Download presentation
Presentation is loading. Please wait.

1
Alan N. Barkun ADVANCES IN THE MANAGEMENT OF NON VARICEAL GASTROINTESTINAL HEMORRHAGE – a 2004 update Division of Gastroenterology McGill University and the McGill University Health Centre Montréal, Canada

2
INTRODUCTION Significant evolution in the management of patients with non variceal upper GI bleeding (supportive care, pharmacological treatment and endoscopic hemostasis) The last Consensus guidelines published: Gut 2002 – incomplete Before that: NIH Consensus Conference, almost 15 years ago
 The last Consensus guidelines published: Gut 2002 – incomplete Before that: NIH Consensus Conference, almost 15 years ago")
3
AIMS To review major advances in the management of patients with gastrointestinal hemorrhage To highlight the contribution of 2 major Canadian initiatives that have helped set the international standards of care: RUGBE The Banff Consensus Conference

4
Ann Int Med., 2003 – Banff Consensus group on Non Variceal Upper GI Bleeding

5
1. Determination of need for guidelines Review background existing literature and the timing of previously published guidelines 2. Membership of the Consensus group Identify participants for their expertise and representation of multiple relevant disciplines and societies 3. Determination of clinically relevant issues Identify clinically relevant topics based on literature review and perceived clinical needs 4. Nature and extent of background preparation Identify key articles and develop narrative reviews, systematic reviews, meta-analyses 5. Delphi consensus process Initiate a Delphi Consensus process six weeks prior to conference to circulate preliminary statements and evidence 6. The Consensus Conference Present recommendation statement, a summary review of evidence and grading for discussion and vote 7. Preparation process and format of the report Draft manuscript and circulate for review by voting conference participants and non-voting chair The Adopted Process of Guideline Development

6
Levels of Evidence I Evidence from at least one randomized controlled trial IIaEvidence from well-designed, non- randomized controlled trials IIbEvidence from well-designed cohort or case-control studies IIcEvidence from poorly-controlled studies; dramatic results from uncontrolled studies IIIExpert opinion

7
Classification of Recommendations AGood supportive evidence BFair supportive evidence CPoor supportive evidence but recommendations reasonable on other grounds DFair contrary evidence EGood contrary evidence

8
Voting on Statements A.Accept completely B.Accept with some reservation C.Accept with major reservation D.Reject with reservation E.Reject completely Accept statements where >50% vote A, B or C Provide median vote in summary

9
NON VARICEAL UPPER GASTROINTESTINAL BLEEDING ALL GI BLEEDERS Identify the high risk Pt 80% stop bleeding20% bleed on, on their ownor re-bleed 20% RE-BLEEDING RATE TARGET GROUP ANY Rx

10
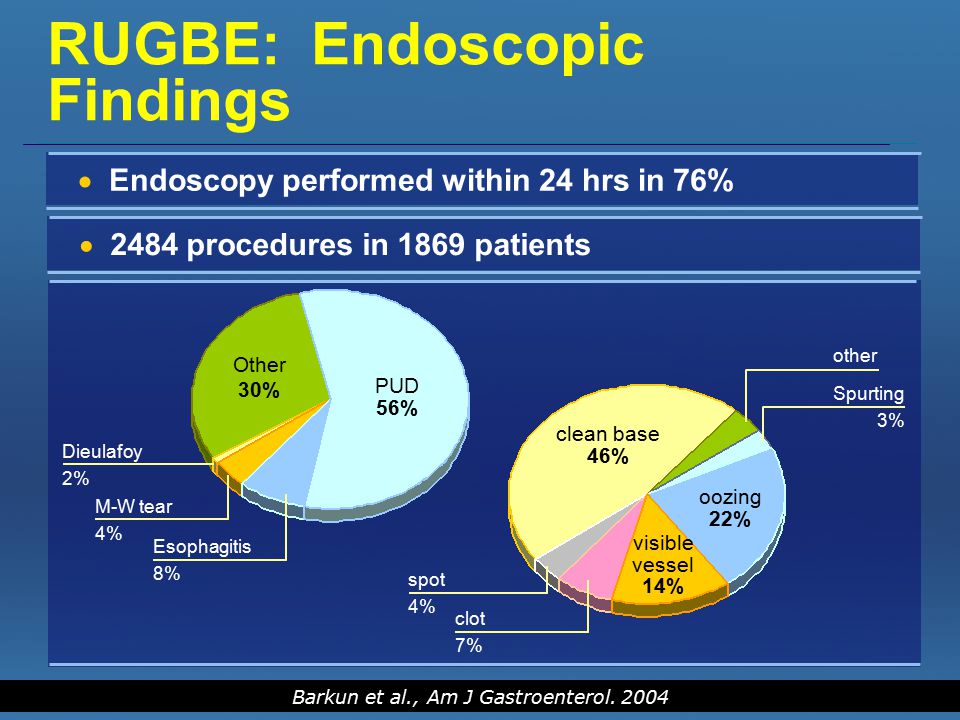
RUGBE: Endoscopic Findings PUD 56% Other 30% Esophagitis 8% M-W tear 4% Dieulafoy 2% oozing 22% visible vessel 14% clean base 46% other Spurting 3% clot 7% spot 4% 2484 procedures in 1869 patients Endoscopy performed within 24 hrs in 76% Barkun et al., Am J Gastroenterol. 2004
11
Main Outcomes Continued bleeding/rebleeding14.1% Surgery 6.5% Mortality 5.4% Mean hospitalization 5.6±6.1 d Barkun et al., Am J Gastroenterol. 2004

