Download presentation
Presentation is loading. Please wait.

1
Transfer of Lipids Mike Clark, M.D.

2
Cholesterol

3
Recommended Daily Diet
45% – 65% of daily kilocalories Carbohydrates (most being complex carbohydrates) 20% - 35% of daily kilocalories from *Fats 10 – 35% of daily kilocalories from Protein Thus on a 2,000 kilocalorie diet you should get Total Carbohydrates grams with at least 25 grams being fiber Total fat grams or less Total Protein grams * Next slide breaks down fats
 20% - 35% of daily kilocalories from *Fats. 10 – 35% of daily kilocalories from Protein. Thus on a 2,000 kilocalorie diet you should get. Total Carbohydrates grams with at least 25 grams being fiber. Total fat grams or less. Total Protein grams. * Next slide breaks down fats.")
4
Daily Recommendations
Cholesterol in the body (1) comes from the diet (2) recycled within the body through reabsorption of bile in the digestive tract or (3) synthesized in the body. For a person of about 70 Kg. person typical total body cholesterol content is about 35 g, with typical daily dietary intake is 200–300 mg in (United States) and approximately 1 gram produced daily by the body. Daily Recommendations total fat: less than 65 g saturated fat: less than 20 g cholesterol: less than 300 mg (milligrams) sodium: less than 2,400 mg Potassium: 3,500 mg
 comes from the diet (2) recycled within the body through reabsorption of bile in the digestive tract or (3) synthesized in the body. For a person of about 70 Kg. person typical total body cholesterol content is about 35 g, with typical daily dietary intake is 200–300 mg in (United States) and approximately 1 gram produced daily by the body. Daily Recommendations. total fat: less than 65 g. saturated fat: less than 20 g. cholesterol: less than 300 mg (milligrams) sodium: less than 2,400 mg. Potassium: 3,500 mg.")
5
Function of Cholesterol
Cholesterol is required to build and maintain cell membranes; it regulates membrane fluidity over the range of physiological temperatures. Within the cell membrane, cholesterol also functions in intracellular transport, cell signalling and nerve conduction. Recently, cholesterol has also been implicated in cell signaling processes, assisting in the formation of lipid rafts in the plasma membrane. In many neurons a myelin sheath, rich in cholesterol since it is derived from compacted layers of Cholesterol is an important precursor molecule for the synthesis of Vitamin D and the steroid hormones, including the adrenal gland hormones cortisol and aldosterone as well as the sex hormones progesterone, estrogens, and testosterone and their derivatives.

6
Cholesterol Structure Cholesterol is a sterol type steroid - are also known as steroid alcohol. When a steroid has an OH (hydroxyl) group at the 3-position of the A-ring – it is termed a sterol.
 group at the 3-position of the A-ring – it is termed a sterol..")
7
What is a Cholesterol Ester?
A cholesteryl ester is, as its name would imply, an ester of cholesterol. The ester bond is formed between the carboxylate group of a fatty acid and the hydroxyl group (on 3rd carbon) of cholesterol. Cholesteryl Esters have a lower solubility in water than Cholesterol. They are associated with atherosclerosis
 of cholesterol. Cholesteryl Esters have a lower solubility in water than Cholesterol. They are associated with atherosclerosis.")
8
Cholesterol Ester

9
Dietary sources Animal fats are complex mixtures of triglycerides, with lesser amounts of phospholipids and cholesterol. Consequently all foods containing animal fat contain cholesterol to varying extents. Major dietary sources of cholesterol include cheese, egg yolks, beef, pork, poultry, and shrimp. Human breast milk also contains significant quantities of cholesterol. Cholesterol is not present in plant based food sources unless it has been added during the food's preparation. However, plant products such as flax seeds and peanuts contain healthy cholesterol-like compounds called phytosterols, which are suggested to help lower serum cholesterol levels.

10
Synthesis About 20–25% of total daily cholesterol production occurs in the liver; other sites of high synthesis rates include the intestines, adrenal glands and reproductive organs. Synthesis within the body starts with one molecule of acetyl CoA and one molecule of acetoacetyl. HMG-CoA reductase is an important enzyme in Cholesterol Production – this is the enzyme targeted by the Statin (HMG-CoA Reductase Inhibitors) drugs.
 drugs.")
11
Regulation of cholesterol synthesis
Biosynthesis of cholesterol is directly regulated by the cholesterol levels present, though the homeostatic mechanisms involved are only partly understood. A higher intake from food leads to a net decrease in endogenous production, while lower intake from food has the opposite effect.

12
Plasma transport and regulation of absorption
Cholesterol is only slightly soluble in water; it can dissolve and travel in the water-based bloodstream at exceedingly small concentrations. Since cholesterol is insoluble in blood, it is transported in the circulatory system within lipoproteins. Cholesterol since it has the polar hydroxyl group is slightly soluble in water – but the esterified form is less soluble in water. It is more able to be packaged into small areas for transport and storage.

13
Cholesterol esters, i.e. with long-chain fatty acids linked to the hydroxyl group, are much less polar than free cholesterol and appear to be the preferred form for transport in plasma and for storage. They do not contribute to membranes but are packed into intracellular lipid particles.

