Download presentation
Presentation is loading. Please wait.

1
Red cells and the critically ill patient “Conservatives” or “Liberals” Dr A. Surekha Devi Consultant, Transfusion Medicine Hyderabad

2
Introduction Blood transfusion is an essential part of modern health care.Transfusions are an index of severity of illness Critical care physician should decide to transfuse based on the risks, benefits and alternatives of treatment Suboptimal patient care due to over-use & under-use of blood products Evidence-based transfusion triggers 90% of RBC transfusions in ICU are for treatment of anemia Total blood management aimed -to improve management of anemia -to reduce or eliminate allogenic transfusions

3
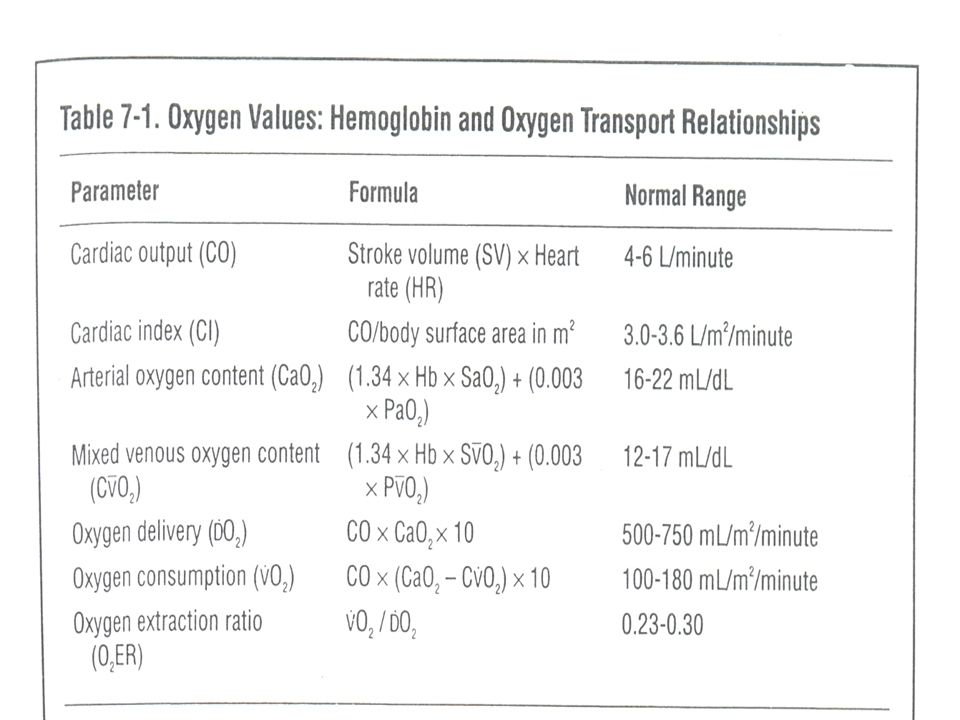
Guidelines for red cell transfusions There is no single value of hemoglobin concentration that justifies or requires transfusion RBCs are administered when Hgb 10 g/dl When Hgb is 7-10 g/dl, red cell transfusion is based on the following factors: - organ ischemia - ongoing bleeding(rate and magnitude) - Patient’s intravascular volume status - Patient’s risk factors for complications of inadequate oxygenation (low cardiopulmonary reserve and high oxygen consumption) - Physiological triggers such as O 2 ER >50%, SVO 2 <50% * Anesthesiology 2006;105:198-208.
 - Patient’s intravascular volume status - Patient’s risk factors for complications of inadequate oxygenation (low cardiopulmonary reserve and high oxygen consumption) - Physiological triggers such as O 2 ER >50%, SVO 2 <50% * Anesthesiology 2006;105:")
5
Indications for red cell transfusion Hemorrhagic shock Acute hemorrhage(35%) with hemodynamic instability inadequate oxygen delivery(25%) Anemia due to - sepsis - hemolysis - decreased production of endogenous erythropoietin - immune associated functional iron deficiency - blunted reticulocyte response - overt or covert blood loss
 with hemodynamic instability inadequate oxygen delivery(25%) Anemia due to - sepsis - hemolysis - decreased production of endogenous erythropoietin - immune associated functional iron deficiency - blunted reticulocyte response - overt or covert blood loss")
6
Crit Care Med 2009;37:3124-57.

