Download presentation
Presentation is loading. Please wait.

1
THE EXTERNAL PUMP IN PRACTICE Predrag B. Djordjevic Academy, US Medical School, Belgrade, Serbia 10 th Meeting of the MGSD 26-29 April, 2007 Istanbul, Turkey

2
In 1993, the Diabetes Control and Complications Trial (DCCT) definitively showed that, in people with type 1 diabetes, a good metabolic control, meaning long-term glucose values as close to normal as possible, (mean HbA1c - 7.2 % in the intensive treatment group, compared to conventional treatment, with a mean HbA1c - 9.0 %) is associated with a significant reduction in the risk for retinopathy (76 %), nephropathy (50%) and neuropathy (60%).In 1993, the Diabetes Control and Complications Trial (DCCT) definitively showed that, in people with type 1 diabetes, a good metabolic control, meaning long-term glucose values as close to normal as possible, (mean HbA1c - 7.2 % in the intensive treatment group, compared to conventional treatment, with a mean HbA1c - 9.0 %) is associated with a significant reduction in the risk for retinopathy (76 %), nephropathy (50%) and neuropathy (60%).
 definitively showed that, in people with type 1 diabetes, a good metabolic control, meaning long-term glucose values as close to normal as possible, (mean HbA1c % in the intensive treatment group, compared to conventional treatment, with a mean HbA1c %) is associated with a significant reduction in the risk for retinopathy (76 %), nephropathy (50%) and neuropathy (60%).In 1993, the Diabetes Control and Complications Trial (DCCT) definitively showed that, in people with type 1 diabetes, a good metabolic control, meaning long-term glucose values as close to normal as possible, (mean HbA1c % in the intensive treatment group, compared to conventional treatment, with a mean HbA1c %) is associated with a significant reduction in the risk for retinopathy (76 %), nephropathy (50%) and neuropathy (60%).")
3
Further on, the DCCT / EDIC study (Epidemiology of Diabetes Interventions and Complications) has demonstrated the sustained benefits of good metabolic control through intensive insulin therapy: the former intensive treatment group continues to exhibit the same reduction in the risks of diabetic retinopathy (75 %), nephropathy (75 %) and neuropathy, starting from a new baseline status at the beginning of EDIC.Further on, the DCCT / EDIC study (Epidemiology of Diabetes Interventions and Complications) has demonstrated the sustained benefits of good metabolic control through intensive insulin therapy: the former intensive treatment group continues to exhibit the same reduction in the risks of diabetic retinopathy (75 %), nephropathy (75 %) and neuropathy, starting from a new baseline status at the beginning of EDIC.
 has demonstrated the sustained benefits of good metabolic control through intensive insulin therapy: the former intensive treatment group continues to exhibit the same reduction in the risks of diabetic retinopathy (75 %), nephropathy (75 %) and neuropathy, starting from a new baseline status at the beginning of EDIC.Further on, the DCCT / EDIC study (Epidemiology of Diabetes Interventions and Complications) has demonstrated the sustained benefits of good metabolic control through intensive insulin therapy: the former intensive treatment group continues to exhibit the same reduction in the risks of diabetic retinopathy (75 %), nephropathy (75 %) and neuropathy, starting from a new baseline status at the beginning of EDIC.")
4
Also cardiovascular events have been reduced by 42 % and the major cardiovascular events (non-fatal MI, stroke, death), by 57 %.Also cardiovascular events have been reduced by 42 % and the major cardiovascular events (non-fatal MI, stroke, death), by 57 %.
, by 57 %.Also cardiovascular events have been reduced by 42 % and the major cardiovascular events (non-fatal MI, stroke, death), by 57 %.")
5
The EDIC study has demonstrated the concept and the importance of the “metabolic memory” in preventing the later course of complications.The EDIC study has demonstrated the concept and the importance of the “metabolic memory” in preventing the later course of complications.

6
The release of DCCT and UKPDS has definitively demonstrated the importance to optimize glycemic control, either through multiple daily injection or continuous subcutaneous insulin infusion (CSII or insulin pump therapy) and also has renewed interest in the role of CSII therapy in improving metabolic outcomes, because it offers a more precise physiological method of insulin administration.The release of DCCT and UKPDS has definitively demonstrated the importance to optimize glycemic control, either through multiple daily injection or continuous subcutaneous insulin infusion (CSII or insulin pump therapy) and also has renewed interest in the role of CSII therapy in improving metabolic outcomes, because it offers a more precise physiological method of insulin administration.
 and also has renewed interest in the role of CSII therapy in improving metabolic outcomes, because it offers a more precise physiological method of insulin administration.The release of DCCT and UKPDS has definitively demonstrated the importance to optimize glycemic control, either through multiple daily injection or continuous subcutaneous insulin infusion (CSII or insulin pump therapy) and also has renewed interest in the role of CSII therapy in improving metabolic outcomes, because it offers a more precise physiological method of insulin administration.")
7
Figure 3. Basal-bolus insulin regimenFigure 3. Basal-bolus insulin regimen H ui Bolus (prandial) insulin 22. 00 3. 00 6. 00 14. 00 18. 00 22. 00 NPH ( ) Glargine ( ) Short-acting insulin ( )
 insulin NPH ( ) Glargine ( ) Short-acting insulin ( ).")
9
The use of insulin glargine as basal insulin therapy has significantly improved the glycaemic control, with a lower rate of hypoglycaemia. Its flat profile of action, the 24 hours duration and a more predictable absorption are important advantages. However, multiple daily injection treatment still has some limitsThe use of insulin glargine as basal insulin therapy has significantly improved the glycaemic control, with a lower rate of hypoglycaemia. Its flat profile of action, the 24 hours duration and a more predictable absorption are important advantages. However, multiple daily injection treatment still has some limits

10
Insufficient cover of “dawn” phenomenon Insufficient cover of “dawn” phenomenon Insufficient cover of “dusk” phenomenonInsufficient cover of “dusk” phenomenon Excessive insulin during the night, when the high insulin sensitivity may predispose to hypoglycaemia Excessive insulin during the night, when the high insulin sensitivity may predispose to hypoglycaemia Delayed action of basal insulin in the morning Delayed action of basal insulin in the morning Variable absorption of insulin, ranging from 19% to 55%, leading to glycaemic fluctuations Variable absorption of insulin, ranging from 19% to 55%, leading to glycaemic fluctuations Flexible lifestyle can be maintained under certain circumstancesFlexible lifestyle can be maintained under certain circumstances Increased number of injections.Increased number of injections.

