Download presentation
Presentation is loading. Please wait.

1
Charlotte McKinley Jessica Midence Izabella Messina
Smallpox Charlotte McKinley Jessica Midence Izabella Messina

2
Smallpox Smallpox is a serious, contagious and sometimes fatal disease. There is no specific treatment for smallpox, and the only prevention is vaccination. The name smallpox is derived from the latin word “spotted” and refers to the raised bumps that appear on the face and body of an infected person. Smallpox is in the Orthopoxvirus genus of viruses.

3
Origin of Smallpox The name Variola was first used in the 6th century. Derived from the Latin word varius (spotted) or varus (pimple). Anglo-Saxons in the 10th century used the word poc or pocca (bag or pouch) to describe an exanthemous disease, possibly smallpox. In the 15th century, the English used the prefix small to distinguish variola the smallpox from syphilis, the great pox.
 to describe an exanthemous disease, possibly smallpox. In the 15th century, the English used the prefix small to distinguish variola the smallpox from syphilis, the great pox.")
4
First Case of Smallpox There is no animal reservoir, and no human carriers. First certain evidence comes from the mummified remains of Ramses. (1157 B.C.) Written descriptions did not appear until the 10th century in Southwestern Asia.
 Written descriptions did not appear until the 10th century in Southwestern Asia.")
5
Smallpox Travel Smallpox was likely carried from Egyptian traders to India during the millennium B.C. where it became established as an endemic infection. Epidemics of the disease can be found in the bible, and in ancient Greek and Roman literature. From Asia and Africa smallpox spread with increasing frequency into less populous areas, and then into Europe.

6
Smallpox in the Ancient World
Peloponnesian Wars (430 B.C.) Thucydides recorded smallpox symptoms. A person aboard a ship from North Africa came to Athens infected with smallpox. Described as violent heats, unnatural, putrid odors, stomach distress, and the body covered with small pustules and ulcers. Also noted that those who survived became immune.
 Thucydides recorded smallpox symptoms. A person aboard a ship from North Africa came to Athens infected with smallpox. Described as violent heats, unnatural, putrid odors, stomach distress, and the body covered with small pustules and ulcers. Also noted that those who survived became immune.")
7
Smallpox in the New World
In the early 16th century smallpox began to imported into the western hemisphere. The Spanish inadvertently owe success in conquering the Aztec and Incas in Mexico to smallpox. Smallpox arrived in North America via Canada, and Mexico.

8
Smallpox as Biological Warfare
Lord Jeffrey Amherst, Commanding General of British Forces in North America during the French and Indian War. ( ) Used blankets (smallpox blankets) coated with smallpox dust as germ warfare to wipe out the Native American population.
 Used blankets (smallpox blankets) coated with smallpox dust as germ warfare to wipe out the Native American population.")
9
History of Variolation and Vaccine
Known that survivors became immune to the disease. As a result, physicians intentionally infected healthy persons with smallpox organisms. Variolation is the act of taking samples (pus from pustules or ground scabs) from patients whose disease had been benign, and introducing it into others through the nose or skin.
 from patients whose disease had been benign, and introducing it into others through the nose or skin.")
10
Survival Rates with Variolation
Two to Three percent of variolated persons died of smallpox, became the source of a new epidemic, or developed other illnesses from the lymph of the donor such as tuberculosis or syphilis. The case fatality rates were still ten times lower in those that were variolated compared to those with naturally occurring smallpox. Side effects of variolation were the appearance of smallpox itself, but it would disappear after a week or so.

11
Variolation in the New World
Reached the New World in 1721. Used to stop the epidemic in Boston. In 1766 American Soldiers under George Washington were unable to take Quebec from the English because of smallpox. Smallpox was apparently one of the main causes of the preservation of Canada in the British Empire. In 1777 Washington had all of his soldiers variolated beginning with new military operations.

12
Cows, Milkmaids, and the Pox
In rural areas of Europe it was known the milkmaids became immune to smallpox after developing smallpox 1774, farmer Benjamin Jesty was the first to vaccinate his wife and kids with material taken from the utters of cows. 1791, school teacher Peter Plett vaccinated his students with material from the utters of cows.

13
Edward Jenner

14
Edward Jenner Studied to become a physician in England.
In May of 1776 dairymaid Sarah Nelmes consulted Jenner about a rash on her hand. He took this opportunity to test the protective properties of cowpox against smallpox. Determined that cowpox can be passed from person to person as well as from cow to person. The next step was to see if the cowpox would protect the patient from smallpox.

15
Edward Jenner Jenner published the data collected in 1798.
However, Jenner’s technique did not catch on as anticipated. After more and more people were becoming immune to smallpox vis a vis cowpox it became accepted as the way of the future. In 1840 variolation was forbidden by an Act of Parliament. In England vaccination with cowpox became compulsory in 1853.

16
Edward Jenner Jenner spent his time supplying cowpox material to others around the world. In recognition of his work the British government awarded Jenner ten thousand pounds in 1802, and twenty thousand pounds in 1807. Jenner was honored for his technique, and vaccine became the universally used term to indicate introducing material under the skin to produce a protection against disease.

17
Eradication In 1801 Jenner said, “The annihilation of the smallpox, the most dreadful scourge of the human species, must be the final result of this practice.” Compulsory vaccinations began in the following years: 1807 in Bavaria 1810 in Denmark 1835 in Prussia 1853 in Britain

18
Eradication Even after vaccination outbreaks still continued because the virus was imported by travelers where there were still endemics. Not until after WWI did most of Europe become smallpox free, and not until after WWII was transmission stopped throughout Europe and North America. In less developed countries smallpox continued largely unabated until the middle of the 20th century.

19
Eradication 1940s: large scale preparations of a stable freeze dried vaccine was perfected by Collier. 1950: Pan American Sanitary Organization decided to undertake a hemisphere wide eradication program. 1958: Union of Soviet Socialist Republics proposed to the WHO that a global smallpox eradication program be undertaken.

20
Eradication The campaign was based on a two fold strategy.
1) Mass vaccination campaigns in each country using a vaccine of ensured potency and stability that would reach at least 80% of the population. 2)Development of a system to detect and contain cases and outbreaks.
 Mass vaccination campaigns in each country using a vaccine of ensured potency and stability that would reach at least 80% of the population. 2)Development of a system to detect and contain cases and outbreaks.")
21
Eradication 26 October 1977 the last naturally occurring case of smallpox was recorded in Merka Somalia. In 1978 two cases were reported. These were both from people working in labs with smallpox in England.

22
Eradication 1980: WHO formally declared that smallpox was dead.
The eradication of smallpox was one of the most important branches of modern medicine. Jenner has been acknowledged as the father of immunology,

23
TAXONOMY FAMILY: POXVIRIDAE
SUBFAMILY: CHORDOPOXVIRINAE (infect vertebrates) GENERA: ORTHOPOXVIRUS (variola, vaccinia, cowpox, monkeypox) AVIPOXVIRUS (fowlpox) CAPRIPOXVIRUS (sheep-pox) LEPORIPOXVIRUS (myxoma) PARAPOXVIRUS (milker’s nodule) SULPOXVIRUS (swinepox) 2. SUBFAMILY: ENTOMOPOXVIRINAE (infect arthropods)
 GENERA: ORTHOPOXVIRUS (variola, vaccinia, cowpox, monkeypox) AVIPOXVIRUS (fowlpox) CAPRIPOXVIRUS (sheep-pox) LEPORIPOXVIRUS (myxoma) PARAPOXVIRUS (milker’s nodule) SULPOXVIRUS (swinepox) 2. SUBFAMILY: ENTOMOPOXVIRINAE (infect arthropods)")
24
Variola is the only one that affects only humans
Species of the Genus Orthopoxvirus Species Animals Infected Host Range Geographic Range Variola Human Narrow Formerly worldwide Vaccinia Human,a cow, pig, buffalo, rabbit, etc. Broad Worldwideb Cowpox Rodent,a cow, human, cat, etc. Europe Monkeypox Squirrel,a monkey, ape, human Western and central Africa Ectromelia Mouse, mole Camelpox Camel Africa and Asia Taterapox Gerbil Western Africa Volepox Vole ? United States Raccoonpox Raccoon Skunkpox Skunk Uasin Gishu Horse Medium Eastern Africa aPrimary host. bSecondary to vaccination; no known natural host. Variola is the only one that affects only humans

25
CHARACTERISTICS SHARED BY SPECIES OF ORTHOPOXVIRUS :
- The largest and most complex viruses Virons particles can be seen with a light microscope - They contain a linear genome of a single double-stranded DNA They replicate in the cytoplasm of the host cell, therefore they must provide their own mRNA and DNA synthetic machinery (including DNA-dependent RNA polymerase) - Inclucison bodies: type B and type A Virions have a brick-like shape and are present in 2 forms, both are infectious: 1. EEV (Extracellular Enveloped Virus) 2. IMV (Intracellular Mature Virus) Serological cross-reactivity - Produce a hemagglutininin antigen (HA) - Vaccinia is the most intensively studied member of the poxvirus family DNA dependent RNA polymerase transcribes mRNA from the viral DNA About vaccinia “Smallpox and its eradication” pg.74; antigens pg75
 - Inclucison bodies: type B and type A. Virions have a brick-like shape and are present in. 2 forms, both are infectious: 1. EEV (Extracellular Enveloped Virus) 2. IMV (Intracellular Mature Virus) Serological cross-reactivity. - Produce a hemagglutininin antigen (HA) - Vaccinia is the most intensively studied member of. the poxvirus family. DNA dependent RNA polymerase transcribes mRNA from the viral DNA. About vaccinia Smallpox and its eradication pg.74; antigens pg75.")
26
Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO

