Download presentation
Presentation is loading. Please wait.

1
History Common Complaints: Abdominal pain Change in appetite
Common Complaints: Abdominal pain Change in appetite Dysphagia/Odynophagia Difficult or painful swallowing Nausea/Vomiting Jaundice Fever Change in bowel habits Melena/Hematochezia Dark tarry or red stools Hemorrhoids

2
Gastrointestinal symptoms
1.Dysphagia difficulty in swallowing,eg:-Achalasia, esophagesophageal stricture, and spasm. 2.odenophagiapain on swallowing-esophageal motility disorders,stricture,esophagitis,candida infection, pill induced, 3.Changes in the bowel function Alternate diarrhea or constipation, eg:-IBD, Ulcerative colitis, Gastoenteritis, amoebiasis Melenablack tarry color stool(Upper GIT bleedingin case of Gastritis,GERDPUD,esophageal varices, HematocheziaLGIT bleeding in case of colon cancer, Diverticulitis,Ulcerative colitis,Crohn’s disease,Hemorrhaids. 4.Heart burn, acid reflux, Gastritis and alcoholic induced 5.Indigestiondyspepsia it is epigastric burn, nausea distension occur after drinking or eating. 6.Jaundiceyellowish discoloration of skin and sclera, liver and biliary tract disease.

3
Dysuria, frequency, urgency, hematuria, incontinence
Genitourinary symptoms Dysuria, frequency, urgency, hematuria, incontinence Gynecological symptoms Vaginal discharge, vaginal bleeding General Fever, Lightheadedness Weight loss, Loss of appetite,

4
Tell me more about your pain….”
Location Quality Severity Onset Duration Modifying factors Change over time

5
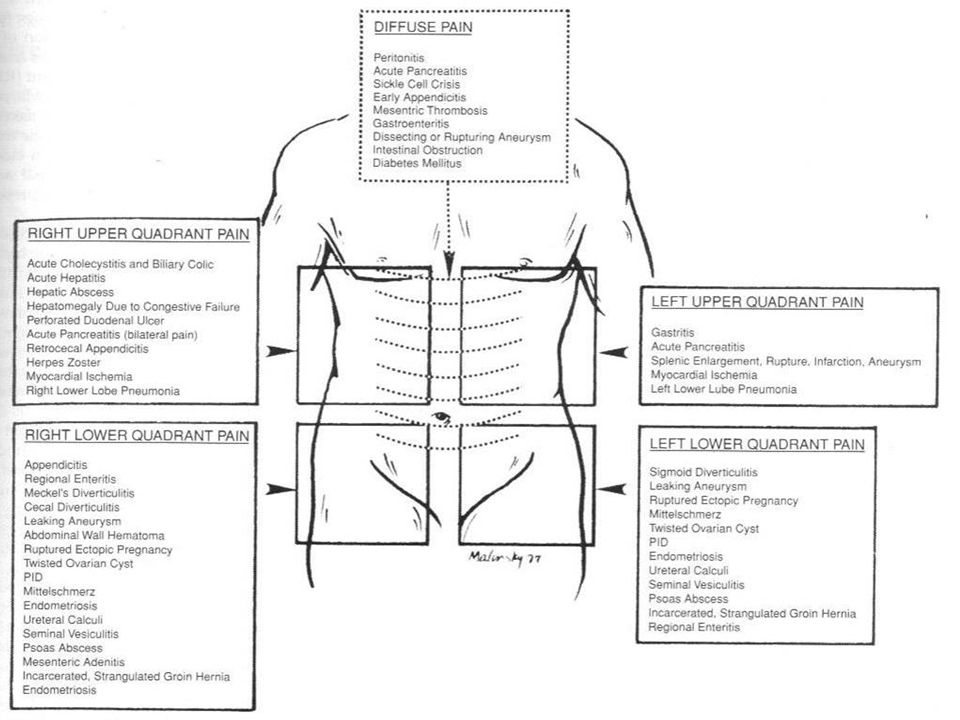
Referred Pain Pain or discomfort that is perceived at a site distant from the affected organ because of overlapping transmission pathways Also reflects embryologic origin: subdiaphragmatic irritation -> ipsilateral supraclavicular or shoulder pain gynecologic pathology -> back or proximal lower extremity pain biliary tract disease -> right infrascapular pain myocardial ischemia ->midepigastric, neck, jaw, or upper extremity pain ureteral obstruction -> ipsilateral testicular pain

7
And don’t forget the history
GI Past abdominal surgeries, h/o GB disease, ulcers; FamHx IBD GU Past surgeries, h/o kidney stones, pyelonephritis, UTI Gyn Last menses, sexual activity, contraception, h/o PID or STDs, h/o ovarian cysts, past gynecological surgeries, pregnancies Vascular h/o MI, heart disease, a-fib, anticoagulation, CHF, PVD, Fam Hx of AAA Other medical history DM, organ transplant, HIV/AIDS, cancer Social Tobacco, drugs – Especially cocaine, alcohol Medications NSAIDs, H2 blockers, PPIs, immunosuppression, coumadin

8
Abdominal Exam Inspection Auscultation Percussion Palpate
percussion includes percussion of liver span, light and deep palpation, palpation of liver edge, spleen tip, kidneys, and aorta. The abdominal examination consists of inspection, auscultation, percussion including percussion of liver span, light and deep palpation, palpation of liver edge, spleen tip, kidneys, and aorta. The abdominal exam is done with the patient supine at 90o Order of exam is critical. Auscultate BEFORE palpating!

