Download presentation
Presentation is loading. Please wait.

1
Cardiology Symposium James T. DeVries, MD Assistant Professor of Medicine Dartmouth Medical School Dartmouth-Hitchcock Medical Center

2
No disclosure or conflicts

3
Outline What is new with revascularization?What is new with revascularization? Bypass surgery (CABG) versus coronary stents (PCI)Bypass surgery (CABG) versus coronary stents (PCI) New technologies in the pipeline- ready for primetime?New technologies in the pipeline- ready for primetime? Aortic valve replacement without opening the chestAortic valve replacement without opening the chest Stroke therapyStroke therapy
 versus coronary stents (PCI)Bypass surgery (CABG) versus coronary stents (PCI) New technologies in the pipeline- ready for primetime New technologies in the pipeline- ready for primetime. Aortic valve replacement without opening the chestAortic valve replacement without opening the chest Stroke therapyStroke therapy.")
4
Coronary Artery Disease Heart disease is the #1 killer in the USHeart disease is the #1 killer in the US We are diagnosing heart disease more frequently due to better testing, improved sensitivity and increased awarenessWe are diagnosing heart disease more frequently due to better testing, improved sensitivity and increased awareness As a nation, we have too much obesity and lack of physical activity, risk factors for the development of coronary artery diseaseAs a nation, we have too much obesity and lack of physical activity, risk factors for the development of coronary artery disease

8
How do we best treat heart disease? Medical therapy?Medical therapy? Coronary stents (PCI)?Coronary stents (PCI)? Bypass surgery (CABG)?Bypass surgery (CABG)?
 Coronary stents (PCI). Bypass surgery (CABG) Bypass surgery (CABG) .")
9
+ Angina relief + Reduced re-intervention + Complete revascularization High costs Invasive + Cost effective + Fast recovery + Reduced acute complications - Increased restenosis - Repeat revascularization PCI CABG The pros and cons of CABG historically outweighed those of PCI CABG & PCI: Historical Pro & Cons

10
Evolution of Revascularization + Off pump technique + Less invasive approach + Increased arterial revascularization + Optimal perioperative monitoring + Improved technique + Improved stent design + DES PCI CABG High costs Invasive Recovery time - Increased restenosis - Repeat revascularization ? Over the last decade, the standard of care for both CABG and PCI has continuously improved, leveling the playing field.