27
Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO

28
MORPHOLOGY OF THE VIRION
- have an brick-like shape; dimensions 400x200nm - four major elements: 1. core ( 9 nm thick membrane, biconcave disk, a tightly compressed nucleoprotein) 2. lateral bodies ( unknown function) 3. outer membrane ( a protein shell 12nm thick, the surface consists of irregularly arranged tubules) 4. envelope ( an inconstant element, proteins are glycosylated and acylated) - Virons are present in two infectious forms: 1. EEV (Extracellular Enveloped Virus)- released from cells spontaneously, by exocytoses are enclosed within a lipoprotein envelope, which contains the haemagglutinin and other specific polypeptides - CEV (Cell Associated Enveloped Virus) 2. IMV (Intracellular Mature Virus) – released by cellular disruption, lacks envelope, “naked virus” Core- nucleoprotein, is maintained in a superhelical configuration , and appears to occur in globuar structures interconnected by DNA-protein fibres , resembling the nucleosome structures of eukaryotic chromatin
 2. lateral bodies ( unknown function) 3. outer membrane ( a protein shell 12nm thick, the surface consists of irregularly arranged tubules) 4. envelope ( an inconstant element, proteins are glycosylated and acylated) - Virons are present in two infectious forms: 1. EEV (Extracellular Enveloped Virus)- released from. cells spontaneously, by exocytoses are enclosed within. a lipoprotein envelope, which contains the haemagglutinin. and other specific polypeptides. - CEV (Cell Associated Enveloped Virus) 2. IMV (Intracellular Mature Virus) – released by. cellular disruption, lacks envelope, naked virus Core- nucleoprotein, is maintained in a superhelical configuration , and appears to occur in globuar structures interconnected by DNA-protein fibres , resembling the nucleosome structures of eukaryotic chromatin.")
29
Vaccinia Virus – Electron micrographs
A. Non- enveloped virion (surface of outer membrane with tubular elements) C. Thin section of non-enveloped virion (biconcave core) B. Enveloped virion, found in extracellular medium D. Viral core, released after treatment of virions with Nonidet Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
 C. Thin section of non-enveloped virion (biconcave core) B. Enveloped virion, found in extracellular medium. D. Viral core, released after treatment of virions with Nonidet. Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460.")
30
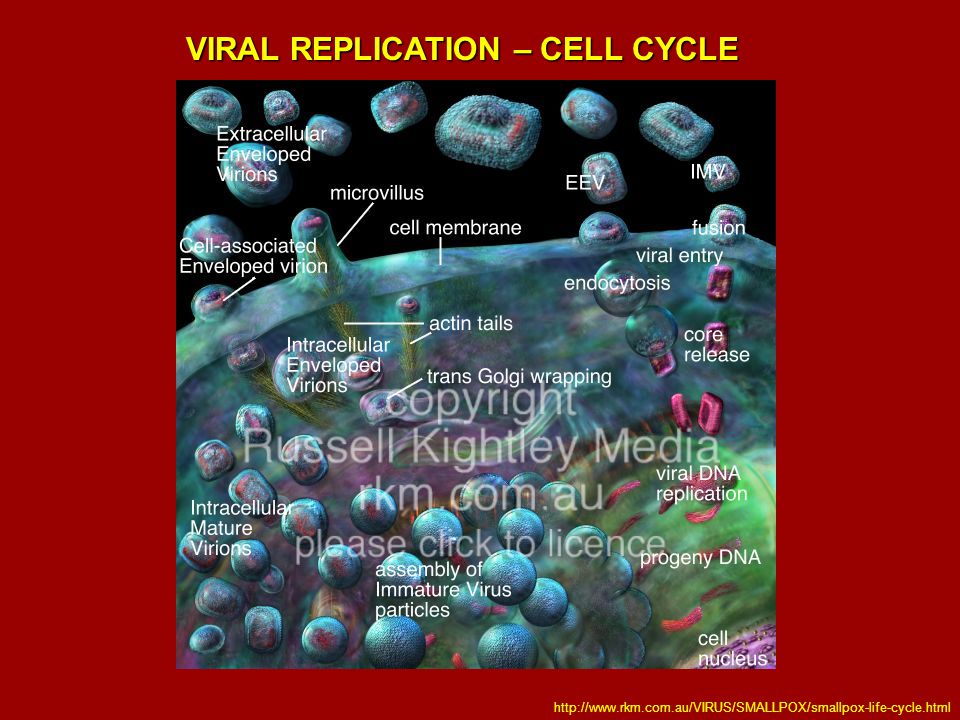
VIRAL REPLICATION – CELL CYCLE
Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460

31
VIRAL REPLICATION – CELL CYCLE
32
CELLULAR CHANGES “Viral factory” visualized in stained cells as
the B-type inclusion body, is first seen at 2.5h cupules first appear at 4 hours and some are completed as immature particles 6-8hours. From 8 hours onwards mature particles appear. “Toxic”changes may occur in the inf.cells, which in monolayer cultures become rounded and retract from each other. Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460

33
Cytoplasmic inclusion bodies in infected cells
B-type (Guarnieri bodies)- sites of viral replication produced by all orhopoxviruses A-type – strongly eosinophilic, found in cells infected with: cowpox,ectromelia and raccoonpox virus; appear late in the infection and are not associated with viral replication (may contain mature virions) Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460
- sites of viral replication. produced by all orhopoxviruses. A-type – strongly eosinophilic, found in cells infected with: cowpox,ectromelia and. raccoonpox virus; appear late in the infection and are not associated with. viral replication (may contain mature virions) Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460.")
34
STRUCTURE OF THE VIRAL GENOME
- Contains a single linear molecule of a double stranded DNA About 200 kbp long; guanine+cytosine content 36% - when denatured the two sister strands form a large single-stranded circular molecule, being attached at each end of the genome by covalent links - for the most part, the DNA sequences in the central part of the genome are unique, but the terminal fragments (inverted terminal repeats) cross-hybridize with each other and with the termini of other species of orthopoxvirus - Schemat of vaccinia virus DNA - The ITR’s include: an A+T-rich, incompletely base-paired, hairpin loop that connects the two DNA strands; set of short tandemly repeated sequences. The ITR’s are variable in length owing to deletions, repetitions, and transpositions Vaccinia is 191kbp; variola is 186kbp ITR resemble eukaryotic telomere - Inverted repeats in vaccinia are 10 kbp long in variola are 725 bp - Variola vs. Vaccinia: genomes are highly conserved with >95% nucleotide identity, however towards the termini the sequences diverge Poxviruses that have been inactivated that don’t damage their DNA can be reactivated
 cross-hybridize with each other. and with the termini of other species of orthopoxvirus. - Schemat of vaccinia virus DNA. - The ITR’s include: an A+T-rich, incompletely base-paired, hairpin loop that connects the. two DNA strands; set of short tandemly repeated sequences. The ITR’s are variable in. length owing to deletions, repetitions, and transpositions. Vaccinia is 191kbp; variola is 186kbp. ITR resemble eukaryotic telomere. - Inverted repeats in vaccinia are 10 kbp long. in variola are 725 bp. - Variola vs. Vaccinia: genomes are highly conserved with >95% nucleotide identity, however towards the termini the sequences diverge. Poxviruses that have been inactivated that don’t damage their DNA. can be reactivated.")
35
VIRAL PROTEINS Encodes about 200 proteins
The central part of the genome encodes for structural and functional proteins; Virulence genes are found near the inverted repeats, -numerous virus-encoded enzymes,are packaged within the virus core, including: * multisubunit DNA-dependent RNA polymerase * RNA polymerase associated protein of 94kd (RAP94) * a transcription factor (VETF) * capping and methylating enzymes * poly(A) polymerase These components are used to synthesize translatable mRNA -Importatnt proteins for replication: * topoisomerase * thymidine kinase – allows the incorporation of Thymidine into DNA * thymidylate kinase – catalyzes the reversible phosphorylotransfer between ATP and TMP * ribonuceoside reductase – converts ribonucleoside diphosphates ( NDP’s ) into deoxyNDP’s * dUTPase – minimize the misincorporation of Uracil into DNA * Uracil-DNA gylclosylase – removes the RNA base (Uracil) from DNA * DNA ligase When RNApolymerase inactivated no replication and virus cannot replicate mRNA for early genes
 * a transcription factor (VETF) * capping and methylating enzymes. * poly(A) polymerase. These components are used to synthesize translatable mRNA. -Importatnt proteins for replication: * topoisomerase. * thymidine kinase – allows the incorporation of Thymidine into DNA. * thymidylate kinase – catalyzes the reversible phosphorylotransfer between ATP and TMP. * ribonuceoside reductase – converts ribonucleoside diphosphates ( NDP’s ) into deoxyNDP’s. * dUTPase – minimize the misincorporation of Uracil into DNA. * Uracil-DNA gylclosylase – removes the RNA base (Uracil) from DNA. * DNA ligase. When RNApolymerase inactivated no replication and virus cannot replicate. mRNA for early genes.")
36
non enzymatic -VIRAL PROTEINS
Membrane proteins: A33R, A34R, A36R :*N-glycosylated, phosphorylated * fromation of actin tail and microvilli, which facilitate viral dissemination A36R : required for kinesin recruitment and is involved in microtubule-based motility of IEV’s A56R: Hemagglutinin, N- and O- glycosylated , promote cell fusion and cell to cell viral spread A27L: required for the formation of IEV, fusion protein, microtubule –dependent movment, normal sized plaques , has additional role in the viral assembly A28L: fusion protein; A28 deficient virions with normal amounts of A27 and A17 (binding partner) are unable to induce cell fusion 2. Core proteins: F17R, L4R, A3L, A10L : account for ~70% of the viral core by weight, bind DNA A36R- is thought to create a link between the actin and microtubule cytoskeleton (nature cell biol, vol3, nov2001 pg ) A28 protein not required for virion assembly, intracellular movment wrapping or exit form the cell
 are unable to induce cell fusion. 2. Core proteins: F17R, L4R, A3L, A10L : account for ~70% of the viral core by weight, bind DNA. A36R- is thought to create a link between the actin and microtubule cytoskeleton (nature cell biol, vol3, nov2001 pg ) A28 protein not required for virion assembly, intracellular movment wrapping or exit form the cell.")
37
VIRAL IMMUNOMODULATORY STRATEGIES
Poxviruses encode multiple classes of immunomodulatory proteins to inhibit diverse processes as: * apoptosis * the production of interferon * the production of chemokines and inflammatory cytokines * the activity of complement, NK, CTL’s, antibodies 2. The inhibitory proteins, produced by virus, fall into three main classes: - Virokines * resemble host cytokines * secreted from infected cells to block hosts receptors * vIL-10, vIL-18 - Viroreceptors * mimic host cellular receptors * altered cellular receptors that have lost their transmembrane sequnces and consequently are secreted from infected cells to sequester ligands * vINF-Rs, vTNFRs - Intracellular proteins * target host signal transduction pathways * inhibit inner antiviral pathways: apoptosis – vFLIP’s, serpins proinflammatory cascades - TNF The “holy grail” of virus infection is the generation of new progeny virions that can disseminate with minimal interference from the host’s defence Apoptosis –proteins that function either as ap inhibitors or serve as suicide caspase substrates

