Download presentation
Presentation is loading. Please wait.

1
Biomarkers in the Cardiorenal Syndromes
Catherine Krawczeski, MD Associate Professor of Pediatrics University of Cincinnati College of Medicine Cardiac Intensive Care Co-Director, Center for Acute Care Nephrology The Heart Institute Cincinnati Children’s Hospital Medical Center

2
Cardiorenal Syndromes
Type I: Acute Cardiorenal Syndrome Abrupt worsening of cardiac function (e.g. acute cardiogenic shock or acutely decompensated CHF) leading to acute kidney injury Type II: Chronic Cardiorenal Syndrome Chronic abnormalities in cardiac function (e.g. chronic CHF) causing progressive and potentially permanent chronic kidney disease Type III: Acute Renocardiac Syndrome Abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia) Type IV: Chronic Renocardiac Syndrome Chronic kidney disease (e.g. chronic glomerular or interstitial disease) contributing to decreased cardiac function, cardiac hypertrophy and/or increased risk of adverse cardiovascular events Type V: Secondary Cardiorenal Syndrome Systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction Combined disorders of the heart and kidney are classified as cardiorenal syndromes. The most recent definition includes 5 subtypes reflecting a variety of conditions where there primary failing organ can be either the heart or the kidney, and a timeframe of disease.
 leading to acute kidney injury. Type II: Chronic Cardiorenal Syndrome. Chronic abnormalities in cardiac function (e.g. chronic CHF) causing progressive and potentially permanent chronic kidney disease. Type III: Acute Renocardiac Syndrome. Abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia) Type IV: Chronic Renocardiac Syndrome. Chronic kidney disease (e.g. chronic glomerular or interstitial disease) contributing to decreased cardiac function, cardiac hypertrophy and/or increased risk of adverse cardiovascular events. Type V: Secondary Cardiorenal Syndrome. Systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction. Combined disorders of the heart and kidney are classified as cardiorenal syndromes. The most recent definition includes 5 subtypes reflecting a variety of conditions where there primary failing organ can be either the heart or the kidney, and a timeframe of disease.")
3
Cardiorenal Syndromes
Type I: Acute Cardiorenal Syndrome Abrupt worsening of cardiac function (e.g. cardiac surgery, cardiogenic shock or acute decompensated HF) leading to acute kidney injury Type II: Chronic Cardiorenal Syndrome Chronic abnormalities in cardiac function (e.g. chronic CHF) causing progressive and potentially permanent chronic kidney disease Type III: Acute Renocardiac Syndrome Abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia) Type IV: Chronic Renocardiac Syndrome Chronic kidney disease (e.g. chronic glomerular or interstitial disease) contributing to decreased cardiac function, cardiac hypertrophy and/or increased risk of adverse cardiovascular events Type V: Secondary Cardiorenal Syndrome Systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction I’m going to focus most of this talk on types 1 and 5 CRS. Type 1 CRS is defined as an abrupt worsening of cardiac function (as occurs with cardiac surgery, cardiogenic shock or acute decompensated HF) leading to acute kidney injury. As you can imagine, as a cardiac intensivist, this is by far the largest group of AKI that I see. Type 5 or secondary CRS occurs when a systemic disease (such as sepsis) causes both cardiac and renal dysfunction.
 leading to acute kidney injury. Type II: Chronic Cardiorenal Syndrome. Chronic abnormalities in cardiac function (e.g. chronic CHF) causing progressive and potentially permanent chronic kidney disease. Type III: Acute Renocardiac Syndrome. Abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia) Type IV: Chronic Renocardiac Syndrome. Chronic kidney disease (e.g. chronic glomerular or interstitial disease) contributing to decreased cardiac function, cardiac hypertrophy and/or increased risk of adverse cardiovascular events. Type V: Secondary Cardiorenal Syndrome. Systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction. I’m going to focus most of this talk on types 1 and 5 CRS. Type 1 CRS is defined as an abrupt worsening of cardiac function (as occurs with cardiac surgery, cardiogenic shock or acute decompensated HF) leading to acute kidney injury. As you can imagine, as a cardiac intensivist, this is by far the largest group of AKI that I see. Type 5 or secondary CRS occurs when a systemic disease (such as sepsis) causes both cardiac and renal dysfunction.")
4
This schematic details the complex interplay between the heart and kidney.
In the face of acute heart disease, a combination of altered hemodynamics, immune mediated damage, activation of the sympathetic nervous system and renin-angiotensin system, and exogenous factors such as nephrotoxin lead to development of acute kidney injury.

