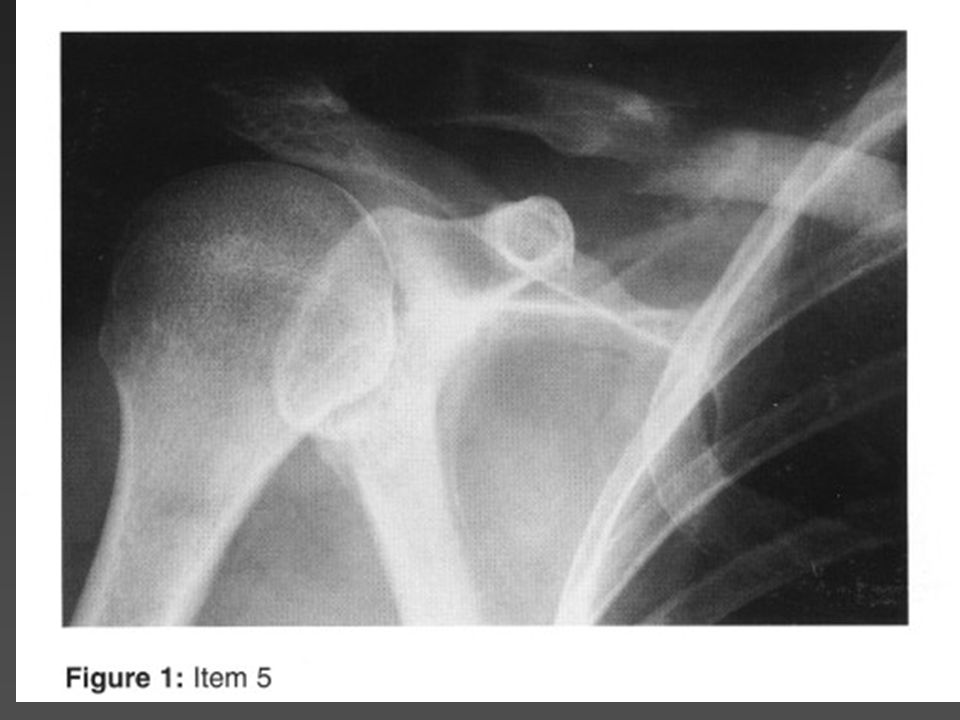
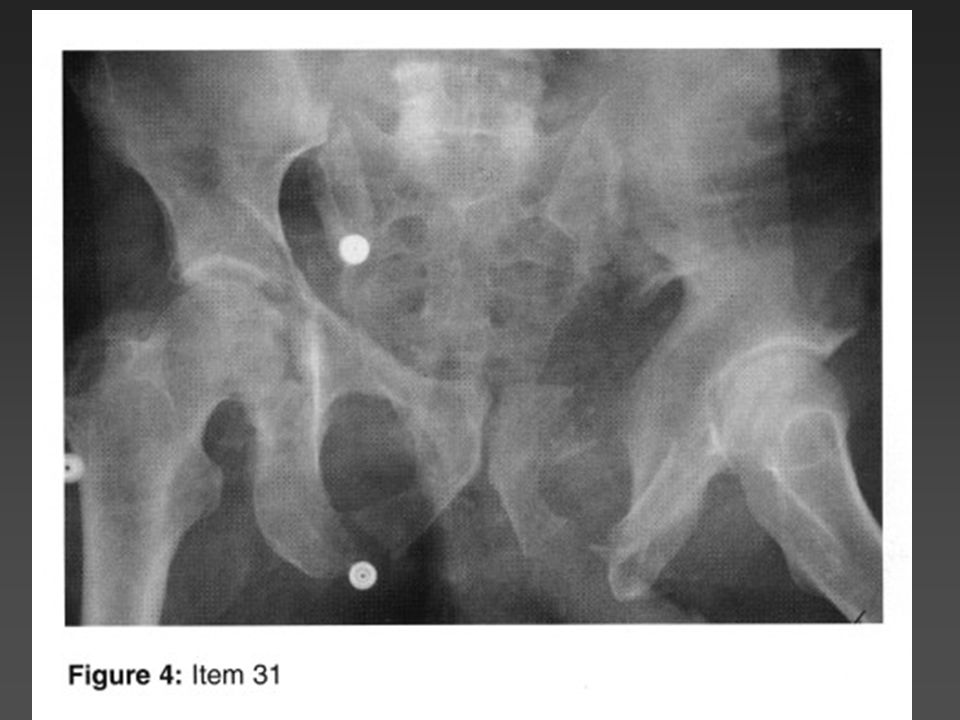