14
Metabolism, recycling and excretion
Cholesterol is oxidized by the liver into a variety of primary bile acids. These primary bile acids are “ cholic acid” and chenodeoxycholic acid. When these primary bile acids are secreted into the intestines in bile - bacteria in the large intestines converts some these into secondary bile acids – deoxycholic acid (from cholic acid) and lithocholic acid (from chenodeoxycholic acid). Bacteria also did this to bilirubin. In the liver some of the primary bile acids are conjugated (covalently bonded to primarily glycine and taurine – making them more water soluble- just as bilirubin was conjugated to make it more water soluble. When the primary bile acids are conjugated they are called bile salts – then named glycocholic acid and taurocholic acid. Thus a mixture of conjugated and non-conjugated bile acids along with cholesterol itself is excreted from the liver into the bile. Approximately 95% of the bile acids are reabsorbed from the intestines and the remainder lost in the feces. The excretion and reabsorption of bile acids forms the basis of the enterohepatic circulation. which is essential for the digestion and absorption of dietary fats.
 and lithocholic acid (from chenodeoxycholic acid). Bacteria also did this to bilirubin. In the liver some of the primary bile acids are conjugated (covalently bonded to primarily glycine and taurine – making them more water soluble- just as bilirubin was conjugated to make it more water soluble. When the primary bile acids are conjugated they are called bile salts – then named glycocholic acid and taurocholic acid. Thus a mixture of conjugated and non-conjugated bile acids along with cholesterol itself is excreted from the liver into the bile. Approximately 95% of the bile acids are reabsorbed from the intestines and the remainder lost in the feces. The excretion and reabsorption of bile acids forms the basis of the enterohepatic circulation. which is essential for the digestion and absorption of dietary fats.")
15
Serum Lipid Transport

16
Some lipids come from diet (exogenous)
Some lipids are produced by the body (endogenously)
")
17
Lipids Fatty Acids Triglycerides Phospholipids Steroids Carotenoids
Eicosanoids Fat Soluble Vitamins

18
Help with the transport involves usage of proteins and phospholipids
Serum Lipids involved in metabolism that need assistance with transport in the blood Fatty Acids Triglycerides Cholesterol Fat Soluble Vitamins Help with the transport involves usage of proteins and phospholipids NOTE: Anything that is lipid soluble or highly oxidative (Iron) also need transport assistance in the blood like lipid hormones (cortisol)
 also need transport assistance in the blood like lipid hormones (cortisol)")
19
General Lipoprotein Structure
A core consisting of hydrophobic substances – cholesterol esters and Triglycerides Surrounding the core are amphipathic and hydrophilic substances – unesterified cholesterol, phospholipids and proteins The density of the lipoprotein depends on the relative percentage of protein – more protein more dense.

20
Lipoprotein Structure
Apoprotein NONPOLAR LIPID CORE Cholesterol Ester Triglyceride POLAR SURFACE COAT Phospholipid Free cholesterol Lipoprotein Structure Adapted from Treatment of Heart Diseases :1992, Etiologies and Treatment of Hyperlipidemia-Scott Grundy, MD, PhD

21
Phospholipid responsibility Protein responsibility
Since they are amphipathic – they give the hydrophobic lipids increased water solubility- emulsification Protein responsibility The proteins are termed apolipoproteins. Responsible for activating certain enzymes in metabolism and as attachments of the lipoprotein to the cell membranes (ligand)
")
22
Micelle Bile assists in this function
Not a lipoprotein but involved in exogenous lipid metabolism Need to get lipids in intestine underneath the water layer so that these lipids can get to the top of the intestinal epithelial cells for absorption – thus need to form a “micelle” This process involves making lipids soluble in water “emulsification” Bile assists in this function

23
Bile Composition Remember bile is formed in the liver and stored in the gallbladder its function is to solubilize (emulsify) fats in the small intestines Water – when stored in gallbladder considerable water is removed from the bile so as to make it more concentrated thus easier to store. Unesterified Cholesterol Bile pigments (Bilirubin) Bile salts (glycocholic acid & taurocholic acid) Bile acids – primary – cholic acid and chenodeoxycholic acid Bile acids – secondary – deoxycholic acid and lithocholic acid Phospholipids (mainly lecithin) Dipalmitoyl phosphatidyl choline Electrolytes Bicarbonate
 fats in the small intestines. Water – when stored in gallbladder considerable water is removed from the bile so as to make it more concentrated thus easier to store. Unesterified Cholesterol. Bile pigments (Bilirubin) Bile salts (glycocholic acid & taurocholic acid) Bile acids – primary – cholic acid and chenodeoxycholic acid. Bile acids – secondary – deoxycholic acid and lithocholic acid. Phospholipids (mainly lecithin) Dipalmitoyl phosphatidyl choline. Electrolytes. Bicarbonate.")
24
Micelle

25
Microvilli (brush border) Absorptive cells Lacteal Goblet cell Blood
capillaries Vilus Mucosa associated lymphoid tissue Enteroendocrine cells Intestinal crypt Venule Muscularis mucosae Lymphatic vessel Duodenal gland Submucosa (b) Figure 23.22b
 Figure 23.22b.")
26
Serum Lipids needing assistance with transport in the blood
Fatty Acids Triglycerides Fat Soluble Vitamins Cholesterol Help with the transport involves usage of proteins and phospholipids