38
VIRAL IMMUNOMODULATORY PROTEINS
j Johnston,J.B.et al.Poxvirus Immunomodulatory Strategis:Current Perspectives. Journal of Virology (2003), 77: p
, 77: p")
39
VIRAL IMMUNOMODULATORY PROTEINS
Complement Regulatory Proteins - VCP – Vaccinia virus Complement control Protein, consists of short consensus repeats found in hosts’ complement regulatory proteins. Inhibits the classic and alternative pathways of complement through binding and inactivating both C4b and C3b SPICE- the smallpox inhibitor of complement enzymes molecularly engineered homologue of VCP (Rosengrad et al;.Univ. of Penn.) Demostrated: the functional advantage of variola complement regulatory protein Over the vaccinia homologue - More human complement specific than VCP 100-fold more potent at inactivating C4b&C3b; SPICE serves to inhibit the formation of the C3/C5 convertases necessary for Complement-mediated viral clearance Due to the nature of variola, the virus that causes smallpox, researchers cannot access the virus conventionally. Therefore, using previously published data on the DNA of smallpox, Penn researchers reverse-engineered a variola protein from vaccinia, a related virus used to vaccinate against smallpox. Their findings are presented in the May 28th edition of the Proceedings of the National Academy of Sciences and suggest new means to develop safer vaccines and potential therapies for smallpox. Due to the nature of variola, the virus that causes smallpox, researchers cannot access the virus conventionally. Therefore, using previously published data on the DNA of smallpox, Penn researchers reverse-engineered a variola protein from vaccinia, a related virus used to vaccinate against smallpox. Their findings are presented in the May 28th edition of the Proceedings of the National Academy of Sciences and suggest new means to develop safer vaccines and potential therapies for smallpox. Because authentic variola proteins are not available ofr study, Rosengard et al. moleculary engineered and characterized SPICE SPICE- provides the first evidence that variola proteins are particulary adept at overcoming human immunity, and the decreased function of VCP suggests one reason why the vaccinia virus vaccine was associated with relatively low mortality. Disabling SPICE may be useful therapeuticaly
 Demostrated: the functional advantage of variola complement regulatory protein. Over the vaccinia homologue. - More human complement specific than VCP. 100-fold more potent at inactivating C4b&C3b; SPICE serves to inhibit the formation of the C3/C5 convertases necessary for. Complement-mediated viral clearance. Due to the nature of variola, the virus that causes smallpox, researchers cannot access the virus conventionally. Therefore, using previously published data on the DNA of smallpox, Penn researchers reverse-engineered a variola protein from vaccinia, a related virus used to vaccinate against smallpox. Their findings are presented in the May 28th edition of the Proceedings of the National Academy of Sciences and suggest new means to develop safer vaccines and potential therapies for smallpox. Due to the nature of variola, the virus that causes smallpox, researchers cannot access the virus conventionally. Therefore, using previously published data on the DNA of smallpox, Penn researchers reverse-engineered a variola protein from vaccinia, a related virus used to vaccinate against smallpox. Their findings are presented in the May 28th edition of the Proceedings of the National Academy of Sciences and suggest new means to develop safer vaccines and potential therapies for smallpox. Because authentic variola proteins are not available ofr study, Rosengard et al. moleculary engineered and characterized SPICE. SPICE- provides the first evidence that variola proteins are particulary adept at. overcoming human immunity, and the decreased function of VCP suggests one. reason why the vaccinia virus vaccine was associated with relatively low mortality. Disabling SPICE may be useful therapeuticaly.")
40
Clinical Presentations, Transmission, Treatment, Vaccination
Smallpox Clinical Presentations, Transmission, Treatment, Vaccination

41
Transmission of Smallpox
Humans are the only natural host of smallpox and it is not known to be transmitted by insects or animals (no animal reservoir) Transmission generally occurs from direct and fairly prolonged face-to-face contact (in order for infected spit particles to pass from one person to another) Infected aerosols and air droplets spread in face-to-face contact with an infected person after fever has begun, esp. if symptoms include coughing Smallpox can also be spread through direct contact with infected bodily fluids or contaminated objects (ie. Bedding and clothing) In rare instances, smallpox can spread through the air of an enclosed area Variola major renders infected people bedridden so spreading to the community is reduced In variola minor, however, the symptoms are so mild that patients remain ambulatory during the infection phase and can spread the virus more widely
 Transmission generally occurs from direct and fairly prolonged face-to-face contact (in order for infected spit particles to pass from one person to another) Infected aerosols and air droplets spread in face-to-face contact with an infected person after fever has begun, esp. if symptoms include coughing. Smallpox can also be spread through direct contact with infected bodily fluids or contaminated objects (ie. Bedding and clothing) In rare instances, smallpox can spread through the air of an enclosed area. Variola major renders infected people bedridden so spreading to the community is reduced. In variola minor, however, the symptoms are so mild that patients remain ambulatory during the infection phase and can spread the virus more widely.")
42
Pathogenesis of Smallpox
The portal of entry for smallpox is the respiratory tract or inoculation on the skin Excretions from the mouth and nose, rather than scabs, are the most important source of infectious virus Studies have shown that primary infection in the nose or mouth do not produce a “primary lesion” that ulcerates and releases virions onto the surface Four models have been studied to learn about the spread of the infection through the body: mousepox in mice, rabbitpox in rabbits, and monkeypox and smallpox in monkeys and apes During incubation the virus proceeds through infection, replication, and liberation (usually accompanied by cell necrosis) first at the site of inoculation and then to the regional lymph nodes, then deeper lymph nodes and possibly into the bloodstream
 first at the site of inoculation and then to the regional lymph nodes, then deeper lymph nodes and possibly into the bloodstream.")
43
Pathogenesis of Smallpox
When tests were performed on humans to determine the pathogenesis, the virus was only rarely collected from the serum of infected persons, even though viraemia had definitely occurred Therefore it was determined that viraemia in ordinary smallpox was restricted to the pre-eruptive and early eruptive stages of the disease In hemorrhagic smallpox, however, virus was readily found in the blood and titers were high; thus hemorrhagic smallpox can be associated with overwhelming infection and the continued release of virus into the bloodstream The primary event for production of lesions of the rash in orthopoxvirus infections is localization (in the small blood vessels of the dermis) of virus particles that circulate in the bloodstream Vasodilation leads to greater density of lesions
 of virus particles that circulate in the bloodstream. Vasodilation leads to greater density of lesions.")
44
Pathogenesis of Smallpox
After introduction of smallpox into the oropharyngeal cavities it spreads to the regional lymph nodes Asymptomatic viremia occurs on the 3rd or 4th day after infection, with further dissemination of the virus to spleen, bone marrow, and other lymph nodes. The virus localizes in small blood vessels of the dermis and oropharyngeal mucosa, leading to initial onset of the enanthem and exanthem, at which point (about day 14) the patient becomes infectious The spleen, lymph nodes, kidneys, liver, bone marrow, and other viscera also may contain large amounts of virus Secondary viremia occurs by the 8th to 12th day after initial infection; this is followed by onset of fever and toxemia. Smallpox is disseminated through the body in the lymph and bloodstream as cell-associated particles Enveloped forms of the virus are more important than non-enveloped in the dissemination of the virions over a distance
 the patient becomes infectious. The spleen, lymph nodes, kidneys, liver, bone marrow, and other viscera also may contain large amounts of virus. Secondary viremia occurs by the 8th to 12th day after initial infection; this is followed by onset of fever and toxemia. Smallpox is disseminated through the body in the lymph and bloodstream as cell-associated particles. Enveloped forms of the virus are more important than non-enveloped in the dissemination of the virions over a distance.")
45
Pathogenesis of Smallpox
The development and evolution of skin lesions is an extremely valuable clue to the diagnosis and involves the following steps: Dilatation of the capillaries in the papillary layer of the dermis occurs initially, followed by swelling of the endothelial cells in the vessel walls; perivascular cuffing with lymphocytes, plasma cells, and macrophages can be seen. Lesions then develop in the epidermis, where the cells become swollen and vacuolated; characteristic B-type inclusion bodies can be found in the cytoplasm. The cells increase in size and the cell membranes rupture, leading to vesicular lesions. Pustulation results from the migration of polymorphonuclear cells into the vesicle. The contents of the pustule gradually become desiccated, leading to crusting or scabbing of the lesions. Re-epithilialization and scarring occur as the lesions heal.