7
“ Conservatives”

8
TRICC trial Canadian Critical Care Trials Group - 838 patients, over 3 yrs from 25 centers – Paul C.Hehert et al Restricted strategy(n=418) Transfusion trigger of 7 g/dl & maintenance of 7-9 g/dl Average 2.6 units given Received 54% less blood 1/3 rd patients did not require transfusions Decreased 30-day all cause mortality, lower MOF, fewer cardiac complications Recommended restrictive transfusion strategy as the clinical outcome was better Liberal strategy(n=420) Transfusion trigger of 10 g/dl & maintenance of 10-12 g/dl Average 5.6 units given All patients required transfusions Septic patients should have liberal transfusion practice Crit Care Med 2009 Vol. 37, No. 12.

9
CRIT study: Data on red cell transfusion and outcome was collected on 4892 patients from 284 ICUs in 213 US hospitals. Mean Hgb was 11 g/dl. 90% of transfusions were for anemia. Blood transfusions were associated with increased mortality ABC study: Cohort of 3534 patients admitted to 146 western European ICUs. Mean Hgb at admission was 11.3 g/dl. Documented longer ICU stay and increased mortality Transfusion triggers in SICU: Robertie & Gravlee Well compensated patients with no heart disease: 6 g/dl Stable cardiac disease & blood loss of 300ml: 8 g/dl Older patients and those with post-op complications: 10 g/dl Crit Care Med 2009;37:3124-57.

10
Johns Hopkins study Steven M.Frank et al. have done study on 48,000 surgical patients from February 2010 to August 2011 at Johns Hopkins hospital 2,981(6.2%) patients received blood transfusions during surgery There was wide variation among surgeons and anesthesiologists in ordering blood transfusion Patients undergoing surgery for pancreatic cancer, orthopedic problems, aortic aneurysms received blood at higher trigger points >10 g/dl It was decided to transfuse at a trigger of <7-8 g/dl as blood is in short supply, pricey and associated with risks like infections, immunomodulation and triggers complex immune reactions Johns Hopkins Medicine News and Publications. 04/24/2012
 patients received blood transfusions during surgery There was wide variation among surgeons and anesthesiologists in ordering blood transfusion Patients undergoing surgery for pancreatic cancer, orthopedic problems, aortic aneurysms received blood at higher trigger points >10 g/dl It was decided to transfuse at a trigger of <7-8 g/dl as blood is in short supply, pricey and associated with risks like infections, immunomodulation and triggers complex immune reactions Johns Hopkins Medicine News and Publications. 04/24/2012.")
11
“ Liberals”

12
Sepsis occurrence in acutely ill patients study (SOAP Study) Prospective, multicenter, observational study, to evaluate epidemiology of sepsis of ICU patients in European countries, initiated by European Society of Intensive Care Transfused patients had a better survival, than those who were not transfused Changes in blood processing so that blood transfusions are safer today in terms of viral transmission that they were a decade ago Leukodepletion of red cells removes negative immunosuppressive effects of transfusion, TRIM, TRALI and also transmission of leukotropic viruses 76% of centers were routinely using leukodepleted blood This study suggests that blood transfusions may not be associated with increased mortality and may be associated with improved survival * Anaesthesiology 2008; 108:31-9.
 Prospective, multicenter, observational study, to evaluate epidemiology of sepsis of ICU patients in European countries, initiated by European Society of Intensive Care Transfused patients had a better survival, than those who were not transfused Changes in blood processing so that blood transfusions are safer today in terms of viral transmission that they were a decade ago Leukodepletion of red cells removes negative immunosuppressive effects of transfusion, TRIM, TRALI and also transmission of leukotropic viruses 76% of centers were routinely using leukodepleted blood This study suggests that blood transfusions may not be associated with increased mortality and may be associated with improved survival * Anaesthesiology 2008; 108:31-9.")
13
Sepsis Although transfusion increases oxygen delivery, tissue utilization of oxygen does not increase in patients with sepsis There is increased splanchnic ischemia following transfusion with old blood in patients with sepsis. This paradoxically decreases microcirculatory oxygen delivery and contribute to tissue hypoxia Marik & Sibbald et al Sepsis is an indication of transfusion need in anaemic patient because of increased tissue oxygen debt and resetting of DO 2 / VO 2 interactions; Shoemaker et al Patients with ARDS have hidden oxygen debt unrelated to Hb level; Bihari et al Should have liberal transfusion strategy