9
Physical Examination General Appearance and Vitals (sick vs Not sick)
Abdominal exam -Inspection (scars, masses, ecchymosis, distention) -Auscultation (bowel sounds, bruits), -Percussion (organomegaly, dullness) -Palpation (tenderness, guarding, rebound, referred pain, masses) -Don't forget GU, Rectal and Pelvic examination
 -Auscultation (bowel sounds, bruits), -Percussion (organomegaly, dullness) -Palpation (tenderness, guarding, rebound, referred pain, masses) -Don t forget GU, Rectal and Pelvic examination.")
10
Empty bladder Patient comfort (pillows and draping) Arms at side or crossed over chest Ask the patient to point to any painful areas; examine last Warm hands and stethoscope Ticklish or nervous patients: slow movements, distraction, use their hands

11
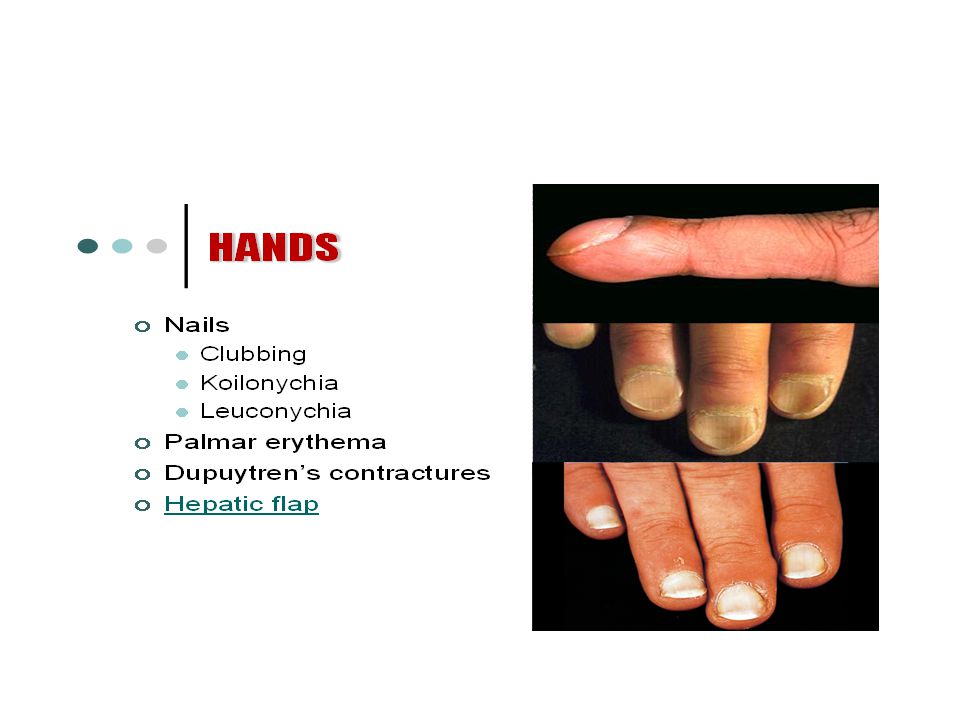
Examine the patients hand
Koilonychia Iron deficiency anemia, Glossitis, dysphagia iron deficiency anemia, and esophageal web (Plummer vinson syndrome) Leukonychia –expansion of the paler half moon at the base of the nail Nail clubbingIBD Palmar erythema Nicotine staining Dupuytren’s contracture--
 Leukonychia –expansion of the paler half moon at the base of the nail. Nail clubbingIBD. Palmar erythema. Nicotine staining. Dupuytren’s contracture--")
13
Flapping tremors (asterixis)
Schamroth’s window test Dupuytren’s contracture Flapping tremors (asterixis)
")
14
Needle track marks(Hepatitis B)
Bruising /peteichae (PT and PTT) Angular stomatitis (Vitamin B12 deficiency) Mouth ulcers glossitis Under the axilla Acanthosis nigricans seen in stomach cancer. Virchows nodes ie sclene node
 Angular stomatitis (Vitamin B12 deficiency) Mouth ulcers glossitis. Under the axilla Acanthosis nigricans seen in stomach cancer. Virchows nodes ie sclene node.")
15
Eye examination Mouth and tongue examination

16
Abdominal Exam Inspection
Contour Flat Scaphoid Distended Symmetry Movement Peristaltic Respirations Aortic pulsation Skin Scars – Striae Discoloration Venous patterns Edema

17
Umbilicus position Hernial orifice

18
Normal-abdomen is Scaphoid. Normal –umbilicus is inverted and and situated centrally between the xiphisternum and pubis symphysis Visible pulsations 1.Aotic pulsations9nervous,anemic and thin persons) 2.Aotic aneurysm(expansile pulsations) 3.Transmitted pulsations 4.Right ventricular pulsation 5.congested liver s.
 2.Aotic aneurysm(expansile pulsations) 3.Transmitted pulsations. 4.Right ventricular pulsation. 5.congested liver s.")
19
Peristalasis- .Normal thin persons, Elderly individuals Children->Congenital Pyloric stenosis Adults- Intestinal obstruction, Carcinoma of the stomach.

20
Hernia sites Ask the patient to stand up and turn his face to one side and cough, if there is an impulse on coughing suggests presence of an. hernia

21
Ascites Prominent veins (caput medusae)
")
22
ABDOMEN: Inspection There should be adequate exposure of the abdomen for proper inspection. The patient should be exposed from the inferior chest to the anterior iliac spines bilaterally. ABDOMEN: Inspection There should be adequate exposure of the abdomen for proper inspection. The patient should be exposed from the inferior chest to the anterior iliac spines bilaterally.

23
ABDOMINAL EXAMINATION AUSCULTATION
Place the diaphragm of the stethoscope to the right of the umbilicus Bowel sounds (borborygmi) are caused by peristaltic movements Occur every 5-10 sec. Absence of b.s.: paralytic ileus or peritonitis Bruits over aorta and renal a. could be a sign of an aneurysm and stenosis
 are caused by peristaltic movements. Occur every 5-10 sec. Absence of b.s.: paralytic ileus or peritonitis. Bruits over aorta and renal a. could be a sign of an aneurysm and stenosis.")
24
Percussion Percussion Percussion: the left and right abdomen should be percussed above and below the umbilicus. Most examiners will percuss 8 or more areas. Note: This percussion is performed as a screening maneuver. Later, the liver Percussion: the left and right abdomen should be percussed above and below the umbilicus. Most examiners will percuss 8 or more areas.

