Download presentation
Presentation is loading. Please wait.

1
Update on Osteoporosis
OsteoporosisWRAP SlideCAST Update on Osteoporosis Sol Epstein, M.D. Clinical Professor of Medicine and Geriatrics Mount Sinai School of Medicine New York, New York

2
Topics to be Visited New data on current therapies New therapies
“Hot topics with therapy Osteopenia and FRAX Drug holiday Waning of fracture effect ONJ Atrial Fibrillation Atypical fractures Atypical osteoclasts and BP’s Non Skeletal benefits of Vit D

3
Therapeutic Strategies
Inhibitors of Bone Resorption Estrogen, SERMs Bisphosphonates Calcitonin Stimulators of Bone Formation Fluoride PTH analogs Sr Ranelate (?) Bone marrow precursors Inhibitors of RANKL Cathepsin K Osteoclast Osteoblasts Lining cells
 Bone marrow precursors. Inhibitors of. RANKL. Cathepsin K. Osteoclast. Osteoblasts. Lining cells.")
4
Ibandronate 2.5mg has 62% RRR in vertebral fractures vs PBO
Ibandronate evidence of anti-fracture efficacy Ibandronate 2.5mg has 62% RRR in vertebral fractures vs PBO (BONE study) Ibrandronate 2.5mg has 69% RRR in non-vertebral fractures vs PBO in higher risk patients (BONE study) Prospective Trials Monthly bandronate150mg has 34 to 38% RRR in non-vertebral fractures in the pivotal registration trials (Harris; Cranney) Meta-analysis of Trials Monthly ibandronate150mg demonstrated statistically greater reduction in vertebral fractures, and comparable rates of non-vertebral / hip fracture vs weekly bisphosphonates in clinical practice settings (VIBE study) Observational Studies
 Ibrandronate 2.5mg has 69% RRR in non-vertebral fractures vs PBO. in higher risk patients. (BONE study) Prospective. Trials. Monthly bandronate150mg has 34 to 38% RRR. in non-vertebral fractures in the pivotal registration trials. (Harris; Cranney) Meta-analysis. of Trials. Monthly ibandronate150mg demonstrated statistically greater reduction in vertebral fractures, and comparable rates of. non-vertebral / hip fracture vs weekly bisphosphonates. in clinical practice settings (VIBE study) Observational. Studies.")
5
Meta-analysis methods1
Meta-analysis of ibandronate registration trials to increase sample size and power identical designs: BMD bridging studies for oral (MOBILE2) and i.v. (DIVA3) non-vertebral fracture data collected with X-ray confirmation Primary endpoint: major non-vertebral fractures including clavicle, humerus, wrist, pelvis, hip and leg Canadian meta-analysis statistical approach Compare patients on high doses versus daily doses time-to-fracture using Kaplan-Meier methods (cumulative fracture rate) relative risk of fracture using Cox regression to control for baseline differences (age, BMD, prior clinical fracture) Compare patients within trials, rather than across trials maintains study randomisation and increases validity of results Group patients on similar therapeutic doses patients grouped according to ACE to increase sample size and include comparable oral and i.v. doses 1Cranney A, et al. Osteoporosis Int. 2008, DOI /s 2Miller PD, et al. J Bone Miner Res 2005;20:1315–22 3Delmas PD, et al. Arthritis Rheum 2006;54:1838–46
 and i.v. (DIVA3) non-vertebral fracture data collected with X-ray confirmation. Primary endpoint: major non-vertebral fractures including clavicle, humerus, wrist, pelvis, hip and leg. Canadian meta-analysis statistical approach. Compare patients on high doses versus daily doses. time-to-fracture using Kaplan-Meier methods (cumulative fracture rate) relative risk of fracture using Cox regression to control for baseline differences (age, BMD, prior clinical fracture) Compare patients within trials, rather than across trials. maintains study randomisation and increases validity of results. Group patients on similar therapeutic doses. patients grouped according to ACE to increase sample size and include comparable oral and i.v. doses. 1Cranney A, et al. Osteoporosis Int. 2008, DOI /s Miller PD, et al. J Bone Miner Res 2005;20:1315–22. 3Delmas PD, et al. Arthritis Rheum 2006;54:1838–46.")
6
Meta-analysis Compares Higher vs Lower Dose Groups
compared with Higher doses (ACE* ~11mg) (ACE* 5.5mg) Monthly oral† 150mg Quarterly i.v. 3mg Daily oral 2.5mg *ACE = annual cumulative exposure = dose x doses/year x absorption (e.g. 2.5 x 365 x 0.6% = 5.5mg ACE) Recognizing the different pharmacokinetics of the oral and intravenous forms of ibandronate, ACE was defined as the total annual dose of bisphosphonate absorbed and therefore available to the bone tissue taking into account the fact that 100% of an intravenous bisphosphonate and 0.6% of an oral dose are absorbed [11, 12]. For example, 2 mg i.v. every 2 months or 3 mg i.v. administered quarterly is equivalent to an ACE of 12 mg. Similarly, 150 mg orally given monthly is equivalent to an ACE of 10.8mg. Bimonthly i.v. 2mg NOT LICENSED *ACE = annual cumulative exposure = dose x doses/year x absorption (e.g. 2.5 x 365 x 0.6% = 5.5mg ACE) †Absorption for oral ibandronate = 0.6%1 1Barrett J, et al. J Clin Pharmacol 2004;44:951–65
 (ACE* 5.5mg) Monthly oral† 150mg. Quarterly i.v. 3mg. Daily oral 2.5mg. *ACE = annual cumulative exposure = dose x doses/year x absorption (e.g. 2.5 x 365 x 0.6% = 5.5mg ACE) Recognizing the different pharmacokinetics of the oral and intravenous forms of ibandronate, ACE was defined as the total annual dose of bisphosphonate absorbed and therefore available to the bone tissue taking into account the fact that 100% of an intravenous bisphosphonate and 0.6% of an oral dose are absorbed [11, 12]. For example, 2 mg i.v. every 2 months or 3 mg i.v. administered quarterly is equivalent to an ACE of 12 mg. Similarly, 150 mg orally given monthly is equivalent to an ACE of 10.8mg. Bimonthly i.v. 2mg. NOT LICENSED. *ACE = annual cumulative exposure = dose x doses/year x absorption (e.g. 2.5 x 365 x 0.6% = 5.5mg ACE) †Absorption for oral ibandronate = 0.6%1. 1Barrett J, et al. J Clin Pharmacol 2004;44:951–65.")
7
Estimated fracture rate (%)
Time to non-vertebral fracture is extended with ibandronate ACE 10.8mg p=0.036 (log-rank)* Estimated fracture rate (%) 6 5 4 3 2 1 Higher doses (ACE 10.8mg) Daily dose (ACE 5.5mg) 38% RRR† p=0.0375 Time (days) *For time to fracture with ibandronate versus daily dose †Cox regression analyses for difference in RR of fracture with ibandronate versus daily dose Cranney A, et al. Osteoporosis Int. 2008, DOI /s
* Estimated fracture rate (%) Higher doses (ACE 10.8mg) Daily dose (ACE 5.5mg) % RRR† p= Time (days) *For time to fracture with ibandronate versus daily dose. †Cox regression analyses for difference in RR of fracture with ibandronate versus daily dose Cranney A, et al. Osteoporosis Int. 2008, DOI /s")
8
Higher dose ibandronate reduced non-vertebral fracture risk at 2 years
6 4 2 38% RRR p=0.0375 Non-vertebral fracture rate at 2 years (%) 4.8 3.1 When compared with the low ACE-group (2.5 mg daily = ACE 5.5 mg) the higher ACE-group showed a 38% relative risk reduction in key non-vertebral fractures. Daily dose Higher doses (ACE 5.5 mg) (ACE ≥10.8 mg)* *Includes marketed 150mg monthly oral (ACE 10.8mg) and 3mg i.v. quarterly (ACE 12mg), plus the unlicensed 2mg every 2 months i.v. dose (ACE 12mg) Fracture rate from Kaplan-Meier analysis; RRR from Cox regression adjusted for baseline characteristics Cranney A, et al. Osteoporosis Int. 2008, DOI /s
 When compared with the low ACE-group (2.5 mg daily = ACE 5.5 mg) the higher ACE-group showed a 38% relative risk reduction in key non-vertebral fractures. Daily dose. Higher doses. (ACE 5.5 mg) (ACE ≥10.8 mg)* *Includes marketed 150mg monthly oral (ACE 10.8mg) and 3mg i.v. quarterly (ACE 12mg), plus the unlicensed 2mg every 2 months i.v. dose (ACE 12mg) Fracture rate from Kaplan-Meier analysis; RRR from Cox regression adjusted for baseline characteristics Cranney A, et al. Osteoporosis Int. 2008, DOI /s")
9
Limitations Strengths
Trials not primarily designed to study fracture efficacy Baseline patient characteristics controlled for, were limited to those collected in study protocol P values not adjusted for multiple comparisons Greater power and sample size to detect differences in fracture rates Evidence from meta-analysis of two large phase III randomised controlled clinical trials Consistent nonvertebral fracture data collection, confirmed by x-ray Validity of analysis increased by maintaining randomisation Study conducted externally by experts in meta-analysis and osteoporosis Cranney A, et al. Osteoporosis Int. 2008, DOI /s