46
Effects on Other Organs
A striking feature of smallpox reports is that there is an absence of specific lesions anywhere except in the skin and mucous membranes The endothelial cells lining the sinusoids of liver were often swollen and occasionally proliferating or necrotic (in more severe cases) Reticulum cell hyperplasia occurred in bone marrow and spleen Spleen was usually engorged with very numerous large lymphoid cells
 Reticulum cell hyperplasia occurred in bone marrow and spleen. Spleen was usually engorged with very numerous large lymphoid cells.")
47
Pathogenesis of Smallpox
When studies were done on rabbits with rabbitpox to determine the cause of death the rabbits had extreme hypertension, leading to a shock-like syndrome, decreased urinary output and a rise in blood-urea and plasma potassium levels Death seemed to be caused by lethal concentrations of potassium ion, which was possibly from the hypertension

48
Clinical Presentations
Smallpox is also called Variola 4 orthopoxviruses are known to infect humans: variola, vaccinia, cowpox, and monkeypox Variola virus is strictly a human virus, although primates and other animals can be infected under lab conditions Infection begins when the virus comes into contact with oropharyngeal (mouth and throat) or respiratory mucosa; virus multiplication then occurs in regional lymph nodes There are 2 clinical forms of Smallpox: Variola Major and Variola Minor Variola major is severe and the most common form with more extensive rash and higher fever with a death rate of about 30% Variola minor has less common presentation and much less severe with death rate of 1% or less
 or respiratory mucosa; virus multiplication then occurs in regional lymph nodes. There are 2 clinical forms of Smallpox: Variola Major and Variola Minor. Variola major is severe and the most common form with more extensive rash and higher fever with a death rate of about 30% Variola minor has less common presentation and much less severe with death rate of 1% or less.")
49
Variola Major has 4 clinical presentations based on the nature and evolution of the lesions; those 4 types are: Ordinary: most frequent (more than 90% of cases in both vaccinated and unvaccinated persons); corresponds to classical description of smallpox Modified: milder and may occur in previously vaccinated people; rarely fatal Flat and Hemorrhagic: very severe but uncommon
; corresponds to classical description of smallpox. Modified: milder and may occur in previously vaccinated people; rarely fatal. Flat and Hemorrhagic: very severe but uncommon.")
51
Stages of Smallpox Incubation Period Prodrome Phase
Lasts on average days but can range from 7-17 days Person is not contagious and exhibits no symptoms Prodrome Phase This is when initial symptoms develop and is also called the pre-eruptive stage Begins abruptly with fever, malaise, headache, head and body aches, prostration, and often nausea and vomiting Body Temperature rises to at least 101F and is often higher Note that this severe febrile prodrome right before the onset of the rash is characteristic of smallpox and can be used to differentiate it from other rash illnesses This phase lasts 2-4 days and is sometimes contagious

52
Stages of Smallpox: Rash Phase
When the first visible lesions appear the fever may start to go down This is the most contagious period (the time when the saliva has the most virus in it) Lasts 4 days Rash emerges as small red spots on tongue and in mouth (about 24 hours before the appearance of rash on the skin) Lesions in the mouth and pharynx enlarge and ulcerate quickly, releasing large amount of virus into the saliva These spots develop into sores that break open and spread large amounts of virus into mouth and throat The rash starts on the face as a few macules, known as herald spots, and spreads to the arms and the legs then to the hands and feet The rash usually spreads to all parts of the body in just 24 hours By the 3rd day of the rash the rash becomes raised bumps or papules By the 4th day the bumps become vesicular, fill with a thick, opaque fluid and often have depression in center that looks like a bellybutton (this umbilication is a major distinguishing characteristic of smallpox especially from chickenpox)
 Lasts 4 days. Rash emerges as small red spots on tongue and in mouth (about 24 hours before the appearance of rash on the skin) Lesions in the mouth and pharynx enlarge and ulcerate quickly, releasing large amount of virus into the saliva. These spots develop into sores that break open and spread large amounts of virus into mouth and throat. The rash starts on the face as a few macules, known as herald spots, and spreads to the arms and the legs then to the hands and feet. The rash usually spreads to all parts of the body in just 24 hours. By the 3rd day of the rash the rash becomes raised bumps or papules. By the 4th day the bumps become vesicular, fill with a thick, opaque fluid and often have depression in center that looks like a bellybutton (this umbilication is a major distinguishing characteristic of smallpox especially from chickenpox)")
53
Stages of Smallpox: Rash Phase
The fever will rise again at this time and remain high until scabs form over the bumps By the 6th or 7th day the lesions have become pustules: they are sharply raised, typically round, tense, firm to the touch (some describe them as feeling like BB’s under the skin) B/w 7 and 10 days the pustules mature and reach their max size, and the umbilications remain throughout the whole time Although lesions are dense around the nose and mouth, the majority of lesions are discrete (in some cases the lesions become confluent) At around 10 days of the rash the pustules begin to form a crust At about 14 days most of the lesions scab over and some begin to separate About 3 weeks after the onset scabs have separates and the site of each lesion is depigmented and eventually becomes pitted scars because of deeper skin layer involvement
 B/w 7 and 10 days the pustules mature and reach their max size, and the umbilications remain throughout the whole time. Although lesions are dense around the nose and mouth, the majority of lesions are discrete (in some cases the lesions become confluent) At around 10 days of the rash the pustules begin to form a crust. At about 14 days most of the lesions scab over and some begin to separate. About 3 weeks after the onset scabs have separates and the site of each lesion is depigmented and eventually becomes pitted scars because of deeper skin layer involvement.")
54
Stages of Smallpox: Rash Phase
The rash of smallpox has a centrifugal distribution, meaning it is most dense on the face, and more dense on the extremities than on the truck The palms of the hands and soles of the feet are involved in the majority of cases These characteristics are important in differentiating smallpox from other causes of rash illness Another differentiating characteristic of smallpox is that the lesions are all in the same stage of development on that part of the body (unlike chickenpox) these stages of development are: macules, papules, vesicles, and crusted lesions
 these stages of development are: macules, papules, vesicles, and crusted lesions.")
58
That was “ordinary” smallpox, now for the 3 other types
Modified: prodromal illness still occurs but is less severe than the ordinary type, usually a fever but not as high, skin lesions tend to evolve more quickly, are more superficial and may not show the uniform characteristic of more typical smallpox Flat (or malignant) smallpox: sever with a high fatality rate; in flat-type the lesions remain more or less flush with the skin and don’t become raised, accounted for 5-10% of cases in India, the prodrome symptoms are severe and last 3-4 days, fever remains elevated throughout the course of the illness and severe toxic symptoms, skin lesions progress very slowly; lesions contain very little fluid and are not umbilicated; the lesions are soft and velvety to the touch, most cases are fatal Hemorrhagic smallpox: sever and uncommon form of smallpox that is almost always fatal, involves extensive bleeding into the skin, mucous membranes and GI tract, in the large Indian series it occurred in 2% of cases, the prodrome has prolonged fever with little or no remission, intense headache, restlessness, extreme prostration and toxicity; death often occurs between the 5th and 7th day of illness when only a few maculopapular cutaneous lesions are present
 smallpox: sever with a high fatality rate; in flat-type the lesions remain more or less flush with the skin and don’t become raised, accounted for 5-10% of cases in India, the prodrome symptoms are severe and last 3-4 days, fever remains elevated throughout the course of the illness and severe toxic symptoms, skin lesions progress very slowly; lesions contain very little fluid and are not umbilicated; the lesions are soft and velvety to the touch, most cases are fatal. Hemorrhagic smallpox: sever and uncommon form of smallpox that is almost always fatal, involves extensive bleeding into the skin, mucous membranes and GI tract, in the large Indian series it occurred in 2% of cases, the prodrome has prolonged fever with little or no remission, intense headache, restlessness, extreme prostration and toxicity; death often occurs between the 5th and 7th day of illness when only a few maculopapular cutaneous lesions are present.")
59
When is a person contagious?
A person with smallpox is sometimes contagious with the onset of fever (the prodrome phase) but a person is most contagious with the onset of the rash Luckily, by the time a person gets the rash they are so sick they can’t likely move around the community An infected person is contagious until the last smallpox scab falls off
 but a person is most contagious with the onset of the rash. Luckily, by the time a person gets the rash they are so sick they can’t likely move around the community. An infected person is contagious until the last smallpox scab falls off.")
60
Clinical Diagnosis There are 3 major criteria for diagnosing if a rash is indeed smallpox: Prodrome that begins 1-4 days before rash onset and includes fever over 101F, and at least one of the following symptoms: prostrations, headache, backache, chills, vomiting, abdominal pains Presence of classic smallpox lesions: firm, round, deep-seated vesicles or pustules Lesions on the palms of the hands and/or soles of the feet There are 5 minor criteria looked at for diagnosis of smallpox: Lesions are centrifugal distribution First lesions appear on the oral mucosa, face, or forearms Patient appears toxic Rash has slow evolution, each stage lasting 1-2 days There are lesions on palms of the hands and/or soles of feet

62
Common conditions confused with Smallpox
Varicella (primary infection with varicella zoster virus) Disseminated herpes zoster Impetigo Drug eruptions Contact dermatitis Erythema multiforme minor Eyrthema multiforme (includes Steven Johnsons Syndrome) Enteroviral infection esp. Hand, foot and mouth disease Disseminated herpes simplex Scabies and insect bites Molluscum contagrosum
 Disseminated herpes zoster. Impetigo. Drug eruptions. Contact dermatitis. Erythema multiforme minor. Eyrthema multiforme (includes Steven Johnsons Syndrome) Enteroviral infection esp. Hand, foot and mouth disease. Disseminated herpes simplex. Scabies and insect bites. Molluscum contagrosum.")
64
Laboratory Diagnosis of Smallpox
Culture on Egg chorioallantoic membrane (CA): classical method; poxvirus grow on CA Direct examination of vesicle or pustular material: aggregations of virus may be seen in certain cytoplasm upon staining Tissue culture: growth in cultured cells EM: negative staining is used to visualize characteristic large brick shape of poxvirus Relatively rapid Can distinguish orthopox viruses from other viral agents Cannot differentiate between variola and vaccinia viruses May not be as sensitive as PCR-Based methods
: classical method; poxvirus grow on CA. Direct examination of vesicle or pustular material: aggregations of virus may be seen in certain cytoplasm upon staining. Tissue culture: growth in cultured cells. EM: negative staining is used to visualize characteristic large brick shape of poxvirus. Relatively rapid. Can distinguish orthopox viruses from other viral agents. Cannot differentiate between variola and vaccinia viruses. May not be as sensitive as PCR-Based methods.")
65
Laboratory Diagnosis of Smallpox
PCR Based method: In North America a positive test is considered diagnostic for vaccinia virus unless medical or epidemiologic evidence suggests otherwise With slight modifications to the fluorescently labeled probe, this assay can also be used to detect variola virus Family specific primers are used first, then subgroup-specific primers are used if the former is not successful in producing PCR product DNA Probes: Assays using immobilized oligonucleotides in a microarray have been developed to identify and discriminate among orthopoxviruses In situ hybridization of formalin-fixed tissues Serology: Classical methods such as complement fixation and gel precipitation commonly were used in the past; experimental enzyme-linked immunoassays are currently being evaluated Strain identification: A restriction fragment length polymorphism assay (RFLP) has been developed by CDC using polymorphisms found on 45 variola strains from 1939 to the 1970s
 has been developed by CDC using polymorphisms found on 45 variola strains from 1939 to the 1970s.")
66
Laboratory Diagnosis Lab diagnosis of smallpox is made by examination of material from a skin lesions For a patient who meets criteria for moderate risk, the most important laboratory procedure is rapid diagnostic testing for varicella zoster virus, or VZV Most common method for detecting VZV is direct fluorescent antibody, or DFA This method detects VZV directly in cells using anti-VZV antibody conjugated to fluorescein dye This technique is very sensitive and specific but is critically dependent on careful collection of material from lesion Electron microscopy, detection of VZV DNA by polymerase chain reaction testing of vesicular fluid or scabs, standard PCR, and cytology smears are other rapid methods for detections of VZV Ultimately, smallpox is a disease which can be easily diagnosed by trained health workers without the need for laboratory support