12
Hospitals should develop institution specific protocols for multidisciplinary management, which should include access to an endoscopist with training in endoscopic hemostasis (III C) A: 100% STATEMENT 1 80% of RUGBE sites did not have a specific protocol
 A: 100% STATEMENT 1 80% of RUGBE sites did not have a specific protocol")
13
Support staff trained to assist in endoscopy should be available for urgent endoscopy (III C) A: 92%, B: 8% STATEMENT 2 Only 40% of all RUGBE sites had a nurse taking availability call
 A: 92%, B: 8% STATEMENT 2 Only 40% of all RUGBE sites had a nurse taking availability call")
14
Immediate evaluation and appropriate resuscitation is critical to proper management (III C) A: 96%, B: 4% STATEMENT 3 Recent level II data suggest that is true, but only historical control group (Baradarian Am J Gastro 2004)
 A: 96%, B: 4% STATEMENT 3 Recent level II data suggest that is true, but only historical control group (Baradarian Am J Gastro 2004)")
15
Clinical (non-endoscopic) stratification of patients into low- and high-risk categories for rebleeding and mortality is important for proper management. Available prognostic scales may be used to assist in decision making. (II-2 B) A: 76%, B: 24% STATEMENT 5
 A: 76%, B: 24% STATEMENT 5.")
16
Blatchford criteria (BMJ, 1997) Risk factor for mortality N=1334 Multifactorial analysis Age >75 vs 45-59 yrs 304 4.5 (2-10) Urea 8-24.9 vs 6.5 mmol/L >25 vs <6.5 mmol/L 678 63 5.5 (2-15) 18 (5.3-59) Blood Pressure (diast.) 60- 69 vs >70 mmHg 70 mmHg 261 116 3.8 (1.8-7.7) 3.1 (1.7-5.6) Co-morbidity Cardiac failure Hepatic failure Disseminated cancer Other major diseases 25 33 71 304 9.4 (3.2-28) 43 (14-133) 3.8 (1.8-8.1) 1.8 (1-3.1) Adapted from BMJ 1997
 Risk factor for mortality N=1334 Multifactorial analysis Age >75 vs yrs (2-10) Urea vs 6.5 mmol/L >25 vs <6.5 mmol/L (2-15) 18 (5.3-59) Blood Pressure (diast.) vs >70 mmHg 70 mmHg ( ) 3.1 ( ) Co-morbidity Cardiac failure Hepatic failure Disseminated cancer Other major diseases (3.2-28) 43 (14-133) 3.8 ( ) 1.8 (1-3.1) Adapted from BMJ 1997")
17
Independent Predictors of Mortality Clinical Scenarios (all patients who were not transferred) Age = 65 Nb of comorbidities > 1 ASA > score 1 Bright blood per NGT = No Systolic blood pressure at initial assessment = 120 mm Hg Inpatients status at time of bleeding yes no Bright blood per rectal exam yes no Bright blood per rectal exam Rebleeding yes no yes no yes no Rebleeding yes no yes no Probability of Mortality 1.3 % 6.6 % 3.8 % 17.3 % 3.6 % 9.9 % 36.7 % 16.4 %
 Age = 65 Nb of comorbidities > 1 ASA > score 1 Bright blood per NGT = No Systolic blood pressure at initial assessment = 120 mm Hg Inpatients status at time of bleeding yes no Bright blood per rectal exam yes no Bright blood per rectal exam Rebleeding yes no yes no yes no Rebleeding yes no yes no Probability of Mortality 1.3 % 6.6 % 3.8 % 17.3 % 3.6 % 9.9 % 36.7 % 16.4 %")
18
In selected patients, the placement of a naso-gastric tube can be considered because the findings may have prognostic value (II-3 B) A: 42%, B: 33%, C: 25% STATEMENT 4
 A: 42%, B: 33%, C: 25% STATEMENT 4")
19
