Download presentation
Presentation is loading. Please wait.

1
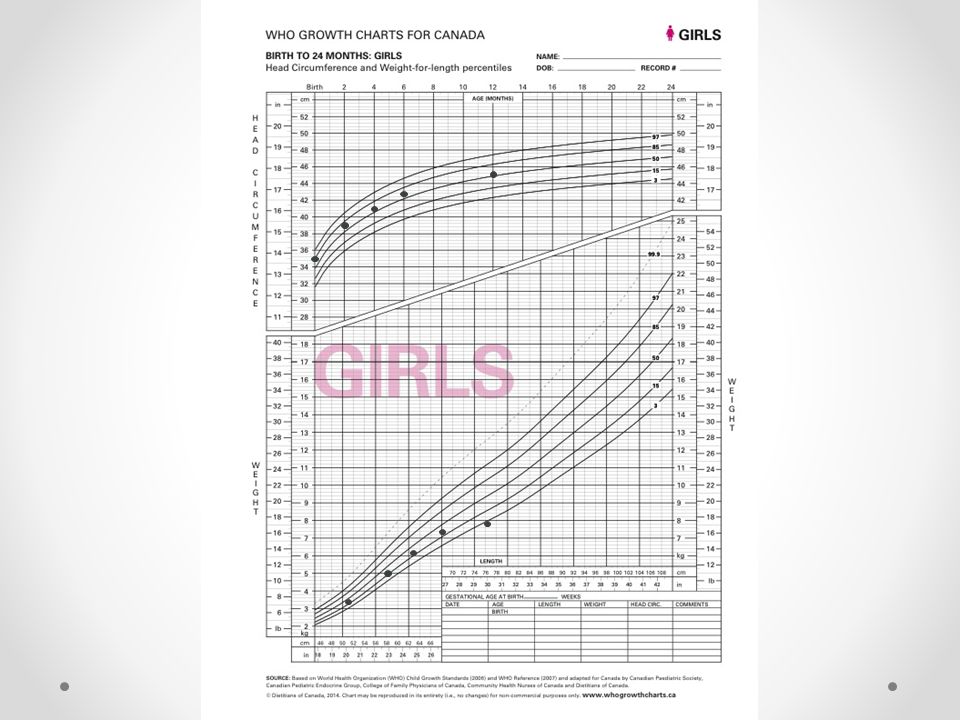
While you wait, please plot out our patient’s growth
Birth wt: 3.4 kg ht: 51 cm hc: 35 cm 2 mo wt: 5.0 kg ht: 58 cm hc: 39 cm 4 mo wt: 6.3 kg ht: 63 cm hc: 41 cm 6 mo wt: 7.4 kg ht: 67 cm hc: 42.6 cm 12 mo wt: 7.8 kg ht: 75 cm hc: 45.2 cm

2
Geneviève Moreau June 9th 2015
Failure to Thrive Geneviève Moreau June 9th 2015

3
Objectives Identify normal and abnormal patterns of infant growth (see attached growth charts) Correctly plot and interpret grown parameters, with an understanding of growth velocities and relationships between growth parameters Develop knowledge of normal infant nutrition Identify failure to thrive and describe its causes, evaluation, management, and sequelae

4
Normal Growth Patterns
What is a normal birth weight for a baby born at term? 3,25 kg (7 lbs) +/- 2SD From the 10th-90th percentile (2,8-4,0 kg) What is the accepted weight loss within the first week of life? 10% When should the newborn have regained this weight? d
 +/- 2SD From the 10th-90th percentile (2,8-4,0 kg) What is the accepted weight loss within the first week of life 10% When should the newborn have regained this weight d")
5
Normal Growth Patterns
What is the expected rate of weight gain in the term newborn? g/d Doubled at 4-5 mo Tripled at 1 yr Quadrupled at 2 yrs

6
Failure to Thrive Indications for Investigation
Weight < 3rd percentile Weight falls across 2 major percentile curves Weight < 80% of expected value for height and age 1- Determine length for age percentile 2- Determine weight for age corresponding to that percentile Rate of daily weight gain less than expected for age 0-3 mo g/d 3-6 mo g/d 6-9 mo g/d 9-12 mo g/d 1-3 yrs 7-9 g/d

7
Case 1 Lynn Thin, a 13 month old girl has just moved to your community and is coming to see you for the first time. Her previous family physician noted that her weight hadn’t increased as expected when he saw her just before moving. Lynn and her mother arrive for the appointment with a list of her previous growth measurements. What should we ask on history?