11
A quarter of a century after its introduction, insulin pumps are widely used in clinical practice, there are now estimated to be >300,000, with approximately 250,000 in the U.S.A quarter of a century after its introduction, insulin pumps are widely used in clinical practice, there are now estimated to be >300,000, with approximately 250,000 in the U.S.

12
For CSII as a form of IIT external insulin pumps are used. These operate with the help of short acting (regular) or rapid acting insulin analogues. The insulin is delivered trough a catheter inserted subcutaneously (the abdomen is preferred site). Basal Rate (BR) of insulin infusion (24h) and insulin boluses (BS) are delivered automatically using the individual programs.For CSII as a form of IIT external insulin pumps are used. These operate with the help of short acting (regular) or rapid acting insulin analogues. The insulin is delivered trough a catheter inserted subcutaneously (the abdomen is preferred site). Basal Rate (BR) of insulin infusion (24h) and insulin boluses (BS) are delivered automatically using the individual programs.
 or rapid acting insulin analogues. The insulin is delivered trough a catheter inserted subcutaneously (the abdomen is preferred site). Basal Rate (BR) of insulin infusion (24h) and insulin boluses (BS) are delivered automatically using the individual programs.For CSII as a form of IIT external insulin pumps are used. These operate with the help of short acting (regular) or rapid acting insulin analogues. The insulin is delivered trough a catheter inserted subcutaneously (the abdomen is preferred site). Basal Rate (BR) of insulin infusion (24h) and insulin boluses (BS) are delivered automatically using the individual programs..")
13
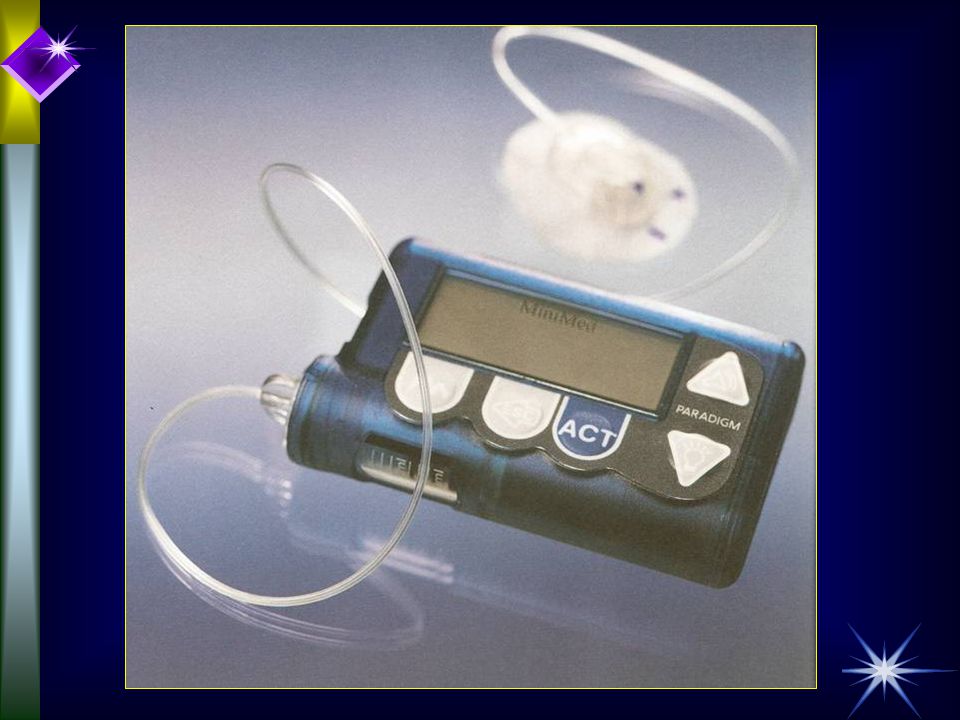
Insulin pump therapy: technical data Modern insulin pump is a pager-size compact, computerized device, which contains a small vial of regular insulin or short-acting insulin analogue (lispro, aspart, glulisine) or a syringe to be filled with insulin. Modern insulin pump is a pager-size compact, computerized device, which contains a small vial of regular insulin or short-acting insulin analogue (lispro, aspart, glulisine) or a syringe to be filled with insulin. It is attached by a catheter inserted under the skin, using a small needle, which is removed. Every two to three days, the catheter must be changed. It is attached by a catheter inserted under the skin, using a small needle, which is removed. Every two to three days, the catheter must be changed. Recent advances also include quick release tubing to enable patients to easily disconnect from the pump during activities such as showering, swimming, and intimacy.Recent advances also include quick release tubing to enable patients to easily disconnect from the pump during activities such as showering, swimming, and intimacy. The pump continuously and automatically delivers small amounts of regular or short acting insulin every few minutes. The pump continuously and automatically delivers small amounts of regular or short acting insulin every few minutes. This is called the basal rate. This is called the basal rate.
 or a syringe to be filled with insulin. It is attached by a catheter inserted under the skin, using a small needle, which is removed. Every two to three days, the catheter must be changed. It is attached by a catheter inserted under the skin, using a small needle, which is removed. Every two to three days, the catheter must be changed. Recent advances also include quick release tubing to enable patients to easily disconnect from the pump during activities such as showering, swimming, and intimacy.Recent advances also include quick release tubing to enable patients to easily disconnect from the pump during activities such as showering, swimming, and intimacy. The pump continuously and automatically delivers small amounts of regular or short acting insulin every few minutes. The pump continuously and automatically delivers small amounts of regular or short acting insulin every few minutes. This is called the basal rate. This is called the basal rate..")
14
Figure 4. “Physiological” insulin pump therapy 0 0,2 0,4 0,6 0,8 1 1,2 1,4 01234567891011121314151617181920212223 H Physiological basal insulin requirement Basal rate settled through insulin pump ui