5
Cardiorenal Syndromes
Impaired kidney function, or worsening kidney function, in the setting of acute decompensated heart failure, portends a significantly worse prognosis Is it possible to prevent AKI in HF patients? How do we manage these patients without damaging their kidneys? Studies have demonstrated that …… This leads to 2 important questions…

6
This demonstrates the delicate balance between volume depletion and acute decompensation in the diseased state. In the normal heart and normal kidney…. Ronco, JACC, 2012 Epub

7
Diagnosing AKI Diagnostic criteria not standard– over 30 definitions in literature- making comparisons between studies difficult Inadequate “gold standard” SCr is delayed and unreliable in the acute setting Quest for biomarkers an intense area of research Particularly important for CS-AKI, a planned ischemic event and in decompensated HF, where hydration status is often difficult to assess Pediatric patients ideal population to study biomarkers So why is it difficult to diagnose AKI and monitor patients for development of CRS? As we’ve discussed, the current gold standard is woefully inadequate. We know that creatinine is a very insensitive marker of AKI, varying widely with age, gender, diet, muscle mass, medications and hydration status.…. As such the quest for biomarkers has been an intense area of research Biomarkers are particularly important for CS-AKI, which is a planned ischemic event where early detection and early therapy is possible and for decompensated HF, where hydration

8
Serum cystatin C, serum creatinine
Antecedents Intermediate stage AKI Outcomes Normal ↑Risk Damage ↓ GFR Kidney Failure Death Biomarkers of structural injury Biomarkers of functional injury NGAL, IL-18, L-FABP, KIM-1 Serum cystatin C, serum creatinine Adapted from Murray, CJASN, 2008; 3:

9
Neutrophil Gelatinase-Associated Lipocalin (NGAL)
Sideraphore binding lipocalin, first identified in a neutrophils Normally very small amounts in kidney tubules Marked upregulation very early after ischemic or nephrotoxic AKI May be measured in plasma or urine May be influenced by other conditions such as systemic or urinary tract infections, inflammatory conditions, and malignancies The most promising biomarker to date is Neutrophil Gelatinase-Associated Lipocalin or NGAL. NGAL was first identified as a neutrophil granule. It is normally found in very small amounts in the kidney tubules and is markedly upregulated very quickly after kidney injury. It may be measured in plasma or blood (which is advantageous in the case of anuria) but may be influenced by other conditions such as…..
 but may be influenced by other conditions such as…..")
10
Pilot study of NGAL Landmark prospective study of 71 congenital heart patients undergoing CPB 20 (28%) developed AKI (defined as >50% increase in SCr from baseline) SCr increase occurred 1-3 days after surgery We investigated NGAL as an early biomarker for AKI after CPB. We chose post-CPB kidney injury since this was a common cause of ischemic AKI and there was a temporally predictable injury, allowing us to collect baseline and post-injury specimens. Our original study involved 71 prospectively enrolled patinets undergoing surgery for congenital heart disease. We defined AKI as a 50% or greater increase in SCr from baseline.
 developed AKI (defined as >50% increase in SCr from baseline) SCr increase occurred 1-3 days after surgery. We investigated NGAL as an early biomarker for AKI after CPB. We chose post-CPB kidney injury since this was a common cause of ischemic AKI and there was a temporally predictable injury, allowing us to collect baseline and post-injury specimens. Our original study involved 71 prospectively enrolled patinets undergoing surgery for congenital heart disease. We defined AKI as a 50% or greater increase in SCr from baseline.")
11
NGAL Both urine and plasma NGAL independent predictors of AKI
AUC 2h plasma NGAL 0.91 AUC 2h urine NGAL 0.998 Postoperative NGAL levels correlate with Duration of AKI Length of hospital stay Length of mechanical ventilation Mortality Looking at their respective ROC curves, both urine and plasma NGAL are excellent predictors of AKI with AUCs of .91 to .998. In our study, postoperative NGAL levels correlated with duration of AKI, length of hospital stay, length of mechanical ventilation and mortality.

