Download presentation
Presentation is loading. Please wait.

1
Routine Anomaly Scan Ilse Erasmus

2
Routine Anomaly Scan Timing: 18 – 23 weeks Costs about R 230 – 00

3
RCOG Guidelines October 1997 Timing of sonars
Best Acceptable Less Accept Dating 8-10 10-20 24 Viability >7 Twins Anytime Chorionicity 8-12 13-15 Fetal anomaly 18-20 NT 8-15* 15-16* 18-20*

4
Routine Anomaly Scan Waste of resource to request routine anomaly scan in the late second or 3rd trimester Waste of resource to request growth scan in 3rd trimester in the absence of an early sonar

5
Routine Anomaly Scan Indication in SA cost considerations???
Routine late bookers High risk Previous fetal/ neonatal anomalies Previous IUD AMA Maternal: disease index pregnancy / history of Medication Congenital anomalies

6
Routine Anomaly Scan Cochrane Database Radius?!?
Reduction in post term inductions Twin Pregnancies Radius?!?

7
Routine Anomaly Scan Screening? 1/55 babies born with major anomaly
Structural anomalies > single gene defects UK Fetal anomalies = 15% of perinatal deaths and 15% of deaths in first year of life

8
Routine Anomaly Scan Screening? Six objectives
Reassurance that baby is apparently normal Or the identification of: Non –viable anomalies Anomalies associated with high morbidity and long term handicap Fetal conditions with the potential for intrauterine therapy Fetal conditions requiring postnatal investigation and/ or therapy Parental preparation

9
Routine Anomaly Scan Screening?
Lethal anomalies – anencheph, BRA, thanatophoric dwarfs High morbidity and long term handicap – NTD, cardiac,aneuploidy Potential intrauterine therapy – RH, Parvo,TTS Fetal conditions requiring postnatal investigation and/ or therapy – renal, facial cleft Parental preparation

10
RCOG Guidelines October 1997 Detection Rates for Specific anomalies
Anomaly <24w Sensitivity Specificity Anencheph/Enc 87 – 100% (>95%) 99 – 100% Intracranial Path 27 – 100% (70%) Renal Agenesis % (85%) Cystic Lung 0- 100% (100%) Cardiac Major 4 – 77% (47%) 98 – 99% CD hernia 0 – 100% (40%) Exomphalos 0 – 100% (>95%) Gastroschisis 0 –100% (66%) % Muscuoloskeletal 0 –100% (50%)
 99 – 100% Intracranial Path. 27 – 100% (70%) Renal Agenesis % (85%) Cystic Lung % (100%) Cardiac Major. 4 – 77% (47%) 98 – 99% CD hernia. 0 – 100% (40%) Exomphalos. 0 – 100% (>95%) Gastroschisis. 0 –100% (66%) % Muscuoloskeletal. 0 –100% (50%)")
11
RCOG Guidelines October 1997 Detection Rates for Specific anomalies
Anomaly < 24 Sensitivity Specificity Spina Bifida 69 – 100% (78%) 99 – 100% Major Renal 26 – 100% (60%)
 99 – 100% Major Renal. 26 – 100% (60%)")
12
RCOG Routine sonar in Pregnancy July 2000
6 year Scottish Study Booking scan only % Minimum standard scan % Anencheph 97 100 ( better) Spina Bifida 61 92 (better) Major cardiac (hypoplastic LV) 14 61 (better) CD Hernia 30 62 (better) Gastroshcisis 86 100 (better) Exomphalos 45 92 (same) Major renal Renal agenesis 76 85 (better)
 Spina Bifida (better) Major cardiac. (hypoplastic LV) (better) CD Hernia (better) Gastroshcisis (better) Exomphalos (same) Major renal. Renal agenesis (better)")
13
RCOG 2000 July Minimum standard for a 20 week anomaly scan
Gestational age BPD, HC, FL, AC