ROLE of NGA Diagnostic criteriaBloodyBloody or coffee grounds Any NGA result other than clear/bile Sensitivity (%)48.4 (CI: 40.3-56.5)80.4 (CI: 73.3-86.4)93.5 (CI: 88.3-96.8) Specificity (%)75.8 (CI: 70.0-80.0)31 (CI: 26.4-36.0)15.8 (CI: 12.3-20.0) PPV (%)45.4 (CI: 37.6-53.3)32.7 (CI: 28.0-37.8)31.6 (CI: 27.4-36.2) NPV (%)77.9 (CI: 73.2-82.0)79.2 (CI: 71.6-85.5)85.3 (CI: 74.6-92.7) Positive likelihood ratio 2.00 (CI: 1.6-2.6)1.20 (CI: 1.1-1.3)1.1 (CI: 1.0-1.2) Diagnostic accuracy (%) 67.7 (CI: 63.7-71.7)45.6 (CI: 41.3-49.9)38.7 (CI: 34.5-42.8) Aljebreen AM et al., 2003
48.4 (CI: )80.4 (CI: )93.5 (CI: ) Specificity (%)75.8 (CI: )31 (CI: )15.8 (CI: ) PPV (%)45.4 (CI: )32.7 (CI: )31.6 (CI: ) NPV (%)77.9 (CI: )79.2 (CI: )85.3 (CI: ) Positive likelihood ratio 2.00 (CI: )1.20 (CI: )1.1 (CI: ) Diagnostic accuracy (%) 67.7 (CI: )45.6 (CI: )38.7 (CI: ) Aljebreen AM et al., 2003")
20
Early stratification of patients into low- and high-risk categories for rebleeding and mortality, based on clinical AND endoscopic criteria, is important for proper management. Available prognostic scales may be used to assist in decision making. (I A) A: 96%, B: 0, C: 4% STATEMENT 6
 A: 96%, B: 0, C: 4% STATEMENT 6.")
21
Rockall Score – Risk assessment of Death/Rebleeding (N=4185) Variable 0 Score 1 2 3 Age (yrs) < 6060-79≥ 80 Shock No shock P < 100 Syst BP ≥ 100 P ≥ 100 plus Sys BP ≥ 100 Hypotension Diagnosis MW tear, normal endoscopy with no blood seen All other diagnosisMalignancy of UGI tract Major SRH None or dark spotBlood in UGI tract Adherant clot, visible or spurting vessel Comorbidity No or mild coexistingModerate coexisting (e.g., hypertension) Severe coexisting (e.g., CHF) Life threatening (e.g., RF) Rockall, Lancet 1996 RUGBE validation of the Rockall scoring has been submitted for publication (Enns et al.)
 Variable 0 Score Age (yrs) < ≥ 80 Shock No shock P < 100 Syst BP ≥ 100 P ≥ 100 plus Sys BP ≥ 100 Hypotension Diagnosis MW tear, normal endoscopy with no blood seen All other diagnosisMalignancy of UGI tract Major SRH None or dark spotBlood in UGI tract Adherant clot, visible or spurting vessel Comorbidity No or mild coexistingModerate coexisting (e.g., hypertension) Severe coexisting (e.g., CHF) Life threatening (e.g., RF) Rockall, Lancet 1996 RUGBE validation of the Rockall scoring has been submitted for publication (Enns et al.)")
22
Early endoscopy ( within the first 24 hours ) Allows for safe and prompt discharge of patients classified as low-risk* (I A) –A: 92%, B: 8% Improves patient outcomes for patients classified as high-risk* (II-2 C) –A: 64%, B: 36% Reduces resource utilization for patients classified as either low- or high-risk* (IA) –A: 88%, B: 12% *by clinical and endoscopic criteria STATEMENT 7 Increasing risk of negative outcome
 Allows for safe and prompt discharge of patients classified as low-risk* (I A) –A: 92%, B: 8% Improves patient outcomes for patients classified as high-risk* (II-2 C) –A: 64%, B: 36% Reduces resource utilization for patients classified as either low- or high-risk* (IA) –A: 88%, B: 12% *by clinical and endoscopic criteria STATEMENT 7 Increasing risk of negative outcome ")
23
Early endoscopy 75%