12
NGAL Validated in multiple adult and pediatric studies, with multiple etiologies of AKI (ischemic, nephrotoxic, sepsis, CIN, etc). But…. AUC not as good in adult studies Co-morbidities? Inflammation, infection, malignancy, lung disease NGAL Meta-analysis of Prospective CPB Studies 2538 cardiac surgical patients Average sensitivity 76% Average specificity 77% Mean AUC 0.78 Studies in decompensated HF confirm elevations in NGAL associated with increase rate of adverse events and short tem mortality NGAL has been validated in multiple adult and pediatric studies and with multiple etiologies of AKI (including ischemic, toxic, septic, and contrast nephropathy). Unfortunately, however, the AUC’s have not been as good in adults studies, possible do to a increased incidence of co-morbidities in the adult population such as inflammation, infection, malignancy, and lung disease, all of which are know to increase baseline NGAL levels. In recent meta-analysis of prospective CPB studies which involved 2538 cardiac surgical patients, average sensitivity was 76%, specificity 77% and AUC Notably this compares well with the iinitial studies of troponin, which had an AUC in a similar range. Haase et al, AJKD 54: , 2009
. Unfortunately, however, the AUC’s have not been as good in adults studies, possible do to a increased incidence of co-morbidities in the adult population such as inflammation, infection, malignancy, and lung disease, all of which are know to increase baseline NGAL levels. In recent meta-analysis of prospective CPB studies which involved 2538 cardiac surgical patients, average sensitivity was 76%, specificity 77% and AUC Notably this compares well with the iinitial studies of troponin, which had an AUC in a similar range. Haase et al, AJKD 54: ,")
13
Biomarkers as Endpoints
JACC 2011;57: One of the difficulties we have with evaluating AKI biomarkers is that we have a flawed gold standard. These are the results of a pooled analysis, looking specifically at outcomes in patients who demonstrate elevations in NGAL but do not have serum creatinine rise, shown here in this column. This subgroup of patients, who did not fit traditional AKI criteria, still had significantly higher mortality and ICU length of stay, than those who did not have NGAL rises. Such results may influence our diagnostic criteria in the future.

14
Interleukin 18 (IL-18) Pro-inflammatory cytokine, activating macrophages Induced and cleaved in the proximal tubule Low concentration at baseline Easily detected in the urine after ischemic injury Levels correlate with outcomes A second promising biomarker is interleuking 18 or IL-18. IL-18 is a pro-inflammatory cytokine which is induced an cleaved in the proximal tubule. IL-18 is in low concentration at baseline but in easily detected in the urine after ischemic injury.

15
Cystatin C Endogenous cysteine proteinase inhibitor produced by nucleated cells at a constant rate Used primarily as assessment of glomerular filtration Serum levels readily measurable using standard laboratory platform Significant rise at 12h after CPB with peak at 24h Can be measured in urine or plasma Cystatin C is an endogenous cysteine proteinase inhibitor. It is produced by nucleated cells at a constant rate. Multiple studies have determined the utility of cystatin C in the measure ment of GFR and unlike the other biomarkers cystatin c may be readily measured using standard current laboratory platforms. In one of our recent studies we found a significant rise in cystatin C at 12 hours after bypass in AKI patients with a peak at 24 hours. We determined that a cutoff value of 1.16 mg/dl at 12 h was predicitve of AKI. Cut-off value of 1.16 mg/dL at 12h predictive of AKI Krawczeski et al, CJASN 2010

16
Other Promising Biomarkers
Kidney Injury Molecule-1 (KIM-1): Epithelial trans-membrane protein, cell-cell interaction. Appears to have strong relationship with severity of renal injury Later increase but perhaps higher specificity Elevations noted in cardiac transplant patients with kidney injury Liver-type Fatty Acid Binding Protein (L-FABP): Member of lipocalin family- binds long-chain fatty acid oxidation products Proximal tubular marker Intermediate elevation after AKI Under Investigation: Monocyte Chemoattractant Protein-1 (MCP-1 ) Hepcidin Alpha-1 Microglobulin (A1M) Albumin - IL-18, KIM-1 and L_FABP are 3 additional proteins which have emerged as promising early AKI biomarkers and are undergoing validation studies. Given the multifactorial etiology of ischemic AKI it is likely that no single biomarker may be ideal and instead that combinations of biomarkers may prove best at identifying patients at risk. 16
: Epithelial trans-membrane protein, cell-cell interaction. Appears to have strong relationship with severity of renal injury. Later increase but perhaps higher specificity. Elevations noted in cardiac transplant patients with kidney injury. Liver-type Fatty Acid Binding Protein (L-FABP): Member of lipocalin family- binds long-chain fatty acid oxidation products. Proximal tubular marker. Intermediate elevation after AKI. Under Investigation: Monocyte Chemoattractant Protein-1 (MCP-1 ) Hepcidin. Alpha-1 Microglobulin (A1M) Albumin. - IL-18, KIM-1 and L_FABP are 3 additional proteins which have emerged as promising early AKI biomarkers and are undergoing validation studies. Given the multifactorial etiology of ischemic AKI it is likely that no single biomarker may be ideal and instead that combinations of biomarkers may prove best at identifying patients at risk. 16.")
17
Biomarker Combinations
AKI has multi-factorial etiology Likely no single biomarker will be sufficient but that a biomarker “panel” may prove to be ideal Variable rise in biomarker concentrations may allow timing of insult and direct appropriate therapy Given the multi-factorial etiology of AKI, it is likely that no single biomarker will be sufficient but that a biomarker “panel” may prove to be ideal.