27
Transporting Lipoproteins
Chylomicron Very Low Density Lipoprotein (VLDL) Low Density Lipoprotein (LDL) Intermediate Density Lipoprotein (IDL) High Density Lipoprotein (HDL)
 Low Density Lipoprotein (LDL) Intermediate Density Lipoprotein (IDL) High Density Lipoprotein (HDL)")
30
Chylomicron Function 80% – 95% Triglyceride 3%-6% Phospholipid
2% - 7% Cholesterol % – 2% Proteins Function Chylomicrons transport exogenous lipids to liver, adipose, cardiac and skeletal muscle tissue where their triglyceride components are unloaded by the activity of lipoprotein lipase. Consequently, chylomicron remnants are left over and are taken up by the liver. Stages There are three stages in the chylomicrons "life cycle": Nascent chylomicron Mature chylomicron - after HDL gives it some apoproteins Chylomicron remnant – after some triglycerides removed

31
Nascent (newly formed) chylomicrons in small intestine epithelial cells
Chylomicrons are created by the absorptive cells of the small intestine. They are relatively large, having a diameter of 75 to 1,200nm. These nascent chylomicrons are released by exocytosis from enterocytes into lacteals, lymphatic vessels originating in the villi of the small intestine, and are then secreted into the bloodstream at the thoracic duct's connection with the left subclavian vein. Nascent chylomicrons are primarily composed of triglycerides (85%) and contain some cholesterol and cholesteryl esters. The main apolipoprotein component is apolipoprotein B-48 (APOB48). Mature chylomicron (after acted upon by HDL) While circulating in lymph and blood, chylomicrons exchange components with high-density lipoproteins (HDL). The HDL donates apolipoprotein C-II (APOC2) and apolipoprotein E (APOE) to the nascent chylomicron and thus converts it to a mature chylomicron (often referred to simply as "chylomicron"). APOC2 is the cofactor for lipoprotein lipase (LPL) activity. Chylomicron remnant (after has loss considerable amounts of triglycerides Once triglyceride stores are distributed, the chylomicron returns APOC2 to the HDL (but keeps APOE) and thus becomes a chylomicron remnant, now only nm. APOB48 and APOE are important to identify the chylomicron remnant in the liver for endocytosis and breakdown.
 and contain some cholesterol and cholesteryl esters. The main apolipoprotein component is apolipoprotein B-48 (APOB48). Mature chylomicron (after acted upon by HDL) While circulating in lymph and blood, chylomicrons exchange components with high-density lipoproteins (HDL). The HDL donates apolipoprotein C-II (APOC2) and apolipoprotein E (APOE) to the nascent chylomicron and thus converts it to a mature chylomicron (often referred to simply as chylomicron ). APOC2 is the cofactor for lipoprotein lipase (LPL) activity. Chylomicron remnant (after has loss considerable amounts of triglycerides. Once triglyceride stores are distributed, the chylomicron returns APOC2 to the HDL (but keeps APOE) and thus becomes a chylomicron remnant, now only nm. APOB48 and APOE are important to identify the chylomicron remnant in the liver for endocytosis and breakdown.")
33
VLDL (mainly carries triglycerides)
55% – 65% Triglyceride %-20% Phospholipid 10% - 15% Cholesterol % – 10% Proteins Very low-density lipoprotein (VLDL) is a type of lipoprotein made by the liver. VLDL transports endogenous products whereas chylomicrons transport exogenous (dietary) products. VLDL transports endogenous triglycerides, phospholipids, cholesterol and cholesteryl esters. It functions as the body's internal transport mechanism for lipids
 is a type. of lipoprotein made by the liver. VLDL transports endogenous products whereas chylomicrons transport exogenous (dietary) products. VLDL transports endogenous triglycerides, phospholipids, cholesterol and cholesteryl esters. It functions as the body s internal transport mechanism for lipids.")
34
Changes during circulation
Nascent VLDL circulates in blood and picks up apolipoprotein C-II and apolipoprotein E donated from High-Density Lipoprotein (HDL). At this point, the nascent VLDL becomes a mature VLDL. Once in circulation, the VLDL will come in contact with lipoprotein lipase (LPL) in the capillary beds in the body (adipose, cardiac, and skeletal muscle). The LPL will remove triglycerides from the VLDL for storage or energy production. The VLDL now meets back up with HDL where apoC-II is transferred back to the HDL (but keeps apoE). In addition to this, the HDL transfers cholesteryl esters to the VLDL in exchange for phospholipids and triglycerides (via cholesteryl ester transfer protein). As more and more triglycerides are removed from the VLDL because of the action of the LPL enzyme, the composition of the molecule changes, and it becomes intermediate density lipoprotein (IDL).