24
Prognostic Factors: Endoscopic Laine, Peterson, N Engl J Med 1994. Ia = spurter Ib = oozer IIaIIb Forrest Incidence of Re-bleeding by Appearance of Ulcer at Endoscopy

25
The clean base ulcer

26
The clean base ulcer / The pigmented dot

27
A finding of low-risk endoscopic stigmata (a clean based ulcer, or a non-protuberant pigmented dot in an ulcer bed) is not an indication for endoscopic hemostatic therapy (I A) A: 100% STATEMENT 8
 is not an indication for endoscopic hemostatic therapy (I A) A: 100% STATEMENT 8")
28
The outcome of adherent clots

29
A finding of clot in an ulcer bed warrants targeted irrigation in an attempt at dislodgment. Endoscopic therapy for persistently adherent clots is controversial (III C -- Ia) A: 32%, B: 56%, C: 4%, D: 8% -- more unanimity STATEMENT 9
 A: 32%, B: 56%, C: 4%, D: 8% -- more unanimity STATEMENT 9.")
30
Visible vessel

32
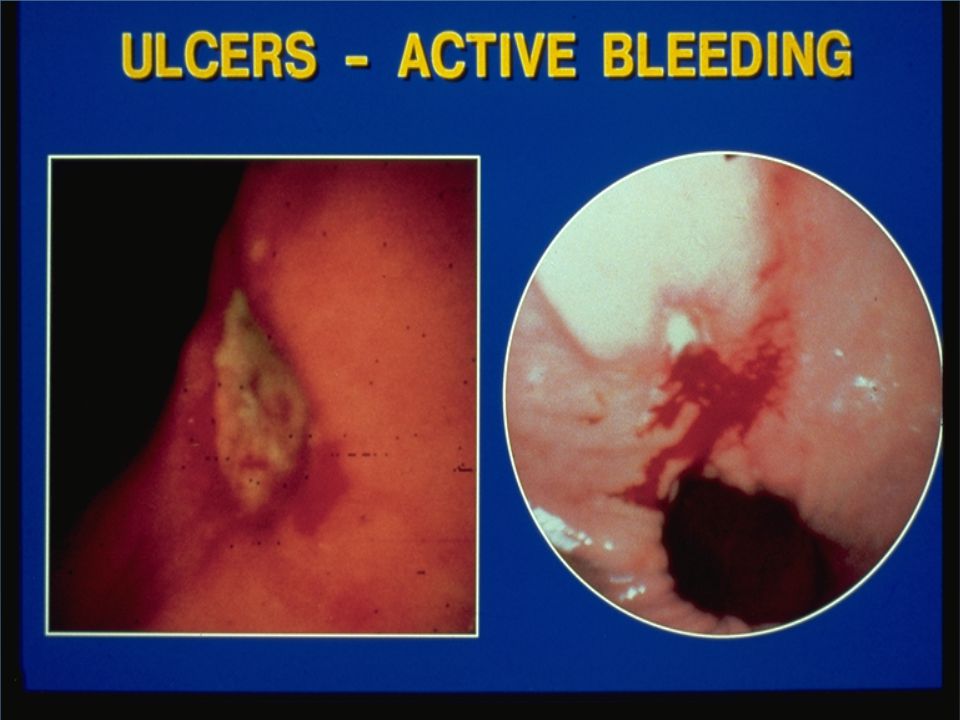
Active bleeding: “Spurter” (= trouble!)
")
33
Trouble – in slow motion