25
ABDOMINAL EXAMINATION FLUID THRILL
Place the palm of your left hand against the left side of the abdomen Flick a finger against the right side of the abdomen Ask the patient to put the edge of a hand on the midline of the abdomen If a ripple is felt upon flicking we call it a fluid thrill = ascites IF IT IS NOT CLEAR

27
Percussion: Liver span
The liver span is estimated by percussion. Remember that it is easier to hear the change from resonance to dullness – so proceed with percussion from areas of resonance to areas of dullness. Upper border: In the midclavicular line start percussing in the chest moving down towards the abdomen about ½ to 1 cm at a time. Note where the percussion notes change from resonate to dull. Lower border: In the midclavicular line begin percussion below the unbillicus and proceed upward until dullness is encounter. 127: Percussion: Liver span The liver span is estimated by percussion. Remember that it is easier to hear the change from resonance to dullness – so proceed with percussion from areas of resonance to areas of dullness. Upper border: In the midclavicular line start percussing in the chest moving down towards the abdomen about ½ to 1 cm at a time. Note where the percussion notes change from resonate to dull. Lower border: In the midclavicular line begin percussion below the unbillicus and proceed upward until dullness is encounter. The distance between the two areas where dullness is first encountered is the liver span. Liver span is normally 6 to 12 cm in the midclavicular line. The distance between the two areas where dullness is first encountered is the liver span. Liver span is normally 6 to 12 cm in the midclavicular line.

28
Liver Span: Scratch Test
Start in the same areas above and below the liver as you would with percussion. Instead of percussing lightly, scratch moving your finger back and forth while listening over the liver. Since sound is conducted better in solids than in air, when the louder sounds are heard you are over the liver. Mark the superior and inferior boarders of the liver span in the midclavicular line Liver Span: May Do Scratch Test If you are unable to determine liver span by percussion then the scratch test may be used. Start in the same areas above and below the liver as you would with percussion. Instead of percussing lightly scratch moving your finger back and forth while listening over the liver. Since sound is conducted better in solids than in air, when the louder sounds are heard you are over the liver. Mark the superior and inferior boarders of the liver span in the midclavicular line

29
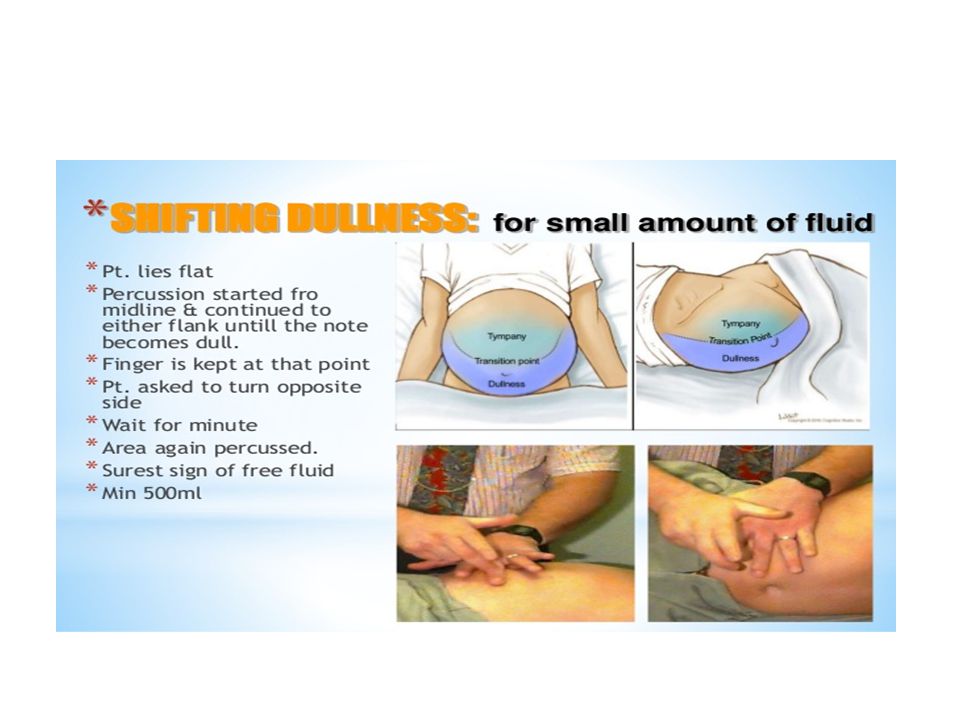
Percuss for shifting dullness 1

30
ABDOMINAL EXAMINATION PALPATION
Tenderness: discomfort and resistance to palpation Involuntary guarding: reflex contraction of the abdominal muscles Rebound tenderness: patient feels pain when the hand is released Tenderness + rigidity: perforated viscus Palpable mass (enlarged organ, faeces, tumour) Aortic pulsation ABNORMAL FINDINGS
 Aortic pulsation. ABNORMAL FINDINGS.")
31
Palpation Palpation of the abdomen should be performed in a systematic way using the 9 named segments of the abdomen: right and left hypochondrium, right and left flank, right and left iliac fossa, the umbilical area, the epigastrium and the suprapubic region. -

32
Abdominal Palpation Palpate lightly in all 4 quadrants. Press down around 1 cm. Remember to look at the patient’s face during palpation to see if any tenderness is elicited Palpation: Lightly, all 4 quadrants Palpate lightly in all 4 quadrants. Press down around 1 cm. Remember to look at the patient’s face during palpation to see if any tenderness is elicited.

33
One should use two hands. Press down around 4 cm
Palpation: Deeply, all 4 quadrants Palpation: Deeply, all 4 quadrants One should use two hands. Press down around 4 cm One should use two hands. Press down around 4 cm