15
Basal insulin dose Serve to maintain glycemia in target range over night and in the absence of meals or change in daily activities. The Total Daily Basal Dose (TDBD) needs to be up to 60% of the Total Insulin Daily Dose (TIDD). BS of short-acting insulin are given 30min and rapid-acting insulin 5-15min before meal. Adjustment of nighttime basal dose is based on 3 a.m and fasting Blood Glucose (BG) and daytime basal dose according BG levels when meals are skipped or delayed. Adjustment of boluses is based on 2-hours postprandial and than pre-meal BG levels.Serve to maintain glycemia in target range over night and in the absence of meals or change in daily activities. The Total Daily Basal Dose (TDBD) needs to be up to 60% of the Total Insulin Daily Dose (TIDD). BS of short-acting insulin are given 30min and rapid-acting insulin 5-15min before meal. Adjustment of nighttime basal dose is based on 3 a.m and fasting Blood Glucose (BG) and daytime basal dose according BG levels when meals are skipped or delayed. Adjustment of boluses is based on 2-hours postprandial and than pre-meal BG levels.
 needs to be up to 60% of the Total Insulin Daily Dose (TIDD). BS of short-acting insulin are given 30min and rapid-acting insulin 5-15min before meal. Adjustment of nighttime basal dose is based on 3 a.m and fasting Blood Glucose (BG) and daytime basal dose according BG levels when meals are skipped or delayed. Adjustment of boluses is based on 2-hours postprandial and than pre-meal BG levels.Serve to maintain glycemia in target range over night and in the absence of meals or change in daily activities. The Total Daily Basal Dose (TDBD) needs to be up to 60% of the Total Insulin Daily Dose (TIDD). BS of short-acting insulin are given 30min and rapid-acting insulin 5-15min before meal. Adjustment of nighttime basal dose is based on 3 a.m and fasting Blood Glucose (BG) and daytime basal dose according BG levels when meals are skipped or delayed. Adjustment of boluses is based on 2-hours postprandial and than pre-meal BG levels..")
16
MAIN ADVANTAGES Maximum flexibility; meals can be skipped or delayed; no peak insulin activity such as intermediate and long-acting insulin; insulin infusion set needs to be changed every 2-3 days instead of 4 daily injections (MDII); can be disconnected for specific activities and substitute with MDII for short periods.Maximum flexibility; meals can be skipped or delayed; no peak insulin activity such as intermediate and long-acting insulin; insulin infusion set needs to be changed every 2-3 days instead of 4 daily injections (MDII); can be disconnected for specific activities and substitute with MDII for short periods.
; can be disconnected for specific activities and substitute with MDII for short periods.Maximum flexibility; meals can be skipped or delayed; no peak insulin activity such as intermediate and long-acting insulin; insulin infusion set needs to be changed every 2-3 days instead of 4 daily injections (MDII); can be disconnected for specific activities and substitute with MDII for short periods.")
17
Other advantages More constant and predictable insulin absorption, with a variability less than 3 %. Both regular insulin and short-acting analogues appear to provide a more consistent, reproducible absorption pattern than intermediate insulin suspensions. Insulin administered by an insulin pump provides the greatest day-to- day reproducibility and insulin availability, and the least unexpected fluctuations in glycaemia control, Reduced risk of severe and exercise induced hypoglycaemia due to fact that there is minimal subcutaneous insulin depot, and a lower temporary basal rate can be settled, Improvement or slowing of other metabolic factors and diabetes complications: diabetic nephropathy, peripheral and autonomic neuropathy, retinopathy, hypertriglyceridemia and hypoalphalipoproteinemia, and diabetic changes in transplanted kidneys.

18
An indirect prove of the certain advantages of insulin pump therapy might be that more than 50% of healthcare professionals with type 1 diabetes who are members of the ADA and American Association of Diabetes Educators as well as many professional athletes(?), use insulin pumps.
, use insulin pumps.")
19
MAIN DISADVANTAGES High price; wear pump 24h/day; interruption of insulin infusion due to the pump or infusion system malfunction cause hiperglycemia and Diabetic KetoAcidosis (DKA) within hours; infection at infusion cite.High price; wear pump 24h/day; interruption of insulin infusion due to the pump or infusion system malfunction cause hiperglycemia and Diabetic KetoAcidosis (DKA) within hours; infection at infusion cite.
 within hours; infection at infusion cite.High price; wear pump 24h/day; interruption of insulin infusion due to the pump or infusion system malfunction cause hiperglycemia and Diabetic KetoAcidosis (DKA) within hours; infection at infusion cite.")
20
MAIN FEATURES IMPORTANT FOR SELECTING OF PUMP TYPE Size; type of infusion set; BS and temporary BR options; display; resistance to moisture; communication with BG meter with automatic calculation of BS; availability of 24h technical assistance and record of reliability.Size; type of infusion set; BS and temporary BR options; display; resistance to moisture; communication with BG meter with automatic calculation of BS; availability of 24h technical assistance and record of reliability.