34
A finding of high-risk endoscopic stigmata (active bleeding or a visible vessel in an ulcer bed) is an indication for immediate endoscopic hemostatic therapy (I A) A: 100% STATEMENT 10
 is an indication for immediate endoscopic hemostatic therapy (I A) A: 100% STATEMENT 10")
35
Endoscopic Therapy Meta-analysis (Cook, et al.Gastroenterol,1992) 30 trials (n=2,412) Similar results in an earlier meta-analysis of 25 trials (Sacks, et al. JAMA,1990) Treatments studied:thermal (laser), few injection, no combination or clips 0.40-0.760.55Mortality 0.28-0.450.36Surgery 0.32-0.450.38 Further Bleeding 95% CIOR OR=odds ratio for treatment vs. controls. Statistical heterogeneity was observed for bleeding and surgery. OR CI Recently confirmed by Bardou et al, 2003 (71 studies, 9000 patients)
 Treatments studied:thermal (laser), few injection, no combination or clips Mortality Surgery Further Bleeding 95% CIOR OR=odds ratio for treatment vs. controls. Statistical heterogeneity was observed for bleeding and surgery. OR CI Recently confirmed by Bardou et al, 2003 (71 studies, 9000 patients).")
36
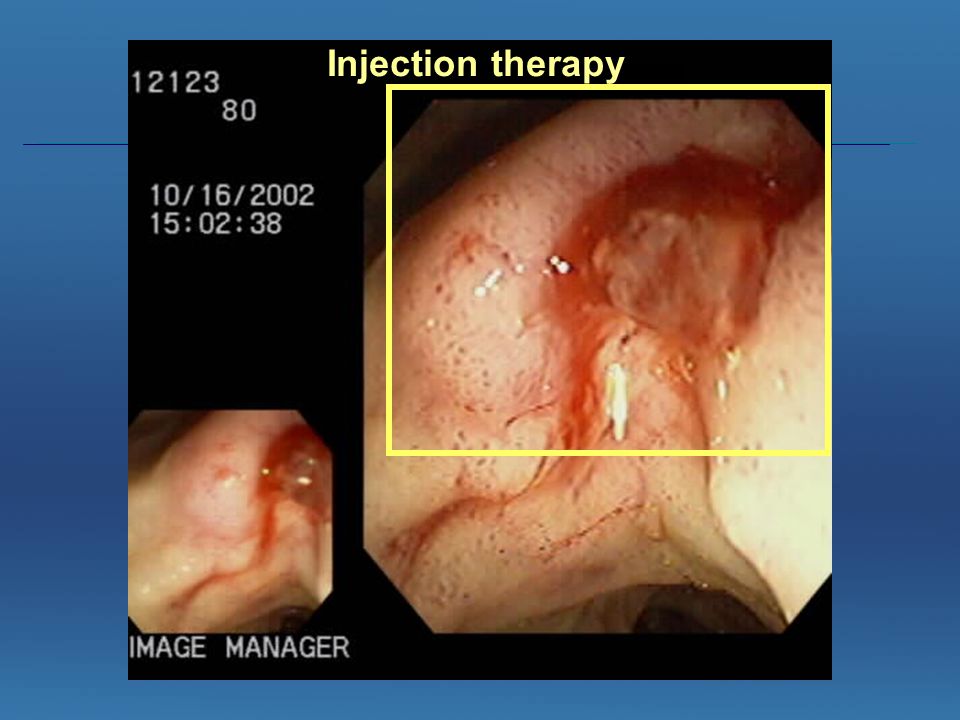
Injection therapy