8
History Nutritional intake Duration of mealtimes Type of food
Quantity of food Food preference and avoidance Juice ingestion Dietary restrictions, allergies Current symptoms Vomiting Diarrhea Rumination Developmental history Psychosocial history

9
History Prenatal and perinatal history Birth weight IUGR
Perinatal stress Prenatal exposures (medications, drugs and alcohol) Past medical history Chronic diseases Past illnesses Frequent recurrent infections Frequent injuries Family history Growth and puberty Parental height and weight Genetic disorders and syndromes
 Past medical history. Chronic diseases. Past illnesses. Frequent recurrent infections. Frequent injuries. Family history. Growth and puberty. Parental height and weight. Genetic disorders and syndromes.")
10
History On history, you find out that Lynn is a first child of healthy parents. Her 23 year old mother smoked during pregnancy, but did not use any alcohol or drugs, and had no medical problems. Lynn was born 10 days early by spontaneous vaginal delivery. She was breastfed until 7 months of age, when her mother had to go back to work. She was started on milk at that time. Solid foods were introduced starting at 8 months. She currently drinks 5 large bottles of milk per day and eats table foods. Her parents find that she is a picky eater and spits out foods that she does not like. They tend to stick to her favourites – applesauce, cookies, and pasta. They are quite frustrated with the difficulties around mealtimes. Lynn has had no medical problems. She has attended all scheduled medical appointments and her vaccinations are up to date. Lynn’s mother reports that she has a distant cousin with cystic fibrosis and another cousin with a “hole in the heart”. She is worried that Lynn may have one of these problems. Lynn’s development is appropriate for her age. Her mother is working part-time as a cashier and her father was recently fired from his job in construction. Nutrition exclusive breastfeeding until 6 mo with vit D supplementation followed by gradual introduction of solids important to introduce iron-containing foods, as breastmilk does not contain iron and the baby’s store of maternal iron runs out at 6 months 6-9 mo: introduction of solids starting with iron rich foods (meats, enriched cereals) then pureed veggies then fruits 9-12 mo: introduction of finger foods, switch to homo milk limit cow milk to 600 mL/day (16 oz/d) from the age of 1-5 yrs old Breastmilk content colostrum (first few days): high protein, low fat, immunoglobulin 70:30 whey:casein ratio, dietary butterfat, lactose Cow milk vs Breastmilk - lower whey:casein ratio, plant fats
 then pureed veggies. then fruits mo: introduction of finger foods, switch to homo milk. limit cow milk to 600 mL/day (16 oz/d) from the age of 1-5 yrs old. Breastmilk content. colostrum (first few days): high protein, low fat, immunoglobulin. 70:30 whey:casein ratio, dietary butterfat, lactose. Cow milk vs Breastmilk. - lower whey:casein ratio, plant fats.")
11
Physical Growth (height, weight, head circumference) Head to toe
Dysmorphic features Tanner staging Signs of abuse or neglect Signs of vitamin deficiency

12
Physical On examination, Lynn is slim and slightly pale. She is cheerful and interactive. Her head-to-toe exam is otherwise normal.

13
Mrs. Thin is very worried about her daughter
Mrs. Thin is very worried about her daughter. She wants to know what the problem is, what investigations need to be done, and whether Lynn’s poor growth will cause long-term problems.

14
Important to ask about changes in the child’s life and environment at the time of the change in slope Must correct for GA if premature (~ 2 yrs) Need 2 points that cross the threshold for investigation
 Need 2 points that cross the threshold for investigation.")
16
Is Lynn’s growth pattern normal?

17
Differential Diagnosis FTT (Wasting)
Inadequate Intake Low volume Diet lacking in nutrients Oromotor dysfunction (neuro, ENT, esophageal) Anorexia (psychosocial, chronic disease, malignancy, meds) Inadequate Absorption or Increased Losses Vomiting Malabsorption (lactose intolerance, cystic fibrosis, IBD, celiac) Biliary atresia Bowel obstruction (pyloric stenosis, malrotation, intussusception) - 90% have non-organic cause (dietary intake, feeding environment, stress)
 Anorexia (psychosocial, chronic disease, malignancy, meds) Inadequate Absorption or Increased Losses. Vomiting. Malabsorption (lactose intolerance, cystic fibrosis, IBD, celiac) Biliary atresia. Bowel obstruction (pyloric stenosis, malrotation, intussusception) - 90% have non-organic cause (dietary intake, feeding environment, stress)")
18
Differential Diagnosis FTT (Wasting)
Increased Needs or Ineffective Utilization Chronic disease (IBD, heart disease, cystic fibrosis, CKD) Chronic or recurrent infection (TB, HIV, toxoplasmosis) Malignancy Chronic metabolic problems (DM, hyperT4, adrenal insufficiency) Based on the history and exam, what investigations, if any, should be considered? Note: Endocrine disorders are more likely to present as short stature
 Chronic or recurrent infection (TB, HIV, toxoplasmosis) Malignancy. Chronic metabolic problems (DM, hyperT4, adrenal insufficiency) Based on the history and exam, what investigations, if any, should be considered Note: Endocrine disorders are more likely to present as short stature.")
19
Investigations FTT (Wasting)
To be considered based on presentation: Food journal CBC, smear Lytes Ferritin, Fe, TIBC Vitamin levels GI workup: OT evaluation, baryum swallow Celiac screen (anti-tTG, IgA) Crohn’s screen (scope, biopsy) Endocrine workup: TSH, T4 Etc etc
 Crohn’s screen (scope, biopsy) Endocrine workup: TSH, T4. Etc etc.")
20
Follow-Up FTT (Wasting)
Catch-up growth (rate of weight gain 2-3 times the normal range) can be seen from 2 days to 2 weeks after then start of an intervention Failure to achieve catch-up growth after 2-3 months of primary care intervention should be referred to a specialist/multidisciplinary team NG tube feeding is indicated if there is no catch-up growth after 4-6 wks with adequate oral intake Gastrostomy tube is indicated if weight gain is inadequate after 3-4 mo of NG tube feeding NG feeding indicated if no catch-up growth after 4-6 wks with adequate oral intake Gastrostomy tube indicated if weight gain inadequate after 3-4 mo of NG feeding
 can be seen from 2 days to 2 weeks after then start of an intervention. Failure to achieve catch-up growth after 2-3 months of primary care intervention should be referred to a specialist/multidisciplinary team. NG tube feeding is indicated if there is no catch-up growth after 4-6 wks with adequate oral intake. Gastrostomy tube is indicated if weight gain is inadequate after 3-4 mo of NG tube feeding. NG feeding indicated if no catch-up growth after 4-6 wks with adequate oral intake. Gastrostomy tube indicated if weight gain inadequate after 3-4 mo of NG feeding.")
21
Sequelae FTT (Wasting)
Cognitive deficits Behavioral problems Learning difficulties 50% of children with FTT have below normal cognitive function it is uncertain whether this is a result of the FTT or of coexisting psychosocial factors