24
Simplicity in your life

26
A great body of evidence proved that insulin pump therapy is associated with significant improvement in glycaemia control, by reducing the extreme high and low blood glucose values, and the fasting hyperglycaemia (“dawn” phenomenon). In the DCCT, 42% of subjects used CSII during their last full year of study treatment. They achieved a further reduction of HbA1C with 0.2% to 0.4% and a significant improvement in lifestyle flexibility. CSII-treated patients maintained a mean HbA1c of 6.8 % vs. 7.0 % in MDI-treated subjects during the trial (p < 0.05).
..")
27
Insulin requirements significantly decreased after switching on insulin pump therapy (pre-CSII: 53.69 ± 0.11 iu/day, or 0.74 ± 0.04 iu / kg / day and post-CSII: 44.19 ± 0.07 iu/day, or 0.62 ± 0.02 iu / kg / day; p < 0.001). Most of the studies showed a decrease in frequency of both mild and severe hypoglycaemic episodes.

28
The annual cost for MDI, with lispro and glargine was 4900 Euro compared to 9373 Euro for pumps.

29
Compared to multiple daily injections with insulin glargine, pump therapy was found to be similar or even better in youth, in terms of glycemic control, frequency of hypoglycaemia or adverse events.

30
Total daily insulin dose was unchanged in the glargine group, but significantly reduced (p < 0.01) in pump group (1.4 units/kg at baseline vs. 0.9 units/kg).
..")
31
The woman with type 1 diabetes considering pregnancy requires an intensive, flexible insulin program to normalize glucose levels before conception. Good glycemic control during pregnancy is associated with less fetal macrosomia and fewer neonatal complications. Intensive antihyperglycaemic therapy in gestational diabetes is associated with a lower risk of adverse events and maternal and fetal complications, as recently demonstrated by ACHOIS (Australian Carbohydrate Intolerance Study in Pregnancy). Insulin pump therapy is ideally suited for these situations due to less variability in blood glucose levels and the possibility to adjust insulin doses in order to rapidly improve glycemic control.
. Insulin pump therapy is ideally suited for these situations due to less variability in blood glucose levels and the possibility to adjust insulin doses in order to rapidly improve glycemic control..")
32
Metabolic benefits: reduced frequency of hypoglycaemia Tight glycemic control is associated with an increased risk for hypoglycaemia, as demonstrated by DCCT. Use of insulin pump has been proved to reduce the variability of glucose levels and severe hypoglycaemia in comparison with MDI, with no discernible reduction in glycemic control. This decrease in hypoglycaemic events has been accompanied by an increase in self-reported warning symptoms of hypoglycaemia, as well as by an increase in counter regulatory hormonal responses to hypoglycaemia

33
Severe hypoglycaemia has now become an accepted indication for initiation of CSII therapy, and may be the greatest advantage offered by CSII. Many studies demonstrated a reduced frequency of hypoglycaemia, a decreased risk of nocturnal hypoglycaemia and a decreased risk of activity- induced hypoglycaemia.

34
An analysis conducted in the United Kingdom compared the cost-effectiveness of CSII with that of MDI and found that CSII was most cost-effective in patients who had more than 2 severe hypoglycaemic events per year and who required admission to hospital at least once every year.

35
Metabolic benefits: weight control Intensive insulin therapy followed by significant improvement of glycemic control can be associated with weight gain. Reduced insulin requirements, greater flexibility in food intake and less hypoglycaemia might result in minimal weight gain among patients who use insulin pump therapy.

36
Indications for insulin pump therapy (CSII) I Insulin pump therapy should be considered for the management of: ü üType 1 diabetes poorly controlled under conventional multiple insulin injections; ü ü"Dawn” phenomenon or "reverse dawn" phenomenon (basal rate is higher from 9 PM to 3 AM and lower from 3 AM to 6 PM in young children); – –Marked daily variations in glucose levels; Brittle diabetes; Hypoglycaemia unawareness or of hypoglycaemic events requiring assistance; – –Need for flexibility in lifestyle;
 I Insulin pump therapy should be considered for the management of: ü üType 1 diabetes poorly controlled under conventional multiple insulin injections; ü ü Dawn phenomenon or reverse dawn phenomenon (basal rate is higher from 9 PM to 3 AM and lower from 3 AM to 6 PM in young children); – –Marked daily variations in glucose levels; Brittle diabetes; Hypoglycaemia unawareness or of hypoglycaemic events requiring assistance; – –Need for flexibility in lifestyle;")
37
Indications for insulin pump therapy (CSII) II Pregnancy, pre-pregnancy, gestational diabetes; – –Low insulin requirements (< 20 U/day), extreme insulin sensitivity; ü üDiabetic complications including neuropathy, retinopathy, who require intense diabetes management; – –Type 2 DM inadequately glycemic controlled by multiple daily injections; – –Glycemic control during regular vigorous exercise in people with type 1 diabetes. – –Diabetics with severe peripheral angiopathy – gangrene ü üPatients who develop DM after pacreatectomy or after pancreatic or islet transplantation

38
CSII – in pregnancy B- breakfast L - lunch D – dinner Female Bolus: 6 IU + 6 IU + 6 IU Basal rate: 00-08 h - 0.6 IU/h 08-00 h - 0.9 IU/h Bolus Basal rate BLD sleeping morning afternoonnight evening

39
Immediately before the transplantation, they were submitted to intensified insulin treatment comprising 4 daily doses using pen (5 patients) or insulin pump treatment (4 patients) in order to obtain strict metabolic control, and the treatment was continued after transplantation at least for a year.
 or insulin pump treatment (4 patients) in order to obtain strict metabolic control, and the treatment was continued after transplantation at least for a year.")
40
PATIENTS SELECTION Strongly motivated: having necessary cognitive and physical capabilities to operate the pump safety and anticipate and evaluate adjustments made in insulin dosage; patients has demonstrated willingness to perform glycemic self control; Patient has financial resources or reimbursement by healthcare insurance (state, private), sponsors; patients can quantify food intake: carbohydrate counting and carbohydrates equivalents.
, sponsors; patients can quantify food intake: carbohydrate counting and carbohydrates equivalents.")
41
PROVIDER ASPECTS Ideally, CSII therapy should be prescribed, implemented, and followed by a skilled professional team familiar with CSII therapy and capable of supporting the patients.Ideally, CSII therapy should be prescribed, implemented, and followed by a skilled professional team familiar with CSII therapy and capable of supporting the patients.