34
Abdominal Physical Exam Palpation - Right Upper Quadrant
Liver: right lobe Gallbladder – Murphy’s sign Stomach: pylorus Duodenum: parts 1-3 Pancreas: head Right suprarenal gland Right kidney Right colic (hepatic) flexure Ascending colon: superior part Transverse colon: right half Liver Lied deep to ribs 7 through 11 and crosses midline to left nipple Sharp inferior border follows right costal margin More inferior when erect Inspire deeply and may palpate Place left hand posteriorly between right 12th rib and iliac crest then place right hand on right upper quadrant - pt takes a deep breath Gallbladder – Murphy’s sign
 flexure. Ascending colon: superior part. Transverse colon: right half. Liver. Lied deep to ribs 7 through 11 and crosses midline to left nipple. Sharp inferior border follows right costal margin. More inferior when erect. Inspire deeply and may palpate. Place left hand posteriorly between right 12th rib and iliac crest then place right hand on right upper quadrant - pt takes a deep breath. Gallbladder – Murphy’s sign.")
35
Palpation: Liver Stand on the pt’s right side. Place your left hand behind the patient’s R side under the 11th and 12th rib area. Press upward with the L hand. Place your R hand on the pt’s abdomen well below where you percussed the liver edge : Palpation: Liver Stand on the pt’s right side. Place your left hand behind the patient’s R side under the 11th and 12th rib area. Press upward with the L hand. Place your R hand on the pt’s abd well below where you percussed the liver edge Ask the patient to take a deep breath and gently push your R hand inward and upward trying to feel the liver edge as it comes down during inspiration. Gradually move your R hand more superior repeating the process until you feel the liver edge or you get to the costal margin.

36
ABDOMINAL EXAMINATION MURPHY’S SIGN
Pain in RUQ Inflammation of gallbladder (cholecystitis) Courvoisier's law Murphy's sign sign of gallbladder disease consisting of pain on taking a deep breath when the examiner's fingers are on the approximate location of the gallbladder. Pain on inspiration during gentle palpation below the right subcostal arch. As the patient breathes in, the liver moves down exposing the gallbladder to pressure from the examiners hand. Murpy’s sign may also be present with hepatitis. The gallbladder (GB) is filled with echogenic sludge (Sl) and a gallstone (red arrow) is impacted in the gallbladder neck. The gallbladder wall (red arrowheads) is markedly thickened indicative of wall edema and there are pericholecystic fluid (blue arrows) pockets surrounding the gallbladder. Courvoisier's law states that in the presence of an enlarged gall bladder which is nontender and accompanied with jaundice, the cause is unlikely to be gallstones.
 Courvoisier s law. Murphy s sign. sign of gallbladder disease consisting of pain on taking a deep breath when the examiner s fingers are on the approximate location of the gallbladder. Pain on inspiration during gentle palpation below the right subcostal arch. As the patient breathes in, the liver moves down exposing the gallbladder to pressure from the examiners hand. Murpy’s sign may also be present with hepatitis. The gallbladder (GB) is filled with echogenic sludge (Sl) and a gallstone (red arrow) is impacted in the gallbladder neck. The gallbladder wall (red arrowheads) is markedly thickened indicative of wall edema and there are pericholecystic fluid (blue arrows) pockets surrounding the gallbladder. Courvoisier s law. states that in the presence of an enlarged gall bladder which is nontender and accompanied with jaundice, the cause is unlikely to be gallstones.")
37
130-131: Palpation of Liver: Alternative Method
It is acceptable during palpation of the liver to use both hands to palpate abdomen. You use the fingers of one hand to palpate and the other hand is used to apply pressure to the dorsum of the other hand. Thus the hand you are using to palpate does not need to be used to apply pressure It is acceptable during palpation of the liver to use both hands to palpate abdomen. You use the fingers of one hand to palpate and the other hand is used to apply pressure to the dorsum of the other hand. Thus the hand you are using to palpate does not need to be used to apply pressure.

38
Abdominal Physical Exam Palpation - Left Upper Quadrant
Liver: left lobe Spleen Stomach Jejunum and proximal ileum Pancreas: body and tail Left Kidney Left Suprarenal gland Left colic (splenic) flexure Transverse colon: left half Descending colon: superior part Spleen Between 9th - 11th ribs Does not extend inferior to the left costal margin
 flexure. Transverse colon: left half. Descending colon: superior part. Spleen. Between 9th - 11th ribs. Does not extend inferior to the left costal margin.")
39
: Palpation: Spleen Palpation: Spleen (correctly - position, breaths, palpating deepest full inspiration, 1 hand under L side, 1 feeling) Palpation: Spleen (if not palpable, R lateral decubitus) : Palpation: Spleen Palpation: Spleen (attempts to do) Palpation: Spleen (correctly - position, breaths, palpating deepest full inspiration, 1 hand under L side, 1 feeling) Palpation: Spleen (if not palpable, R lateral decubitus)
 : Palpation: Spleen. Palpation: Spleen (attempts to do) Palpation: Spleen (correctly - position, breaths, palpating deepest full inspiration, 1 hand under L side, 1 feeling) Palpation: Spleen (if not palpable, R lateral decubitus)")
40
Right lateral decubitus
PALPATION OF SPLEEN Palpation of Spleen: Right lateral decubitus. Right lateral decubitus

41
Palpating for the spleen
Palpate for the liver

42
R L 135-136: Palpation of Kidneys
Palpation:R kidney (take a deep breath, capture kidney, exhale, slowly release kidney) Palpation:L kidney (take a deep breath, capture kidney, exhale, slowly release kidney) L Right kidney (take a deep breath, capture kidney, exhale, slowly release kidney Left kidney (take a deep breath, capture kidney, exhale, slowly release kidney)
 Palpation:L kidney (take a deep breath, capture kidney, exhale, slowly release kidney) L. Right kidney (take a deep breath, capture kidney, exhale, slowly release kidney. Left kidney (take a deep breath, capture kidney, exhale, slowly release kidney)")
43
Abdominal Physical Exam Palpation - Right Lower Quadrant
Cecum Vermiform appendix McBurney’s Point Rovsing’s sign Psoas sign Obturator sign Most of ileum Ascending colon: inferior part Right ovary Right uterine tube Right spermatic cord Uterus (if enlarged) Urinary bladder (if full) 43
 Urinary bladder (if full) 43.")
44
Appendicitis: Psoas Sign