67
Outcomes of Infection:
Those who survive usually have scars If eye involvement then blindness could occur Recovery results in long lasting immunity to reinfection with variola virus; no evidence of chronic or recurrent infection with variola virus In fatal cases death usually occurs b/w the 10th and 16th days of illness The cause of death from smallpox is not exactly clear since the infection involves multiple organs; perhaps uncontrolled immune response as well as overwhelming viremia and soluble variola antigens

68
Treatment of Smallpox Vaccine is administered up to 4 days after exposure to the virus and before the rash appears, provides protective immunity and can prevent infection or ameliorate the severity of the disease There is really no effective treatment, other than the management of the symptoms Adequate fluid intake (difficult) Alleviation of pain and fever Keeping skin lesions clean to prevent bacterial infection Some compounds, such as Cidofovir, are under investigation as chemotherapeutic agents
 Alleviation of pain and fever. Keeping skin lesions clean to prevent bacterial infection. Some compounds, such as Cidofovir, are under investigation as chemotherapeutic agents.")
69
Vaccination In 1796, Edward Jenner demonstrated that immunity to smallpox could be produced by inoculating a human with material from a lesion on the udder of a cow (cowpox); Jenner called this material vaccine from vacca which is Latin for cow At some time during the nineteenth century, the virus used for smallpox ceased to be cowpox and was changed to vaccinia Vaccinia is in the same family has cowpox and smallpox but genetically different In the early 1950s (150 years after Jenner’s vaccination came out) an estimated 50 million cases of smallpox occurred in the world each year, which feel to around million by 1967 b/c of vaccination
; Jenner called this material vaccine from vacca which is Latin for cow. At some time during the nineteenth century, the virus used for smallpox ceased to be cowpox and was changed to vaccinia. Vaccinia is in the same family has cowpox and smallpox but genetically different. In the early 1950s (150 years after Jenner’s vaccination came out) an estimated 50 million cases of smallpox occurred in the world each year, which feel to around million by 1967 b/c of vaccination.")
70
Vaccination The smallpox vaccine is actual live vaccinia virus, unlike other vaccines which use dead virus; for this reason the vaccination site must be cared for to prevent spread Smallpox vaccine is administered using a bifurcated needle, not an injection, unlike any other vaccine The bifurcated needle is dipped into the vaccine and then used to prick the skin 15 times in about 3 seconds in a 5mm radius area It is administered into the superficial layer of the skin

73
Vaccination If vaccination is successful a red, itchy bump develops at the vaccine site in 3-4 days; this is caused by the vaccinia virus replicating in the basal cells of the epidermis producing a papule surrounded by erythema In the first week the bump becomes a blister, fills with pus, and begins to drain A person is considered protected with the development of a pustule like this at the vaccination site During the second week the blister begins to dry and a scab forms; the scab then falls off leaving a scar Most people experience the side effects of a sore arm, fever, and body aches and axillary lymphadenopathy (3-5 days after vaccination) 1st time vaccinators have a stronger reaction than those who are re-vaccinated Because the virus is live it can be spread to other parts of the body or to other people so great care must be given to the vaccination site to prevent this
 1st time vaccinators have a stronger reaction than those who are re-vaccinated. Because the virus is live it can be spread to other parts of the body or to other people so great care must be given to the vaccination site to prevent this.")
74
Vaccination The vaccine provides a high level of immunity for 3-5 years and decreasing immunity thereafter If a person is re-vaccinated the immunity lasts even longer Studies show that even 30 years after a vaccination, while a person may not be protected against smallpox they have a less severe disease The vaccine has been effective in preventing smallpox in 95% of people vaccinated Evidence for a brisk cell-mediated immune response has also been detected It is believed that healing of the vaccinia infection is associated with intact cell-mediated or T-cell and cytokine immune competence, and that viremia is defended by an intact antibody or B-cell immune competence If the vaccine is given in 1-2 days after exposure to smallpox it is effective in preventing smallpox or mitigating the symptoms of those who have been exposed The fatality rate among people vaccinated less than 10 years before exposure was 1.3%; it was 7% among those vaccinated years prior, and 11% among those vaccinated 20 or more years prior to infection; 52% of unvaccinated people died

75
Vaccination The antibodies induced by the vaccinia vaccine cross protect for other Orthopoxviruses (including monkeypox, cowpox, and smallpox) Three different smallpox vaccines are available (or will soon be) in the U.S. All 3 contain the New York City Board of Health strain of live vaccinia virus Dryvax is the currently licensed vaccine; it was produced by Wyeth Lederle in the early 1980s from calph lymph containing live vaccinia virus; the vaccine is provided as a freeze dried powder in a multi-dose vial Dryvax is produced by infecting a calf with vaccinia and then collecting the lymph from the virus filled pustules on the calf’s udder Dryvax contains the antibiotics polymyxin B, streptomycin, tetracycline and neomycin A second vaccine produced years ago by Aventis Pasteur would be available in the case of an emergency
 in the U.S. All 3 contain the New York City Board of Health strain of live vaccinia virus. Dryvax is the currently licensed vaccine; it was produced by Wyeth Lederle in the early 1980s from calph lymph containing live vaccinia virus; the vaccine is provided as a freeze dried powder in a multi-dose vial. Dryvax is produced by infecting a calf with vaccinia and then collecting the lymph from the virus filled pustules on the calf’s udder. Dryvax contains the antibiotics polymyxin B, streptomycin, tetracycline and neomycin. A second vaccine produced years ago by Aventis Pasteur would be available in the case of an emergency.")
76
Vaccination New smallpox vaccines also contain live New York City Board of Health vaccinia virus, but are produced using cell culture technology rather than live animals; these vaccines may also be distributed as a freeze dried powder but do not contain antibiotic In October 2002 Acambis-Baxter Laboratories began preparing Tissue culture cell vaccines The two types of cells being used to cultivate the vaccinia virus are: Vero monkey kidney cells, and human fibroblast cell line (MRC5) It is thought that these cell cultured vaccines will have less side-effects than the calph-lymph vaccine The other vaccines currently being developed: Modified vaccinia Ankara (MVA) vaccine, Japanese strain LC16m8 vaccine Current supply: there are 14.8 million doses of DryVax available and 85 million doses of the Aventis product, and when the Acambis vaccines are available there will be an additional 209 million doses available
 It is thought that these cell cultured vaccines will have less side-effects than the calph-lymph vaccine. The other vaccines currently being developed: Modified vaccinia Ankara (MVA) vaccine, Japanese strain LC16m8 vaccine. Current supply: there are 14.8 million doses of DryVax available and 85 million doses of the Aventis product, and when the Acambis vaccines are available there will be an additional 209 million doses available.")
77
Who Should Not Get the Vaccine?
The vaccine is contraindicated for: Persons who have experienced a serious allergic reaction to a prior dose of vaccine or to a vaccine component Persons with significant immunosuppression from any cause (HIV, transplant, receiving treatment for cancer) or anyone with an immunosuppressed person in their household Pregnant women and persons with a pregnant person in the household Breastfeeding women Children under 12 months; in fact the Advisory Committee on Immunization Practices (ACIP) advises against non-emergency vaccination in children under 18 Persons with any heart problems, stroke or transient ischemic attack, high blood pressure, high cholesterol, or diabetes Persons with any sort of skin condition Persons with inflammatory eye diseases requiring steroid therapy
 or anyone with an immunosuppressed person in their household. Pregnant women and persons with a pregnant person in the household. Breastfeeding women. Children under 12 months; in fact the Advisory Committee on Immunization Practices (ACIP) advises against non-emergency vaccination in children under 18. Persons with any heart problems, stroke or transient ischemic attack, high blood pressure, high cholesterol, or diabetes. Persons with any sort of skin condition. Persons with inflammatory eye diseases requiring steroid therapy.")
78
4 Main Complications of Vaccination
Ecxema vaccinatum Occurred in vaccinated persons or unvaccinated contacts who were suffering from or had a history of eczema An eruption occurred at the sites on the body that were at the time affected by eczema or had been Symptoms severe; eruptions became intensely inflamed Occurred in 74 persons with no deaths; 60 cases from contact with vaccinated persons with 1 death Progressive vaccinia (vaccinia necrosum) Occurred in persons who suffered from an immune deficiency or with humoral or immune globulin deficiencies Local lesion at the vaccination site failed to heal; all lesions spread progressively until the patient died, usu. 2-5 months later Occurred in 11 person, with 4 deaths Generalized vaccinia Occurred in otherwise healthy individuals Characterized by development, from 6-9 days after vaccination, of a generalized rash, sometimes covering whole body Prognosis good Occurred in 143 persons with no deaths Postvaccinial encephalitis Most serious complication Occurred in 2 forms: 1. seen in infants under 2 years old, had violent onset, characterized by convulsions 2. seen in children older than 2 years had abrupt onset, with fever, vomiting, headache, and malaise Fatality rate was about 35%, with death usually occurring within a week Occurred in 16 persons with 4 deaths Other complications: congenital vaccinia (infection of fetus), accidental implantation (autoinoculation of any disrupted skin), vaccinia keratitis (autoinoculation of the eye and prior eye disease) Finally, in the past 1000 for every 10 million people vaccinated for the first time experiences reaction that was serious but not life threatening; b.w people developed life threatening symptoms
 Occurred in persons who suffered from an immune deficiency or with humoral or immune globulin deficiencies. Local lesion at the vaccination site failed to heal; all lesions spread progressively until the patient died, usu. 2-5 months later. Occurred in 11 person, with 4 deaths. Generalized vaccinia. Occurred in otherwise healthy individuals. Characterized by development, from 6-9 days after vaccination, of a generalized rash, sometimes covering whole body. Prognosis good. Occurred in 143 persons with no deaths. Postvaccinial encephalitis. Most serious complication. Occurred in 2 forms: 1. seen in infants under 2 years old, had violent onset, characterized by convulsions 2. seen in children older than 2 years had abrupt onset, with fever, vomiting, headache, and malaise. Fatality rate was about 35%, with death usually occurring within a week. Occurred in 16 persons with 4 deaths. Other complications: congenital vaccinia (infection of fetus), accidental implantation (autoinoculation of any disrupted skin), vaccinia keratitis (autoinoculation of the eye and prior eye disease) Finally, in the past 1000 for every 10 million people vaccinated for the first time experiences reaction that was serious but not life threatening; b.w people developed life threatening symptoms.")
79
Eczema Vaccinia Progressive Vaccinia Generalized Vaccinia