42
“Whole package” of insulin pump therapy Therapeutic patient education generally addressed to diabetes control and specifically to insulin pump is mandatory. It is important patient to understand the real benefits of insulin pump therapy and to have realistic expectations. Rigorous self-monitoring of blood glucose is also required.

43
Common misconceptions are related to the belief that:Common misconceptions are related to the belief that: –the insulin pump will cure the patient’s diabetes the patient will have a totally unrestricted free diet the patient will have a totally unrestricted free diet –pump therapy is easy with little or no adjustment needed –they will have perfect blood glucose control with the pump the patient will not have to check their blood glucose levels regularly. the patient will not have to check their blood glucose levels regularly.

44
All these beliefs should be specifically addressed in the education programme, to create the real picture of insulin pump therapy.

45
Case Report Patient J.M; female; 17 y. old, pupil.Patient J.M; female; 17 y. old, pupil. Came in our diabetic department withCame in our diabetic department with MAIN DISCONFORT: fatigue, thirst, drinking increased volume of liquid, increased volume of urine, symptoms and signs of hypogycaemiaMAIN DISCONFORT: fatigue, thirst, drinking increased volume of liquid, increased volume of urine, symptoms and signs of hypogycaemia

46
Anamnesis Diabetes mellitus type 1 appeared in 9 th year, immediate start of insulin therapy. Due to bad glycoregulation (HbA1c 11.3%) intensive insulin therapy was introduced before 6 moths (Actrapid HM and NPH). Insulin daily dose: 3 times premeal rapid acting insulin analogue NovoRapid (25+25+25=75IU) and once long acting NPH as basal insulin (46IU in the evening, before sleep). TOTAL DAILY DOSE OF INSULIN = 121 IU !!!
 intensive insulin therapy was introduced before 6 moths (Actrapid HM and NPH). Insulin daily dose: 3 times premeal rapid acting insulin analogue NovoRapid ( =75IU) and once long acting NPH as basal insulin (46IU in the evening, before sleep). TOTAL DAILY DOSE OF INSULIN = 121 IU !!!.")
47
Frequent hypoglycaemia, medium degree Keep the diet insufficient BMI =26 kg/m 2 Hyperprolactinemia. Amenorrhoea

48
Due to this reasons external insulin pump (MiniMed 508) was introduced (CSII)Due to this reasons external insulin pump (MiniMed 508) was introduced (CSII) Basal rate 1 IU / h = 24 IUBasal rate 1 IU / h = 24 IU Boluses 14+14+14 = 42 IUBoluses 14+14+14 = 42 IU TOTAL DAILY DOSE OF INSULIN = 66 IUTOTAL DAILY DOSE OF INSULIN = 66 IU
 was introduced (CSII)Due to this reasons external insulin pump (MiniMed 508) was introduced (CSII) Basal rate 1 IU / h = 24 IUBasal rate 1 IU / h = 24 IU Boluses = 42 IUBoluses = 42 IU TOTAL DAILY DOSE OF INSULIN = 66 IUTOTAL DAILY DOSE OF INSULIN = 66 IU")
49
After 2 month: HbA1c 12%, predominat hyperglycaemia, rare hypoglycaemiaAfter 2 month: HbA1c 12%, predominat hyperglycaemia, rare hypoglycaemia Daily profile of glycaemia: 07h 15.0mmol/L (before breakfast), 2h after 5.0, before lunch 24.9, 2h after 25.6, before dinner 19.4, 2h after 15.6, 24h 14.7, 03h 19.9 mmol/LDaily profile of glycaemia: 07h 15.0mmol/L (before breakfast), 2h after 5.0, before lunch 24.9, 2h after 25.6, before dinner 19.4, 2h after 15.6, 24h 14.7, 03h 19.9 mmol/L No ketosesNo ketoses
, 2h after 5.0, before lunch 24.9, 2h after 25.6, before dinner 19.4, 2h after 15.6, 24h 14.7, 03h 19.9 mmol/LDaily profile of glycaemia: 07h 15.0mmol/L (before breakfast), 2h after 5.0, before lunch 24.9, 2h after 25.6, before dinner 19.4, 2h after 15.6, 24h 14.7, 03h 19.9 mmol/L No ketosesNo ketoses")
50
Multiple insulin injection was introduced again:Multiple insulin injection was introduced again: NovoRapid boluses before meal: 18+18+18 IU, Insulatard 30 IU in the evening.NovoRapid boluses before meal: 18+18+18 IU, Insulatard 30 IU in the evening. TOTAL DAILY DOSE OF INSULIN = 84 IUTOTAL DAILY DOSE OF INSULIN = 84 IU