45
Abdominal Physical Exam Palpation - Left Lower Quadrant
Sigmoid colon Descending colon: inferior part Left ovary Left uterine tube Left ureter: abdominal part Left spermatic cord: abdominal part Uterus (if enlarged) Urinary bladder (if full) 45
 Urinary bladder (if full) 45.")
46
137: Palpation: For abdominal aorta
Palpation: For abdominal aorta (to feel both the left and right walls of the aorta) In correct order: Inspection, auscultation, percussion and palpation Abdominal Examination was done at 0. 137: Palpation: For abdominal aorta Palpation: For abdominal aorta (to feel both the left and right walls of the aorta) In correct order: Inspection, auscultation, percussion and palpation Abdominal Examination was done at 0.
 In correct order: Inspection, auscultation, percussion and palpation. Abdominal Examination was done at 0. 137: Palpation: For abdominal aorta. Palpation: For abdominal aorta (to feel both the left and right walls of the aorta) In correct order: Inspection, auscultation, percussion and palpation. Abdominal Examination was done at 0.")
47
What kind of tests should you order?
Depends what you are looking for! Abdominal series 3 views: upright chest, flat view of abdomen, upright view of abdomen Limited utility: restrict use to patients with suspected obstruction or free air Ultrasound Good for diagnosing AAA but not ruptured AAA Good for pelvic pathology CT abdomen/pelvis Noncontrast for free air, renal colic, ruptured AAA, (bowel obstruction) Contrast study for abscess, infection, inflammation, unknown cause MRI Most often used when unable to obtain CT due to contrast issue Labs CBC: “What’s the white count?” Chemistries Liver function tests, Lipase Coagulation studies Urinalysis, urine culture GC/Chlamydia swabs LDH
 Contrast study for abscess, infection, inflammation, unknown cause. MRI. Most often used when unable to obtain CT due to contrast issue. Labs. CBC: What’s the white count Chemistries. Liver function tests, Lipase. Coagulation studies. Urinalysis, urine culture. GC/Chlamydia swabs. LDH.")
48
Radiology: Plain Films
Advantages: Quick, easy, non-invasive, less radiation, lower cost, can be done at bedside and can help make decisions in certain disease states. Disadvantages: Only useful in certain conditions – otherwise low yield, difficult to position sick patients.

49
Radiology: Plain Films
When are they useful? Obstruction/Ileus Volvulus (cecal and sigmoid) Free air Radiopaque foreign bodies Constipation?
 Free air Radiopaque foreign bodies Constipation")
50
Plain Films: Small bowel obstruction

51
Cecal Volvulus and Sigmoid Volvulus

52
Radiology: Ultrasound
Advantages: Can be done at bedside, easy to learn, repeatable, no radiation, cheap, can be used in pregnancy, patient does not need to leave the department Disadvantages: Highly dependent on user’s skill level. Limited by body habitus and bowel gas

53
Radiology: Ultrasound
What conditions is it most useful for? Gallbladder disease AAA Hydronephrosis Obstetrics and gynecological (Ectopic pregnancy, Ovarian pathology) Appendicitis (particularly in children)
 Appendicitis (particularly in children)")
54
Ultrasound: Cholecystitis
Normal GB GB stone

55
Ultrasound: Appendicitis
Normal appendix Inflammed appendix

56
Cases… A 23 year old female presents with severe, intermittent right lower quadrant pain associated with nausea and vomiting. She has no medical history. Her vital signs reveal tachycardia but are otherwise normal. Physical exam shows a soft abdomen, RLQ TTP without peritoneal signs. Pelvic (which is part of the physical exam), shows scant discharge. If you could only order one test, what would it be? What is on your differential?
, shows scant discharge. If you could only order one test, what would it be What is on your differential")
57
Differential diagnosis
Ectopic Pregnancy Ruptured Ovarian Cyst Appendicitis Right-sided diverticulitis Ovarian Torsion Nephrolithiasis Pyelonephritis Endometriosis UTI Heterotopic pregnancy Terminal ileitis

58
Case #1 24 yo healthy M with one day hx of abdominal pain. Pain was generalized at first, now worse in right lower abd & radiates to his right groin. He has vomited twice today. Denies any diarrhea, fevers, dysuria or other complaints. No appetite today. ROS otherwise negative. PMHx: negative PSurgHx: negative Meds: none NKDA Social hx: no alcohol, tobacco or drug use Family hx: non-contributory Basic cases to go through the most common abd pain complaints we see in the ED

59
Abdominal pain What else do you want to know?
What is on your differential diagnosis so far? (healthy male with RLQ abd pain….) How do you approach the complaint of abdominal pain in general? Let’s review in this lecture: Types of pain History and physical examination Labs and imaging Abdominal pain in special populations (Elderly, HIV) Clinical pearls to help you in the ED
 How do you approach the complaint of abdominal pain in general Let’s review in this lecture: Types of pain. History and physical examination. Labs and imaging. Abdominal pain in special populations (Elderly, HIV) Clinical pearls to help you in the ED.")
60
What kind of pain is it? Visceral Parietal Referred
Involves hollow or solid organs; midline pain due to bilateral innvervation Steady ache or vague discomfort to excruciating or colicky pain Poorly localized Epigastric region: stomach, duodenum, biliary tract Periumbilical: small bowel, appendix, cecum Suprapubic: colon, sigmoid, GU tract Parietal Involves parietal peritoneum Localized pain Causes tenderness and guarding which progress to rigidity and rebound as peritonitis develops Referred Produces symptoms not signs Based on developmental embryology Ureteral obstruction → testicular pain Subdiaphragmatic irritation → ipsilateral shoulder or supraclavicular pain Gynecologic pathology → back or proximal lower extremity Biliary disease → right infrascapular pain MI → epigastric, neck, jaw or upper extremity pain

61
Moving on to the Physical Exam
General Vital Signs Abdomen Look for distention, scars, masses Auscultate – hyperactive or obstructive BS increase likelihood of SBO fivefold – otherwise not very helpful Percuss for tympany Palpate for tenderness, masses, aortic aneurysm, organomegaly, rebound, guarding, rigidity Look for hernias! rectal exam Pelvic exam Vaginal discharge – Culture Adenexal mass or fullness Cardiac Lungs Orthostatic VS are less reliable in the diabetic, elderly, those on beta-blocker. Pulse increase of 30 or presyncope on standing are highly sensitive for loss of 1 L of blood or 3L of fluid. BP changes are less reliable. Patient must be standing at least one minute before measurements are taken.