80
Progressive Vaccinia Developed Erythema Multiforme 1 mo. After vaccine Secondary herpes infection Contact Vaccinia

81
Treatments for Complications from Vaccination
Vaccinia Immune Globulin (VIG) is a sterile solution of the immunoglubulin fraction of plasma from person who was vaccinated with smallpox vaccine VIG was produces in the 1960s and it contained a high titer of anti-vaccinia neutralizing antibody VIG has shown to work in the treatment of smallpox vaccine adverse reactions caused by continued replication of vaccinia virus, such as the above mentioned complications VIG is available from CDC under an investigational new drug protocol Cidofovir is an antiviral medication (not previously used in humans) used to treat vaccinia infection; it is considered a second line therapy for smallpox vaccine adverse reactions A new intravenous formulation of VIG is being produces to support treatment of adverse events that may result from smallpox vaccination VIG is not recommended for mild instances of inadvertent inoculation, mild generalized vaccinia, erythema multiform, post-vaccination encephalities, and isolated vaccinia keratitis
 is a sterile solution of the immunoglubulin fraction of plasma from person who was vaccinated with smallpox vaccine. VIG was produces in the 1960s and it contained a high titer of anti-vaccinia neutralizing antibody. VIG has shown to work in the treatment of smallpox vaccine adverse reactions caused by continued replication of vaccinia virus, such as the above mentioned complications. VIG is available from CDC under an investigational new drug protocol. Cidofovir is an antiviral medication (not previously used in humans) used to treat vaccinia infection; it is considered a second line therapy for smallpox vaccine adverse reactions. A new intravenous formulation of VIG is being produces to support treatment of adverse events that may result from smallpox vaccination. VIG is not recommended for mild instances of inadvertent inoculation, mild generalized vaccinia, erythema multiform, post-vaccination encephalities, and isolated vaccinia keratitis.")
82
Vaccinations Now Routine vaccination in the U.S ended in 1972 for children and 1976 for healthcare workers On December 13, 2002, President Bush announced the following US policy: Smallpox vaccinations are required for military personnel; according to the Department of Health and Human Services (DHHS), approximately 500,000 military personnel will be vaccinated. Smallpox vaccinations are recommended for smallpox response teams comprised of public health staff and healthcare workers likely to be involved in the initial care of any patients with smallpox. Smallpox vaccinations also are being offered to other healthcare workers and to first-responders (including police officers, firefighters, and emergency medical technicians). Smallpox vaccinations likely will be made available to the general public on a voluntary basis once large stockpiles of the vaccine are licensed. Small Response Teams: Department of Health and Human Services will work with state and local governments to form volunteer smallpox response teams who can provide critical services in the event of a smallpox outbreak
, approximately 500,000 military personnel will be vaccinated. Smallpox vaccinations are recommended for smallpox response teams comprised of public health staff and healthcare workers likely to be involved in the initial care of any patients with smallpox. Smallpox vaccinations also are being offered to other healthcare workers and to first-responders (including police officers, firefighters, and emergency medical technicians). Smallpox vaccinations likely will be made available to the general public on a voluntary basis once large stockpiles of the vaccine are licensed. Small Response Teams: Department of Health and Human Services will work with state and local governments to form volunteer smallpox response teams who can provide critical services in the event of a smallpox outbreak.")
84
Vaccinations Now On April 30, 2003, the President signed into law the Smallpox Emergency Personnel Protection Act of 2003 The law establishes a no-fault program to provide benefits and compensation to certain individuals (ie, healthcare workers and emergency responders) who are injured as a result of administration of smallpox vaccination or other smallpox countermeasures
 who are injured as a result of administration of smallpox vaccination or other smallpox countermeasures.")
85
Vaccinations Now In a report released in August 2003, the Institute of Medicine (IOM) Committee on Smallpox Vaccination Program Implementation made several recommendations regarding offering smallpox vaccination to the general public Specifically, the Committee recommended that CDC proceed by: Conducting brief quantitative surveys to determine public interest and desire for smallpox vaccine; these surveys should include public and private health agencies as well as the general public, in order to understand the potential scope of public interest. Determining the budgetary and other requirements that would meet the demand noted. Identifying, monitoring, and referring people to existing or planned smallpox vaccine clinical research trials or other well-structured clinical programs that meet the basic requirements of medical and public health ethics, including assurances for safety of vaccinees and their contacts, acceptable balance between risk and benefit, and acceptable distribution of scarce public health resources to meet all preparedness as well as other public health goals; The committee encourages CDC to consider utilizing a pilot program or some other means of evaluating the initial experiences with this effort.
 Committee on Smallpox Vaccination Program Implementation made several recommendations regarding offering smallpox vaccination to the general public. Specifically, the Committee recommended that CDC proceed by: Conducting brief quantitative surveys to determine public interest and desire for smallpox vaccine; these surveys should include public and private health agencies as well as the general public, in order to understand the potential scope of public interest. Determining the budgetary and other requirements that would meet the demand noted. Identifying, monitoring, and referring people to existing or planned smallpox vaccine clinical research trials or other well-structured clinical programs that meet the basic requirements of medical and public health ethics, including assurances for safety of vaccinees and their contacts, acceptable balance between risk and benefit, and acceptable distribution of scarce public health resources to meet all preparedness as well as other public health goals; The committee encourages CDC to consider utilizing a pilot program or some other means of evaluating the initial experiences with this effort.")
86
This approach is incorporated into the current CDC Smallpox Plan
During the smallpox eradication campaign (1970s) and during smallpox outbreaks in the past, a "ring vaccination" (used in 1967) strategy has been followed This approach is incorporated into the current CDC Smallpox Plan Ring vaccination essentially involves creating a circle of vaccinated persons around each case to interrupt the chain of transmission. The strategy involves the following steps: Rapid identification and isolation of all smallpox cases Identification and vaccination of contacts of smallpox cases Monitoring contacts for development of fever and isolating them if fever occurs Vaccination of household members of contacts if no contraindications to vaccination exist In addition to ring vaccination, rapid voluntary vaccination of a large population may be required to: Supplement priority surveillance and containment control strategies in areas with smallpox cases Reduce the "at-risk" population for additional intentional releases of smallpox virus if the probability of such occurrences is considered significant Address heightened public or political concerns regarding access to voluntary vaccination
 and during smallpox outbreaks in the past, a ring vaccination (used in 1967) strategy has been followed. This approach is incorporated into the current CDC Smallpox Plan. Ring vaccination essentially involves creating a circle of vaccinated persons around each case to interrupt the chain of transmission. The strategy involves the following steps: Rapid identification and isolation of all smallpox cases. Identification and vaccination of contacts of smallpox cases. Monitoring contacts for development of fever and isolating them if fever occurs. Vaccination of household members of contacts if no contraindications to vaccination exist. In addition to ring vaccination, rapid voluntary vaccination of a large population may be required to: Supplement priority surveillance and containment control strategies in areas with smallpox cases. Reduce the at-risk population for additional intentional releases of smallpox virus if the probability of such occurrences is considered significant. Address heightened public or political concerns regarding access to voluntary vaccination.")
87
Management of an Outbreak
Surveillance of smallpox infection is probably easier than for any other infectious disease because of the distinctive rash, which is wholly characteristic Containment involves efficient detection of cases and identification and vaccination of contacts Patients diagnosed with smallpox should be physically isolated All specimen collectors, care givers and attendants coming into close contact with patients should be vaccinated as soon as smallpox is diagnosed as the cause of an outbreak Medical care givers, attendants, and mortuary workers, even if vaccinated, should wear gloves, caps, gowns, and surgical masks Contaminated clothing and bedding, if not incinerated, should be autoclaved or washed in hot water containing bleach Fumigation of premises may be done with formaldehyde

88
Isolation Precautions
Airborne and Contact Precautions in addition to Standard Precautions should be implemented for patients with suspected smallpox. Airborne Precautions: Place the patient in a private room with negative air-pressure ventilation (minimum 6 air exchanges/hr). Use external air exhaust or high-efficiency particulate air (HEPA) filters if the air is recirculated. Keep the door to the room closed. Contact Precautions: Place the patient in a private room if available. If a private room is not available, place the patient in a room with a patient who has active infection with the same organism (ie, cohort patients with smallpox). Wear gloves when entering the room, change gloves after having contact with infectious material, remove gloves before leaving the room, and immediately wash hands using an antimicrobial agent. Wear a gown when entering the room if clothing will have significant patient contact; remove the gown before leaving the room. Move and transport the patient for essential purposes only. If transport is necessary, a mask should be placed on the patient. When possible, dedicate the use of noncritical patient-care equipment.
. Use external air exhaust or high-efficiency particulate air (HEPA) filters if the air is recirculated. Keep the door to the room closed. Contact Precautions: Place the patient in a private room if available. If a private room is not available, place the patient in a room with a patient who has active infection with the same organism (ie, cohort patients with smallpox). Wear gloves when entering the room, change gloves after having contact with infectious material, remove gloves before leaving the room, and immediately wash hands using an antimicrobial agent. Wear a gown when entering the room if clothing will have significant patient contact; remove the gown before leaving the room. Move and transport the patient for essential purposes only. If transport is necessary, a mask should be placed on the patient. When possible, dedicate the use of noncritical patient-care equipment.")
89
Autopsy and Burial Procedures
According to WHO "Cadavers should be cremated, in a properly designed facility, whenever possible and all persons coming in contact with them should be vaccinated or at least placed on daily fever watch. Body bags treated with hypochlorite bleach can also be used." Consideration should be given to using sealed systems when burying patients who have died of smallpox. An example of the type of system that can be used to seal remains prior to placing them in a casket for burial is the BioSeal Facility System, produced by Barrier Products This system utilizes a poly-aluminum foil–extruded laminate material that when used with a heat sealer will provide Level 1 containment for all gases, fluids, vapors, and odors associated with the transport and storage of human and animal remains.