10
Primary analysis: monthly ibandronate vs weekly bisphosphonates at 12 months
RR=0.36 p<0.01 RR=1.06 p=0.84 RR=0.88 p=0.26 RR=0.82 p=0.052 Fx=15 0.20 Fractures Monthly oral ibandronate (n=7,345) Weekly oral BPs (n=56,837) Fx=103 Non-vertebral Hip Vertebral Any Fracture incidence (%) 1.30 Fx=858 Fx=8 Fx=135 Fx=106 Fx=95 Fx=738 1.29 0.19 0.24 0.11 1.51 1.40 1.6 1.2 0.8 0.4 The bars reflect the crude (unadjusted) fracture incidence. Fx reflects absolute number of fractures. RR reflects the adjusted RR (hazard ratio) using Cox regression controlling for potential confounding variables. A RR < 1 means the hazard ratio favors ibandronate. RR = adjusted RR (hazard ratio) using Cox regression controlling for potential confounding variables; Persistent patient cohort with no refill gap >45 days (monthly) or 30 days (weekly); Fx = absolute number of fractures Reginster JY et al. Ann Rheum Dis 2008;67,Suppl. II; 539, Abstr. SAT0338 and SAT0339
 Weekly oral BPs (n=56,837) Fx=103. Non-vertebral Hip Vertebral Any. Fracture incidence (%) Fx=858. Fx=8. Fx=135. Fx=106. Fx=95. Fx= The bars reflect the crude (unadjusted) fracture incidence. Fx reflects absolute number of fractures. RR reflects the adjusted RR (hazard ratio) using Cox regression controlling for potential confounding variables. A RR < 1 means the hazard ratio favors ibandronate. RR = adjusted RR (hazard ratio) using Cox regression controlling for potential confounding variables; Persistent patient cohort with no refill gap >45 days (monthly) or 30 days (weekly); Fx = absolute number of fractures. Reginster JY et al. Ann Rheum Dis 2008;67,Suppl. II; 539, Abstr. SAT0338 and SAT0339.")
11
Proposed Mechanism of Local Recycling of Zoledronic Acid in Bone
HO N O = P OH ZOL has long duration of action Zoledronic Acid has high affinity for bone mineral leading to: BP Avid uptake BP Low desorption BP High re-attachment through recycling BPs can be detected in body fluids many months after injection Proposed Mechanism of Local Recycling of Zoledronic Acid in Bone Differences in binding affinities and effects on mineral surface properties are likely to be reflected in the apparent clinical differences among these bisphosphonates, including differences in potency, pharmacokinetics, and persistence of effect. These clinical differences may result from differences in uptake and retention on the skeleton, diffusion of the drug within bone, release of adsorbed drug from bone, potential recycling of the desorbed drug back onto bone surfaces, effects on mineral dynamics, and effects on cellular function. Reference Nancollas GH, Tang R, Phipps RJ, et al. Novel insights into actions of bisphosphonates on bone: differences in interactions with hydroxyapatite. Bone. 2006;38: BP High Affinity BPs may diffuse less well in bone and remain nearer accessible surfaces G Russell 2005