51
Other investigations Insulin antibody 13.9% INCEREASED (serum, RIA, upper normal limit 5.2%)Insulin antibody 13.9% INCEREASED (serum, RIA, upper normal limit 5.2%) IgE antibodies specific for human insulin <0.35 kUA (normal range 2-100)IgE antibodies specific for human insulin <0.35 kUA (normal range 2-100) IgA 2.148 gr/L (normal); IgG 10.34 gr/L (normal); IgM 1.24 gr/L (normal) ; Total amount IgE <9.0 kU/LIgA 2.148 gr/L (normal); IgG 10.34 gr/L (normal); IgM 1.24 gr/L (normal) ; Total amount IgE <9.0 kU/L Immune complexes: 2.253, INCREASED (normal <0.5)Immune complexes: 2.253, INCREASED (normal <0.5)
Insulin antibody 13.9% INCEREASED (serum, RIA, upper normal limit 5.2%) IgE antibodies specific for human insulin <0.35 kUA (normal range 2-100)IgE antibodies specific for human insulin <0.35 kUA (normal range 2-100) IgA gr/L (normal); IgG gr/L (normal); IgM 1.24 gr/L (normal) ; Total amount IgE <9.0 kU/LIgA gr/L (normal); IgG gr/L (normal); IgM 1.24 gr/L (normal) ; Total amount IgE <9.0 kU/L Immune complexes: 2.253, INCREASED (normal <0.5)Immune complexes: 2.253, INCREASED (normal <0.5)")
52
The new regime of insulin therapy was introduced:The new regime of insulin therapy was introduced: Lantus insulin in the morning 44 IULantus insulin in the morning 44 IU NovoRapid insulin in the morning 14IU and in the evening 28 IUNovoRapid insulin in the morning 14IU and in the evening 28 IU TOTAL DAILY INSULIN DOSE = 72 IUTOTAL DAILY INSULIN DOSE = 72 IU Keep the diet further insufficientKeep the diet further insufficient

53
After one month:After one month: Lantus insulin in the morning 40 IULantus insulin in the morning 40 IU NovoRapid insulin in the morning 14 IU and in the evening 14 IU = 28 IUNovoRapid insulin in the morning 14 IU and in the evening 14 IU = 28 IU TOTAL DAILY INSULIN DOSE = 68 IUTOTAL DAILY INSULIN DOSE = 68 IU Daily profile of glycaemia: mean 9.0 mmol/LDaily profile of glycaemia: mean 9.0 mmol/L Rare, mild hypoglycaemia, NOT DURING THE NIGHTRare, mild hypoglycaemia, NOT DURING THE NIGHT Better adherence to diet, motivation, education for IIT, support from familyBetter adherence to diet, motivation, education for IIT, support from family Every day 24h contact with our departmentEvery day 24h contact with our department

54
Summary I Bad glycoregulation in log period of time despite: Enormous total daily dose of insulin Application of MDII (121 IU) after that CSII (66 IU) Immunological insulin resistance: insulin antibodies, >1 IU/kg of insulin Bad adherence to diet, no motivation, education, support from family Insufficient contact with state diabetic care services
 after that CSII (66 IU) Immunological insulin resistance: insulin antibodies, >1 IU/kg of insulin Bad adherence to diet, no motivation, education, support from family Insufficient contact with state diabetic care services")
55
Summary II Good effects of insulin analogues: Lantus insulin (long acting) NovoRapid (rapid, short-acting) Total daily dose ≈ 1 IU/kg One may expect further decrease of total insulin daily dose If insulin pump intent to be used again in this patients rapid, short-acting insulin analogues need to be introduced (NovoRapid ? Lispro ?)
.")
56
Conclusion Pup therapy (CSII) has many biological, medical, social limitations especially if contraindications are not respectedPup therapy (CSII) has many biological, medical, social limitations especially if contraindications are not respected Insulin analogues may be useful in some cases of MDII and CSII failureInsulin analogues may be useful in some cases of MDII and CSII failure
 has many biological, medical, social limitations especially if contraindications are not respectedPup therapy (CSII) has many biological, medical, social limitations especially if contraindications are not respected Insulin analogues may be useful in some cases of MDII and CSII failureInsulin analogues may be useful in some cases of MDII and CSII failure")
57
Aspart vs Lispro vs Regular CSII in Type 1 Diabetes N = 146, mean age 38, BMI 25 AspartLisproRegular Base 4 moBase 4 moBase 4mo HbA 1c %7.34 7.367.29 7.47 7.477.63 PG 90 min after dinner mmol/l7.6 (p<0.02)9.19.5 Pump or line blockageNo differences HypoglycemiaNo differences Bode BW et al. Diabetes; 50(Suppl 2):A106
:A106.")
58
Episodes/month/patient 0 2 4 6 8 10 12 NovoRapid®human insulininsulin lispro p<0.05 p<0.05 NovoRapid® vs human insulin vs insulin lispro in CSII study: Self-Reported Hypoglycaemia ANA 2024, Data on File