62
Abdominal Findings Guarding Rebound
Voluntary Contraction of abdominal musculature in anticipation of palpation Diminish by having patient flex knees Involuntary Reflex spasm of abdominal muscles aka: rigidity Suggests peritoneal irritation Rebound Present in 1 of 4 patients without peritonitis Pain referred to the point of maximum tenderness when palpating an adjacent quadrant is suggestive of peritonitis Rovsing’s sign in appendicitis Rectal exam Little evidence that tenderness adds any useful information beyond abdominal examination Gross blood or melena indicates a GIB Heme positive stool – 10% of people over the age of 50 sent home with diagnosis of NSAP and heme positive stools were found to have cancer within a year. Heme positive stool in the setting of suspected PUD should elicit more urgent referral for further evaluation

63
Differential Diagnosis
Use history and physical exam to narrow it down Rule out life-threatening pathology

64
Back to Case #1….24 yo with RLQ pain
Physical exam: T: 37.8, HR: 95, BP 118/76, R: 18, O2 sat: 100% room air Uncomfortable appearing, slightly pale Abdomen: soft, non-distended, tender to palpation in RLQ with mild guarding; hypoactive bowel sounds Genital exam: normal What is your differential diagnosis and what do you do next?

65
Appendicitis Classic presentation
Periumbilical pain Anorexia, nausea, vomiting Pain localizes to RLQ Occurs only in ½ to 2/3 of patients 26% of appendices are retrocecal and cause pain in the flank; 4% are in the RUQ A pelvic appendix can cause suprapubic pain, dysuria Males may have pain in the testicles Findings Depends on duration of symptoms Rebound, voluntary guarding, rigidity, tenderness on rectal exam Psoas sign Obturator sign Fever (a late finding) Urinalysis abnormal in 19-40% CBC is not sensitive or specific Abdominal xrays Appendiceal fecalith or gas, localized ileus, blurred right psoas muscle, free air CT scan Pericecal inflammation, abscess, periappendiceal phlegmon, fluid collection, localized fat stranding
 Urinalysis abnormal in 19-40% CBC is not sensitive or specific. Abdominal xrays. Appendiceal fecalith or gas, localized ileus, blurred right psoas muscle, free air. CT scan. Pericecal inflammation, abscess, periappendiceal phlegmon, fluid collection, localized fat stranding.")
66
Appendicitis: Psoas Sign

67
Appendicitis: Obturator Sign
Passively flex right hip and knee then internally rotate the hip

68
Appendicitis Diagnosis Treatment WBC
Clinical appendicitis – call your surgeon Maybe appendicitis - CT scan Not likely appendicitis – observe for 6-12 hours or re-examination in 12 hours Treatment NPO IVFs Preoperative antibiotics – decrease the incidence of postoperative wound infections Cover anaerobes, gram-negative and enterococci Zosyn grams IV or Unasyn 3 grams IV Analgesia

69
Case #2 68 yo F with 2 days of LLQ abd pain, diarrhea, fevers/chills, nausea; vomited once at home. PMHx: HTN, diverticulosis PSurgHx: negative Meds: HCTZ NKDA Social hx: no alcohol, tobacco or drug use Family hx: non-contributory69

70
Case #2 Exam T: 37.6, HR: 100, BP: 145/90, R: 19, O2sat: 99% room air
Gen: uncomfortable appearing, slightly pale CV/Pulmonary: normal heart and lung exam, no LE edema, normal pulses Abd: soft, moderately TTP LLQ Rectal: normal tone, guaiac test –ve,(Fecal occult blood test) What is your differential diagnosis & what next?
 What is your differential diagnosis & what next")
71
Diverticulitis Risk factors Clinical features Physical Exam
Diverticula Increasing age Clinical features Steady, deep discomfort in LLQ Change in bowel habits Urinary symptoms Tenesmus Paralytic ileus SBO Physical Exam Low-grade fever Localized tenderness Rebound and guarding Left-sided pain on rectal exam Occult blood Peritoneal signs Suggest perforation or abscess rupture

72
Diverticulitis Diagnosis Treatment CT scan (IV and oral contrast)
Pericolic fat stranding Diverticula Thickened bowel wall Peridiverticular abscess Leukocytosis present in only 36% of patients Treatment Fluids Correct electrolyte abnormalities NPO Abx: gentamicin AND metronidazole OR clindamycin OR levaquin/flagyl For outpatients (non-toxic) liquid diet x 48 hours cipro and flagyl
 liquid diet x 48 hours. cipro and flagyl.")
73
Case #3 46 yo M with hx of alcohol abuse with 3 days of severe upper abd pain, vomiting, subjective fevers. Med Hx: negative Surg Hx: negative Meds: none; Allergies: NKDA Social hx: homeless, heavy alcohol use, smokes 2ppd, no drug use

74
Case #3 Exam Vital signs: T: 37.4, HR: 115, BP: 98/65, R: 22, O2sat: 95% room air General: ill-appearing, appears in pain CV: tachycardic, normal heart sounds, pulses normal Lungs: clear Abdomen: mildly distended, moderately TTP epigastric, +voluntary guarding Rectal: heme neg stool What is your differential diagnosis & what next?

75
Pancreatitis Risk Factors Clinical Features Physical Findings Alcohol
Gallstones Drugs Amiodarone, antivirals, diuretics, NSAIDs, antibiotics, more….. Severe hyperlipidemia Idiopathic Clinical Features Epigastric pain Constant, boring pain Radiates to back Severe N/V bloating Physical Findings Low-grade fevers Tachycardia, hypotension Respiratory symptoms Atelectasis Pleural effusion Peritonitis – a late finding Ileus Cullen sign* Bluish discoloration around the umbilicus Grey Turner sign* Bluish discoloration of the flanks *Signs of hemorrhagic pancreatitis

76
Pancreatitis Treatment Diagnosis NPO IV fluid resuscitation
Maintain urine output of 100 mL/hr NGT if severe, persistent nausea No antibiotics unless severe disease E coli, Klebsiella, enterococci, staphylococci, pseudomonas Imipenem or cipro with metronidazole Mild disease, tolerating oral fluids Discharge on liquid diet Follow up in hours All others, admit Diagnosis Lipase Elevated more than 2 times normal Sensitivity and specificity >90% Amylase Nonspecific Don’t bother… RUQ US if etiology unknown CT scan Insensitive in early or mild disease NOT necessary to diagnose pancreatitis Useful to evaluate for complications