90
BIOTERRORISM The Center for Disease Control and Prevention (CDC) divided biological agents that are critical biothreat agents into 3 categories ( A, B,C ) based upon their risk for causing mass casualties in the event of bioterrorist atack. Variola ( smallpox) wass classified as a category A agent: * poses a risk to national security (it can be easily disseminated or transmitted person to person) * causes high mortality, with potential for major public health impact * might cause public panic and social disruption * demands special action for public health preparedness - Variola requires Lab. Biosafty Level 4
 based upon. their risk for causing mass casualties in the event of bioterrorist atack. Variola ( smallpox) wass classified as a category A agent: * poses a risk to national security (it can be easily disseminated or transmitted. person to person) * causes high mortality, with potential for major public health impact. * might cause public panic and social disruption. * demands special action for public health preparedness. - Variola requires Lab. Biosafty Level 4.")
91
BIOTERRORISM Smallpox is a disease that followed humanity for thousands of years until ~30 years ago. It was possible to eradicate smallpox, because an effective live vaccine from crossreacting virus – vaccinia was developed. The global vaccination program was financed and managed by the World Health Organization (WHO) and the official eradiction announcement was made in 1980. Over 20 years have passed since general vaccinations stopped and very few people are protected against the disease today. General vaccination, due to the number of complications that can be expected, is probably not possible with the present vaccines, except in an emergency. There is ongoing research in order to develop new vaccines. Let’s review some facts Tengell et al. Smallpox-eradicated, but growing terror threat. Clin Microbiol Infect (2002), 8:
 and the official eradiction announcement was made in Over 20 years have passed since general vaccinations stopped and very few people. are protected against the disease today. General vaccination, due to the number of complications that can be expected, is probably not possible with the present vaccines, except in an emergency. There is ongoing research in order to develop new vaccines. Let’s review some facts. Tengell et al. Smallpox-eradicated, but growing terror threat. Clin Microbiol Infect (2002), 8:")
92
BIOTERRORISM It was formerly thought that smallpox was not very suitable for biological warfare, because it was too infectious. An attack would entail a high risk of a worldwide epidemic, striking even the populations of the attackers. Terrorists generally lack the means for vaccinating large groups of people and have less opportunity to run large – scale virus cultures. Thus, it has been considered far more probable that they would prefer bacterial resource such as anthrax, which entails less risk of uncontrollable epidemics. Terrorist movement or the military command of a state could draw a conclusion that an attack with variola in the USA could allow the epidemic to remain local because of the expected vigorous countermeasures. If the risk of a worldwide epidemic seems small, an attack might be an attempt. Additionally, we have now seen that terrorist can be extremely fanatical. The attacks on September 11th, 2001 demonstrated the great ruthlessness and considerable resources of some terrorists. Atlas R.F. Bioterrorism: From Threat to Reality. Annu Rev.Microbiol.(2002)56:
56:")
93
BIOTERRORISM Why is variola virus considered an ideal bioterrorist weapon: It is highly transmissible by the aerosol route from infected to susceptible people; The civilian populations of most countries contain a high proportion of susceptible persons; Smallpox is associated with high morbidity and about 30% mortality; Initially, diagnosis of a disease that has not been seen for 20 years would be difficult; At present, other than the vaccine, which may be effective in the first few days post-infection, there is no proven drug treatment available for clinical smallpox; - It induces panic; Mahy,B.W.J. An overview on the use of a viral pathogen as a bioterrorism agent: why smallpox? (2003) Antiviral Research 57: 1-5
 Antiviral Research 57: 1-5.")
94
BIOTERRORISM Vaccinia virus, if released as an aerosol and not exposed to UV lights may persist for as long as 24 hours. It is belived that variola virus would exhibit similar properties. -Vaccinia virus, if released as an aerosol, is almost completely destroyed within 6 hours in an atmosphere of high temperature (31C – 33 C) and humidity (80%). In cooler temperatures (10 C- 11 C) and humidity (20%), nearly two thirds of a vaccinia aerosol survives for as long as 24 hours. It is belived that variola would behave similarly. Virus in scabs is more durable. At a temperature of 35 C and 65% humidity , the virus can persist for 3 weeks. At cooler temp. (26 C) the virus has survived for 8 weeks at high humidity and 12 weeks at a relative humidity less than 10% Dutch investigators demonstrated that it was possible to isolate variola virus from scabs that had been sitting on a shelf for 13 years. Vaccinia / Variola viruses are sensitive to disinfectants like hypochlorite (bleach) and ammonia – are effective for cleaning surfaces Other properties of the vaccinia virus Henderson,D.A. et al. Smallpox as Biological Weapon. (1999) JAMA, 281 :
 and. humidity (80%). In cooler temperatures (10 C- 11 C) and humidity (20%), nearly. two thirds of a vaccinia aerosol survives for as long as 24 hours. It is belived that. variola would behave similarly. Virus in scabs is more durable. At a temperature of 35 C and 65% humidity , the virus can persist for 3 weeks. At cooler temp. (26 C) the virus has survived. for 8 weeks at high humidity and 12 weeks at a relative humidity less than 10% Dutch investigators demonstrated that it was possible to isolate variola virus from. scabs that had been sitting on a shelf for 13 years. Vaccinia / Variola viruses are sensitive to disinfectants like hypochlorite (bleach) and ammonia – are effective for cleaning surfaces. Other properties of the vaccinia virus. Henderson,D.A. et al. Smallpox as Biological Weapon. (1999) JAMA, 281 :")
95
BIOTERRORISM Bill Patrick, a former bioweaponeer who worked at Fort Detrick, Md. , before the American offensive biological weapons program was dismanteled in 1969, says: - Bioweaponeers in the US program had begun weaponizing smallpox before the US biological weapons offensive effort was halted. “We made a beautiful powder for smallpox. We used chemical to protect it during dissemination and aerozolation” A gram of powdered virus ( equivalent of a quarter of a teaspoon of baking powder) would infect 100 people. Aerozolation is the most effective way to spread
 would infect 100 people. Aerozolation is the most effective way to spread.")
96
BIOTERRORISM There are only two official stocks of smallpox virus that are held: 1. USA: at CDC in Atlanta, Georgia 2. Russia: at Vector in Novosibirsk, Siberia (moved in 1984 from Moscow) Dr. Kenneth Alibek (formerly Kanatjan Alibekow), a native from Kazakhstan, medical doctor, and officer of the Red Army, he worked from 1975 to 1992 for the Soviet Biopreparat complex ( an ostensibly civilian pharmaceutical production association that was actually a top-secret branch of the Soviet biological weapons program). Dr.Alibek was the Chief Scientist and first deputy director of Biopreparat in He defected to the USA in 1992. The two locations: to continue antiviral research and also work on more efficient vaccines Vector – biotechnology institute
 Dr. Kenneth Alibek (formerly Kanatjan Alibekow), a native from Kazakhstan, medical doctor, and officer of the Red Army, he worked from 1975 to 1992 for the Soviet Biopreparat. complex ( an ostensibly civilian pharmaceutical production. association that was actually a top-secret branch of. the Soviet biological weapons program). Dr.Alibek was the Chief Scientist and first deputy director. of Biopreparat in He defected to the USA in The two locations: to continue antiviral research and also work on more efficient vaccines. Vector – biotechnology institute.")
97
BIOTERRORISM - His book ( with Stephen Handelman) Biohazard: The Chilling True Story of the Largest Covert Biological Weapons Program in the World (Random House 1999) describes his experience with Russian biological warfare (BW) activites. In 1998, Dr.Alibek visited the Center for Nonproliferation Studies in Monterey and met with the staff for the Chemi- Cal and Biological Weapons Nonproliferation Project (CBWNP). He was interviewed by Jonathan B. Tucker, CBWNP Director. Additionally he released a statement, where he discussed the BW situation in Russia in a great detail. 1.The Soviet Union had the most efficient, sophisticated, and powerful offensive BW programs in the world. It developed a completely new class of weapons based on genetically modified agents, eg. during the 1980’s they developed antibiotic-resistant strains of plague, anthrax, and tularemia. Also, Since his arrival to the USA Dr. Alibek gave many interviews in which he openly talked about the biological weapons in the former Soviet Union. Disscussed issues.
 describes his experience with Russian biological warfare (BW) activites. In 1998, Dr.Alibek visited the Center for Nonproliferation. Studies in Monterey and met with the staff for the Chemi- Cal and Biological Weapons Nonproliferation Project. (CBWNP). He was interviewed by Jonathan B. Tucker, CBWNP Director. Additionally he released a statement, where he discussed the BW situation in Russia in a. great detail. 1.The Soviet Union had the most efficient, sophisticated, and powerful offensive BW programs in the world. It. developed a completely new class of weapons based on. genetically modified agents, eg. during the 1980’s they. developed antibiotic-resistant strains of plague, anthrax, and tularemia. Also, Since his arrival to the USA Dr. Alibek gave many interviews in which he openly talked about the biological weapons in the former Soviet Union. Disscussed issues.")
98
BIOTERRORISM 2. Russia researched the genetic alteration of smallpox.
* “In 1990 and 1991, we engineered a smallpox at Vector. It was found that several areas of the smallpox genome can be used for the introduction of some foreign genetic material. The first development was smallpox and VEE. VEE, or Venezuelan equine encephalitis, is a brain virus. It causes a severe headache and near-coma, but it is generally not lethal. Alibek said that the researchers spliced VEE into smallpox . The result was a recombinant chimera virus: Veepox.” * More recently, Alibek claims, the Vector researchers may have created a recombinant Ebola-smallpox chimera. One could call it Ebolapox. ABC News - Dec. 3, by Brian Ross