39
Endoscopic Therapy

40
Monotherapy, with injection or thermal coagulation, is an effective endoscopic hemostatic technique for high-risk stigmata; however, the combination is superior to either treatment alone (I B) A: 36%, B: 48%, C: 16% STATEMENT 13
 A: 36%, B: 48%, C: 16% STATEMENT 13")
41
Endoscopic therapy -0,4-0,3-0,2-0,100,10,2 A: ressaignement Clips Thermique Injection Pharmaco Combinaison bénéfiquesContrôle meilleur -0,08-0,06-0,04-0,0200,020,040,060,08 B: mortalité Combinaisons bénéfiquesContrôle meilleur Clips Thermique Injection Pharmaco Thermique Injection Phamaco C: ressaignement Injection puis thermique bénéfiqueContrôle meilleur -0,3-0,2-0,10 0,1 Thermique Injection Pharmaco D: mortalité Injection puis thermique bénéfiqueContrôle meilleur -0,04-0,03-0,02-0,0100,010,02 Toutes combinaisons Injection suivie d’un traitement thermique Combinaisons versus injection : Ressaignement -16.7% [-18.2%; -15.2%], Mortalité -2.7% [-3.6%; -1.7%]
![Endoscopic therapy -0,4-0,3-0,2-0,100,10,2 A: ressaignement Clips Thermique Injection Pharmaco Combinaison bénéfiquesContrôle meilleur -0,08-0,06-0,04-0,0200,020,040,060,08 B: mortalité Combinaisons bénéfiquesContrôle meilleur Clips Thermique Injection Pharmaco Thermique Injection Phamaco C: ressaignement Injection puis thermique bénéfiqueContrôle meilleur -0,3-0,2-0,10 0,1 Thermique Injection Pharmaco D: mortalité Injection puis thermique bénéfiqueContrôle meilleur -0,04-0,03-0,02-0,0100,010,02 Toutes combinaisons Injection suivie d’un traitement thermique Combinaisons versus injection : Ressaignement -16.7% [-18.2%; -15.2%], Mortalité -2.7% [-3.6%; -1.7%]](http://images.slideplayer.com/18/6103308/slides/slide_41.jpg "Endoscopic therapy -0,4-0,3-0,2-0,100,10,2 A: ressaignement Clips Thermique Injection Pharmaco Combinaison bénéfiquesContrôle meilleur -0,08-0,06-0,04-0,0200,020,040,060,08 B: mortalité Combinaisons bénéfiquesContrôle meilleur Clips Thermique Injection Pharmaco Thermique Injection Phamaco C: ressaignement Injection puis thermique bénéfiqueContrôle meilleur -0,3-0,2-0,10 0,1 Thermique Injection Pharmaco D: mortalité Injection puis thermique bénéfiqueContrôle meilleur -0,04-0,03-0,02-0,0100,010,02 Toutes combinaisons Injection suivie d’un traitement thermique Combinaisons versus injection : Ressaignement -16.7% [-18.2%; -15.2%], Mortalité -2.7% [-3.6%; -1.7%]")
42
Adding a second procedure reduced: - further bleeding rate from 18.4% to 10.6% (OR 0.53, 95% CI:0.40–0.69), - surgery from 11.3% to 7.6% (OR: 0.64, 95% CI: 0.46–0.90), and - mortality fell from 5.1% to 2.6% (OR: 0.51, 95% CI: 0.31–0.84)
, - surgery from 11.3% to 7.6% (OR: 0.64, 95% CI: 0.46–0.90), and - mortality fell from 5.1% to 2.6% (OR: 0.51, 95% CI: 0.31–0.84)")
43
The placement of clips is a promising endoscopic hemostatic therapy for high-risk stigmata (I B) A: 44%, B: 52%, C: 4% STATEMENT 14
 A: 44%, B: 52%, C: 4% STATEMENT 14")
44
Clipping a visible vessel / oozer

46
Routine second look endoscopy is not recommended (I E) STATEMENT 15 A: 92%, B: 8%
 STATEMENT 15 A: 92%, B: 8%")
47
P=0.03

48
In cases of rebleeding, a second attempt at endoscopic therapy is generally recommended (I A) A: 100% STATEMENT 16
 A: 100% STATEMENT 16")
49
Somatostatin and octreotide are not recommended in the routine management of patients (I C) ** A: 96%, B: 4% STATEMENT 19
 ** A: 96%, B: 4% STATEMENT 19")
50
Most re-bleeding occurs within the first 72 hours Lau et al, 1998 Early Risk of Re-bleeding Natural History of the Visible Vessel 25 6 13 9 5 9 88 0 0 20 40 80 100 Day 1Day 2Day 3 Presence following endoscopic treatment on Day 0 Visible Vessels n = 25-52 60 Adherent clot Visible vessel Active bleeding %