. At this point, the nascent VLDL becomes a mature VLDL. Once in circulation, the VLDL will come in contact with lipoprotein lipase (LPL) in the capillary beds in the body (adipose, cardiac, and skeletal muscle). The LPL will remove triglycerides from the VLDL for storage or energy production. The VLDL now meets back up with HDL where apoC-II is transferred back to the HDL (but keeps apoE). In addition to this, the HDL transfers cholesteryl esters to the VLDL in exchange for phospholipids and triglycerides (via cholesteryl ester transfer protein). As more and more triglycerides are removed from the VLDL because of the action of the LPL enzyme, the composition of the molecule changes, and it becomes intermediate density lipoprotein (IDL).")
35
Intermediate Density Lipoprotein (IDL) (transient role has equal amounts of cholesterol and triglycerides) 50% of IDLs are recognized by receptors in the liver cells (because of the apoB-100 and apoE they contain) and are endocytosed. The other 50% of IDL lose their apoE. When their cholesterol content becomes greater than the triglyceride content, they become low-density lipoprotein (LDL), with the primary apolipoprotein being apoB-100.
 and are endocytosed. The other 50% of IDL lose their apoE. When their cholesterol content becomes greater than the triglyceride content, they become low-density lipoprotein (LDL), with the primary apolipoprotein being apoB-100.")
36
Low Density Lipoprotein (primarily carries cholesterol) sometimes referred to as your “Bad Cholesterol” 10% Triglyceride % Phospholipid 45 % Cholesterol % Proteins Low-density lipoprotein (LDL) is a type of lipoprotein that transports cholesterol and triglycerides from the liver to peripheral tissues. When a cell requires cholesterol, it synthesizes the necessary LDL receptors, and inserts them into the plasma membrane. The LDL receptors diffuse freely until they associate with clathrin-coated pits. LDL particles in the blood stream bind to these extracellular LDL receptors. The clathrin-coated pits then form vesicles that are endocytosed into the cell. The LDL is taken into a cell via the LDL receptor (endocytosis) where the contents are either stored, used for cell membrane structure, or converted into other products (steroid hormones or bile acids).
 is a type of lipoprotein that transports cholesterol and triglycerides from the liver to peripheral tissues. When a cell requires cholesterol, it synthesizes the necessary LDL receptors, and inserts them into the plasma membrane. The LDL receptors diffuse freely until they associate with clathrin-coated pits. LDL particles in the blood stream bind to these extracellular LDL receptors. The clathrin-coated pits then form vesicles that are endocytosed into the cell. The LDL is taken into a cell via the LDL receptor (endocytosis) where the contents are either stored, used for cell membrane structure, or converted into other products (steroid hormones or bile acids).")
37
5% Triglyceride 30 % Phospholipid 20% Cholesterol 45% – 55% Proteins
High Density Lipoprotein (HDL) (scavenges extra cholesterol taking to the liver) sometimes called your “Good Cholesterol” 5% Triglyceride % Phospholipid 20% Cholesterol % – 55% Proteins HDL is produced by the liver Function is to scoop up and transport excess cholesterol from peripheral tissues to the liver Provides apolipoproteins to Chylomicrons, VLDL and LDL
 (scavenges extra cholesterol taking to the liver) sometimes called your Good Cholesterol 5% Triglyceride 30 % Phospholipid. 20% Cholesterol 45% – 55% Proteins. HDL is produced by the liver. Function is to scoop up and transport excess cholesterol from peripheral tissues to the liver. Provides apolipoproteins to Chylomicrons, VLDL and LDL.")
38
Bile mixes with lipids forming a micelle
Complete Story Eat meal with cholesterol, triglycerides, fatty acids and fat soluble vitamins Triglycerides are broken down to a monoglyceride and two fatty acids by pancreatic lipase (some salivary and gastric) – all other lipids stay as they are In order to absorb lipids need bile to emulsify the lipids so as to allow them to pass below the water layer lining the intestines– bile enters first part of intestines (Duodenum) from hepatopancreatic duct – same duct that allowed the pancreatic lipase into the intestines. Bile mixes with lipids forming a micelle The Micelle allows the fat to move to the top of the intestinal epithelial cells
 – all other lipids stay as they are. In order to absorb lipids need bile to emulsify the lipids so as to allow them to pass below the water layer lining the intestines– bile enters first part of intestines (Duodenum) from hepatopancreatic duct – same duct that allowed the pancreatic lipase into the intestines. Bile mixes with lipids forming a micelle. The Micelle allows the fat to move to the top of the intestinal epithelial cells.")
39
Triglyceride