77
Case #4 72 yo M with hx of CAD on aspirin and Plavix with several days of dull upper abd pain and now with worsening pain “in entire abdomen” today. Some relief with food until today, now worse after eating lunch. Med Hx: CAD, HTN, CHF Surg Hx: appendectomy Meds: Aspirin, Plavix, Metoprolol, Lasix Social hx: smokes 1ppd, denies alcohol or drug use, lives alone

78
Case #4 Exam T: 99.1, HR: 70, BP: 90/45, R: 22, O2sat: 96% room air
General: elderly, thin male, ill-appearing CV: normal Lungs: clear Abd: mildly distended and diffusely tender to palpation, +rebound and guarding Rectal: blood-streaked heme + brown stool What is your differential diagnosis & what next?

79
Peptic Ulcer Disease Physical Findings Epigastric tenderness
Risk Factors H. pylori NSAIDs Smoking Hereditary Clinical Features Burning epigastric pain Sharp, dull, achy, or “empty” or “hungry” feeling Relieved by milk, food, or antacids Awakens the patient at night Nausea, retrosternal pain and belching are NOT related to PUD Atypical presentations in the elderly Physical Findings Epigastric tenderness Severe, generalized pain may indicate perforation with peritonitis Occult or gross blood per rectum or NGT if bleeding

80
Peptic Ulcer Disease Diagnosis Treatment Empiric treatment
Rectal exam for occult blood CBC Anemia from chronic blood loss LFTs Evaluate for GB, liver and pancreatic disease Definitive diagnosis is by EGD or upper GI barium study Treatment Empiric treatment Avoid tobacco, NSAIDs, aspirin PPI or H2 blocker Immediate referral to GI if: >45 years Weight loss Long h/o symptoms Anemia Persistent anorexia or vomiting Early satiety GIB

81
Perforated Peptic Ulcer
Abrupt onset of severe epigastric pain followed by peritonitis IV, oxygen, monitor CBC, T&C, Lipase Acute abdominal x-ray series Lack of free air does NOT rule out perforation Broad-spectrum antibiotics Surgical consultation

82
Case #5 35 yo healthy F to ED c/o nausea and vomiting since yesterday along with generalized abdominal pain. No fevers/chills, +anorexia. Last stool 2 days ago. Med Hx: negative Surg Hx: s/p hysterectomy (for fibroids) Meds: none, Allergies: NKDA Social Hx: denies alcohol, tobacco or drug use Family Hx: non-contributory
 Meds: none, Allergies: NKDA. Social Hx: denies alcohol, tobacco or drug use. Family Hx: non-contributory.")
83
Case #5 Exam T: 36.9, HR: 100, BP: 130/85, R: 22, O2 sat: 97% room air
General: mildly obese female, vomiting CV: normal Lungs: clear Abd: moderately distended, mild TTP diffusely, hypoactive bowel sounds, no rebound or guarding What is your differential and what next?

84
Upright abd x-ray

85
Bowel Obstruction Physical Findings Mechanical or nonmechanical causes
#1 - Adhesions from previous surgery #2 - Groin hernia incarceration Clinical Features Crampy, intermittent pain Periumbilical or diffuse Inability to have BM or flatus N/V Abdominal bloating Sensation of fullness, anorexia Physical Findings Distention Tympany Absent, high pitched or tinkling bowel sound or “rushes” Abdominal tenderness: diffuse, localized, or minimal

86
Bowel Obstruction Diagnosis CBC and electrolytes
electrolyte abnormalities WBC >20,000 suggests bowel necrosis, abscess or peritonitis Abdominal x-ray series Flat, upright, and chest x-ray Air-fluid levels, dilated loops of bowel Lack of gas in distal bowel and rectum CT scan Identify cause of obstruction Delineate partial from complete obstruction Treatment Fluid resuscitation NGT Analgesia Surgical consult Hospital observation for ileus OR for complete obstruction Peri-operative antibiotics Zosyn or unasyn

87
Case #6 48 yo obese F with one day hx of upper abd pain after eating, does not radiate, is intermittent cramping pain, +N/V, no diarrhea, subjective fevers. No prior similar symptoms. Med hx: denies Surg hx: denies No meds or allergies Social hx: no alcohol, tobacco or drug use

88
Case #6 Exam T: 100.4, HR: 96, BP: 135/76, R: 18, O2 sat: 100% room air General: moderately obese, no acute distress CV: normal Lungs: clear Abd: moderately TTP RUQ, +Murphy’s sign, non-distended, normal bowel sounds What is your differential and what next?

89
Cholecystitis Clinical Features Physical Findings
RUQ or epigastric pain Radiation to the back or shoulders Dull and achy → sharp and localized Pain lasting longer than 6 hours N/V/anorexia Fever, chills Physical Findings Epigastric or RUQ pain Murphy’s sign Patient appears ill Peritoneal signs suggest perforation

90
Cholecystitis Diagnosis Treatment CBC, LFTs, Lipase RUQ US HIDA scan
Elevated alkaline phosphatase Elevated lipase suggests gallstone pancreatitis RUQ US Thicken gallbladder wall Pericholecystic fluid Gallstones or sludge Sonographic murphy sign HIDA scan more sensitive & specific than US H&P and laboratory findings have a poor predictive value – if you suspect it, get the US Treatment Surgical consult IV fluids Correct electrolyte abnormalities Analgesia Antibiotics Ceftriaxone 1 gram IV If septic, broaden coverage to zosyn, unasyn, imipenem or add anaerobic coverage to ceftriaxone NGT if intractable vomiting

91
Case #7 34 yo healthy M with 4 hour hx of sudden onset left flank pain, +nausea/vomiting; no prior hx of similar symptoms; no fevers/chills. +difficulty urinating, no hematuria. Feels like has to urinate but cannot. PMHx: neg Surg Hx: neg Meds: none, Allergies: NKDA Social hx: occasional alcohol, denies tobacco or drug use Family hx: non-contributory

92
Case #7 Exam T: 98.9, HR: 110, BP: 150/90, R: 20, O2 sat: 99% room air
General: writhing around on stretcher in pain, +diaphoretic CV: tachycardic, heart sounds normal Lungs: clear Abd: soft; non-tender Back: mild left CVA tenderness Genital exam: normal Neuro exam: normal What is your differential diagnosis and what next?