11
CABG vs PCI Trials Results Summary TrialTrial Clinical ParametersClinical Parameters Angiographi c Endpoints Cost Assessment Mortality & MI Angina Relief Repeat Revasculariza tion GABI PCIPCICABG No difference n/a EAST CABGCABGCABGPCI RITA CABGCABGn/an/a ERACI CABGCABGn/aPCI CABRI CABGCABGn/an/a BARI n/aCABGn/an/a MASS-2 CABG (MI) n/aCABGn/a No differenc e AWESOME CABGn/an/a ERACI-2 PCIn/aCABGCABG SoS CABG (Mortality) CABGCABGn/an/a ARTS No difference n/aCABGn/aPCI Superior Treatment Modality No stents used Stents used CABG No difference PCI Significant decrease of revascularization expected with DES Repeat Revascularization
 n/aCABGn/a No differenc e AWESOME CABGn/an/a ERACI-2 PCIn/aCABGCABG SoS CABG (Mortality) CABGCABGn/an/a ARTS No difference n/aCABGn/aPCI Superior Treatment Modality No stents used Stents used CABG No difference PCI Significant decrease of revascularization expected with DES Repeat Revascularization")
12
TAXUS I TAXUS II Mean stent length [mm] E-SIRIUS SIRIUS TAXUS IV C-SIRIUS Lesion Complexity [% C Type] RAVEL Complex Lesions Long Stented lengths TAXUS VI TAXUS V QCA long lesion breakdown pending Drug Eluting Stent Trials … expanding lesion & procedural complexity with randomized trials
![TAXUS I TAXUS II Mean stent length [mm] E-SIRIUS SIRIUS TAXUS IV C-SIRIUS Lesion Complexity [% C Type] RAVEL Complex Lesions Long Stented lengths TAXUS VI TAXUS V QCA long lesion breakdown pending Drug Eluting Stent Trials … expanding lesion & procedural complexity with randomized trials](http://images.slideplayer.com/18/6094647/slides/slide_12.jpg "TAXUS I TAXUS II Mean stent length [mm] E-SIRIUS SIRIUS TAXUS IV C-SIRIUS Lesion Complexity [% C Type] RAVEL Complex Lesions Long Stented lengths TAXUS VI TAXUS V QCA long lesion breakdown pending Drug Eluting Stent Trials … expanding lesion & procedural complexity with randomized trials")
13
Arterial Revascularization Therapies Part II: a non-randomized comparison of contemporary PCI and coronary artery bypass grafting (CABG) in patients with multi-vessel coronary artery lesions ARTS-II Trial
 in patients with multi-vessel coronary artery lesions ARTS-II Trial")
14
Sirolimus-eluting stent 3.7 stents per patient Avg total length: 73 mm n = 607 Sirolimus-eluting stent 3.7 stents per patient Avg total length: 73 mm n = 607 ARTS-II Trial Historical Controls from ARTS I: 1202 patients with multivessel coronary lesions 18.2% diabetic 28% 3 vessel disease 7.5% type C lesions Historical Controls from ARTS I: 1202 patients with multivessel coronary lesions 18.2% diabetic 28% 3 vessel disease 7.5% type C lesions 607 patients with multivessel coronary lesions 26.2% diabetic 54% 3 vessel disease 13.9% type C lesions 607 patients with multivessel coronary lesions 26.2% diabetic 54% 3 vessel disease 13.9% type C lesions CABG n = 602 CABG n = 602 Bare Metal Stent 2.8 stents per patient Avg total length: 48 mm n = 600 Bare Metal Stent 2.8 stents per patient Avg total length: 48 mm n = 600 Endpoints: Primary – Major adverse cardiac and cerebrovascular events (MACCE), including death, cerebrovascular event, myocardial infarction, and revascularization, at 1 year for the comparison of CABG treated patients in the ARTS I trial with sirolimus-eluting stent patients in the ARTS II trial Secondary – MACCE at 30 days, 6 months, 3 and 5 years. – Total cost at 30 days – Cost, cost effectiveness, quality of life at six mo, and 1, 3, and 5 years Endpoints: Primary – Major adverse cardiac and cerebrovascular events (MACCE), including death, cerebrovascular event, myocardial infarction, and revascularization, at 1 year for the comparison of CABG treated patients in the ARTS I trial with sirolimus-eluting stent patients in the ARTS II trial Secondary – MACCE at 30 days, 6 months, 3 and 5 years. – Total cost at 30 days – Cost, cost effectiveness, quality of life at six mo, and 1, 3, and 5 years
, including death, cerebrovascular event, myocardial infarction, and revascularization, at 1 year for the comparison of CABG treated patients in the ARTS I trial with sirolimus-eluting stent patients in the ARTS II trial Secondary – MACCE at 30 days, 6 months, 3 and 5 years. – Total cost at 30 days – Cost, cost effectiveness, quality of life at six mo, and 1, 3, and 5 years.")
15
ARTS II: Event free survival p = <0.001 p = 0.003 p = 0.46

16
ARTS II: MACCE at one year Overall MACCE at 1 year At 1 year, there was no difference in the incidence of MACCE between the ARTS II SES group and the ARTS I CABG group. The ARTS I bare metal stent group was associated with a significantly higher rate of 1 year MACCE compared to the other groups