59
A retrospective study on 82 adults with type 1 diabetes, duration 19.7 ± 9.9 years, who started CSII after a MDI regimen with either NPH or glargine, regular or short acting analogues showed that after 3 months of CSII, HbA1c significantly decreased, 8.35 ± 1.06 % vs. 9.39 ± 1.35%, (p < 0.001) and the reduction was maintained over the whole CSII treatment. Significant decrease of severe hypoglycaemic episodes (0.35 ± 0.07 per patient/year during MDI vs. 0.10 ± 0.02 during CSII, p < 0.001) and insulin requirement (52.1 ± 17.5 units/day vs. 38.8 ± 12.3, p < 0.001) have been found. According to this study, older age and higher baseline HbA1c predict the better glycemic improvement.
 and the reduction was maintained over the whole CSII treatment. Significant decrease of severe hypoglycaemic episodes (0.35 ± 0.07 per patient/year during MDI vs ± 0.02 during CSII, p < 0.001) and insulin requirement (52.1 ± 17.5 units/day vs ± 12.3, p < 0.001) have been found. According to this study, older age and higher baseline HbA1c predict the better glycemic improvement..")
60
STARTING INSULIN DOSE Firstly, reduce TIDD on MDII by 25-30%. Staring dose must be individualized for each patient. TDBD should be 40-60% of TIDD (divide by 24 to obtain hourly BR, usual range 0.5-2.0 U/hour for type 2 diabetics). TDBD can be calculated by multiplying the patients weight in kg by 0.3 (divide by 24 to obtain hourly BR). Higher BR from 3-9am, intermediate during the day, lower at bedtime. For pre-meal BS (from TDBD): breakfast 20%, lunch 10%, supper 15%, bedtime 5%. Calculation based according to patient’s sensitivity (i.e. 0.5-2.0 U/15g carbohydrate). Adjusted BR and BS by 10-20% based on BG readings before and after meals, at bedtime and at 3am. All patients on IIT should be provided with correction BS or supplemental BS guidelines to correct out-of-range BG values, using the 1700 rule.Firstly, reduce TIDD on MDII by 25-30%. Staring dose must be individualized for each patient. TDBD should be 40-60% of TIDD (divide by 24 to obtain hourly BR, usual range 0.5-2.0 U/hour for type 2 diabetics). TDBD can be calculated by multiplying the patients weight in kg by 0.3 (divide by 24 to obtain hourly BR). Higher BR from 3-9am, intermediate during the day, lower at bedtime. For pre-meal BS (from TDBD): breakfast 20%, lunch 10%, supper 15%, bedtime 5%. Calculation based according to patient’s sensitivity (i.e. 0.5-2.0 U/15g carbohydrate). Adjusted BR and BS by 10-20% based on BG readings before and after meals, at bedtime and at 3am. All patients on IIT should be provided with correction BS or supplemental BS guidelines to correct out-of-range BG values, using the 1700 rule.
. TDBD can be calculated by multiplying the patients weight in kg by 0.3 (divide by 24 to obtain hourly BR). Higher BR from 3-9am, intermediate during the day, lower at bedtime. For pre-meal BS (from TDBD): breakfast 20%, lunch 10%, supper 15%, bedtime 5%. Calculation based according to patient’s sensitivity (i.e U/15g carbohydrate). Adjusted BR and BS by 10-20% based on BG readings before and after meals, at bedtime and at 3am. All patients on IIT should be provided with correction BS or supplemental BS guidelines to correct out-of-range BG values, using the 1700 rule.Firstly, reduce TIDD on MDII by 25-30%. Staring dose must be individualized for each patient. TDBD should be 40-60% of TIDD (divide by 24 to obtain hourly BR, usual range U/hour for type 2 diabetics). TDBD can be calculated by multiplying the patients weight in kg by 0.3 (divide by 24 to obtain hourly BR). Higher BR from 3-9am, intermediate during the day, lower at bedtime. For pre-meal BS (from TDBD): breakfast 20%, lunch 10%, supper 15%, bedtime 5%. Calculation based according to patient’s sensitivity (i.e U/15g carbohydrate). Adjusted BR and BS by 10-20% based on BG readings before and after meals, at bedtime and at 3am. All patients on IIT should be provided with correction BS or supplemental BS guidelines to correct out-of-range BG values, using the 1700 rule..")
61
PUMP MALFUNCTION If it occurs, use usual dose of short or rapid-acting insulin before meals and long-acting insulin at bedtime. If it occurs, use usual dose of short or rapid-acting insulin before meals and long-acting insulin at bedtime. If the patients wish to disconnect pump it is possible up to 2 to 4 hours without any adverse consequences. If the patients wish to disconnect pump it is possible up to 2 to 4 hours without any adverse consequences. For the period longer than 4 hours the usual basal-bolus therapy should be given. For the period longer than 4 hours the usual basal-bolus therapy should be given. The dose of the long-acting Glargine will be equal to TDBD. The dose of the long-acting Glargine will be equal to TDBD. It is important to teach patients to adjust short or rapid- acting insulin for variations in food intake and to adjust insulin for exerciseIt is important to teach patients to adjust short or rapid- acting insulin for variations in food intake and to adjust insulin for exercise

62
PREVENTION OF HYPERGLYCEMIA AND HYPOGLYCEMIA as well must be performed continuously. HYPERGLYCEMIA>13.9mmol/l must be treated to prevent DKA especially during pregnancy.PREVENTION OF HYPERGLYCEMIA AND HYPOGLYCEMIA as well must be performed continuously. HYPERGLYCEMIA>13.9mmol/l must be treated to prevent DKA especially during pregnancy. TO PREVENT HYPOGLYCEMIA educate patient and family; teach patient a systemic approach to matching insulin to food intake and change in routine; patients should check BG levels at least 4 times daily (before meals and bedtime), weekly at 3am, before and after exercise, every 2 hours during illness, before driving reach BG values>80mg/dl; bedtime snacks consisting protein and carbohydrate to avoid nocturnal hypoglycemia.TO PREVENT HYPOGLYCEMIA educate patient and family; teach patient a systemic approach to matching insulin to food intake and change in routine; patients should check BG levels at least 4 times daily (before meals and bedtime), weekly at 3am, before and after exercise, every 2 hours during illness, before driving reach BG values>80mg/dl; bedtime snacks consisting protein and carbohydrate to avoid nocturnal hypoglycemia.
, weekly at 3am, before and after exercise, every 2 hours during illness, before driving reach BG values>80mg/dl; bedtime snacks consisting protein and carbohydrate to avoid nocturnal hypoglycemia.TO PREVENT HYPOGLYCEMIA educate patient and family; teach patient a systemic approach to matching insulin to food intake and change in routine; patients should check BG levels at least 4 times daily (before meals and bedtime), weekly at 3am, before and after exercise, every 2 hours during illness, before driving reach BG values>80mg/dl; bedtime snacks consisting protein and carbohydrate to avoid nocturnal hypoglycemia..")
63
SAFETY CSII with pump is as safe as MDII when recommended indications and procedure are followed. Undetected interruptions in insulin delivery may result in ketotic episodes more often and more quickly with CSII which is of particular concern in pregnancy. Infections or inflammation at the needle cite may occur also.CSII with pump is as safe as MDII when recommended indications and procedure are followed. Undetected interruptions in insulin delivery may result in ketotic episodes more often and more quickly with CSII which is of particular concern in pregnancy. Infections or inflammation at the needle cite may occur also.