40
Figure 23.36

41
6. The lipids are allowed into the intestinal epithelial cells by simple diffusion – particularly at the ileum (last part of small intestine) 7. The bile forming the micelle will stay behind and some is absorbed later in the small intestine and large intestines (enterohepatic circulation) and some is eliminated in the feces. Remember in the large intestines, normal flora bacteria convert some of the primary acids in bile to secondary acids and half of the bilirubin was converted to urobilinogen (lecture given earlier on bilirubin). 8. Once the fats are in the in the intestinal epithelial cells – the monoglycerides are reunited to form triglycerides and all of the lipids are packaged into the chylomicrons.
 7. The bile forming the micelle will stay behind and some is absorbed later in the small intestine and large intestines (enterohepatic circulation) and some is eliminated in the feces. Remember in the large intestines, normal flora bacteria convert some of the primary acids in bile to secondary acids and half of the bilirubin was converted to urobilinogen (lecture given earlier on bilirubin). 8. Once the fats are in the in the intestinal epithelial cells – the monoglycerides are reunited to form triglycerides and all of the lipids are packaged into the chylomicrons.")
42
Figure 23.20

43
9. The chylomicrons are too large to diffuse through the epithelial cell membrane or the through the basement membrane so they are extruded by exocytosis. 10. The chylomicrons then enter the central lacteal of the lymphatics and the lymphatics carry them to the bloodstream at the Thoracic Duct. 11. Once in the bloodstream capillary endothelial cells in skeletal muscle, cardiac muscle and adipose tissue– produce and secrete “lipoprotein lipase” – this causes the chylomicron to hydrolyze the triglycerides ( to breakdown to glycerol and 3 fatty acids) these are absorbed into the myocytes and adipocytes. Some fatty acids are whisked away by albumin to go to other cells in particular the liver cells. When the Chylomicron releases some of its triglycerides and HDL takes its cholesterol and apolipoproteins becomes a Chylomicron Remnant. The Chylomicron remnant enters the liver cells by endocytosis for breakdown – thus the remaining triglycerides along with the absorbed cholesterol are now in the liver for storage or subsequent transport. Lipoprotein lipase is an enzyme that hydrolyzes lipids in lipoproteins, such as those found in chylomicrons and very low-density lipoproteins (VLDL), into three free fatty acids and one glycerol molecule. It requires Apo-CII as a cofactor. Lipoprotein lipase is specifically found in endothelial cells lining the capillaries. LPL encodes lipoprotein lipase, which is expressed in heart, muscle, and adipose tissue. LPL functions as a homodimer, and has the dual functions of triglyceride hydrolase and ligand/bridging factor for receptor-mediated lipoprotein uptake. Severe mutations that cause LPL deficiency result in type I hyperlipoproteinemia, while less extreme mutations in LPL are linked to many disorders of lipoprotein metabolism. Regulation Insulin is known to enhance LPL synthesis in adipocytes and its placement in the capillary endothelium. LPL has different isozymes in different tissues. The form that is in adipocytes is activated by insulin, whereas that in muscle and myocardium is not. This helps to explain why adipose cells gain fat in a well-fed state. Pathology Lipoprotein lipase deficiency leads to hypertriglyceridemia (elevated levels of triglycerides in the bloodstream).
 these are absorbed into the myocytes and adipocytes. Some fatty acids are whisked away by albumin to go to other cells in particular the liver cells. When the Chylomicron releases some of its triglycerides and HDL takes its cholesterol and apolipoproteins becomes a Chylomicron Remnant. The Chylomicron remnant enters the liver cells by endocytosis for breakdown – thus the remaining triglycerides along with the absorbed cholesterol are now in the liver for storage or subsequent transport. Lipoprotein lipase is an enzyme that hydrolyzes lipids in lipoproteins, such as those found in chylomicrons and very low-density lipoproteins (VLDL), into three free fatty acids and one glycerol molecule. It requires Apo-CII as a cofactor. Lipoprotein lipase is specifically found in endothelial cells lining the capillaries. LPL encodes lipoprotein lipase, which is expressed in heart, muscle, and adipose tissue. LPL functions as a homodimer, and has the dual functions of triglyceride hydrolase and ligand/bridging factor for receptor-mediated lipoprotein uptake. Severe mutations that cause LPL deficiency result in type I hyperlipoproteinemia, while less extreme mutations in LPL are linked to many disorders of lipoprotein metabolism. Regulation. Insulin is known to enhance LPL synthesis in adipocytes and its placement in the capillary endothelium. LPL has different isozymes in different tissues. The form that is in adipocytes is activated by insulin, whereas that in muscle and myocardium is not. This helps to explain why adipose cells gain fat in a well-fed state. Pathology. Lipoprotein lipase deficiency leads to hypertriglyceridemia (elevated levels of triglycerides in the bloodstream).")
44
Figure 23.21b, c

45
13. The liver stores some of the lipids and some it sends out by forming VLDL. This is high in Triglycerides (55%- 65%) and somewhat lower in cholesterol (10% -15%). 14. The VLDL then circulates until it is met by lipoprotein lipase in the capillary endothelial cells of adipose tissue (need insulin) , cardiac muscle and skeletal muscle. Lipoprotein Lipase as before causes triglycerides to dissolve and be absorbed by the mentioned cells. This then increases the density of the lipoprotein forming IDL (Intermediate Density Lipoprotein). 15. Some (50%) of IDL is taken up by the liver and broken down – the other 50% loses more triglycerides thus increasing the relative density of the lipoprotein and the amount of cholesterol – until finally becoming LDL (Low Density Lipoprotein).
 , cardiac muscle and skeletal muscle. Lipoprotein Lipase as before causes triglycerides to dissolve and be absorbed by the mentioned cells. This then increases the density of the lipoprotein forming IDL (Intermediate Density Lipoprotein). 15. Some (50%) of IDL is taken up by the liver and broken down – the other 50% loses more triglycerides thus increasing the relative density of the lipoprotein and the amount of cholesterol – until finally becoming LDL (Low Density Lipoprotein).")
46
Low Density Lipoprotein primarily carries Cholesterol (45%)
Low Density Lipoprotein primarily carries Cholesterol (45%). It circulates until it is bound to LDL receptors. Every cell in the body forms LDL receptors in that every cell in the body needs cholesterol. Some cells such as those forming the steroid hormones need more receptors. The amount of receptors placed in the cell membrane is under the control of homeostasis. The liver generally sports lots of LDL receptors thus clearing about 70% of LDL. The liver does to store cholesterol and decrease the amount of cholesterol in the circulation – thus minimizing atherosclerosis. LDL and its lipid contents are taken into cells by receptor mediated endocytosis and broken down. The cell that performed the endocytosis uses the lipids for its own purposes. However – the cholesterol in the liver is stored so as to be transported to cells that need cholesterol – by forming VLDL again – thus the story starts again.
. It circulates until it is bound to LDL receptors. Every cell in the body forms LDL receptors in that every cell in the body needs cholesterol. Some cells such as those forming the steroid hormones need more receptors. The amount of receptors placed in the cell membrane is under the control of homeostasis. The liver generally sports lots of LDL receptors thus clearing about 70% of LDL. The liver does to store cholesterol and decrease the amount of cholesterol in the circulation – thus minimizing atherosclerosis. LDL and its lipid contents are taken into cells by receptor mediated endocytosis and broken down. The cell that performed the endocytosis uses the lipids for its own purposes. However – the cholesterol in the liver is stored so as to be transported to cells that need cholesterol – by forming VLDL again – thus the story starts again.")
47
18. HDL is not part of the conversion process of VLDL to IDL to LDL
18. HDL is not part of the conversion process of VLDL to IDL to LDL. It is produced independently primarily by the liver and some by intestinal cells It functions to scoop up and transport excess cholesterol from peripheral tissues to the liver- thus scavenging the excess cholesterol “Good Cholesterol” It also provides apolipoproteins to Chylomicrons and VLDL – thus enhancing their efforts to keep excess triglycerides out of the circulation