17
ARTS II: components of MACCE % ACC 2005 p=NS

18
ARTS II: Summary Among patients with multivessel coronary lesions, patients treated with sirolimus-eluting stents had significantly lower rates of MACCE compared with a historical registry of similar patients treated with bare metal stents and rates of MACCE statistically equivalent to patients from the same registry treated with CABG. Among patients with multivessel coronary lesions, patients treated with sirolimus-eluting stents had significantly lower rates of MACCE compared with a historical registry of similar patients treated with bare metal stents and rates of MACCE statistically equivalent to patients from the same registry treated with CABG. The majority of the difference in MACCE between the ARTS II and ARTS I BMS groups was driven by the increased need for repeat revascularization in the bare metal stent group. The ARTS II group had equal rates of revascularization to the ARTS I CABG group, despite having increased length and complexity of lesions. The majority of the difference in MACCE between the ARTS II and ARTS I BMS groups was driven by the increased need for repeat revascularization in the bare metal stent group. The ARTS II group had equal rates of revascularization to the ARTS I CABG group, despite having increased length and complexity of lesions. Among patients with multivessel coronary lesions, patients treated with sirolimus-eluting stents had significantly lower rates of MACCE compared with a historical registry of similar patients treated with bare metal stents and rates of MACCE statistically equivalent to patients from the same registry treated with CABG. Among patients with multivessel coronary lesions, patients treated with sirolimus-eluting stents had significantly lower rates of MACCE compared with a historical registry of similar patients treated with bare metal stents and rates of MACCE statistically equivalent to patients from the same registry treated with CABG. The majority of the difference in MACCE between the ARTS II and ARTS I BMS groups was driven by the increased need for repeat revascularization in the bare metal stent group. The ARTS II group had equal rates of revascularization to the ARTS I CABG group, despite having increased length and complexity of lesions. The majority of the difference in MACCE between the ARTS II and ARTS I BMS groups was driven by the increased need for repeat revascularization in the bare metal stent group. The ARTS II group had equal rates of revascularization to the ARTS I CABG group, despite having increased length and complexity of lesions.

19
Syntax Overall Study Goal To provide real-world answers to these questions in order to develop new guidelines for the beginning of the 21 st century. This goal requires a novel study approach:To provide real-world answers to these questions in order to develop new guidelines for the beginning of the 21 st century. This goal requires a novel study approach: allcomer study instead of highly selected patient population consensus physician decision (surgeon & cardiologist) instead of inclusion & exclusion criteria nested registry for CABG only and PCI only patients to capture patient characteristics and outcomes
 instead of inclusion & exclusion criteria nested registry for CABG only and PCI only patients to capture patient characteristics and outcomes.")
20
Eligible Study Population left main + 1-vessel disease left main + 2-vessel disease 3-vessel disease left main + 3-vessel disease Question of optimal treatment approach? new disease Isolated left main Previous interventions (PCI or CABG) excluded Acute MI with CK>2x Concomitant valve surgery Revascularization in all 3 vascular territories
 excluded Acute MI with CK>2x Concomitant valve surgery Revascularization in all 3 vascular territories.")
21
Patient Flow define CABG only population (2750 pts) define PCI only population (50 pts) Establish profiles of non randomizable patients and their outcomes amenable for ≤1 interventional treatment TAXUSCABG vs Patients with de novo 3-vessel-disease and / or left main disease screening Local Heart Team (surgeon and interventionalist) registration Randomize 1500 pts Registries amenable for both treatments options Multi-center randomized controlled trial TAXUS DES non inferior to CABG for 12 months binary MACCE rate
 define PCI only population (50 pts) Establish profiles of non randomizable patients and their outcomes amenable for ≤1 interventional treatment TAXUSCABG vs Patients with de novo 3-vessel-disease and / or left main disease screening Local Heart Team (surgeon and interventionalist) registration Randomize 1500 pts Registries amenable for both treatments options Multi-center randomized controlled trial TAXUS DES non inferior to CABG for 12 months binary MACCE rate")
22
MACCE Post-allocation/procedure to 5 years Follow Up and Data Collection Multi-center randomized controlled trial Registries CABG only 750 pts Randomly selected out of approx.>2750 pts PCI only <50 pts Baseline data QOL & Costs Baseline to 5 years PCI 750 pts CABG 750 pts

23
SYNTAX Results- 1 Year End Point CABGStent p value Revascularization5.9%13.7%0.001 Death/MI/Stroke7.6%7.7%NS Stroke2.2%0.6%0.001 MI3.2%4.8%NS