51
Effect of acid suppression Acid is associated with Decreased platelet aggregation, and platelet disaggregation (in vivo, and animal models) – ideal pH approximately 6.5 Increased clot lysis due to pepsin activation by acid (in vitro) Increased fibrinolytic activity, that is impaired by acid suppression (in vitro, cell culture assays)
 – ideal pH approximately 6.5 Increased clot lysis due to pepsin activation by acid (in vitro) Increased fibrinolytic activity, that is impaired by acid suppression (in vitro, cell culture assays)")
52
H2 receptor antagonists are not recommended in the management of patients (I D) A: 92%, B: 8% STATEMENT 18
 A: 92%, B: 8% STATEMENT 18")
53
Effect of IV H 2 RA on Upper GI Bleeding: meta analysis of 1062 patients, 24 RCT’s NO differences in outcomes attributable to IV H2RA’s for ALL patientsNO differences in outcomes attributable to IV H2RA’s for ALL patients Only significant differences amongst patients with bleeding gastricOnly significant differences amongst patients with bleeding gastric ulcers ulcers Levine JA et al., APT, 2002 Absolute change(%) IV H2RA vs placebo -7.2% NNT =14 -3.2% NNT =15 -6.7% ** NNT =32 Re-bleedingSurgeryMortality o
 IV H2RA vs placebo -7.2% NNT = % NNT = % ** NNT =32 Re-bleedingSurgeryMortality o")
54
Tolerance of H2RA Netzer, 1999 Omeprazole IV Ranitidine IV Gastric pH

55
Role of PPI for UGI Bleeding: Continuous Infusion Lau, et al. NEJM 2000. 3 RCT’s concur 1RCT “negative”*

56
An IV bolus followed by continuous infusion intravenous proton pump inhibitor is effective in decreasing rebleeding in patients who have undergone successful endoscopic therapy (I A) A: 100% STATEMENT 20
 A: 100% STATEMENT 20")
57
ci IV PPI vs placebo ci IV PPI vs H2RA Continuous Infusion IV PPI vs H2RA and placebo: meta-analysis Bardou et al., submitted, 2004 20% 15.6% 2.8% Absolute risk reduction in % in the model Meta-analysis of 71 studies and over 9000 patients included 16 H2RA and 4 CI IVPPI studies since 1990 * * *

58
PUR-STUDY – RESULT PRIMARY ENDPOINT At 72 hours: S1= need for endoscopy without hemostatic therapy S2= need for endoscopy with hemostatic therapy S3 = surgery S4 = death Problem was most likely patient selection – will be an issue for any future true multicenter trial Barkun et al., DDW 2004

59
p=0.038* Outcome rates (S1-4) in % (ITT) PUR-STUDY – RESULT secondary analysis – outcomes according to initial Forrest class (22/209) (23/221) (30/341) (25/321) (16/55) (8/64) Barkun et al., DDW 2004
 in % (ITT) PUR-STUDY – RESULT secondary analysis – outcomes according to initial Forrest class (22/209) (23/221) (30/341) (25/321) (16/55) (8/64) Barkun et al., DDW 2004")
60
PUR-STUDY – RESULT secondary analysis – outcomes according to ulcer site (13/263) (28/250) Outcome rates (S1-4) in patients with gastric ulcer ITT p=0.009* Barkun et al., DDW 2004
 (28/250) Outcome rates (S1-4) in patients with gastric ulcer ITT p=0.009* Barkun et al., DDW 2004")
61
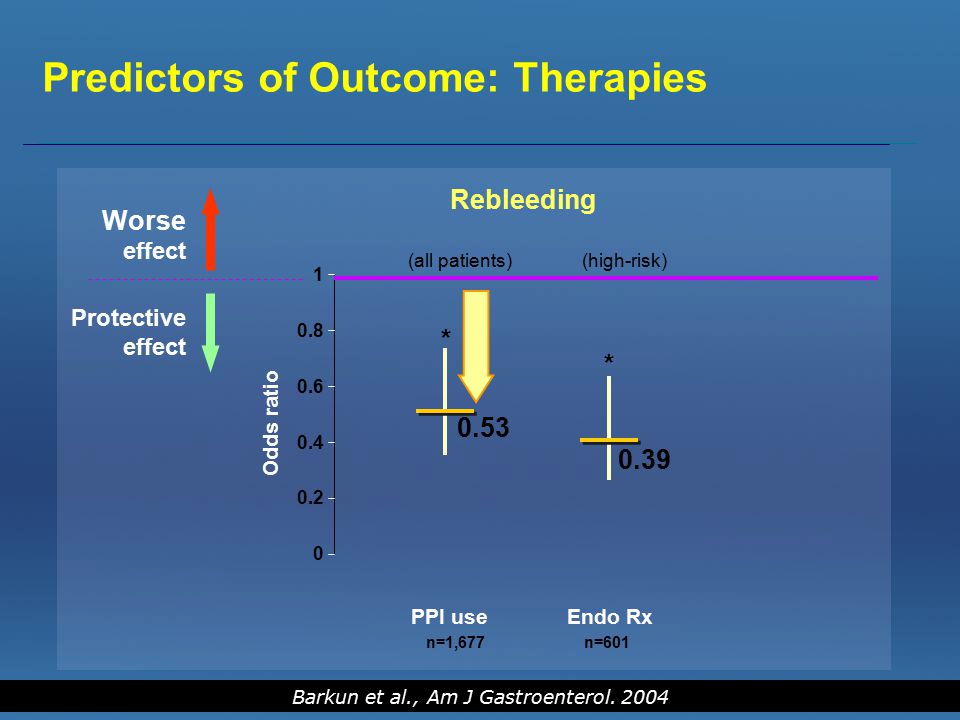
0 0.2 0.6 0.8 0.4 1 PPI use Endo Rx Rebleeding (all patients) (high-risk) Worse effect Protective effect Odds ratio 0.53 * 0.39 * n=1,677n=601 Predictors of Outcome: Therapies Barkun et al., Am J Gastroenterol. 2004
62
0 0.2 0.6 0.8 0.4 1 Mortality (out-patients and high-risk) PPI useEndo Rx Worse effect Protective effect Odds ratio 0.18 * 0.31 * n=432 Predictors of Outcome: Therapies Barkun et al., Am J Gastroenterol. 2004