18
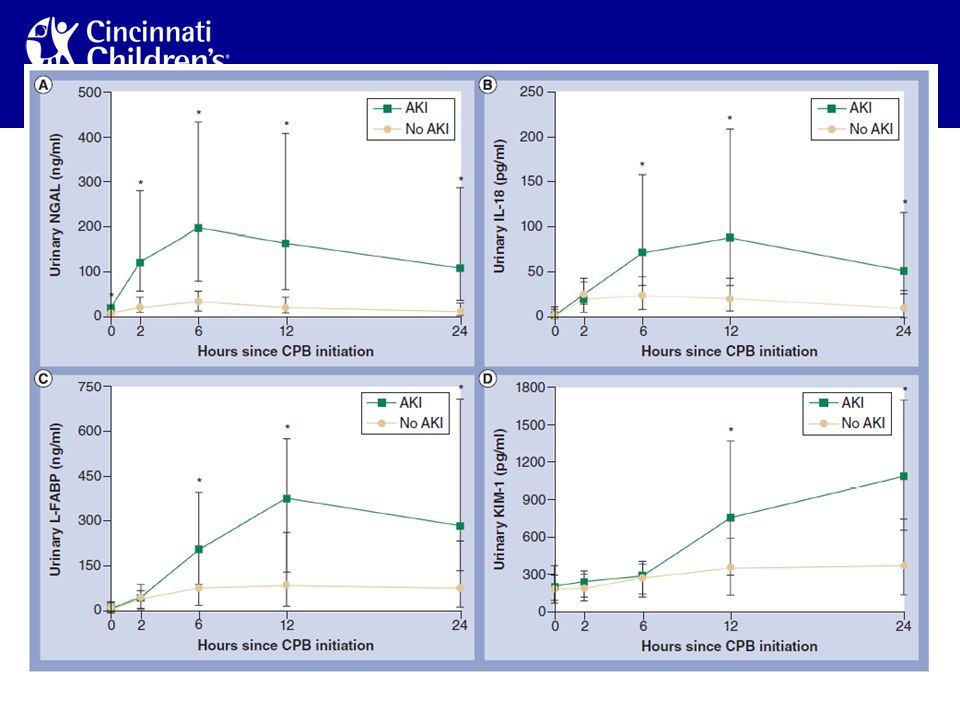
Biomarker Combinations
JACC 2011;58: 220 pediatric CPB patients Evaluation of: Urine NGAL, IL-18, KIM-1, and L-FABP Sequential pattern determined Correlation with outcomes and severity of AKI Combination of biomarkers was most predictive of AKI Elevations able to predict “severe” AKI Because of this, we recently looked at combinations of biomarkers in pediatric patients undergoing CPB. In this study of 220 patients, NGAL, IL-18, KIM-1 and L-FABP were evaluated both alone and as a panel. Since the results are being discussed at an upcoming session, I can’t go into too much detail but we determined a sequential pattern of elevation in these biomarkers, demonstrated their correlation with outcomes and severity of AKI and most importantly, demonstrated that using a combination or panel of biomarkers proved most predictive of AKI

20
Coupling Cardiac and AKI Biomarkers
Addition of NGAL to known cardiac biomarkers (such as BNP) may allow full interpretation of fluid status in decompensated HF and direct clinical care Ronco, et al
 may allow full interpretation of fluid status in decompensated HF and direct clinical care. Ronco, et al.")
21
Summary Current diagnostic standard is inadequate and outdated and has limited potential therapeutic advances Tools of modern science are providing us with highly promising candidates to improve the outcomes of AKI What is needed: Refinement of AKI definition Evaluation of biomarker performance in all etiologies of CRS Development of rapid diagnostic tests -- ? Biomarker “panels” Therapeutic trials In summary,

Similar presentations




 in adults has grown rapidly. Although.>")














 Collaborative Study Group N Eng J Med 345:851-860, 2001 Edmund J. Lewis, M.D. Muehrcke Family Professor of.>")