24
The Bottom Line Choice between CABG and PCI is complex, and depends on patient factors as well as technical considerationsChoice between CABG and PCI is complex, and depends on patient factors as well as technical considerations CABG tends to have less revascularizationCABG tends to have less revascularization There is no “one size fits all” approachThere is no “one size fits all” approach Discussion regarding the pro’s and cons of each approach is importantDiscussion regarding the pro’s and cons of each approach is important

25
Communication is Important!

26
Future Tech- Coming to a cath lab near you!

27
Aortic Valve Replacement- Without Surgery!

28
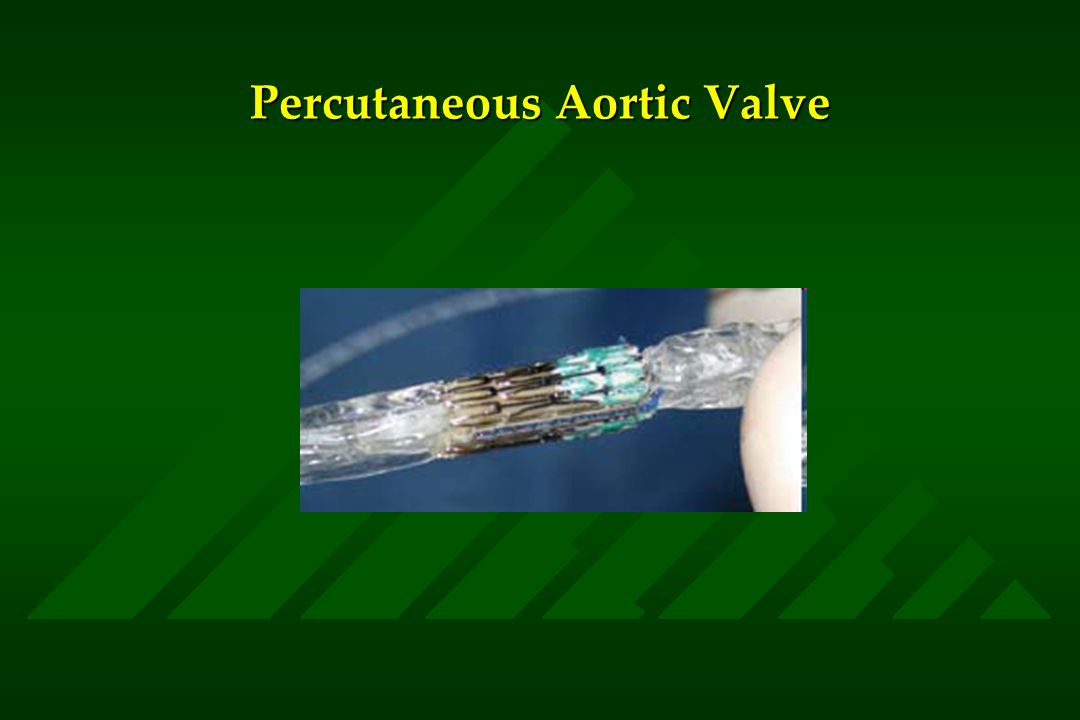
Aortic Stenosis Common cause of cardiovascular morbidity and mortality, particularly in the elderlyCommon cause of cardiovascular morbidity and mortality, particularly in the elderly Narrowing of aortic valve results in increased work load on the heartNarrowing of aortic valve results in increased work load on the heart Symptoms include shortness of breath, chest pain, and passing out (syncope)Symptoms include shortness of breath, chest pain, and passing out (syncope) Currently, only open heart surgery with valve replacement can correct this problemCurrently, only open heart surgery with valve replacement can correct this problem
Symptoms include shortness of breath, chest pain, and passing out (syncope) Currently, only open heart surgery with valve replacement can correct this problemCurrently, only open heart surgery with valve replacement can correct this problem")
29
Aortic Valve Replacement