48
Desired Blood Lipid Levels
Desirable Borderline High High Cholesterol (Adult) < 200 mg/dl >240 LDL < > 160 HDL > 45 TC/HDL ratio <4.5 Triglycerides < 150
 < 200 mg/dl >240. LDL < > 160. HDL > 45. TC/HDL ratio <4.5. Triglycerides < 150.")
50
What drugs are most commonly used to treat high cholesterol and triglycerides?
The drugs of first choice for elevated LDL cholesterol are the HMG CoA reductase inhibitors Another class of drugs for lowering LDL is the bile acid sequestrants — colesevelam, cholestyramine and colestipol — and nicotinic acid (niacin). Other available drugs are gemfibrozil, fenofibrate and clofibrate. These fibric acid derivatives are primarily used for lowering high triglyceride levels.
. Other available drugs are gemfibrozil, fenofibrate and clofibrate. These fibric acid derivatives are primarily used for lowering high triglyceride levels.")
51
The drugs of first choice for elevated LDL cholesterol are the HMG CoA reductase inhibitors, e.g., atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvastatin and simvastatin. Statin drugs are very effective for lowering LDL cholesterol levels and have few immediate short-term side effects.

52
Another class of drugs for lowering LDL is the bile acid sequestrants — colesevelam, cholestyramine and colestipol — and nicotinic acid (niacin). These have been shown to reduce the risk for coronary heart disease in controlled clinical trials. Nicotinic acid is preferred in patients with triglyceride levels that exceed 250 mg/dL because bile acid sequestrants tend to raise triglyceride levels.