22
Case 2 Your next patient, Julie Petit, is a 24 month old girl who comes in for her routine vaccinations. As usual, you add the latest growth measurements to her chart.

24
Differential Diagnosis Short Stature

25
Differential Diagnosis Short Stature
Endocrine disorders (hypoT4, Cushing’s, GH deficiency, CNS tumor) Rhumatologic disease (JIA) Renal disease Malignancy This is Ddx for baby/infant; there are more ddx for older children
 Rhumatologic disease (JIA) Renal disease. Malignancy. This is Ddx for baby/infant; there are more ddx for older children.")
26
Case 3 Your next patient, William Turner, is brought in by his parents who are worried because “he is much smaller than all of the other kids his age”. After performing a complete history and physical exam, you plot out his latest growth points.

28
Differential Diagnosis Proportionally Small Weight and Height

29
Differential Diagnosis Proportionally Small Weight and Height
Familial short stature Constitutional growth delay IUGR Syndromes and chromosomal disorders (Turner, Down, Prader-Willi, Russell-Silver) Skeletal dysplasia (scoliosis, achondroplasia) IUGR babies expected to catch up by 2 yrs Russell-Silver: IUGR + post-natal growth retardation + facial features (prominent forehead, triangular face, downturned corners of mouth + body asymmetry - facial features become less apparent with age Proportionate: IUGR, chromosomal Disproportionate: - U/L ratio elevated: achondroplasia - U/L ratio low: scoliosis Normal U/L ratio 1.8:1 in newborns 1:1 in 8 yo
 Skeletal dysplasia (scoliosis, achondroplasia) IUGR babies expected to catch up by 2 yrs. Russell-Silver: IUGR + post-natal growth retardation + facial features (prominent forehead, triangular face, downturned corners of mouth + body asymmetry. - facial features become less apparent with age. Proportionate: IUGR, chromosomal. Disproportionate: - U/L ratio elevated: achondroplasia. - U/L ratio low: scoliosis. Normal U/L ratio. 1.8:1 in newborns. 1:1 in 8 yo.")
30
Calculations Proportionally Small Weight and Height
Mid-parental height Boys: (father + mother + 13 cm)/2 Girls: (father + mother - 13 cm)/2 Predicted definitive height Bony age determination by XR Mid-parental height target height = this value +/- 10 cm determine the percentile of the target height in adults the child should be within that percentile Compare bony age to chronological age BA = CA: likely familial BA < CA: likely constitutional delay
/2 Girls: (father + mother - 13 cm)/2 Predicted definitive height Bony age determination by XR Mid-parental height. target height = this value +/- 10 cm. determine the percentile of the target height in adults. the child should be within that percentile. Compare bony age to chronological age. BA = CA: likely familial. BA < CA: likely constitutional delay.")
31
Thank You

32
Extras

33
Management of the normal growth pattern and a worried parent
Reassure In the first 3 years of life, children’s percentiles may fluctuate (it should not change from 3 yrs of age until puberty) Breastfed babies tend to grow faster in the first 6 months of life, whereas formula-fed babies grow faster after 6 months Continue to monitor growth In the first 2 yrs of life of normal children: 30% cross 1 major percentile line 23% cross 2 major percentile lines
 Breastfed babies tend to grow faster in the first 6 months of life, whereas formula-fed babies grow faster after 6 months. Continue to monitor growth. In the first 2 yrs of life of normal children: 30% cross 1 major percentile line. 23% cross 2 major percentile lines.")
34
Counselling the parent of a picky eater
Allow the child to develop a sense of autonomy Eat as a family Create a positive atmosphere at the table Encourage exercise and play Give time to prepare and settle down before meals Limit time at the table Limit distractions at the table Avoid grazing between meals and snacks Avoid excessive amounts of milk or juice Avoid coaxing or coercing

Similar presentations