30
Percutaneous Aortic Valve

32
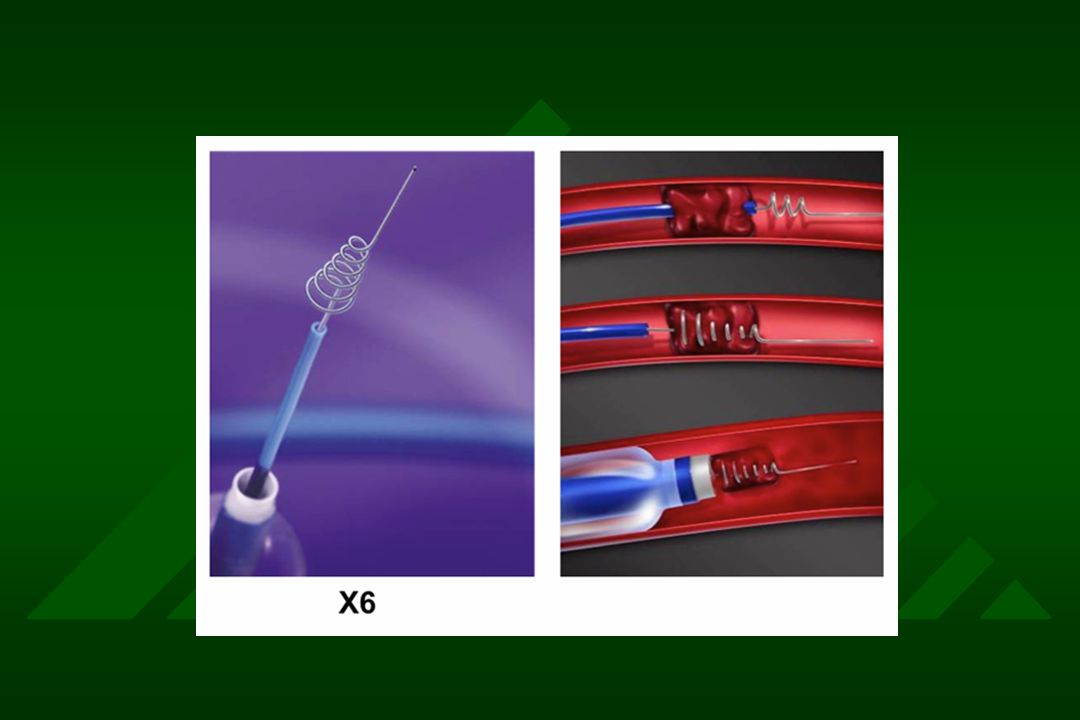
Technique for Insertion

33
Aortic Valvuloplasty

34
Stroke Therapy

35
Stroke Statistics There are over 700,000 strokes per year in the USThere are over 700,000 strokes per year in the US Stroke is the leading cause of adult disability and the third most common cause of deathStroke is the leading cause of adult disability and the third most common cause of death The vast majority of strokes result from blockage in the arteries of the brainThe vast majority of strokes result from blockage in the arteries of the brain The risk factors for stroke are the same as the risk factors for coronary heart diseaseThe risk factors for stroke are the same as the risk factors for coronary heart disease Treatment of strokes is limited, consisting mostly of supportive careTreatment of strokes is limited, consisting mostly of supportive care

36
Stroke Therapy Intravenous thrombolytic (“clot buster”) is the only currently approved therapy for strokeIntravenous thrombolytic (“clot buster”) is the only currently approved therapy for stroke Must be given within 3 hours of onset of symptomsMust be given within 3 hours of onset of symptoms Less effective in large strokes, risk of bleeding into the brainLess effective in large strokes, risk of bleeding into the brain Nationwide, it is used in less than 3% of strokesNationwide, it is used in less than 3% of strokes
 is the only currently approved therapy for strokeIntravenous thrombolytic ( clot buster ) is the only currently approved therapy for stroke Must be given within 3 hours of onset of symptomsMust be given within 3 hours of onset of symptoms Less effective in large strokes, risk of bleeding into the brainLess effective in large strokes, risk of bleeding into the brain Nationwide, it is used in less than 3% of strokesNationwide, it is used in less than 3% of strokes")
37
Stroke Therapy Increasing interest in catheter-based therapies for acute strokeIncreasing interest in catheter-based therapies for acute stroke Mechanically “open” the artery with devices, pull out the clotMechanically “open” the artery with devices, pull out the clot Stroke teams are integral part of this therapy, available 24/7 for rapid activationStroke teams are integral part of this therapy, available 24/7 for rapid activation Many similarities to treating heart attackMany similarities to treating heart attack