53
Other available drugs are gemfibrozil, fenofibrate and clofibrate
Other available drugs are gemfibrozil, fenofibrate and clofibrate. These fibric acid derivatives are primarily used for lowering high triglyceride levels. Fibric acid derivatives (FADs) are a class of drugs that have been shown to reduce the production of very low-density lipoprotein (VLDL) while enhancing VLDL clearance due to the stimulation of lipoprotein lipase activity. The drugs can reduce plasma triglyceride levels while raising high-density lipoprotein (HDL) cholesterol levels. Their effects on low-density lipoprotein (LDL) cholesterol levels are less marked and more variable
 are a class of drugs that have been shown to reduce the production of very low-density lipoprotein (VLDL) while enhancing VLDL clearance due to the stimulation of lipoprotein lipase activity. The drugs can reduce plasma triglyceride levels while raising high-density lipoprotein (HDL) cholesterol levels. Their effects on low-density lipoprotein (LDL) cholesterol levels are less marked and more variable.")
54
Coronary Heart Disease and Artery Disease
Arteriosclerosis versus Atherosclerosis Arteriosclerosis is a general term describing any hardening (and loss of elasticity) of medium or large arteries. It should not be confused with "arteriolosclerosis" or "atherosclerosis".
 of medium or large arteries. It should not be confused with arteriolosclerosis or atherosclerosis .")
55
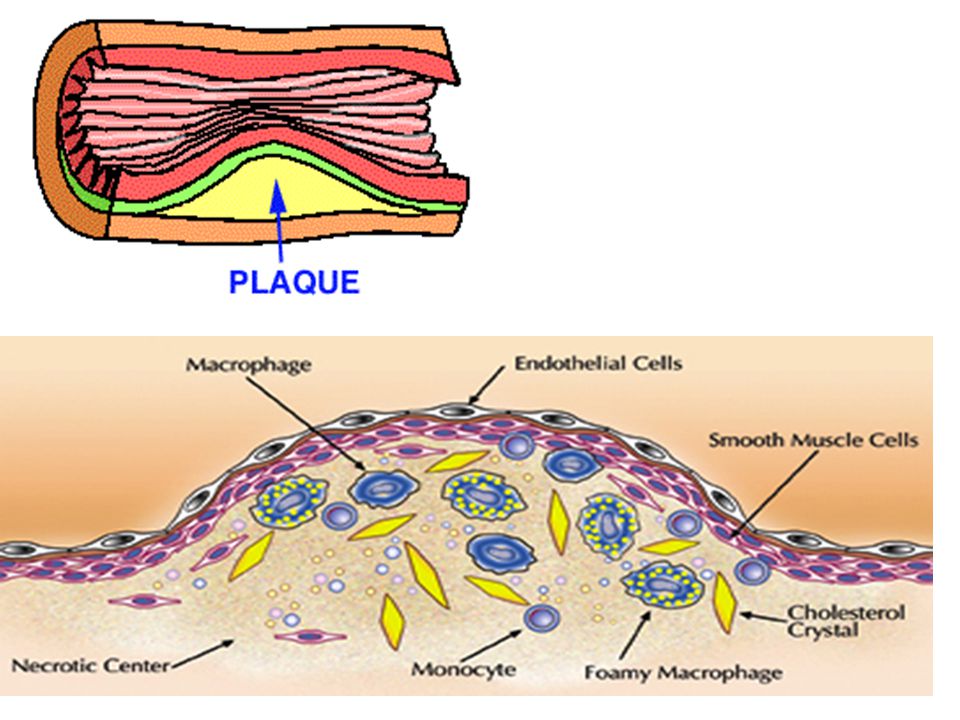
Arteriolosclerosis is any hardening (and loss of elasticity) of arterioles (small arteries). It is often due to hypertension. Atherosclerosis is a hardening of an artery specifically due to an atheromatous plaque. Atherosclerosis is the most common form of arteriosclerosis. Atherosclerosis is characterized by a thickening of the intima with plaques that can contain lipid-laden macrophages ("foam cells"). The plaques contain free lipid (cholesterol, etc.) and are prone to calcification and ulceration.
. The plaques contain free lipid (cholesterol, etc.) and are prone to calcification and ulceration.")
56
Other Types of Arteriosclerosis
Arteriosclerosis obliterans is typically seen in medium and large arteries of the lower extremity. Characterized by fibrosis of the intima and calcification of the media. The lumen of the vessel may be obliterated or markedly narrowed. Medial calcific sclerosis (Monckeberg’s calcific sclerosis) is seen mostly in the elderly, commonly in arteries of the thyroid and uterus. Characterized by calcification of the internal elastic lamina but without thickening of the intima or narrowing of the vessel lumen. A similar form of an intramural calcification, presenting the picture of an early phase of arteriosclerosis, appears to be induced by a number of drugs that have an antiproliferative mechanism of action.[2]
 is seen mostly in the elderly, commonly in arteries of the thyroid and uterus. Characterized by calcification of the internal elastic lamina but without thickening of the intima or narrowing of the vessel lumen. A similar form of an intramural calcification, presenting the picture of an early phase of arteriosclerosis, appears to be induced by a number of drugs that have an antiproliferative mechanism of action.[2]")
57
Coronary Artery Disease (CAD)
Cocaine-induced arrhythmias and myocardial infarcts: the heart beats faster and more forcefully, increasing myocardial oxygen requirements Blood lipids and CAD Triglyceride: derived from ingested fat as well as from carbohydrates and sugar Cholesterol: derived from ingested cholesterol and dietary fat; saturated fat (found in meats and dairy products) raises blood cholesterol; unsaturated fats (found in fish, poultry, and most vegetable oils) tends to lower cholesterol
 raises blood cholesterol; unsaturated fats (found in fish, poultry, and most vegetable oils) tends to lower cholesterol.")
58
Coronary Artery Disease
Homocysteine and CAD: Vitamin B and folic acid are necessary to metabolize homocysteine; elevated homocysteine blood levels is a risk factor for atherosclerosis comparable to high lipids, smoking and hypertension; homocysteine levels are higher in men than in premenopausal women but increase in menopausal women Chlamydia pneumoniae and CAD: Chlamydia pneumoniae has been isolated in plaques, which may contribute to arterial intimal damage Several recent studies have shown a link between dental disease and coronary heart disease. There is a correlation of coronary artery disease with dental plaque. Salivary levels of Streptococcus sanguis and complaints of xerostomia. In some cases dental disease is a larger risk factor for heart disease than being overweight, having a high cholesterol level, not exercising or smoking.

59
Coronary Heart Disease
Caused by atherosclerosis of the large coronary arteries, where the arteries narrow owing to accumulation of fatty materials The lipid deposits, consisting of neutral fat and cholesterol, accumulate in the arteries by diffusion from the bloodstream Pathogenesis of atherosclerosis Endothelial injury Lipids accumulate and precipitate Secondary fibrosis and calcification Formation of atheroma

61
Coronary Heart Disease Risk Factors
Elevated blood lipids High blood pressure Cigarette smoking Diabetes Other risk factors that play a less important role Obesity accompanied by high blood lipids and elevated blood pressure Personality: type A personality, which is aggressive, hard driving, and competitive

62
Manifestations of Coronary Heart Disease
Also referred to as Ischemic Heart Disease It is related to a decrease in blood supply to the heart muscle caused by narrowing or obstruction of the coronary arteries The clinical manifestations are quite variable Some individuals are free of symptoms Some experience chest oppression that may radiate into neck or arms The pain which is caused by myocardial ischemia is called Angina pectoris Stable angina: pain occurs on exertion, subsides with rest, and is relieved by nitroglycerine