12
HORIZON Recurrent Fracture Trial: Overview and Study Design
Objective: Demonstrate potential of once yearly zoledronic acid to reduce number of clinical fractures after surgical repair of recent low-trauma hip fracture Multicenter, event-driven, randomized, double-blind, placebo-controlled, parallel-group clinical trial 2127 men and women from 148 clinical centers in 23 countries Patients enrolled and maintained until prespecified number of clinical fracture events occurred, or when patient reached 36 months HORIZON-Recurrent Fracture Trial: Overview and Study Design Key point The HORIZON Recurrent Fracture Trial (RFT) was a multicenter, event-driven, randomized, double-blind, placebo-controlled, parallel- group trial in men and women who had recent surgical repair of a low-trauma hip fracture. The trial population included 2127 men and women from 148 clinical centers in 23 countries.1,2 Supplemental notes Vitamin D levels were not routinely measured but a loading dose of vitamin D (50,000 to 125,000 IU orally or intramuscularly) was given to patients and they were started on 1000 to 1500 mg of elemental calcium plus 800 to 1200 IU of vitamin D supplementation per day for at least 14 days prior to the study drug infusions.3 Daily supplementation with these amounts of calcium and vitamin D continued post infusion for the entirety of the study.1 Patients received their study drug infusion within 90 days after surgical repair of their low trauma hip fracture. An IV formulation of study medication was administered every 12 months before the end-of-study visit.1 Follow-up visits were conducted at Months 6, 12, 24, and 36, and telephone interviews were conducted every 3 months starting at Month 9.2 The 36-month cutoff was the result of a protocol amendment implemented to limit the number of zoledronic acid infusions to a maximum of three. At the time this amendment was implemented, several patients had already received four doses of study medication, and one patient had received five. Patients who had already received four or more doses were instructed to undergo an end of study visit within 90 days. Because of the long enrollment period, patients were followed for different lengths of time. Median time was 1.9 years.1 References Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med ;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. Reclast® (zoledronic acid) Injection [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; June 2008. *All patients received calcium 1000–1500 mg/d and vitamin D 800–1200 IU/d and follow-up telephone calls every 3 months starting at Month 9. 1. Lyles KW, et al. N Engl J Med. 2007;357: 2. Lyles KW, et al. Presented at: 29th ASBMR; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. 12
 was a multicenter, event-driven, randomized, double-blind, placebo-controlled, parallel- group trial in men and women who had recent surgical repair of a low-trauma hip fracture. The trial population included 2127 men and women from 148 clinical centers in 23 countries.1,2. Supplemental notes. Vitamin D levels were not routinely measured but a loading dose of vitamin D (50,000 to 125,000 IU orally or intramuscularly) was given to patients and they were started on 1000 to 1500 mg of elemental calcium plus 800 to 1200 IU of vitamin D supplementation per day for at least 14 days prior to the study drug infusions.3 Daily supplementation with these amounts of calcium and vitamin D continued post infusion for the entirety of the study.1. Patients received their study drug infusion within 90 days after surgical repair of their low trauma hip fracture. An IV formulation of study medication was administered every 12 months before the end-of-study visit.1. Follow-up visits were conducted at Months 6, 12, 24, and 36, and telephone interviews were conducted every 3 months starting at Month 9.2. The 36-month cutoff was the result of a protocol amendment implemented to limit the number of zoledronic acid infusions to a maximum of three. At the time this amendment was implemented, several patients had already received four doses of study medication, and one patient had received five. Patients who had already received four or more doses were instructed to undergo an end of study visit within 90 days. Because of the long enrollment period, patients were followed for different lengths of time. Median time was 1.9 years.1. References. Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract Reclast® (zoledronic acid) Injection [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; June *All patients received calcium 1000–1500 mg/d and vitamin D 800–1200 IU/d and follow-up telephone calls every 3 months starting at Month Lyles KW, et al. N Engl J Med. 2007;357: Lyles KW, et al. Presented at: 29th ASBMR; September 16-19, 2007; Honolulu, Hawaii. Abstract")
13
HORIZON Recurrent Fracture Trial: Study Population
Inclusion1 Male or female patients ≥ 50 years of age Randomized up to 90 days following surgical procedure for a low-trauma hip fracture Ambulatory prior to hip fracture Normal serum calcium Exclusion1,2 Use of oral bisphosphonates within prespecified washout period Use of IV bisphosphonates within 2 years Calculated creatinine clearance <30 mL/min HORIZON Recurrent Fracture Trial: Study Population Key point HORIZON-RFT included male and female patients 50 years of age or older who recently had surgical repair of a hip fracture. Patients could walk prior to fracture. Supplemental notes Inclusion criteria for HORIZON-RFT included male or female patients 50 years of age or older. Patients could be randomized up to 90 days following surgical repair of a low-trauma hip fracture, and all patients were required to be ambulatory with or without an assistive device prior to the hip fracture.1 Patients who had used any bisphosphonate within the past 2 years were excluded according to the following prespecified washout periods: Oral bisphosphonate for greater than 48 weeks: washout period of 2 years. Oral bisphosphonate for greater than 8 but less than 48 weeks: washout period of 1 year. Oral bisphosphonate for greater than 2 but less than or equal to 8 weeks: washout period of 6 months. Any IV bisphosphonate therapy: washout period of 2 years. Exclusion criteria included: use of oral bisphosphonates; calculated creatinine clearance <30.0 mL/min; serum calcium >11 mg/dL (>2.75 mmoL/L); hypocalcemia (serum corrected calcium 8 mg/dL [<2.0 mmol/L] at screening and/or randomization); primary hyperparathyroidism, hypoparathyroidism, osteogenesis imperfecta, Paget’s disease, or any other metabolic bone disease than osteoporosis; any prior use of IV bisphosphonate within 2 years; and any prior use of parathyroid hormone and analogs for >1 week.1,2 References Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. 1. Lyles KW, et al. N Engl J Med. 2007;357: 2. Lyles KW, et al. Presented at: 29th ASBMR; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. 13
; hypocalcemia (serum corrected calcium 8 mg/dL [<2.0 mmol/L] at screening and/or randomization); primary hyperparathyroidism, hypoparathyroidism, osteogenesis imperfecta, Paget’s disease, or any other metabolic bone disease than osteoporosis; any prior use of IV bisphosphonate within 2 years; and any prior use of parathyroid hormone and analogs for >1 week.1,2. References. Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract Lyles KW, et al. N Engl J Med. 2007;357: Lyles KW, et al. Presented at: 29th ASBMR; September 16-19, 2007; Honolulu, Hawaii. Abstract")
14
Cumulative Incidence (%)
HORIZON Recurrent Fracture Trial: Zoledronic Acid Reduced Cumulative 3-Year Risk of Fractures by 35% Over Time 2 4 6 8 10 12 14 16 18 20 35%* Zoledronic acid (n = 1065) Placebo (n = 1062) P = .001 Cumulative Incidence (%) HORIZON Recurrent Fracture Trial: Zoledronic Acid Reduced Cumulative 3-Year Risk of Clinical Fractures by 35% Over Time Key point As illustrated in this Kaplan-Meier curve, zoledronic acid reduced the cumulative 3-year risk of clinical fractures by 35%.1 Supplemental notes Hazard Ratio, 0.65 (95% CI, 0.50–0.84). Absolute risk reduction, 5.3%. Clinical fracture defined as any fracture that came to the attention of the clinician during the course of the study, typically owing to symptoms such as pain, and including vertebral, hip, and non-vertebral fractures (non-vertebral fracture includes wrist, rib, arm, shoulder, and hip fracture; excludes finger, toe, and craniofacial fracture). References Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. 4 8 12 16 20 24 28 32 36 Month Clinical fracture defined as any fracture that came to the attention of the clinician during the course of the study, typically owing to symptoms such as pain, and including vertebral, hip, and non-vertebral fractures (excluding facial and digital fractures and fractures in abnormal bone (eg bone containing metastases). *Relative risk reduction vs placebo Lyles KW, et al. N Engl J Med. 2007;357: 14
 Placebo (n = 1062) P = Cumulative Incidence (%) HORIZON Recurrent Fracture Trial: Zoledronic Acid Reduced Cumulative 3-Year Risk of Clinical Fractures by 35% Over Time. Key point. As illustrated in this Kaplan-Meier curve, zoledronic acid reduced the cumulative 3-year risk of clinical fractures by 35%.1. Supplemental notes. Hazard Ratio, 0.65 (95% CI, 0.50–0.84). Absolute risk reduction, 5.3%. Clinical fracture defined as any fracture that came to the attention of the clinician during the course of the study, typically owing to symptoms such as pain, and including vertebral, hip, and non-vertebral fractures (non-vertebral fracture includes wrist, rib, arm, shoulder, and hip fracture; excludes finger, toe, and craniofacial fracture). References. Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract Month. Clinical fracture defined as any fracture that came to the attention of the clinician during the course of the study, typically owing to symptoms such as pain, and including vertebral, hip, and non-vertebral fractures (excluding facial and digital fractures and fractures in abnormal bone (eg bone containing metastases). *Relative risk reduction vs placebo. Lyles KW, et al. N Engl J Med. 2007;357:")
15
HORIZON Recurrent Fracture Trial: Zoledronic Acid Reduced Subsequent Fracture Risk Over Time
Placebo 35%* (16%, 50%) 46%† (8%, 68%) 20 18 13.9% (139/1062) 16 14 12 Event Rate (%) 8.6% (92/1065) 10 8 3.8% (39/1062) 6 1.7% (21/1065) 4 HORIZON Recurrent Fracture Trial: Zoledronic Acid Reduced Subsequent Fracture Risk Over Time Key point Zoledronic acid reduced risk of all clinical fractures and of clinical vertebral fractures vs placebo. Supplemental notes With respect to the primary efficacy variable (reduction in rate of clinical fracture), 231 patients had at least one adjudicated clinical fracture (92 in Reclast and 139 in placebo).1 References Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. 2 All Clinical Fractures Clinical Vertebral Fractures *P = .0012; †P = .0210, relative risk reduction vs placebo. Values above bars are cumulative event rates based on Kaplan-Meier estimates at Month 24. Lyles KW, et al. N Engl J Med. 2007;357: 15
 46%† (8%, 68%) % (139/1062) Event Rate (%) 8.6% (92/1065) % (39/1062) % (21/1065) 4. HORIZON Recurrent Fracture Trial: Zoledronic Acid Reduced Subsequent Fracture Risk Over Time. Key point. Zoledronic acid reduced risk of all clinical fractures and of clinical vertebral fractures vs placebo. Supplemental notes. With respect to the primary efficacy variable (reduction in rate of clinical fracture), 231 patients had at least one adjudicated clinical fracture (92 in Reclast and 139 in placebo).1. References. Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract All Clinical Fractures. Clinical Vertebral Fractures. *P = .0012; †P = .0210, relative risk reduction vs placebo. Values above bars are cumulative event rates based on Kaplan-Meier estimates at Month 24. Lyles KW, et al. N Engl J Med. 2007;357:")
16
Mean % Change From Baseline
HORIZON Recurrent Fracture Trial: Zoledronic Acid Significantly Increased BMD Over 3 Years Zoledronic Acid Placebo 8 6.4%* 7 4.4%† 6 5 4 Mean % Change From Baseline 3 2 1 HORIZON Recurrent Fracture Trial: Zoledronic Acid Significantly Increased BMD Over 3 Years Key point Treatment with zoledronic acid produced significant increases in BMD over 3 years at total hip and femoral neck. Supplemental notes Femoral neck: Treatment with zoledronic acid resulted in an increase of 0.76%, 2.21%, and 3.62% (least squares mean) at Months 12, 24, and 36, while treatment with placebo resulted in a decrease of 1.73%, 2.08%, and 0.73% respectively.1,2 The mean differences between zoledronic acid and placebo at Month 12 (2.49%), Month 24 (4.29%), and Month 36 (4.35%) were all statistically significant (P < for Months 12 and 24, P = for Month 36).1,2 Total Hip: Treatment with zoledronic acid resulted in an increase of 2.59%, 4.68%, and 5.45% (least squares mean) at Months 12, 24, and 36, while treatment with placebo resulted in a decrease of 1.04%, 0.74%, and 0.91% respectively.1,3 The mean differences between Reclast and placebo at Month 12 (3.64%), Month 24 (5.42%), and Month 36 (6.36%) were all statistically significant (P < .0001).1,3 References Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Data on file. Study CZOL446L2310. Novartis Pharmaceuticals Corporation. Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. -1 -2 -3 Total Hip Femoral Neck Values are least-squares mean difference, Zoledronic acid vs placebo. *P < .0001; †P = .0003; P-value computed from 2-way ANOVA with treatment and region in the model. 1. Lyles KW, et al. N Engl J Med. 2007;357: Data on file. Study CZOL446L2310. Novartis Pharmaceuticals Corporation. 3. Lyles KW, et al. Presented at: 29th ASBMR; September 16-19, 2007; Honolulu, Hawaii. Abstract 1055. 16
