Download presentation
Presentation is loading. Please wait.

1
Screening & brief alcohol interventions in primary care Dr Eileen Kaner Dr Paul Cassidy Professor Nick Heather Session 2 – Brief Alcohol Intervention

2
Linking screening to brief intervention Avoid labelling Start with reference to the patient’s screening score or consumption level Ask the patient how they feel about their screening score/consumption level –eg. You appear to be drinking at a rate that increases your risk of harm. What do you think? –eg. The way in which you are drinking may be affecting your health. What do you think?

3
Assessing interest/motivation Not all patients are the same Alcohol may not be at the top of their agenda

5
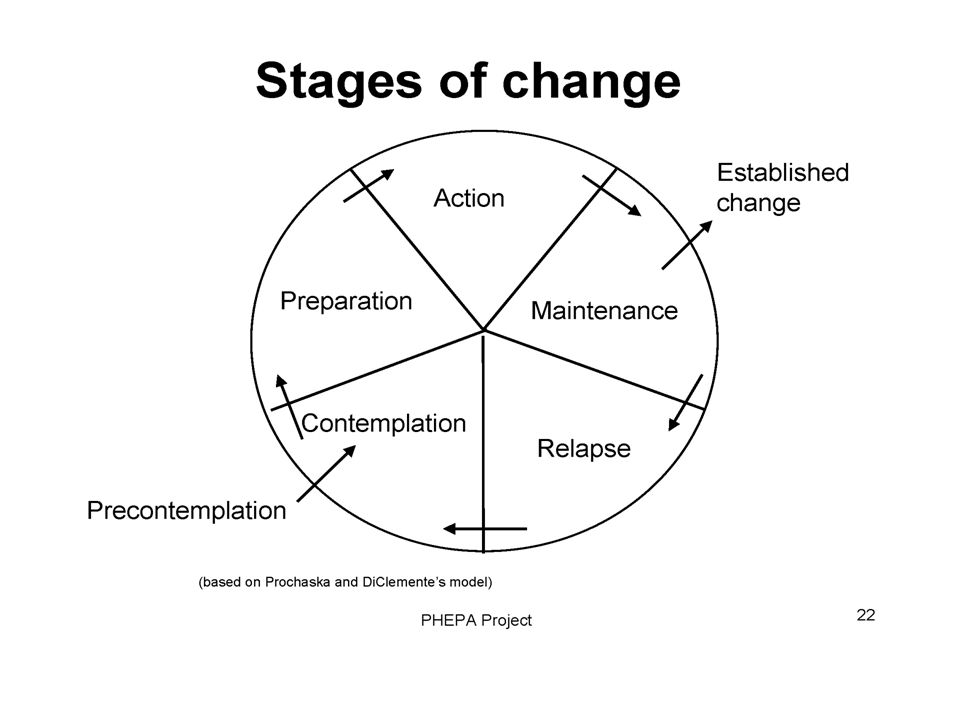
Stage of change & brief intervention Precontemplation (unaware/unready) intervention unlikely to succeed, give information about risks Contemplation (aware/ambivalent) offer advice &/or motivational work to move patient along Preparation (planning) set date, make plans, be specific, anticipate difficulties Action (ready to go) encourage, support, offer to follow-up Maintenance (keeping it up) reinforce success, advise on managing slips/relapse prevention
 intervention unlikely to succeed, give information about risks Contemplation (aware/ambivalent) offer advice &/or motivational work to move patient along Preparation (planning) set date, make plans, be specific, anticipate difficulties Action (ready to go) encourage, support, offer to follow-up Maintenance (keeping it up) reinforce success, advise on managing slips/relapse prevention")
6
Risk status & brief intervention Low Risk - Brief congratulation, positive reinforcement. Possibly ‘unit awareness’ work. Hazardous drinkers – Simple structured advice (level 1 BI), offer further support Harmful drinkers – Simple structured advice (level 1 BI) and offer motivational intervention (level 2 BI) Dependent drinking – Referral to specialist services
, offer further support Harmful drinkers – Simple structured advice (level 1 BI) and offer motivational intervention (level 2 BI) Dependent drinking – Referral to specialist services.")
7
Clinical flow Case finding Negative screen Congratulate Positive Screen Assess interest/motivation No interest – offer PIL Keep door open for future Interest/hazardous drinker Simple structured advice Interest/ harmful drinker Extended brief intervention Possible dependence Assess further, refer on