93
Renal Colic Clinical Features Physical Findings
Acute onset of severe, dull, achy visceral pain Flank pain Radiates to abdomen or groin including testicles N/V and sometimes diaphoresis Fever is unusual Waxing and waning symptoms Physical Findings non tender or mild tenderness to palpation Anxious, pacing, writhing in bed – unable to sit still

94
Renal Colic Diagnosis Treatment Urinalysis CBC BUN/Creatinine CT scan
RBCs WBCs suggest infection or other etiology for pain (ie appendicitis) CBC If infection suspected BUN/Creatinine In older patients If patient has single kidney If severe obstruction is suspected CT scan In older patients or patients with comorbidities (DM, SCD) Not necessary in young patients or patients with h/o stones that pass spontaneously Treatment IV fluid boluses Analgesia Narcotics NSAIDS If no renal insufficiency Strain all urine Follow up with urology in 1-2 weeks If stone > 5mm, consider admission and urology consult If toxic appearing or infection found IV antibiotics Urologic consult
 CBC. If infection suspected. BUN/Creatinine. In older patients. If patient has single kidney. If severe obstruction is suspected. CT scan. In older patients or patients with comorbidities (DM, SCD) Not necessary in young patients or patients with h/o stones that pass spontaneously. Treatment. IV fluid boluses. Analgesia. Narcotics. NSAIDS. If no renal insufficiency. Strain all urine. Follow up with urology in 1-2 weeks. If stone > 5mm, consider admission and urology consult. If toxic appearing or infection found. IV antibiotics. Urologic consult.")
95
Just a few more to go….hang in there
Ovarian torsion Testicular torsion GI bleeding Abd pain in the Elderly

96
Abdominal Pain in the Elderly
Mortality rate for abdominal pain in the elderly is 11-14% Perception of pain is altered Altered reporting of pain: stoicism, fear, communication problems Most common causes: Cholecystitis Appendicitis Bowel obstruction Diverticulitis Perforated peptic ulcer Don’t miss these: AAA, ruptured AAA Mesenteric ischemia Myocardial ischemia Aortic dissection

97
Abdominal Pain in the Elderly
Appendicitis – do not exclude it because of prolonged symptoms. Only 20% will have fever, N/V, RLQ pain and ↑WBC Acute cholecystitis – most common surgical emergency in the elderly. Perforated peptic ulcer – only 50% report a sudden onset of pain. In one series, missed diagnosis of PPU was leading cause of death. Mesenteric ischemia – we make the diagnosis only 25% of the time. Early diagnosis improves chances of survival. Overall survival is 30%. Increased frequency of abdominal aortic aneurysms AAA may look like renal colic in elderly patients

98
Mesenteric Ischemia Consider this diagnosis in all elderly patients with risk factors Atrial fibrillation, recent MI Atherosclerosis, CHF, digoxin therapy Hypercoagulability, prior DVT, liver disease Severe pain, often refractory to analgesics Relatively normal abdominal exam Embolic source: sudden onset (more gradual if thrombosis) Nausea, vomiting and anorexia are common 50% will have diarrhea Eventually stools will be guiaic-positive Metabolic acidosis and extreme leukocytosis when advanced disease is present (bowel necrosis) Diagnosis requires mesenteric angiography or CT angiography
 Nausea, vomiting and anorexia are common. 50% will have diarrhea. Eventually stools will be guiaic-positive. Metabolic acidosis and extreme leukocytosis when advanced disease is present (bowel necrosis) Diagnosis requires mesenteric angiography or CT angiography.")
99
Abdominal Aortic Aneurysm
Risk increases with age, women >70, men >55 Abdominal pain in 70-80% (not back pain!) Back pain in 50% Sudden onset of significant pain Atypical locations of pain: hips, inguinal area, external genitalia Syncope can occur Hypotension may be present Palpation of a tender, enlarged aorta on exam is an important finding May present with hematuria Suspect it in any older patient with back, flank or abdominal pain especially with a renal colic presentation Ultrasound can reveal the presence of a AAA but is not helpful for rupture. CT abd/pelvis without contrast for stable patients. High suspicion in an unstable patient requires surgical consult and emergent surgery.
 Back pain in 50% Sudden onset of significant pain. Atypical locations of pain: hips, inguinal area, external genitalia. Syncope can occur. Hypotension may be present. Palpation of a tender, enlarged aorta on exam is an important finding. May present with hematuria. Suspect it in any older patient with back, flank or abdominal pain especially with a renal colic presentation. Ultrasound can reveal the presence of a AAA but is not helpful for rupture. CT abd/pelvis without contrast for stable patients. High suspicion in an unstable patient requires surgical consult and emergent surgery.")
100
GI Bleeding Upper Lower Proximal to Ligament of Treitz
Peptic ulcer disease most common Erosive gastritis Esophagitis Esophageal and gastric varices Mallory-Weiss tear Lower Hemorrhoids most common Diverticulosis Angiodysplasia First: r/o upper GI bleed Lower GI bleed: most common hemorrhoids Diverticulosis has potential for massive bleeding

101
Medical History Common Presentation: High level of suspicion with
Hematemesis (source proximal to right colon) Coffee-ground emesis Melena Hematochezia (distal colorectal source) High level of suspicion with Hypotension Tachycardia Angina Syncope Weakness Confusion Cardiac arrest
 Coffee-ground emesis. Melena. Hematochezia (distal colorectal source) High level of suspicion with. Hypotension. Tachycardia. Angina. Syncope. Weakness. Confusion. Cardiac arrest.")
Similar presentations









 The McGraw-Hill Companies, Inc. Permission required for reproduction or display. 23-1 Chapter 23 Abdominal and Gastrointestinal Disorders.>")