 at Months 12, 24, and 36, while treatment with placebo resulted in a decrease of 1.73%, 2.08%, and 0.73% respectively.1,2. The mean differences between zoledronic acid and placebo at Month 12 (2.49%), Month 24 (4.29%), and Month 36 (4.35%) were all statistically significant (P < for Months 12 and 24, P = for Month 36).1,2. Total Hip: Treatment with zoledronic acid resulted in an increase of 2.59%, 4.68%, and 5.45% (least squares mean) at Months 12, 24, and 36, while treatment with placebo resulted in a decrease of 1.04%, 0.74%, and 0.91% respectively.1,3. The mean differences between Reclast and placebo at Month 12 (3.64%), Month 24 (5.42%), and Month 36 (6.36%) were all statistically significant (P < .0001).1,3. References. Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Data on file. Study CZOL446L2310. Novartis Pharmaceuticals Corporation. Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Efficacy and safety of zoledronic acid 5 mg in preventing fractures in men and women with prevalent hip fracture: the HORIZON-Recurrent Fracture Trial. Presented at: 29th Annual Meeting of the American Society for Bone and Mineral Research; September 16-19, 2007; Honolulu, Hawaii. Abstract Total Hip. Femoral Neck. Values are least-squares mean difference, Zoledronic acid vs placebo. *P < .0001; †P = .0003; P-value computed from 2-way ANOVA with treatment and region in the model. 1. Lyles KW, et al. N Engl J Med. 2007;357: Data on file. Study CZOL446L2310. Novartis Pharmaceuticals Corporation. 3. Lyles KW, et al. Presented at: 29th ASBMR; September 16-19, 2007; Honolulu, Hawaii. Abstract")
17
HORIZON Fracture Trials: Efficacy Conclusions
Proven to reduce fractures in 2 large clinical trials HORIZON Pivotal Fracture Trial1 HORIZON Recurrent Fracture Trial2 In women with postmenopausal osteoporosis, once-yearly infusion of zoledronic acid over 3 years significantly reduced: Vertebral fractures (morphometric 70%) Hip fractures (41%) Nonvertebral fractures(25%) In patients, once-yearly infusion of zoledronic acid within 90 days after a surgical procedure for low-trauma hip fracture significantly reduced: Overall clinical fractures by 35% Clinical vertebral fractures by 46% (MORTALITY decreased) HORIZON Fracture Trials: Efficacy Conclusions Key point The HORIZON Pivotal Fracture Trial and Recurrent Fracture Trial were two large trials which met their primary endpoints and demonstrated significant reductions in fracture risk with Reclast. Supplemental notes In the Pivotal Fracture Trial involving postmenopausal women with osteoporosis, once-yearly infusion of Reclast® (zoledronic acid) 5 mg over 3 years significantly reduced the risk of vertebral fractures (70%), hip fractures (41%), and nonvertebral fractures (25%).1 In the Recurrent Fracture Trial, which included patients who had experienced a surgical procedure for low-trauma hip fracture within the last 90 days, Reclast significantly reduced the risk of overall clinical fracture by 35% and clinical vertebral fractures by 46%.2 References Black DM, Delmas PD, Eastell R, et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007;356: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Black DM, et al. N Engl J Med. 2007;356: Lyles KW, et al. N Engl J Med. 2007;357: 17
 Hip fractures (41%) Nonvertebral fractures(25%) In patients, once-yearly infusion of zoledronic acid within 90 days after a surgical procedure for low-trauma hip fracture significantly reduced: Overall clinical fractures by 35% Clinical vertebral fractures by 46% (MORTALITY decreased) HORIZON Fracture Trials: Efficacy Conclusions. Key point. The HORIZON Pivotal Fracture Trial and Recurrent Fracture Trial were two large trials which met their primary endpoints and demonstrated significant reductions in fracture risk with Reclast. Supplemental notes. In the Pivotal Fracture Trial involving postmenopausal women with osteoporosis, once-yearly infusion of Reclast® (zoledronic acid) 5 mg over 3 years significantly reduced the risk of vertebral fractures (70%), hip fractures (41%), and nonvertebral fractures (25%).1. In the Recurrent Fracture Trial, which included patients who had experienced a surgical procedure for low-trauma hip fracture within the last 90 days, Reclast significantly reduced the risk of overall clinical fracture by 35% and clinical vertebral fractures by 46%.2. References. Black DM, Delmas PD, Eastell R, et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007;356: Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357: Black DM, et al. N Engl J Med. 2007;356: Lyles KW, et al. N Engl J Med. 2007;357:")
18
Other Indications for Zoledronic Acid
GIOP Male Osteoporosis (approved) Adjuvant therapy for breast cancer
 Adjuvant therapy for breast cancer.")
19
Pre-fusion Osteoclast Multinucleated Osteoclast
RANK Ligand Is an Essential Mediator of Osteoclast Formation, Function, and Survival CFU-M Pre-fusion Osteoclast RANKL RANK Multinucleated Osteoclast Hormones Growth Factors Cytokines Activated Osteoclast In the presence of low levels of macrophage colony-stimulating factor (M-CSF), RANK ligand is an essential mediator for osteoclast formation, function, and survival in both cortical and trabecular bone throughout the skeleton.1-6 The RANK ligand polypeptide is a type II transmembrane protein found on the surface of expressing cells as well as in a proteolytically released (cleaved) soluble form.1,4 RANK ligand is expressed (both in a transmembrane and soluble form) from the osteoblast lineage cells.1,3 Additionally, RANK ligand is expressed in various cell types including, but not limited to, lymphoid cells;7 basal epithelial, luminal epithelial, and stromal cells from normal prostate8 and non-malignant breast tissue9 including mammary epithelial cells;10 tumor cells including breast cancer cells,9 prostate cancer cells, and subsequent bone metastases;8 dendritic cells; activated T cells and B cells;11 osteoclasts; mesenchymal cells; proliferative chondrocytes; early osteocytes and periosteal cells; synovial tissue;12 cardiomyocytes; vascular smooth muscle cells; endothelial cells;13 and the GI tract.14 The clinical significance of these findings is unknown. RANK ligand subsequently binds to its receptor, RANK, on immature and mature osteoclasts, which leads to maturation of pre-fusion osteoclasts to multinucleated osteoclasts, and finally to activated osteoclasts.1 RANK is another member of the TNF receptor family and is expressed on osteoclasts and osteoclast progenitors.11,15 In addition, RANK has been observed on cartilage cells (chondrocytes), mammary gland epithelial cells, and trophoblast cells.1,10,15 Boyle WJ, et al. Nature. 2003;423: Fuller K, et al. J Exp Med. 1998;188: Lacey DL, et al. Am J Pathol. 2000;157: Lacey DL, et al. Cell. 1998;93: Yasuda H, et al. Proc Natl Acad Sci U S A. 1998;95: Hofbauer LC, Schoppet M. JAMA. 2004;292: Kong Y-Y, et al. Nature. 1999;397: Brown JM, et al. Urology. 2001;57: Van Poznak C, et al. J Clin Pathol. 2006;59:56-63. Fata JE, et al. Cell. 2000;103:41-50. Anderson DM, et al. Nature. 1997;390: Crotti TN, et al. Ann Rheum Dis. 2002;61: Ueland T, et al. Circulation. 2005;111: Moschen AR, et al. Gut. 2005;54: Hsu H, et al. Proc Natl Acad Sci USA. 1999;96: Osteoblasts Bone Formation Bone Resorption Adapted from: Boyle WJ, et al. Nature. 2003;423: © 2007 Amgen. All rights reserved. Provided as an educational resource. Do not copy or distribute.
, RANK ligand is an essential mediator for osteoclast formation, function, and survival in both cortical and trabecular bone throughout the skeleton.1-6. The RANK ligand polypeptide is a type II transmembrane protein found on the surface of expressing cells as well as in a proteolytically released (cleaved) soluble form.1,4. RANK ligand is expressed (both in a transmembrane and soluble form) from the osteoblast lineage cells.1,3 Additionally, RANK ligand is expressed in various cell types including, but not limited to, lymphoid cells;7 basal epithelial, luminal epithelial, and stromal cells from normal prostate8 and non-malignant breast tissue9 including mammary epithelial cells;10 tumor cells including breast cancer cells,9 prostate cancer cells, and subsequent bone metastases;8 dendritic cells; activated T cells and B cells;11 osteoclasts; mesenchymal cells; proliferative chondrocytes; early osteocytes and periosteal cells; synovial tissue;12 cardiomyocytes; vascular smooth muscle cells; endothelial cells;13 and the GI tract.14 The clinical significance of these findings is unknown. RANK ligand subsequently binds to its receptor, RANK, on immature and mature osteoclasts, which leads to maturation of pre-fusion osteoclasts to multinucleated osteoclasts, and finally to activated osteoclasts.1. RANK is another member of the TNF receptor family and is expressed on osteoclasts and osteoclast progenitors.11,15 In addition, RANK has been observed on cartilage cells (chondrocytes), mammary gland epithelial cells, and trophoblast cells.1,10,15. Boyle WJ, et al. Nature. 2003;423: Fuller K, et al. J Exp Med. 1998;188: Lacey DL, et al. Am J Pathol. 2000;157: Lacey DL, et al. Cell. 1998;93: Yasuda H, et al. Proc Natl Acad Sci U S A. 1998;95: Hofbauer LC, Schoppet M. JAMA. 2004;292: Kong Y-Y, et al. Nature. 1999;397: Brown JM, et al. Urology. 2001;57: Van Poznak C, et al. J Clin Pathol. 2006;59: Fata JE, et al. Cell. 2000;103: Anderson DM, et al. Nature. 1997;390: Crotti TN, et al. Ann Rheum Dis. 2002;61: Ueland T, et al. Circulation. 2005;111: Moschen AR, et al. Gut. 2005;54: Hsu H, et al. Proc Natl Acad Sci USA. 1999;96: Osteoblasts. Bone Formation. Bone Resorption. Adapted from: Boyle WJ, et al. Nature. 2003;423: © 2007 Amgen. All rights reserved. Provided as an educational resource. Do not copy or distribute.")
20
RANK Ligand Plays a Key Role in Osteoporosis and Other Conditions of Bone Loss and Destruction
Postmenopausal Osteoporosis Treatment-Induced Bone Loss Cancer-Related Bone Destruction Bone Erosion of RA RANK ligand plays a key role in osteoclast-mediated bone loss and destruction across a broad range of conditions.1,2 The effects of RANK ligand are physiologically counterbalanced by the soluble receptor, OPG.1 When RANK ligand overwhelms the effects of OPG, the imbalance in the bone remodeling process results in bone loss and destruction including the following1,2: Postmenopausal osteoporosis.3 Treatment-induced bone loss resulting from sex hormone ablative therapies, chronic exposure to glucocorticoids, and immunosuppression.1,4,5 Rheumatoid arthritis.6,7 Bone metastases.8,9 Hofbauer LC, Schoppet M. JAMA. 2004;292: Kostenuik PJ. Curr Opin Pharmacol. 2005;5: Eghbali-Fatourechi G, et al. J Clin Invest. 2003;111: Hofbauer LC, et al. Endocrinology. 1999;140: Theriault RL. Oncology. 2004;18(suppl 3):11-15. Gravallese EM, et al. Arthritis Rheum. 2000;43: Kong Y-Y, et al. Nature. 1999;420: Roodman GD. N Engl J Med. 2004;350: Kitazawa S, et al. J Pathol. 2002;198: Hofbauer LC, Schoppet M. JAMA. 2004;292: Eghbali-Fatourechi G, et al. J Clin Invest. 2003;111: Hofbauer LC, et al. Endocrinology. 1999;140: Theriault RL. Oncology. 2004;18(suppl 3):11-15. Gravallese EM, et al. Arthritis Rheum. 2000;43: Roodman GD. N Engl J Med. 2004;350: Kong Y-Y, et al. Nature. 1999;402: Kitazawa S, et al. J Pathol. 2002;198:
: Gravallese EM, et al. Arthritis Rheum. 2000;43: Kong Y-Y, et al. Nature. 1999;420: Roodman GD. N Engl J Med. 2004;350: Kitazawa S, et al. J Pathol. 2002;198: Hofbauer LC, Schoppet M. JAMA. 2004;292: Eghbali-Fatourechi G, et al. J Clin Invest. 2003;111: Hofbauer LC, et al. Endocrinology. 1999;140: Theriault RL. Oncology. 2004;18(suppl 3): Gravallese EM, et al. Arthritis Rheum. 2000;43: Roodman GD. N Engl J Med. 2004;350: Kong Y-Y, et al. Nature. 1999;402: Kitazawa S, et al. J Pathol. 2002;198:")
21
Denosumab and Cancer Induced Bone Loss
Denosumab and AI in non metastatic breast cancer. Increased BMD vs Placebo at all sites Denosumab and breast cancer mets. Decreased BTM and skeletal related events comparable to IV ZOL Denosumab and treatment of prostate cancer and bone mets. Decreased BTMS compared to IV (ZOL).
.")
22
Denosumab in Osteoporosis
Denosumab fracture trial.( FREEDOM ). Study characteristics. Primary outcome is reduction of new vertebral fractures. Secondary endpoints include risk of non vertebral fractures and hip fractures. 7686 patients enrolled. Age between yrs, Mean age =72yrs. Mean T score at lumbar spine or total hip = -2.8 and total hip % had prevalent fractures at baseline. 80 % completed the trial.. Fracture reduction showed a reduction of vertebral fractures of 61 % at 1year.78% year 2 and 65 % year 3. Non vert fracture reduction was 20%. Hip Fracture reduction was 40%. A/Es showed no differences particular with regard to malignancy, infection. No cases of ONJ reported. No delayed fracture healing seen. Data not shown included changes in PTH , serum calcium bone biopsies, and worsening of fractures ASBMR Sep 2008
. Study characteristics. Primary outcome is reduction of new vertebral fractures. Secondary endpoints include risk of non vertebral fractures and hip fractures patients enrolled. Age between yrs, Mean age =72yrs. Mean T score at lumbar spine or total hip = -2.8 and total hip % had prevalent fractures at baseline. 80 % completed the trial.. Fracture reduction showed a reduction of vertebral fractures of 61 % at 1year.78% year 2 and 65 % year 3. Non vert fracture reduction was 20%. Hip Fracture reduction was 40%. A/Es showed no differences particular with regard to malignancy, infection. No cases of ONJ reported. No delayed fracture healing seen. Data not shown included changes in PTH , serum calcium bone biopsies, and worsening of fractures. ASBMR Sep")
23
FRAX®: Gauging 10-Year Fracture Probability
Slide ID: 22790 FRAX®: Gauging 10-Year Fracture Probability Key point This slide describes the new FRAX tool for calculating 10-year fracture risk. The tool, from the World Health Organization and Sheffield University, was designed to help identify those patients that might benefit from osteoporosis treatment. Supplemental notes This example is of a 67 year-old-woman with femoral neck t-score -2.1, history of fracture, and who is a smoker. Her risk of major osteoporotic fracture in the next 10 years is 29%, of hip fracture is 6.0%.