99
BIOTERRORISM EBOLAPOX
*Ebola virus uses the molecule RNA for its genetic code, whereas smallpox uses DNA. Alibek believes that the Russian researchers made a DNA copy of the disease-causing parts of Ebola, then grafted them into smallpox. Alibek said he thinks that the Ebolapox virus is stable -- that is, that it will replicate successfully in a test tube or in animals – which means that, once created, Ebolapox will live forever in a laboratory, and will not uncreate itself. Thus a new form of life may have been brought into the world. *"The Ebolapox could produce the form of smallpox called blackpox," Alibek says. Blackpox, sometimes known as hemorrhagic smallpox, is the most severe type of smallpox disease. In a blackpox infection, the skin does not develop blisters. Instead, the skin becomes dark all over. Blood vessels leak, resulting in severe internal hemorrhaging. Blackpox is invariably fatal. "As a weapon, the Ebolapox would give the hemorrhages and high mortality rate of Ebola virus" Alibek said. ABC News - Dec. 3, by Brian Ross

100
BIOTERRORISM Mousepox
Mark Buller, a scientist, who is funded by the US government, deliberately created a deadly form of mousepox, which is closely related to the smallpox virus, through genetic engineering. Reason: to study what bioterrorists might do. Another team ,Ramshaw's team, continued research by adding a gene called IL-4 to the modified mousepox. He expected that doing this would boost antibody production, but instead, the new mousepox virus was far more lethal, killing 60 percent of vaccinated mice. Debora Mackenzie. US develops lethal new viruses.(2003) New Scientist Additionally, Alibek stated : * No dry smallpox weapon was developed, just one in a liquid form. * Some supplies of smallpox (also plague and anthrax) were manufactured, stored, and stockpiled. Immediately after receiving an order it would take just two or three days to transfer these agents from storage tanks into cluster bomblets and spray tanks. Each 500kg cluster bomb contained more than 100 bomblets. The bombs would be stored in the refrigerated bunkers until use. The Nonproliferation Review / Spring-Summer 1999 Storage: 2 refrigerates TR-50 (50kg) and TR-250 (250kg). Alibek’s comment on mousepox and other(rabbitpox) “The idea was that all research and development work would be conducted using these model viruses. Once we Obtain a set of positive results, it would take just two weeks to conduct the same manipulations with smallpox virus And to stockpile the warfare agent” (The nonproliferation Review)
 New Scientist. Additionally, Alibek stated : * No dry smallpox weapon was developed, just one in a liquid form. * Some supplies of smallpox (also plague and anthrax) were manufactured, stored, and stockpiled. Immediately after receiving an order it would take just. two or three days to transfer these agents from storage tanks into cluster. bomblets and spray tanks. Each 500kg cluster bomb contained more than 100. bomblets. The bombs would be stored in the refrigerated bunkers until use. The Nonproliferation Review / Spring-Summer Storage: 2 refrigerates TR-50 (50kg) and TR-250 (250kg). Alibek’s comment on mousepox and other(rabbitpox) The idea was that all research and development work would be conducted using these model viruses. Once we. Obtain a set of positive results, it would take just two weeks to conduct the same manipulations with smallpox virus. And to stockpile the warfare agent (The nonproliferation Review)")
101
BIOTERRORISM Q: What was the logic of developing an agent like smallpox, which is so contagious that it could create a huge pandemic? A: Unfortunately, it is a normal progression to develop more powerful weapons. Why, for example, did we develop a 100-megaton hydrogen bomb when both superpowers had 10-megaton and 20- megaton bombs? For the Soviet Union, the main doctrine was to use biological weapons in so – called total wars involving possible mutual destruction between the USA and the Soviet Union and their allies Given, however, the economic situation in the former Soviet Union, the incentive to sell equipment and knowledge suitable for biological weapons production without regard to their eventual use is great both for the government and for individual scientists and businessmen. The Russian government has long been short of funds, and its biotechnology arena has also been adversely affected. Many of its scientist are unemployed; those that are employed are paid poorly or not at all. Russian allies: Scientists traveling or moving abroad ( unconfirmed reports of visits to North Korea in early 90’) Scientists from other countries coming to Russia for training in biotechnology, microbiology, genetic engineering Techniques. For years Moscow State Univ. provided such training to scientist from: North Korea, Iran, Iraq, Syria, Libya, Eastern Block nations, Cuba The Nonproliferation Review / Spring-Summer 1999
 Scientists from other countries coming to Russia for training in biotechnology, microbiology, genetic engineering. Techniques. For years Moscow State Univ. provided such training to scientist from: North Korea, Iran, Iraq, Syria, Libya, Eastern Block nations, Cuba. The Nonproliferation Review / Spring-Summer")
102
BIOTERRORISM CDC plan and guidelines for containment and vaccination in the event of smallpox bioterrorist attack: The plan calls for isolation of confirmed or suspected smallpox patients to limit the potential exposure of nonimmune persons. Vaccinia vaccine would be recommended for persons who were exposed to the initial release of the virus: - Persons who had face-to-face, household, or close-proximity contact (~2m) with confirmed or suspected smallpox patients - Laboratory personnel involved in the collection or processing of clinical specimens from confirmed or suspected smallpox patients And other persons who have an increased likelihood of contact with infectious materials from a smallpox patient Atlas R.F. Bioterrorism: From Threat to Reality. Annu Rev.Microbiol.(2002)56:
 with. confirmed or suspected smallpox patients. - Laboratory personnel involved in the collection or processing of clinical specimens. from confirmed or suspected smallpox patients. And other persons who have an increased likelihood of contact with infectious. materials from a smallpox patient. Atlas R.F. Bioterrorism: From Threat to Reality. Annu Rev.Microbiol.(2002)56:")
Similar presentations




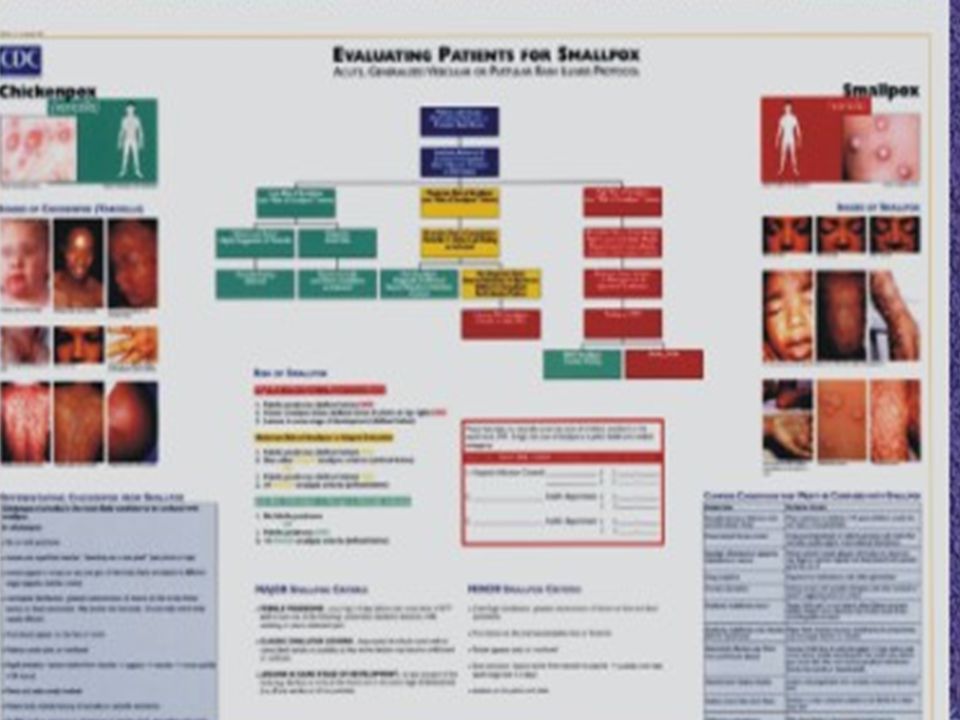
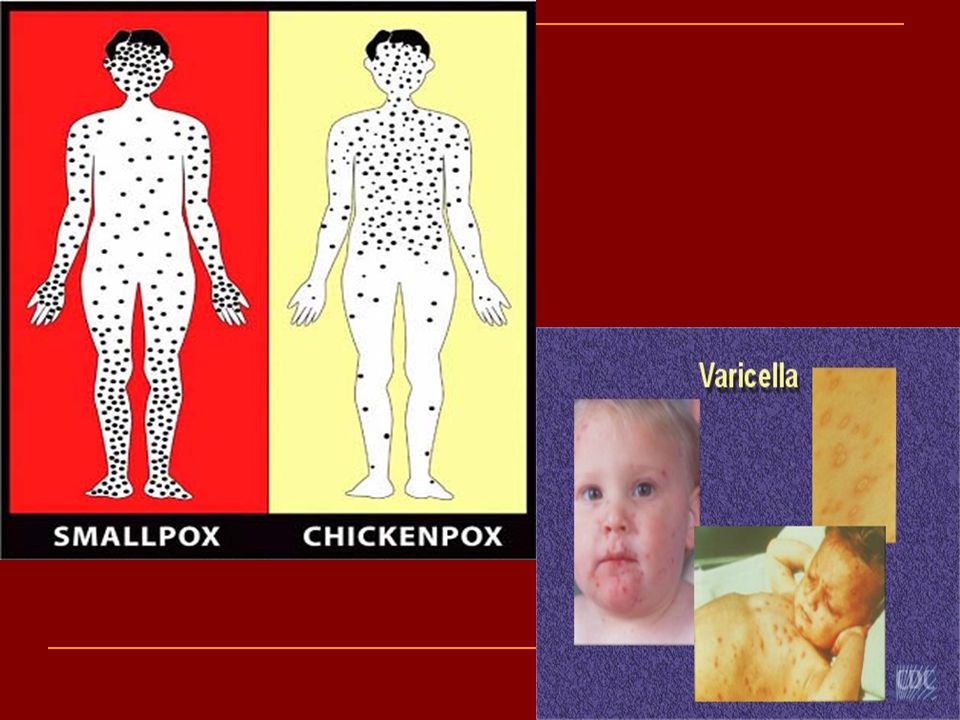






 is a severe, often-fatal disease in humans and nonhuman primates (monkeys,>")





 Management Presentation>")
 SC.912.L.14.52 Explain the basic functions of the human immune system, including specific and nonspecific immune response, vaccines,>")
. Viruses are made of genetic material (DNA or RNA) surrounded.>")



 is a respiratory disease of pigs caused by type A influenza virus.>")

 Virus>")