42
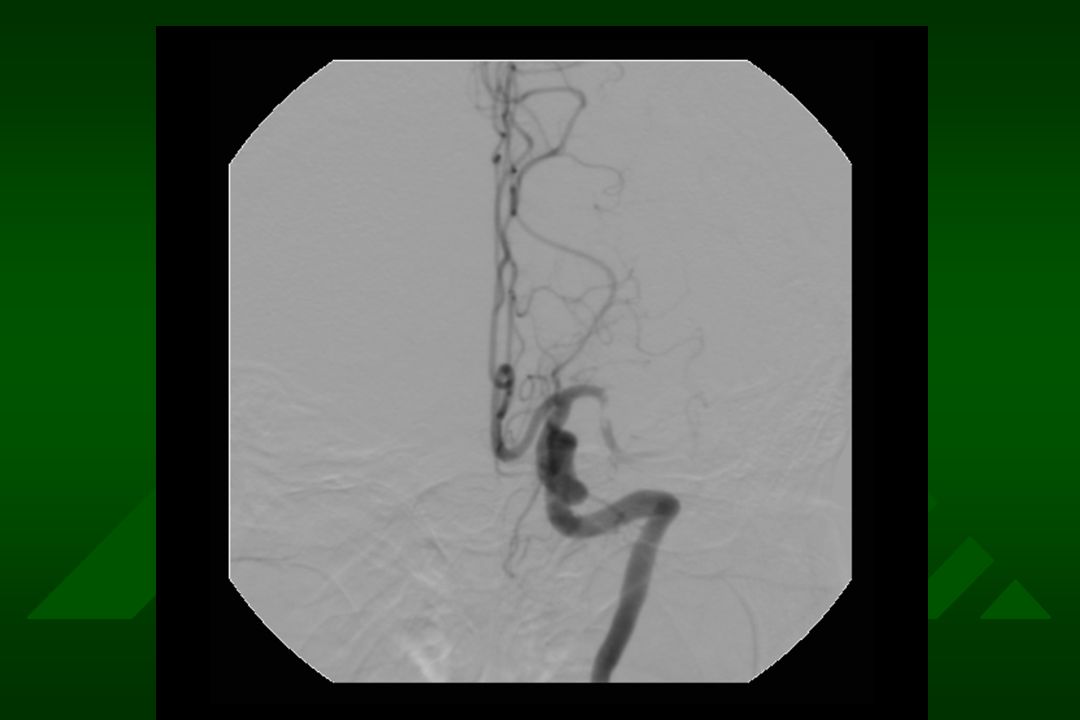
Case Example 49 yo mother of three presents with ride sided paralysis, inability to speak, onset 1 hour prior49 yo mother of three presents with ride sided paralysis, inability to speak, onset 1 hour prior Given thrombolytic drugs and transferredGiven thrombolytic drugs and transferred Remained with dense paralysis, inability to speak 2 hours laterRemained with dense paralysis, inability to speak 2 hours later Brought to angiographyBrought to angiography

46
Case Immediately recovered partial use of right hand and footImmediately recovered partial use of right hand and foot Talking the following dayTalking the following day Was discharged to home 3 days later with mild right sided weakness, but speech intactWas discharged to home 3 days later with mild right sided weakness, but speech intact

47
Technology is not always easy…..

48
Summary What we can do through catheters is increasing every dayWhat we can do through catheters is increasing every day Many trials ongoing to determine the best therapy for stroke and heart diseaseMany trials ongoing to determine the best therapy for stroke and heart disease Stay tuned!Stay tuned!

Similar presentations


























>")