24
NOF Guidelines: When to Treat
Slide ID: 22792 NOF guidelines: When to Treat This slide describes the new guidelines from the National Osteoporosis Foundation regarding who and when to treat. Absolute fracture risk methodology assures that people with the highest fracture risk get treated. Those at highest risk include postmenopausal women and older men with a diagnosis of osteoporosis, based on a BMD test T-score of -2.5 or lower, or those with a clinical diagnosis based on having sustained a hip or spine fracture. Absolute fracture risk calculations help to resolve many of the questions about management of low bone mass (osteopenia), which is a T-score between -1.0 and -2.5 on BMD test. In the past, there was much uncertainty about when to treat people with osteopenia. Reference National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. National Osteoporosis Foundation; Washington, DC
, which is a T-score between -1.0 and -2.5 on BMD test. In the past, there was much uncertainty about when to treat people with osteopenia. Reference. National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. National Osteoporosis Foundation; Washington, DC")
25
Debated Topics Osteonecrosis of the Jaw (ONJ)
Atrial Fibrillation and BP’s Atypical Fractures and BP’s Drug Holiday Combination/ sequential therapy eg BP followed by anabolic . Giant Osteoclasts with BP’s

26
Observations Regarding Osteonecrosis of the Jaw
April 20, 2017 Observations Regarding Osteonecrosis of the Jaw 26

27
Osteonecrosis of the Jaw
April 20, 2017 Although there is no universally accepted definition of osteonecrosis of the jaw (ONJ), several authors have observed that ONJ is an oral cavity lesion characterized by 1 or more spots of bare alveolar or hard palate bone, in the absence of local malignancy or radiation therapy to the head or neck.1–6 Persisting for 6-8weeks. Known risk factors for ONJ include: IV bisphosphonates Duration of treatment Dental extraction Diagnosis of cancer Concomitant therapies (eg, chemotherapy, radiotherapy, and corticosteroids) Poor oral hygiene Comorbid disorders (eg, pre-existing dental disease, anemia, coagulopathy, and infection) The mechanism by which ONJ occurs is currently uncertain.1 Osteonecrosis of the Jaw Osteonecrosis of the jaw (ONJ) is an oral cavity lesion characterized by 1 or more spots of bare alveolar or hard palate bone, in the absence of local malignancy or radiation therapy to the head or neck.1–6 Patients with ONJ may present without symptoms or ONJ may be swollen and painful. The patient may notice rough spots or a numb sensation in the area of the lesion. Clinical findings may include bare bone, inflammation, necrotic tissue, infection, and fistulas with purulent discharge. The recent dental history may include a tooth extraction or other dental surgery.1–3 According to the Prescribing Information for FOSAMAX® (alendronate sodium), known risk factors for ONJ include diagnosis of cancer, concomitant therapies (eg, chemotherapy, radiotherapy, and corticosteroids), comorbid disorders including pre-existing dental disease (such as periodontitis), and poor oral hygiene. The mechanism by which ONJ occurs is currently uncertain.1 References: 1. Migliorati CA, Casiglia J, Epstein J, et al. Managing the care of patients with bisphosphonate-associated osteonecrosis: an American Academy of Oral Medicine position paper. J Am Dent Assoc. 2005;136:1658–1668. 2. Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL: Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg. 2004;62:527–534. 3. Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg. 2005;63:1567–1575. 4. Bamias A, Kastritis E, Bamia C, et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. 2005;23:8580–8587. 5. Lenz JH, Steiner-Krammer B, Schmidt W, et al. Does avascular necrosis of the jaws in cancer patients only occur following treatment with bisphosphonates? J Craniomaxillofac Surg. 2005;33:395–403. 6. Farrugia MC, Summerlin DJ, Krowiak E, et al. Osteonecrosis of the mandible or maxilla associated with the use of new generation bisphosphonates. Laryngoscope. 2006;116:115–120. 27
, several authors have observed that ONJ is an oral cavity lesion characterized by 1 or more spots of bare alveolar or hard palate bone, in the absence of local malignancy or radiation therapy to the head or neck.1–6. Persisting for 6-8weeks. Known risk factors for ONJ include: IV bisphosphonates. Duration of treatment. Dental extraction. Diagnosis of cancer. Concomitant therapies (eg, chemotherapy, radiotherapy, and corticosteroids) Poor oral hygiene. Comorbid disorders (eg, pre-existing dental disease, anemia, coagulopathy, and infection) The mechanism by which ONJ occurs is currently uncertain.1. Osteonecrosis of the Jaw. Osteonecrosis of the jaw (ONJ) is an oral cavity lesion characterized by 1 or more spots of bare alveolar or hard palate bone, in the absence of local malignancy or radiation therapy to the head or neck.1–6. Patients with ONJ may present without symptoms or ONJ may be swollen and painful. The patient may notice rough spots or a numb sensation in the area of the lesion. Clinical findings may include bare bone, inflammation, necrotic tissue, infection, and fistulas with purulent discharge. The recent dental history may include a tooth extraction or other dental surgery.1–3. According to the Prescribing Information for FOSAMAX® (alendronate sodium), known risk factors for ONJ include diagnosis of cancer, concomitant therapies (eg, chemotherapy, radiotherapy, and corticosteroids), comorbid disorders including pre-existing dental disease (such as periodontitis), and poor oral hygiene. The mechanism by which ONJ occurs is currently uncertain.1. References: 1. Migliorati CA, Casiglia J, Epstein J, et al. Managing the care of patients with bisphosphonate-associated. osteonecrosis: an American Academy of Oral Medicine position paper. J Am Dent Assoc. 2005;136:1658– Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL: Osteonecrosis of the jaws associated with the use of. bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg. 2004;62:527– Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of. the jaws: risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg. 2005;63:1567– Bamias A, Kastritis E, Bamia C, et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. 2005;23:8580– Lenz JH, Steiner-Krammer B, Schmidt W, et al. Does avascular necrosis of the jaws in cancer patients only occur. following treatment with bisphosphonates J Craniomaxillofac Surg. 2005;33:395– Farrugia MC, Summerlin DJ, Krowiak E, et al. Osteonecrosis of the mandible or maxilla associated with the use of. new generation bisphosphonates. Laryngoscope. 2006;116:115–")
28
ONJ: Clinical Presentation
April 20, 2017 Clinical Features of Suspected ONJ Exposed bone in maxillofacial area that occurs in association with dental surgery or occurs spontaneously, with no evidence of healing* Working Diagnosis of ONJ No evidence of healing after 6 weeks of appropriate evaluation and dental care No evidence of metastatic disease in the jaw or osteoradionecrosis Typical locations of ONJ: Top: posterior lingual part of mandible Bottom: nonhealing extraction socket Clinical Features of Suspected ONJ Exposed bone in maxillofacial area that occurs in association with dental surgery or occurs spontaneously, with no evidence of healing* Working Diagnosis of ONJ No evidence of healing after 6 weeks of appropriate evaluation and dental care No evidence of metastatic disease in the jaw or osteoradionecrosis *Refer for appropriate dental evaluation and care as soon as possible. *Refer for appropriate dental evaluation and care as soon as possible. 28