66
CSII EVOLUTION Pump therapy in type 1 diabetics starts in 1970’s. Since than, pumps have become much smaller more durable and easier to use. Modern pump have electronic memory, multiple BR, different BS options, safety alarms and remote controls. New software permitted the correction BS for an out-of- range BG level and how much insulin to give for a certain amount of carbohydrate.Pump therapy in type 1 diabetics starts in 1970’s. Since than, pumps have become much smaller more durable and easier to use. Modern pump have electronic memory, multiple BR, different BS options, safety alarms and remote controls. New software permitted the correction BS for an out-of- range BG level and how much insulin to give for a certain amount of carbohydrate.

67
FUTURE OF PUMP THERAPY Once continuous glucose monitoring is available, the effectiveness of pump therapy in achieving near-normal glycemia will be enhanced and patients than may avoid hypoglycemic or hypoglicemyc episodes. Almost the final steps will be closed-loop systems as an external or implantible feeding back to an external or implantable pump.Once continuous glucose monitoring is available, the effectiveness of pump therapy in achieving near-normal glycemia will be enhanced and patients than may avoid hypoglycemic or hypoglicemyc episodes. Almost the final steps will be closed-loop systems as an external or implantible feeding back to an external or implantable pump.

68
SonorSonor MonitorMonitor Com-stationCom-station SoftwereSoftwere

73
NEW THERAPEUTIC AREA FOR EXTERNAL PUMPS For type 2 DM the CSII is used also. But, whether it is ever necessary or advantageous compared with a less complex treatment is unknown. Nevertheless, in these patients much lower risk of hypoglycemia exists. Some studies showed that the glycemic control may be as good as or better than with MDII regime. Recent results shoved the benefit of short term CSII in the case of secondary failure of per oral therapy and in newly diagnosed type 2 DMFor type 2 DM the CSII is used also. But, whether it is ever necessary or advantageous compared with a less complex treatment is unknown. Nevertheless, in these patients much lower risk of hypoglycemia exists. Some studies showed that the glycemic control may be as good as or better than with MDII regime. Recent results shoved the benefit of short term CSII in the case of secondary failure of per oral therapy and in newly diagnosed type 2 DM

74
Conclusions I In most patients, mean blood glucose levels and glycated haemoglobin A1c are either slightly lower or similar on CSII versus MDI; In most patients, mean blood glucose levels and glycated haemoglobin A1c are either slightly lower or similar on CSII versus MDI; Hypoglycaemia is markedly less frequent than during intensive injection therapy; Hypoglycaemia is markedly less frequent than during intensive injection therapy; Diabetes ketoacidosis occurs at the same rate; Diabetes ketoacidosis occurs at the same rate; Nocturnal glycemic control is improved with insulin pumps; Nocturnal glycemic control is improved with insulin pumps; Basal rate changes help to minimize the "dawn phenomenon“; Basal rate changes help to minimize the "dawn phenomenon“; Insulin pump therapy is safe and effective in children and adolescents, where fewer episodes of severe hypoglycaemia have been found, with no increase in ketoacidosis while maintaining the glycemic control. One of the particular benefits of CSII in infants and toddlers is its ability to reduce the risk of severe hypoglycaemia. Even limited use of CSII for overnight basal insulin replacement in children 7 to 10 years of age has been shown to be effective. Insulin pump therapy is safe and effective in children and adolescents, where fewer episodes of severe hypoglycaemia have been found, with no increase in ketoacidosis while maintaining the glycemic control. One of the particular benefits of CSII in infants and toddlers is its ability to reduce the risk of severe hypoglycaemia. Even limited use of CSII for overnight basal insulin replacement in children 7 to 10 years of age has been shown to be effective.

75
Conclusions II The small age of the patient should not, itself, be a barrier to initiation of this therapy. The small age of the patient should not, itself, be a barrier to initiation of this therapy. Use of lispro, aspart or glulisine in CSII is particularly suitable for infants and toddlers, who have unpredictable appetites and eating patterns, because it can be administered either before or after meal, depending on the amount of carbohydrate that is eaten; Use of lispro, aspart or glulisine in CSII is particularly suitable for infants and toddlers, who have unpredictable appetites and eating patterns, because it can be administered either before or after meal, depending on the amount of carbohydrate that is eaten; A successful therapy with CSII involves the appropriate selection, evaluation and training of individuals, a skilled and motivated health care team and close contact between the pump user and the health care team.A successful therapy with CSII involves the appropriate selection, evaluation and training of individuals, a skilled and motivated health care team and close contact between the pump user and the health care team. CGMS usage serves to optimize therapy and metabolic control in patients children and adults, with type 1 Diabetes mellitus, and CSII. CGMS provides a new level of protection against dangerous hyperglicaemia and especially hypoglicaemia. CGMS is an very important part of CSII now in even more in the future. CGMS usage serves to optimize therapy and metabolic control in patients children and adults, with type 1 Diabetes mellitus, and CSII. CGMS provides a new level of protection against dangerous hyperglicaemia and especially hypoglicaemia. CGMS is an very important part of CSII now in even more in the future.

Similar presentations






















>")