63
Role of PPI for UGI Bleeding – Oral - Following Endoscopic Therapy Khuroo et a., 1997, Javid et al, 2001, Kaviani et al., 2002 As follow-up and in response to criticisms of the study by Khuroo et al, 1997 OME PO 40 mg q12h x 5d (n=82) Placebo PO q12h x 5d (n=84) P<0.022 P=NS Outcomes in 166 patients treated with oral PPI or placebo after injection (Ia to IIb) OME PO 20 mg q6 h x 5d (n=82) Placebo PO q12h x 5d (n=84) 17 33 GENERALIZABILITY OF RESULTS? Re: choice of endoscopic therapy and effect of pharmacotherapy

64
In patients awaiting endoscopy, empiric therapy with high dose proton pump inhibitor should be considered (III C) A: 40%, B: 32%, C: 16%, D: 12% STATEMENT 21
 A: 40%, B: 32%, C: 16%, D: 12% STATEMENT 21")
65
Patients with ulcer bleeding should be tested for Helicobacter pylori and receive eradication therapy if infection is present (I A) A: 96%, B: 4% STATEMENT 23
 A: 96%, B: 4% STATEMENT 23")
66
Cost-effectiveness of IV PPI therapy in 2004 Oral PPI’s? Effectiveness Cost increased decreased increased decreased PRE- ENDOSCOPY POST- ENDOSCOPY US – Barkun, abs 2002 Canada – Barkun, abs 2002 US – Gagnon, 2003 Canada – Enns, 2003 HK – Lee, 2002 US – Spiegel, 2003 US – Barkun, 2004 Canada – Gregor, abs 2001 Barkun, 2004 Hospitalization - rebleed: CDN $5,220 – US $11,802 - no rebleed: CDN $2696 – US $7,993 Yet over-utilization noted … (Cornish et al, 2002, Romagnuolo et al. x2 2004)
.")
67
Why are IVPPI so cost-effective? Medication costs $240 Cost of 1 re- bleeding $11,802 NNT – approx 5-6

68
Barkun et al., CJG, 2004

69
Future directions ABC’s and triaging remain the cornerstone of optimal management More data are needed regarding –Hemostatic clips and how they compare to other endoscopic hemostatic therapies –Combination endoscopic therapies –Optimal IV PPI dosing, utilization patterns –Role of oral PPIs –Role of PPIs prior to endoscopy An effort must be made to improve utilization

Similar presentations



















>")