14
Measurments

15
RCOG 2000 July Minimum standard for a 20 week anomaly scan
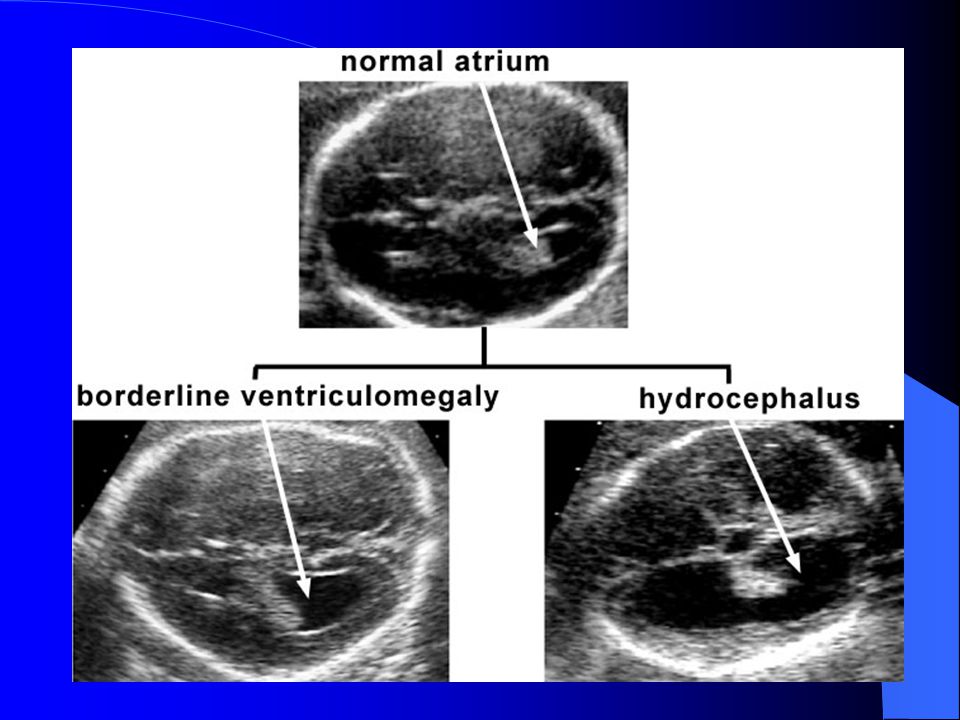
Gestational age BPD, HC, FL, AC Fetal Normality Head shape and internal structures CSP, Cerebellum, Ventricular size at atrium (<10mm) Spine longitudinal and transverse Abdominal shape and content at the level of the stomach
 Spine longitudinal and transverse. Abdominal shape and content at the level of the stomach.")
16
RCOG 2000 July Minimum standard for a 20 week anomaly scan
Renal Pelvis (<5mm AP) Longitudinal axis – abdominal thoracic appearance (diaphragm/bladder) Thorax at level of 4ch cardiac view Arms – 2 x 3 long bones + hands (not counting fingers) Legs - 2 x 3 long bones + feet (not counting toes)
 Longitudinal axis – abdominal thoracic appearance (diaphragm/bladder) Thorax at level of 4ch cardiac view. Arms – 2 x 3 long bones + hands (not counting fingers) Legs - 2 x 3 long bones + feet (not counting toes)")
17
RCOG 2000 July Minimum standard for a 20 week anomaly scan

18
RCOG 2000 July Optimal standard for a 20 week anomaly scan
The above plus: Cardiac outflow tracts Face and lips

19
RCOG 2000 July Marker scans Not considered “routine”
Isolated markers of dubious value Increased overall detection rate increase from 51% - 55% but FPR from 1/2332 to 1/188!!!!! (Boyd PA Lancet 1998) Two or more markers significant Screening using maternal age, age + NT, age+ serum will identify 50 – 80% So marker scan as screening in unscreened population unlikely to be of use
 Two or more markers significant. Screening using maternal age, age + NT, age+ serum will identify 50 – 80% So marker scan as screening in unscreened population unlikely to be of use.")
20
RCOG 2000 July Marker scans “Markers” CPC
Ventriculomegaly(>10mm at atrium) Echogenic bowel(equivalent to bone density) Head shape Nuchal skinfold thickness(>5mm at 20 weeks) CM Cleft lip Echogenic intracardiac focus
 Echogenic bowel(equivalent to bone density) Head shape. Nuchal skinfold thickness(>5mm at 20 weeks) CM. Cleft lip. Echogenic intracardiac focus.")
21
RCOG 2000 July Marker scans Dilated renal pelvis(>5mmAP)
Short Femur/Humerus Talipes Sandal gap Clinodactyly Clenched hand Two vessel cord

22
RCOG 2000 July Marker scans Other risk factors Maternal age > 35
Serum screening results Nuchal translucency at 11 – 14 weeks

23
Standard views Pilu, Nicolaides CD - ROM ISUOG Standards

24
Standard views Intrauterine Amount of fetuses Cardiac activity
Placental Position, Appearance Cord vessels Liquor

25
Standard views Head and Brain

26
Standard views Face

27
Standard views Face

28
Standard views Spine

29
Standard views Heart

30
Standard views GIT

31
Standard views Limbs

32
Anomaly scan Skull & Brain Normal and abnormal

38
Anomaly scan Face Normal and abnormal

42
Anomaly scan Spine Normal and abnormal

43
Normal Spine

44
Abnormal Spine

45
Anomaly scan GIT Normal and abnormal

48
Anomaly scan Heart Normal and abnormal

52
Anomaly scan Kidneys Normal and abnormal

54
Anomaly scan Limbs Normal and abnormal

Similar presentations






























 Maternal Newborn Nursing Care. Forth Edition. Addison Wesley.>")