29
Proposed Mechanisms of ONJ
Inhibition of angiogenesis Decreased bone turnover impeding healing and new bone formation. Mandible, maxilla and tooth eruption differs developmentally and anatomically from cancellous and cortical bone in other sites. Immune system may play a role in mechanism ???? 29

30
ONJ and Bisphosphonates
April 20, 2017 Incidence of ONJ Occurs rarely Reported in patients not taking bisphosphonates1–3 No ICD9 code available for diagnosis Bisphosphonate-associated ONJ has predominantly occurred in cancer patients receiving IV bisphosphonates4: ONJ has been reported rarely in osteoporosis patients taking alendronate and other oral bisphosphonates (ibandronate and risedronate zolendronate).5–7 ONJ was added to the “Precautions” section of the Prescribing Information for ALL IV and oral bisphosphonates (effective July 2005 for alendronate). Since their market introduction, over 191 million total prescriptions have been dispensed for alendronate sodium, risedronate, and ibandronate; 77% of these have been dispensed as alendronate.8 ONJ and Bisphosphonates The risk of ONJ has been greatest in patients receiving IV bisphosphonates, which are generally used for the treatment of hypercalcemia and bone pain associated with bone metastases in cancer patients.1 ONJ has been reported rarely in patients taking oral bisphosphonates for osteoporosis and Paget’s disease of bone.2,3 The first published reports linking ONJ with bisphosphonate use occurred in 2003 and cited only IV pamidronate and zoledronate.4,5 A review by Woo et al in May 2006 cited a total of 368 patients treated with bisphosphonates who were diagnosed with ONJ. Seventeen (17) patients were taking an oral bisphosphonate only and 4 patients were taking both an IV and oral bisphosphonate.3 ONJ has been reported very rarely in postmarketing use with alendronate and other oral bisphosphonates (ibandronate and risedronate).3,6,7 ONJ was added to the “Precautions” section of the Prescribing Information for ALL IV and oral bisphosphonates (effective July 2005 for alendronate). Since their market introduction, over 191 million total prescriptions have been dispensed for FOSAMAX® (alendronate sodium), Actonel, and Boniva; 77% of these have been dispensed as alendronate.8 ONJ occurs rarely, is not coded as a separate disease, and is ill defined. No prospective clinical trials exist using ONJ as an end point, making determination of causality of ONJ by bisphosphonates currently very difficult. References: 1. Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL: Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg. 2004; 62:527–534. 2. Oral Health and Bone Disease. National Institutes of Health Osteoporosis and Related Bone Diseases—National Resource Center. Revised November 2005; Available at: Accessed May 1, 2006. 3. Woo SB, Hellstein JW, Kalmar JR. Systemic review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med. 2006;144:753–761. 4. Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003;61:1115–1117. 5. Migliorati CA. Bisphosphonates and oral cavity avascular bone necrosis. J Clin Oncol. 2003;21:4253–4254. 6. Ruggiero S, Gralow J, Marx RE, et al. Practical guidelines for the prevention, diagnosis, and treatment of osteonecrosis of the jaw in patients with cancer. JOP. 2006;2:7–14. 7. Bamias A, Kastritis E, Bamia C, et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. 2005;23:8580–8587. 8. IMS HEALTH. NPA Plus™ May 2006. 30
.5–7. ONJ was added to the Precautions section of the Prescribing Information for ALL IV and oral bisphosphonates (effective July 2005 for alendronate). Since their market introduction, over 191 million total prescriptions have been dispensed for alendronate sodium, risedronate, and ibandronate; 77% of these have been dispensed as alendronate.8. ONJ and Bisphosphonates. The risk of ONJ has been greatest in patients receiving IV bisphosphonates, which are generally used for the treatment of hypercalcemia and bone pain associated with bone metastases in cancer patients.1 ONJ has been reported rarely in patients taking oral bisphosphonates for osteoporosis and Paget’s disease of bone.2,3. The first published reports linking ONJ with bisphosphonate use occurred in 2003 and cited only IV pamidronate and zoledronate.4,5 A review by Woo et al in May 2006 cited a total of 368 patients treated with bisphosphonates who were diagnosed with ONJ. Seventeen (17) patients were taking an oral bisphosphonate only and 4 patients were taking both an IV and oral bisphosphonate.3. ONJ has been reported very rarely in postmarketing use with alendronate and other oral bisphosphonates (ibandronate and risedronate).3,6,7 ONJ was added to the Precautions section of the Prescribing Information for ALL IV and oral bisphosphonates (effective July 2005 for alendronate). Since their market introduction, over 191 million total prescriptions have been dispensed for FOSAMAX® (alendronate sodium), Actonel, and Boniva; 77% of these have been dispensed as alendronate.8. ONJ occurs rarely, is not coded as a separate disease, and is ill defined. No prospective clinical trials exist using ONJ as an end point, making determination of causality of ONJ by bisphosphonates currently very difficult. References: 1. Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL: Osteonecrosis of the jaws associated with the use of. bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg. 2004; 62:527– Oral Health and Bone Disease. National Institutes of Health Osteoporosis and Related Bone Diseases—National. Resource Center. Revised November 2005; Available at: Accessed. May 1, Woo SB, Hellstein JW, Kalmar JR. Systemic review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med. 2006;144:753– Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003;61:1115– Migliorati CA. Bisphosphonates and oral cavity avascular bone necrosis. J Clin Oncol. 2003;21:4253– Ruggiero S, Gralow J, Marx RE, et al. Practical guidelines for the prevention, diagnosis, and treatment of osteonecrosis. of the jaw in patients with cancer. JOP. 2006;2:7– Bamias A, Kastritis E, Bamia C, et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. 2005;23:8580– IMS HEALTH. NPA Plus™ May")
31
Experience with Bisphosphonates in Clinical Trials
April 20, 2017 In controlled clinical trials involving more than 17,000 patients, contributing as much as 10 years’ data with alendronate,1,2 there have been no reports of ONJ: Includes ≈3,000 osteoporosis patients taking alendronate for 3 to 5 years Includes ≈800 osteoporosis patients taking alendronate for 8 to 10 years Includes 167 patients taking alendronate in a 2-year study of patients with pre-existing controlled periodontal disease (investigational use) Zoledronic acid osteoporosis trial (HORIZON PFT) there was 1 case in the placebo and 1 case in the treated group. Cases were marred by underlying disease and oral lesions. Experience with Alendronate in Clinical Trials In controlled clinical trials involving more than 17,000 patients, contributing as much as 10 years’ data with alendronate,1–4 there have been no reports of ONJ: Include ≈3,000 osteoporosis patients taking alendronate for 3 to 5 years Includes ≈800 osteoporosis patients taking alendronate for 8 to 10 years Includes 167 patients taking alendronate in a 2-year study of patients with pre-existing periodontal disease (investigational use) There has been no reports of ONJ in osteoporotic patients in controlled clinical trials for alendronate, including: Two studies with 10 years of experience: Phase III study: About 597 patients randomized to alendronate (Years 1 to 3) About 346 patients randomized to alendronate in the 1st extension (Years 4 to 5) About 197 patients randomized to alendronate in the 2nd extension (Years 6 to 7) About 164 patients treated with alendronate in the 3rd extension (Years 8 to10)1 Fracture Intervention Trial (FIT) and FIT Long-term Extension (FLEX) studies: FIT Vertebral Fracture Arm (VFA): About 1,022 patients randomized to alendronate for 3 years (average 2.9 years)2 FIT Clinical Fracture Arm (CFA): About 2,214 patients randomized to alendronate for 4 years (average 4.2 years)3 FLEX: About 662 patients treated with alendronate in the 5-year extension of FIT4 References: 1. Bone HG, Hosking D, Devogelaer J-P, et al, for the Alendronate Phase III Osteoporosis Treatment Study Group. Ten years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med. 2004;350:1189–1199. 2. Black DM, Cummings SR, Karpf DB, et al, for the Fracture Intervention Trial Research Group. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet. 1996;348:1535–1541. 3. Cummings SR, Black DM, Thompson DE, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA. 1998;280:2077–2082. 4. Black D, Schwartz A, Ensrud K, et al. A 5 year randomized trial of the long-term efficacy and safety of alendronate: the FIT Long-term Extension (FLEX). J Bone Miner Res. 2004;suppl 1:S45. 1. Bone HG et al. N Engl J Med. 2004;350:1189–1199. 2. Black D et al. J Bone Miner Res. 2004;suppl 1:S45. 31
 Zoledronic acid osteoporosis trial (HORIZON PFT) there was 1 case in the placebo and 1 case in the treated group. Cases were marred by underlying disease and oral lesions. Experience with Alendronate in Clinical Trials. In controlled clinical trials involving more than 17,000 patients, contributing as much as 10 years’ data with alendronate,1–4 there have been no reports of ONJ: Include ≈3,000 osteoporosis patients taking alendronate for 3 to 5 years. Includes ≈800 osteoporosis patients taking alendronate for 8 to 10 years. Includes 167 patients taking alendronate in a 2-year study of patients with pre-existing periodontal disease. (investigational use) There has been no reports of ONJ in osteoporotic patients in controlled clinical trials for alendronate, including: Two studies with 10 years of experience: Phase III study: About 597 patients randomized to alendronate (Years 1 to 3) About 346 patients randomized to alendronate in the 1st extension (Years 4 to 5) About 197 patients randomized to alendronate in the 2nd extension (Years 6 to 7) About 164 patients treated with alendronate in the 3rd extension (Years 8 to10)1. Fracture Intervention Trial (FIT) and FIT Long-term Extension (FLEX) studies: FIT Vertebral Fracture Arm (VFA): About 1,022 patients randomized to alendronate for 3 years (average 2.9 years)2. FIT Clinical Fracture Arm (CFA): About 2,214 patients randomized to alendronate for 4 years (average 4.2 years)3. FLEX: About 662 patients treated with alendronate in the 5-year extension of FIT4. References: 1. Bone HG, Hosking D, Devogelaer J-P, et al, for the Alendronate Phase III Osteoporosis Treatment Study Group. Ten. years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med. 2004;350:1189– Black DM, Cummings SR, Karpf DB, et al, for the Fracture Intervention Trial Research Group. Randomised trial of. effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet. 1996;348:1535– Cummings SR, Black DM, Thompson DE, et al. Effect of alendronate on risk of fracture in women with low. bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA. 1998;280:2077– Black D, Schwartz A, Ensrud K, et al. A 5 year randomized trial of the long-term efficacy and safety of alendronate: the. FIT Long-term Extension (FLEX). J Bone Miner Res. 2004;suppl 1:S Bone HG et al. N Engl J Med. 2004;350:1189– Black D et al. J Bone Miner Res. 2004;suppl 1:S")
32
Warnings and Precautions: Osteonecrosis of the Jaw (1/2)
Osteonecrosis of the jaw (ONJ) has been reported rarely in patients treated with bisphosphonates, including zoledronic acid Most cases have been in cancer patients undergoing dental procedures Some cases have occurred in patients with PMO treated with either oral or IV bisphosphonates Routine oral exam should be provided by the prescriber prior to treatment While on treatment, patients with concomitant risk factors should avoid invasive dental procedures if possible The clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment Warnings and Precautions: Osteonecrosis of the Jaw (1/2) A dental examination with appropriate preventive dentistry should be considered prior to treatment with bisphosphonates in patients with a history of concomitant risk factors (e.g., cancer, chemotherapy, corticosteroids, poor oral hygiene) While on treatment, patients with concomitant risk factors should avoid invasive dental procedures if possible For patients who develop ONJ while on bisphosphonate therapy, dental surgery may exacerbate the condition For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ The clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment
 has been reported rarely in patients treated with bisphosphonates, including zoledronic acid. Most cases have been in cancer patients undergoing dental procedures. Some cases have occurred in patients with PMO treated with either oral or IV bisphosphonates. Routine oral exam should be provided by the prescriber prior to treatment. While on treatment, patients with concomitant risk factors should avoid invasive dental procedures if possible. The clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment. Warnings and Precautions: Osteonecrosis of the Jaw (1/2) A dental examination with appropriate preventive dentistry should be considered prior to treatment with bisphosphonates in patients with a history of concomitant risk factors (e.g., cancer, chemotherapy, corticosteroids, poor oral hygiene) While on treatment, patients with concomitant risk factors should avoid invasive dental procedures if possible. For patients who develop ONJ while on bisphosphonate therapy, dental surgery may exacerbate the condition. For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ. The clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment.")
33
Further Reading on ONJ Consensus practice guidelines on ONJ.
Sambrook P. Nature Clinical Practice Rheumatology. Jan 2009 ONJ .Who gets it, and why? Reid I .BONE 44 (2009) 4-10.
")
34
Atrial Fibrillation