14
Crit Care Med 2009;37:3124-57.

15
Liberal transfusion strategy Red cells: Hb <7-9 g/dl (in absence of significant coronary artery disease, acute hemorrhage or lactic acidosis) Hb <10 g/dl in patients with low central venous oxygen saturation during first 6 hrs of resuscitation of septic shock Erythropoietin is not recommended in severe sepsis Liberal transfusion strategy is also followed in ARDS MOF Traumatic brain injury Cerebrovascular disease Crit care Med 2004; 32: 858-873.
 Hb <10 g/dl in patients with low central venous oxygen saturation during first 6 hrs of resuscitation of septic shock Erythropoietin is not recommended in severe sepsis Liberal transfusion strategy is also followed in ARDS MOF Traumatic brain injury Cerebrovascular disease Crit care Med 2004; 32:")
16
Red cell transfusion risks Transfusions cause immunosuppression by decreasing cell mediated immunity, altering of T-cell ratios Associated with increased nosocomial infections - wound infection - Cystitis - pneumonia - bacteremia - sepsis - line infections It is independent risk factor for MOF and SIRS Associated with longer ICU and hospital stay Increased morbidity and mortality There is a relationship between transfusion and ALI & ARDS Possible development of immunomodulation and autoimmune diseases later Febrile & allergic reactions, TRALI, TACO, TRIM, hemolytic reactions and human errors Crit Care Med 2009;37:3124-57.

17
Crit Care Med 2002 Vol.30, No.10

18
Indian J Crit Care Med October-December 2007 Vol 11 Issue 4.

19
Leucoreduction of red cells Pre-storage leucoreduction of RBCs is recommended for critically ill patients Lowers transfusion associated immunosuppression lowers incidence of post-operative infections Red cells should be <15 days old - as older blood decreases microcirculatory oxygen delivery - decreases red cell 2,3 DPG concentration in old blood - increased splanchnic ischemia occurs with old blood

20
Neonatal intensive care(NICU) Red cells should be compatible with the ABO group and Rh type as well as unexpected red cell antibodies in the maternal serum Red cells of <7days old, preserved in CPDA1 (avoidance of preservative solution), HbS negative, CMV reduced risk and irradiated Transfusion volumes on the basis of ml/kg body weight Minimal donor exposure; one unit is designated and aliquoted for a given neonate 3 kg neonate has total plasma volume of 150 ml; hence group identical RDPs and cryo should be transfused Venous Hb of <13 g/dl in the first 24 hrs of life indicates anaemia; healthy FT neonate <10 g/dl; PT neonate <7-9 g/dl Use of rhEPO with efforts to reduce blood loss from phlebotomy for lab tests can reduce / avoid transfusions Pediatric transfusion 2 nd ed. AABB 2006.

21
Pediatric intensive care(PICU) Red cells: 10-15 ml/kg = 2-3 gm/dL Platelets: 5-10 ml/kg = 50,000-1,00,000/μL FFP: 10-15 ml/kg = factor activity 15-20% Cryo: 1-2 units/10 kg = 60-100 mg/dL(infant) 5-10 mg/dL (older children) CPDA1 red cells should be given in infants less than 4 months old, red cells with preservative are not recommended Decision to transfuse critically ill pediatric patients should be individualised and restricted to patients with Hb levels <9 g/d L Pediatric transfusion 2 nd ed. AABB 2006.

22
Blood conservation Outcomes can be improved, risk reduced and costs saved To reduce acute blood loss - Antifibrinolytic agents: Aprotinin, TA, EACA - Recombinant activated factor VII - Artificial O 2 carriers: HBOCs, Perflurocarbons - Postoperative blood recovery: cell salvage To prevent subacute anemia - Erythropoietin(rHuEpo) - Restrictive red cell transfusion trigger - Reduction in diagnostic laboratory testing - Use of low-volume adult/pediatric blood sampling tubes CMAJ Jan 2008; 178:49-57.
 - Restrictive red cell transfusion trigger - Reduction in diagnostic laboratory testing - Use of low-volume adult/pediatric blood sampling tubes CMAJ Jan 2008; 178:49-57.")
23
Transfusion 2012;52:1643. Study at University of Pittsburgh Medical Center

24
Transfusion 2012;52:1640-45. On-screen warning

25
Transfusion 2012;52:1642. Comparison of monthly no.of RBC alerts

26
Summary Implementing a hospital-based blood management strategy Restrictive transfusion strategy is superior to liberal transfusion strategy as clinical outcomes are better Critically ill patients can tolerate anemia to an Hgb level of 7 g/dl There is no single value of Hgb concentration that justifies transfusion, patient’s clinical situation should also be evaluated Pre-storage leucoreduced RBCs minimizes adverse effects of transfusion RBC transfusions are associated with increased infections, longer ICU stay, immunomodulation, increased morbidity and mortality Adopting blood conservation techniques–meticulous hemostasis, use of desmopressin, IV iron, rHuEpo, rFVIIa, use of cell salvage, reduction of transfusion triggers and minimizing blood loss for diagnostic purposes

27
“ The best transfusion is the transfusion not given ……” Thank you for your attention

Similar presentations

 1:100 TACO1:100 TRALI1:5,000 Sepsis1:5,000 Acute hemolytic1:75,000 HBV1:160,000.>")
 The timely application of evidence-based medical and.>")
