8
What generally happens now?

9
Example 1 - avoidance

10
Example 2 - evasion

11
Example 3 – dictating

12
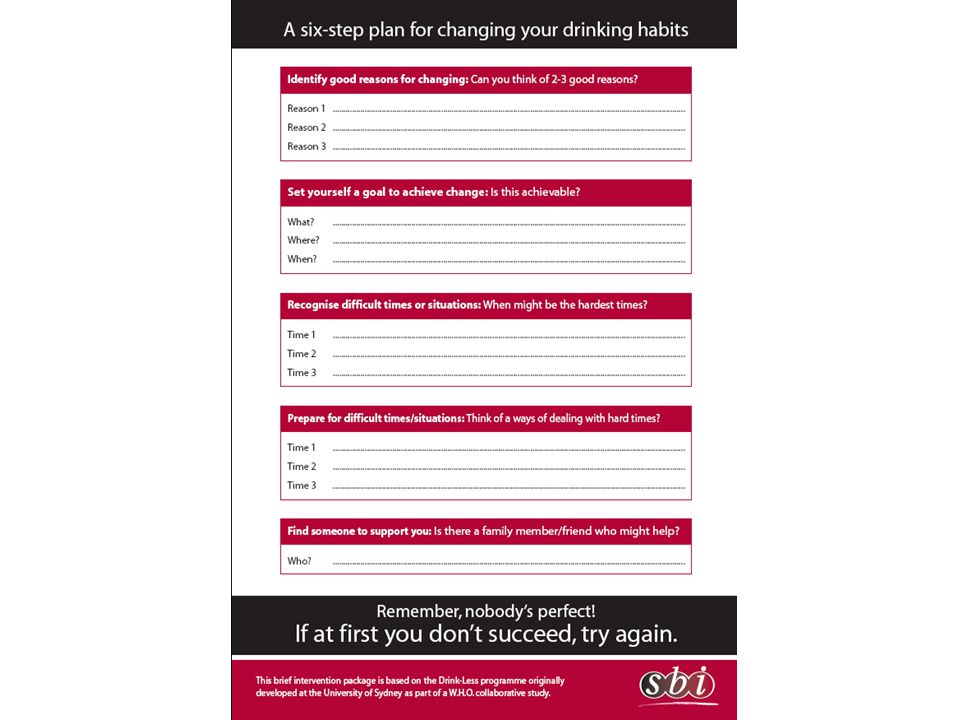
Level 1 brief intervention Simple structured advice Delivered in 1-2 minutes Following ‘How Much is Too Much’ protocol (level 1) Practical - ‘common sense’ content Offer of future follow-up/further discussion Clinicians already do many elements of BI –just needs some more structure
 Practical - ‘common sense’ content Offer of future follow-up/further discussion Clinicians already do many elements of BI –just needs some more structure")
13
BI structure – FRAMES Feedback (personalised) Responsibility (with patient) Advice (clear, practical) Menu (variety of options) Empathy (warm, reflective) Self-efficacy (boosts confidence)
 Responsibility (with patient) Advice (clear, practical) Menu (variety of options) Empathy (warm, reflective) Self-efficacy (boosts confidence)")
16
Discussion Issues to think about –What are the essential elements if time is short? –When, where and by whom? –What resources are required –What if patients want more than simple advice?

17
Level 2 brief intervention Motivationally enhanced intervention not MI Behaviour change counselling based on Rollnick S., et al. (1999) Health Behaviour Change: A Guide for Practitioners Following ‘How much is Too Much’ – level 2 Takes 15-20 minutes 2-3 hour skill-based training available - Dr Malcolm Thomas, Effective Professional Interactions (http://www.effectivepi.co.uk)
 Health Behaviour Change: A Guide for Practitioners Following ‘How much is Too Much’ – level 2 Takes minutes 2-3 hour skill-based training available - Dr Malcolm Thomas, Effective Professional Interactions (")
18
Motivational approach fits with patient centred practice Both clinicians and patients are experts Distinction between disease and illness Understanding patients in a context Finding common ground Mutual decision making

19
Patient presents problem Gathering information Parallel search of two frameworks Disease framework Doctor’s agenda: Symptoms Signs Investigations Pathophysiology Differential diagnosis Illness framework Patient’s agenda: Ideas Concerns Expectations Feelings Understanding the patient’s unique experience of illness Integration of the two frameworks Shared understanding & decision making

20
Patient centred practice - active listening What I say What I hear What I mean or feel What I understand patient practitioner

21
Clinician assumptions This person ought to change this person wants to change patient’s health is motivation no change=failure either do or don’t Now is the right time being tough is best I know - my advice is good negotiation is always best

22
Motivational Interviewing ‘client-centred, directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence’ 1. Express empathy 2. Develop discrepancy 3. Avoid argumentation 4. Roll with resistance 5. Support self-efficacy Miller & Rollnick 2002

23
Behaviour change counselling ‘ways of structuring a conversation which maximises the individual’s freedom to talk and think about change in an atmosphere free of coercion and the provision of premature solutions’ Rollnick et al. 1999 –Assessing readiness –Weighing up pros and cons –Determining action - moving patients on Rollnick et al. 1999

26
Discussion Issues to think about –How could this fit in PHC? –Who might be best place to deliver this? –In what context could it be offered? –How should it be incentivised –What about patients who need more?

27
Referral (1) Patients should be referred to specialist services who : show a relatively high level of alcohol dependence or alcohol-related harm are harmful drinkers who have not benefited from brief counselling and wish to receive further help for their alcohol problems
 Patients should be referred to specialist services who : show a relatively high level of alcohol dependence or alcohol-related harm are harmful drinkers who have not benefited from brief counselling and wish to receive further help for their alcohol problems")
28
Referral (2) can be defined as score of 20+ on the full AUDIT obvious signs of physical dependence (e.g. withdrawal symptoms, withdrawal relief or avoidance drinking, very high tolerance, blackouts) severe alcohol-related problems or risk of such problems (e.g. possible loss of job, family, etc.) score on recognised measure of dependence (e.g. 10-item Leeds Dependence Questionnaire)
 severe alcohol-related problems or risk of such problems (e.g. possible loss of job, family, etc.) score on recognised measure of dependence (e.g. 10-item Leeds Dependence Questionnaire).")
Similar presentations

















. 4-2 How Does Behavior Change? Behavior ABehavior B.>")


 Presentation Objectives Understand theory & spirit of MI Brief review of evidence using MI with teens Learn some MI techniques.>")