35
Atrial Fibrillation Atrial Fibrillation with zoledronic acid in the HORIZON PFT Adjudicated SAEs of atrial fibrillation occurred in 1.3% of patients (50 out of 3862) compared to 0.4% (17 out of 3852) in the placebo group Overall incidence of atrial fibrillation AEs was 2.5% of zoledronic acid patients (96 out of 3862) vs 1.9% (75 out of 3852) in placebo Over 90% of these events in both groups occurred more than a month after the infusion In an ECG sub-study ECG measurements were performed on a subset of 559 patients before and 9 to 11 days after treatment There was no difference in the incidence of atrial fibrillation between treatment groups suggesting these events were not related to the acute infusions Adverse Reactions Adjudicated by independent panel of cardiology experts
 compared to 0.4% (17 out of 3852) in the placebo group. Overall incidence of atrial fibrillation AEs was 2.5% of zoledronic acid patients (96 out of 3862) vs 1.9% (75 out of 3852) in placebo. Over 90% of these events in both groups occurred more than a month after the infusion. In an ECG sub-study. ECG measurements were performed on a subset of 559 patients before and 9 to 11 days after treatment. There was no difference in the incidence of atrial fibrillation between treatment groups suggesting these events were not related to the acute infusions. Adverse Reactions. Adjudicated by independent panel of cardiology experts.")
36
Atrial Fibrillation November 12th 2008, FDA reported that there is no clear association with bisphosphonate use and atrial fibrillation based on reviews from 4 pharmaceutical sponsor’s placebo controlled clinical trial’s data. This evaluation included19,687bisphosphonate treated patients and 18,358 placebo treated patients.