63
Myocardial Infarction Location
Most often involves left ventricle Anterior wall Left anterior descending artery distribution Lateral wall Circumflex artery distribution Posterior wall Right coronary distribution Massive anterior and lateral wall Main left coronary distribution

64
Myocardial Infarction Triggers
Any one of four basic mechanisms may trigger a heart attack in a patient with coronary heart disease Sudden blockage of a coronary artery, usually caused by a clot, coronary thrombosis Hemorrhage into an atheromatous plaque, usually caused by rupture of a small blood vessel adjacent to the plaque, which enlarges the plaque, further narrowing the lumen of the artery

65
Myocardial Infarction Triggers
3. Arterial spasm, which occurs adjacent to atheromatous plaque and precipitates arterial narrowing or obstruction 4. Sudden, greatly increased myocardial oxygen requirements, caused by vigorous activity such as running which abruptly increases cardiac output, which in turn raises myocardial oxygen consumption

66
Myocardial Infarction Complications
Arrhythmias: disturbances of cardiac rhythm, most serious is ventricular fibrillation, which leads to cessation of circulation Heart failure: ventricles may be badly damaged, unable to maintain normal cardiac function, and heart fails Intracardial thrombi: may be carried to systemic circulation, causing infarction to brain, kidneys, spleen

67
Myocardial Infarction Complications
Pericarditis: infarct extends to the epicardial surface, which leads to accumulation of fluid and inflammatory cells in the pericardial sac Cardiac rupture: a perforation may occur through the necrotic muscle, permits blood to leak into the pericardial sac, compressing the heart; ventricles cannot fill in diastole, causing cardiac tamponade Papillary muscle dysfunction: the papillary muscle becomes infarcted, unable to contract normally, causing the mitral valve to prolapse slightly into the LA, and causing mitral insufficiency

68
Myocardial Infarction Complications
Ventricular aneurysm: late complication, an outward bulging of the healing infarct during ventricular systole. Aneurysm sac fills with blood rather than being ejected to the aorta and cardiac output is reduced. Survival Depends on size, patient’s age, complications, other diseases Mortality rates vary from 6% with small infarcts that do not develop heart failure to more than 50% with large infarcts that develop severe heart failure

69
Myocardial Infarction Complications
Major causes of death following an MI Fatal arrhythmia Heart failure Cardiac rupture with cardiac tamponade 90% of hospitalized patients survive

70
Myocardial Infarction Diagnosis
Medical history: may at times be inconclusive because severe angina may be similar to the pain of MI Physical examination: will usually not be abnormal unless patient exhibits evidence of shock, heart failure, etc. Laboratory data: physician must rely on these Electrocardiogram: measures the transmission of electrical impulses associated with cardiac contraction, indicating the location and size of infarct (elevated ST segment means MI happening now whereas Q wave means old MI)
")
71
Myocardial Infarction Diagnosis
Enzyme tests: heart muscle is rich in enzymes and proteins that regulate its activities, that leak from the necrotic cells into circulation when muscle becomes infarcted Most importantly Troponin T and troponin I (proteins concerned with muscle contractions) Creatine kinase (heart muscle enzyme) 3. Lactic dehydrogenase (heart muscle enzyme) 4. Myoglobin (muscle protein)
 Creatine kinase (heart muscle enzyme) 3. Lactic dehydrogenase (heart muscle enzyme) 4. Myoglobin (muscle protein)")
72
Myocardial Infarction: Treatment
Anticoagulant drugs: to reduce the coagulability of blood, decreasing the likelihood of thrombus and emboli Beta-blockers: reduce myocardial irritability, often given to patients after recovering from MI Aspirin: small amount to inhibit platelet function, therefore making them less likely to adhere to roughened atheromatous plaques that can initiate a thrombosis

73
Myocardial Infarction: Treatment
Factors controlled or eliminated Cessation of smoking Control of hypertension 3.An anticoronary diet- low cholesterol and fat 4. Weight reduction 5. Graduated exercise program Surgical treatment: myocardial revascularization procedures Bypass surgery: bypasses the obstructions in the coronary arteries usually by means of segments of saphenous veins obtained from the patient’s legs

74
Myocardial Infarction: Treatment
Coronary angioplasty: dilates areas of narrowing within coronary arteries, rather than bypassing them (major surgery) A guided catheter introduced through skin and into a large artery in the arm or leg threaded under fluoroscopic control into the narrowed coronary artery, and positioned at the site of narrowing. Then a balloon catheter is inflated under very high pressure, which smashes the plaque and pushes it into the arterial wall, enlarging the lumen of the artery
 A guided catheter introduced through skin and into a large artery in the arm or leg threaded under fluoroscopic control into the narrowed coronary artery, and positioned at the site of narrowing. Then a balloon catheter is inflated under very high pressure, which smashes the plaque and pushes it into the arterial wall, enlarging the lumen of the artery.")
Similar presentations












 75% of your cholesterol is.>")
 it must have a charge –Triglycerides don’t have any.>")




>")


 Atheroma as the presence of fatty material within the walls of arteries. The link between atheroma and the increased.>")