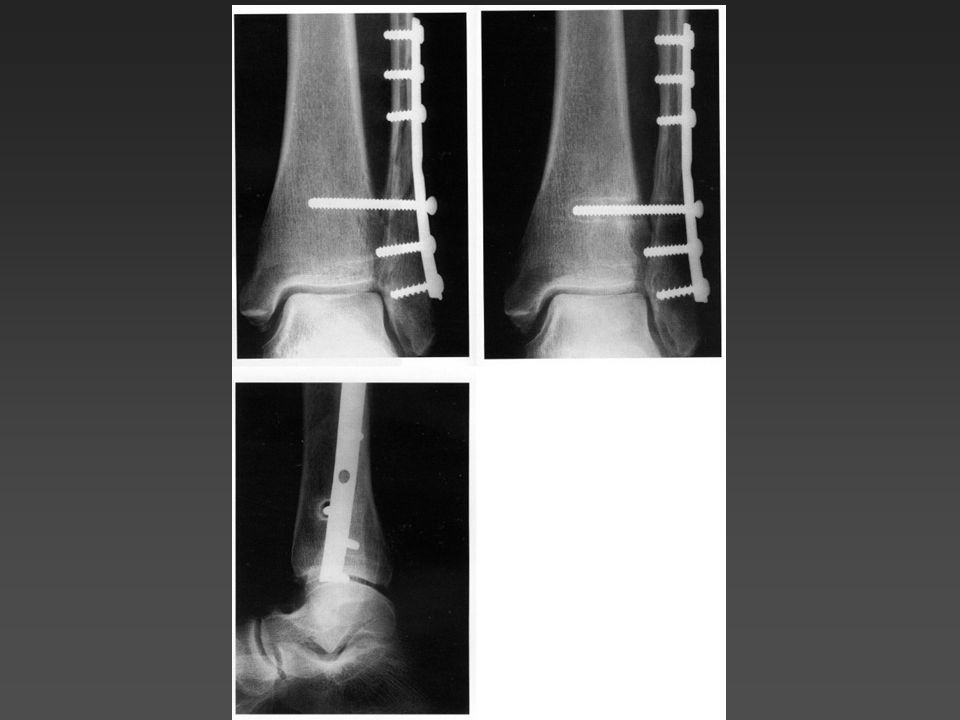

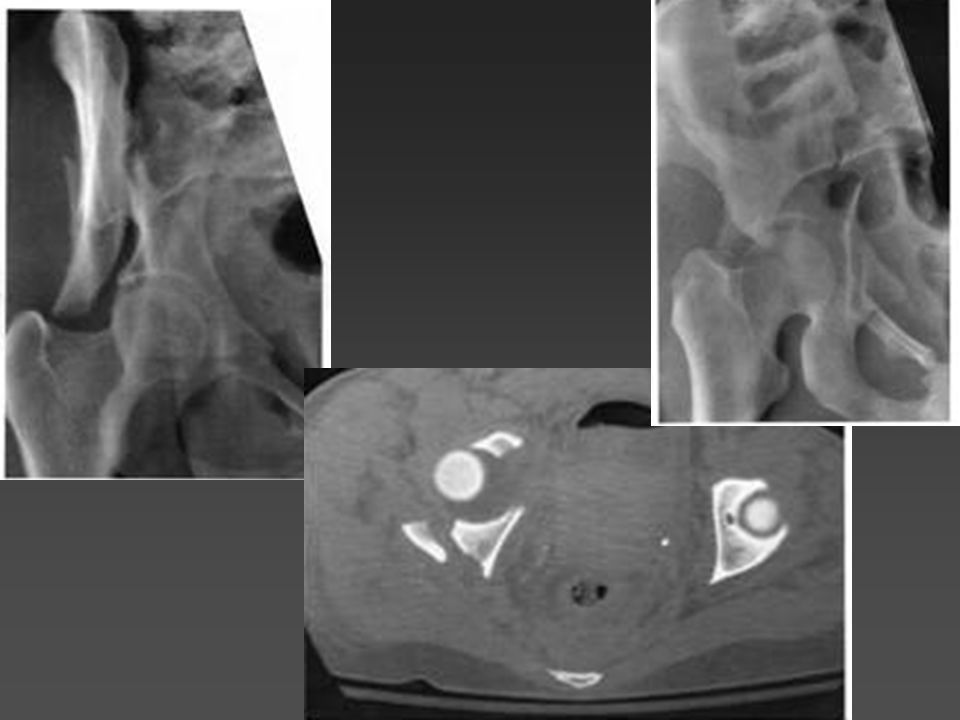



, F.R.C.S.(C )>")


Extension of traumatized wound to allow identification of zone of injury 2)Detection & removal of foreign material, especially.>")