37
FLEX-Lumbar Spine BMD Changes From FIT Baseline (mITT)
Mean Percent Change ( SE) in Lumbar Spine BMD From Original FIT Baseline 16 14 12 10 Mean Percent Change 8 6 4 2 12 24 36 48 60 72 84 96 108 120 Month P<0.001 ALN/ALN vs ALN/PBO. = ALN/Placebo = ALN/ALN (Pooled 5 mg and 10 mg groups)
 in Lumbar Spine BMD. From Original FIT Baseline Mean Percent Change Month. P<0.001 ALN/ALN vs ALN/PBO. = ALN/Placebo. = ALN/ALN (Pooled 5 mg and 10 mg groups)")
38
FLEX-Total Hip BMD Changes From FIT Baseline (mITT)
Mean Percent Change ( SE) in Total Hip BMD From Original FIT Baseline –1 1 2 3 4 5 12 24 36 48 60 72 84 96 108 120 Mean Percent Change Month P<0.001 ALN/ALN vs ALN/PBO. = ALN/Placebo = ALN/ALN (Pooled 5 mg and 10 mg groups)
 in Total Hip BMD. From Original FIT Baseline. – Mean Percent Change. Month. P<0.001 ALN/ALN vs ALN/PBO. = ALN/Placebo. = ALN/ALN (Pooled 5 mg and 10 mg groups)")
39
Drug Holiday:Fractures (Exploratory) Cumulative Incidence During FLEX
ALN/PBO (N = 437) ALN/ALN (N = 662) Any clinical (symptomatic) 93 (21.9) 132 (20.6) Clinical non-vertebral 83 (19.6) 125 (19.5) Hip 12 (2.9) 20 (3.1) Forearm 19 (4.5) 31 (4.9) Clinical vertebral 23 (5.4) 16 (2.5)* Morphometric vertebral 46 (11.3) 60 (9.8) *P=0.011 vs ALNPBO. **P=0.006 vs ALN/PBO.
 ALN/ALN (N = 662) Any clinical (symptomatic) 93 (21.9) 132 (20.6) Clinical non-vertebral. 83 (19.6) 125 (19.5) Hip. 12 (2.9) 20 (3.1) Forearm. 19 (4.5) 31 (4.9) Clinical vertebral. 23 (5.4) 16 (2.5)* Morphometric vertebral. 46 (11.3) 60 (9.8) *P=0.011 vs ALNPBO. **P=0.006 vs ALN/PBO.")
40
Atypical Fractures in Pts on Long Term Bisphosphonates
Odvina et al ;Spontaneous non Vert Fractures with severely suppressed bone turnover. Lane et al Association of long term BP use and “insufficiency” fractures of the femur Retrospective case control study: X-ray pattern shows transverse fracture sub trochanteric in areas of thickened cortices. OR = 4.4 and Xray association OR =15.3. Solomon et al : BP use and non union of humeral fractures. ( days post Fx). OR =2.37. Cause and effect ?? Association??/ Possible etiologies Identification of those at risk Practice change
. OR =2.37. Cause and effect Association / Possible etiologies. Identification of those at risk. Practice change.")
41
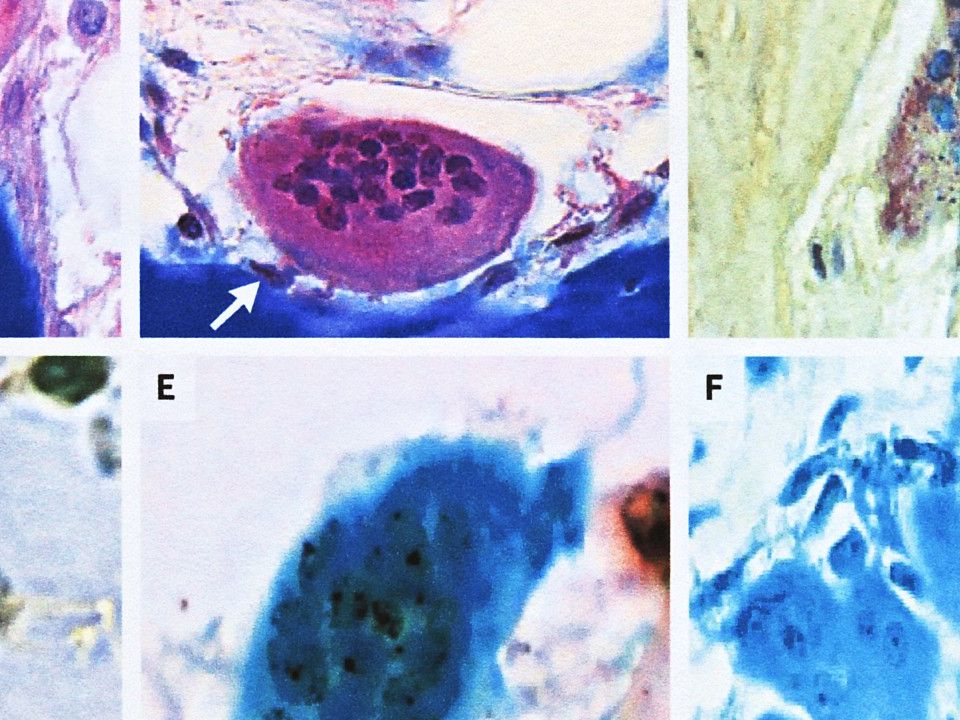
Bisphosphonates and Multinucleated Osteoclasts (Oc’s)
Retrospective bone biopsy study from 51 specimens. Patients on 10mg alendronate for years. Giant hypernucleated Oc’s which have prolonged apoptosis (27%) Osteoclast count increased 2.6x vs placebo. BMD increased on Rx 3-4%. Normal Oc’s may be poor bone resorbers. Giant Oc’s compensatory response??? Weinstein et al. NEJM Jan 2009
 Osteoclast count increased 2.6x vs placebo. BMD increased on Rx 3-4%. Normal Oc’s may be poor bone resorbers. Giant Oc’s compensatory response Weinstein et al. NEJM Jan")
44
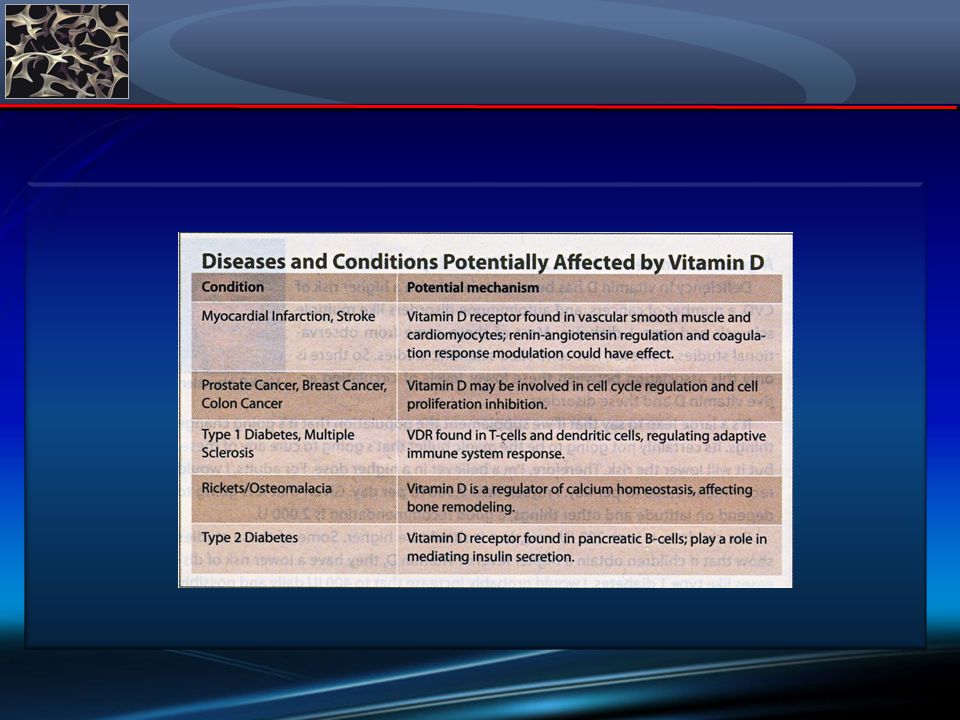
Other Disease States: Role of Vitamin D: Osteoarthritis2
Falls/neuromuscular function3 Multiple sclerosis4 Fibromyalgia5 Type I diabetes6 Cardiovascular disease6 Periodontal disease7 Cancers: Breast prostate Role of Vitamin D Much has been written in the literature on the role of vitamin D deficiency in other common chronic and serious conditions, including some common cancers, type 1 diabetes, and cardiovascular disease.1–7 Epidemiologic studies suggest that exposure to sunlight, which enhances the production of vitamin D3 in the skin, is important in preventing many chronic diseases.5 1. Women to women. Available at: Accessed July 6, 2005. 2. Lane NE et al. Arthritis Rheum. 1999;42:854–860. 3. Bischoff-Ferrari HA et al. JAMA. 2004;291:1999–2006. 4. Munger KL et al. Neurology. 2004;62:60–65. 5. Plotnikoff GA et al. Mayo Clin Proc. 2003;78:1463–1470. 6. Holick MF. Am J Clin Nutr. 2004;79:362–371. 7. Dietrich T et al. Am J Clin Nutr ;80:108–113. References: 1. Women to Women. Vitamin D—the new breakthrough? Available at: Accessed July 6, 2005. 2. Lane NE, Gore LR, Cummings SR, et al, for the Study of Osteoporotic Fractures Research Group. Serum vitamin D levels and incident changes of radiographic hip osteoarthritis: a longitudinal study. Arthritis Rheum. 1999;42:854–860. 3. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, et al. Effect of vitamin D on falls: a meta-analysis. JAMA. 2004;291:1999–2006. 4. Munger KL, Zhang SM, O’Reilly, et al. Vitamin D intake and incidence of multiple sclerosis. Neurology. 2004;62:60–65. 5. Plotnikoff GA, Quigley JM. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 2003;78:1463–1470. 6. Holick MF. Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004;79:362–371. 7. Dietrich T, Joshipura KJ, Dawson-Hughes B, Bischoff-Ferrari HA. Association between serum concentrations of 25-hydroxyvitamin D3 and periodontal disease in the US population. Am J Clin Nutr. 2004;80:108–113.

46
25Hydroxy Vitamin D and Risk of Myocardial Infarction in Men
Men deficient in Vit D < 15ng/ml had a 2.09 increased relative risk than those >30ng/ml for MI. Men with intermediate levels ng/ml had an increased relative risk of for MI. Men with levels of ng/ml had an increased relative risk of 1.43 for MI. Giovannucci E et al Arch Intern Med 168,

47
3258 male and female patients scheduled for coronary angiography
Independent Association of Low Serum 25 Hydroxy Vitamin D levels with All-Cause and Cardiovascular Mortality 3258 male and female patients scheduled for coronary angiography 25 OH D, and 1,25 OH 2 D levels measured as quartiles over a mean of 7.7yrs. All cause mortality at 7.6 and 13.3 ngs/ml = x higher respectively. Similar for CV mortality. Both compared to mean 28.4ng/ml. Similar results occurred with the lowest 1.25OHD 2 quartile. Dobnig et al. Arch Intern Med 168,12: 1340 –

48
Thank You

Similar presentations

>")

:>")

 FOSALAN (alendronate) is a trademark.>")

>")









 on Aromatase Inhibitor-Associated Bone Loss in Postmenopausal Women with Early Breast Cancer Receiving Adjuvant Letrozole:>")


